
Aquatic Therapy versus Standard Rehabilitation after Surgical Rotator Cuff Repair: A Randomized Prospective Study

 , and
, and
Abstract
:Simple Summary
Abstract
1. Introduction
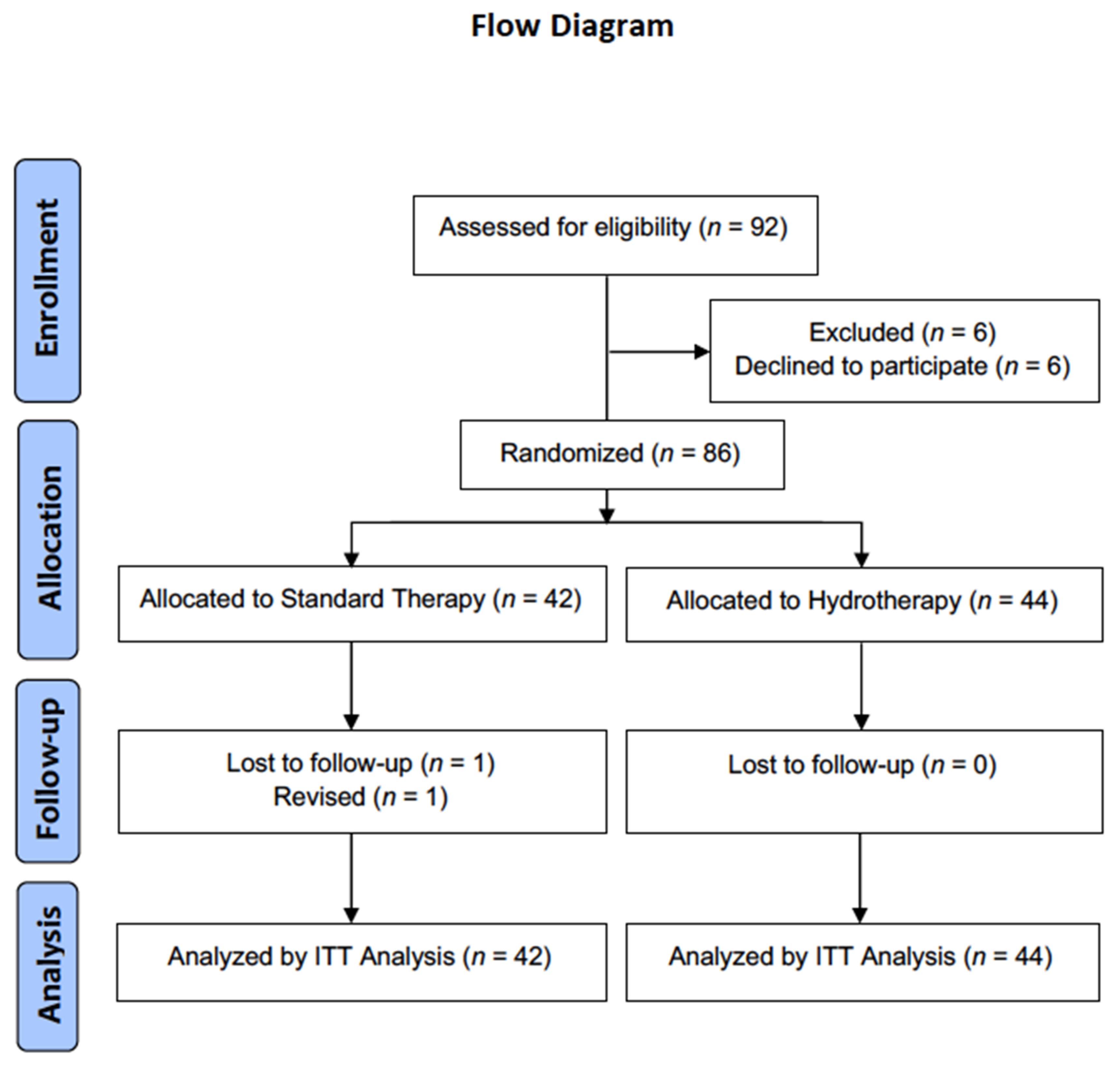
2. Materials and Methods
2.1. Pre- and Post-Operative Clinical Assessment
2.2. Randomization Process
2.3. Surgical Procedure
2.4. Rehabilitation Protocol
2.5. Statistical Analysis
3. Results
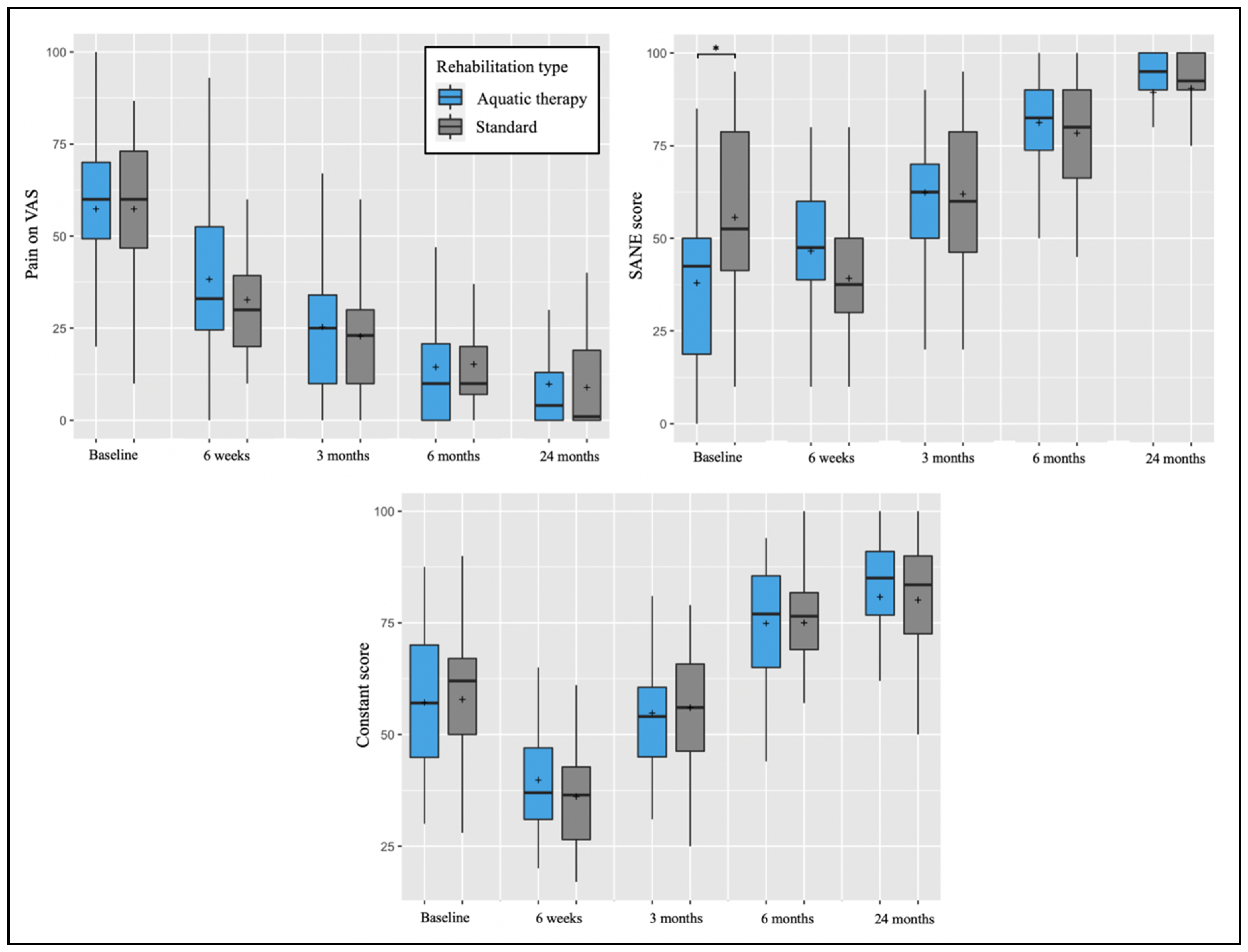
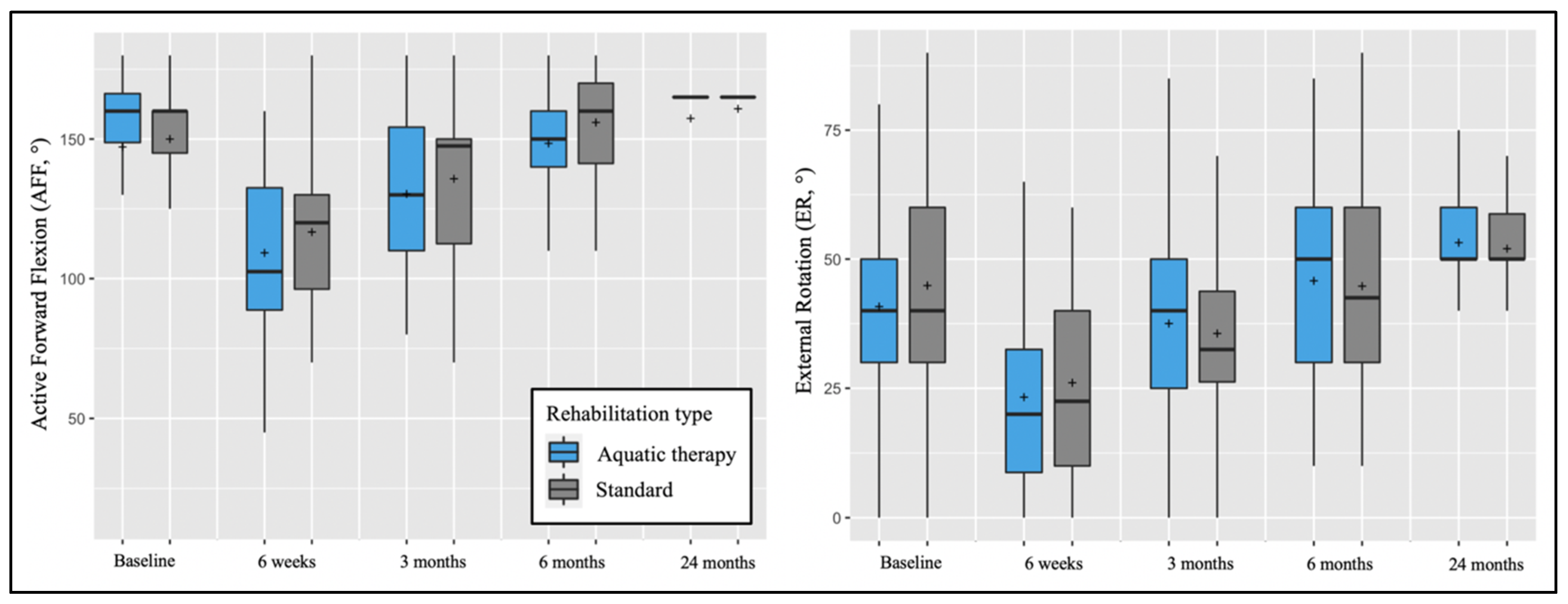
Clinical Outcomes
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Boileau, P.; Brassart, N.; Watkinson, D.J.; Carles, M.; Hatzidakis, A.M.; Krishnan, S.G. Arthroscopic repair of full-thickness tears of the supraspinatus: Does the tendon really heal? J. Bone Joint Surg. Am. 2005, 87, 1229–1240. [Google Scholar] [CrossRef] [PubMed]
- Collin, P.; Abdullah, A.; Kherad, O.; Gain, S.; Denard, P.J.; Lädermann, A. Prospective evaluation of clinical and radiologic factors predicting return to activity within 6 months after arthroscopic rotator cuff repair. J. Shoulder Elbow Surg. 2015, 24, 439–445. [Google Scholar] [CrossRef] [PubMed]
- Collin, P.G.; Gain, S.; Nguyen Huu, F.; Lädermann, A. Is rehabilitation effective in massive rotator cuff tears? Orthop. Traumatol. Surg. Res. 2015, 101, S203–S205. [Google Scholar] [CrossRef] [PubMed]
- Denard, P.J.; Lädermann, A.; Burkhart, S.S. Prevention and management of stiffness after arthroscopic rotator cuff repair: Systematic review and implications for rotator cuff healing. Arthroscopy 2011, 27, 842–848. [Google Scholar] [CrossRef]
- Peltz, C.D.; Sarver, J.J.; Dourte, L.M.; Wurgler-Hauri, C.C.; Williams, G.R.; Soslowsky, L.J. Exercise following a short immobilization period is detrimental to tendon properties and joint mechanics in a rat rotator cuff injury model. J. Orthop. Res. 2010, 28, 841–845. [Google Scholar] [CrossRef] [Green Version]
- Burmaster, C.; Eckenrode, B.J.; Stiebel, M. Early Incorporation of an Evidence-Based Aquatic-Assisted Approach to Arthroscopic Rotator Cuff Repair Rehabilitation: Prospective Case Study. Phys. Ther. 2016, 96, 53–61. [Google Scholar] [CrossRef] [Green Version]
- Brady, B.; Redfern, J.; MacDougal, G.; Williams, J. The addition of aquatic therapy to rehabilitation following surgical rotator cuff repair: A feasibility study. Physiother. Res. Int. 2008, 13, 153–161. [Google Scholar] [CrossRef]
- Speer, K.P.; Cavanaugh, J.T.; Warren, R.F.; Day, L.; Wickiewicz, T.L. A role for hydrotherapy in shoulder rehabilitation. Am. J. Sports Med. 1993, 21, 850–853. [Google Scholar] [CrossRef]
- Thomson, S.; Jukes, C.; Lewis, J. Rehabilitation following surgical repair of the rotator cuff: A systematic review. Physiotherapy 2016, 102, 20–28. [Google Scholar] [CrossRef]
- Giaquinto, S.; Ciotola, E.; Dall’Armi, V.; Margutti, F. Hydrotherapy after total knee arthroplasty. A follow-up study. Arch. Gerontol. Geriatr. 2010, 51, 59–63. [Google Scholar] [CrossRef]
- Rahmann, A.E.; Brauer, S.G.; Nitz, J.C. A specific inpatient aquatic physiotherapy program improves strength after total hip or knee replacement surgery: A randomized controlled trial. Arch. Phys. Med. Rehabil. 2009, 90, 745–755. [Google Scholar] [CrossRef] [PubMed]
- Chae, C.S.; Jun, J.H.; Im, S.; Jang, Y.; Park, G.Y. Effectiveness of Hydrotherapy on Balance and Paretic Knee Strength in Patients with Stroke: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Am. J. Phys. Med. Rehabil. 2020, 99, 409–419. [Google Scholar] [CrossRef] [PubMed]
- Lädermann, A.; Kadri, F.; Cikes, A. Evaluation of 3 different rehabilitation protocols after rotator cuff repair, and the effectiveness of pool therapy: A randomized control study. Orthop. J. Sports Med. 2021, 9. [Google Scholar] [CrossRef]
- Lädermann, A.; Burkhart, S.S.; Hoffmeyer, P.; Neyton, L.; Collin, P.; Yates, E.; Denard, P.J. Classification of full-thickness rotator cuff lesions: A review. EFORT Open Rev. 2016, 1, 420–430. [Google Scholar] [CrossRef]
- Patte, D. Classification of rotator cuff lesions. Clin. Orthop. Relat. Res. 1990, 254, 81–86. [Google Scholar] [CrossRef]
- Goutallier, D.; Postel, J.M.; Bernageau, J.; Lavau, L.; Voisin, M.C. Fatty muscle degeneration in cuff ruptures. Pre- and postoperative evaluation by CT scan. Clin. Orthop. Relat. Res. 1994, 304, 78–83. [Google Scholar] [CrossRef]
- Abrassart, S.; Kolo, F.; Piotton, S.; Chiu, J.C.-H.; Stirling, P.; Hoffmeyer, P.; Lädermann, A. ‘Frozen shoulder’ is ill-defined. How can it be described better? EFORT Open Rev. 2020, 5, 273–279. [Google Scholar] [CrossRef]
- Williams, G.N.; Gangel, T.J.; Arciero, R.A.; Uhorchak, J.M.; Taylor, D.C. Comparison of the Single Assessment Numeric Evaluation method and two shoulder rating scales. Outcomes measures after shoulder surgery. Am. J. Sports Med. 1999, 27, 214–221. [Google Scholar] [CrossRef]
- Constant, C.R.; Murley, A.H. A clinical method of functional assessment of the shoulder. Clin. Orthop. Relat. Res. 1987, 214, 160–164. [Google Scholar] [CrossRef]
- Richards, R.R.; An, K.N.; Bigliani, L.U.; Friedman, R.J.; Gartsman, G.M.; Gristina, A.G.; Iannotti, J.P.; Mow, V.C.; Sidles, J.A.; Zuckerman, J.D. A standardized method for the assessment of shoulder function. J. Shoulder Elbow Surg. 1994, 3, 347–352. [Google Scholar] [CrossRef]
- Roy, J.S.; Macdermid, J.C.; Faber, K.J.; Drosdowech, D.S.; Athwal, G.S. The simple shoulder test is responsive in assessing change following shoulder arthroplasty. J. Orthop. Sports Phys. Ther. 2010, 40, 413–421. [Google Scholar] [CrossRef] [PubMed]
- Plomb-Holmes, C.; Clavert, P.; Kolo, F.; Tay, E.; Ladermann, A.; French Arthroscopic, S. An orthopaedic surgeon’s guide to ultrasound imaging of the healthy, pathological and postoperative shoulder. Orthop. Traumatol. Surg. Res. 2018, 104, S219–S232. [Google Scholar] [CrossRef] [PubMed]
- Collin, P.; Yoshida, M.; Delarue, A.; Lucas, C.; Jossaume, T.; Lädermann, A.; French Society for Shoulder and Elbow (SOFEC). Evaluating postoperative rotator cuff healing: Prospective comparison of MRI and ultrasound. Orthop. Traumatol. Surg. Res. 2015, 101, S265–S268. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lädermann, A.; Chague, S.; Preissmann, D.; Kolo, F.C.; Zbinden, O.; Kevelham, B.; Bothorel, H.; Charbonnier, C. Acromioplasty during repair of rotator cuff tears removes only half of the impinging acromial bone. JSES Int. 2020, 4, 592–600. [Google Scholar] [CrossRef] [PubMed]
- Collin, P.; McCoubrey, G.; Lädermann, A. Posterosuperior rotator cuff repair by an independent double-row technique. Technical note and radiological and clinical results. Orthop. Traumatol. Surg. Res. 2016, 102, 405–408. [Google Scholar] [CrossRef]
- Barth, J.; Andrieu, K.; Fotiadis, E.; Hannink, G.; Barthelemy, R.; Saffarini, M. Critical period and risk factors for retear following arthroscopic repair of the rotator cuff. Knee Surg. Sports Traumatol. Arthrosc. 2017, 25, 2196–2204. [Google Scholar] [CrossRef]
- Hay, L.; Wylie, K. Towards evidence-based emergency medicine: Best BETs from the Manchester Royal Infirmary. BET 4: Hydrotherapy following rotator cuff repair. Emerg. Med. J. 2011, 28, 634–635. [Google Scholar] [CrossRef]
- Brislin, K.J.; Field, L.D.; Savoie, F.H., 3rd. Complications after arthroscopic rotator cuff repair. Arthroscopy 2007, 23, 124–128. [Google Scholar] [CrossRef]
- Huberty, D.P.; Schoolfield, J.D.; Brady, P.C.; Vadala, A.P.; Arrigoni, P.; Burkhart, S.S. Incidence and treatment of postoperative stiffness following arthroscopic rotator cuff repair. Arthroscopy 2009, 25, 880–890. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Standard Therapy (n = 42) | Aquatic Therapy (n = 44) | p-Value | |
|---|---|---|---|
| Age | 58.5 ± 9.8 | 55.0 ± 10.4 | 0.107 |
| BMI | 27.4 ± 16.9 | 25.4 ± 4.1 | 0.739 |
| Male sex (%) | 59.5 | 61.9 | 1.000 |
| Dominant side (%) | 69.0 | 76.2 | 0.813 |
| Standard (n = 42 Patients) | Aquatic Therapy (n = 44 Patients) | p-Value * | |||
|---|---|---|---|---|---|
| Mean ± SD | (Range) | Mean ± SD | (Range) | ||
| AFF (°) | |||||
| Baseline | 150.0 ± 28.2 | (15.0–180.0) | 147.2 ± 32.7 | (35.0–180.0) | 1.000 |
| 6 weeks | 116.7 ± 26.4 | (70.0–180.0) | 109.2 ± 30.8 | (45.0–160.0) | 1.000 |
| 3 months | 135.8 ± 30.5 | (70.0–180.0) | 130.3 ± 28.1 | (80.0–180.0) | 1.000 |
| 6 months | 156.0 ± 19.5 | (110.0–180.0) | 148.4 ± 18.9 | (100.0–180.0) | 0.225 |
| 2 years | 160.8 ± 15.9 | (75.0–180.0) | 157.4 ± 22.3 | (45.0–165.0) | 1.000 |
| ER (°) | |||||
| Baseline | 44.9 ± 22.3 | (0.0–90.0) | 40.8 ± 15.8 | (0.0–80.0) | 1.000 |
| 6 weeks | 26.1 ± 19.8 | (0.0–90.0) | 23.3 ± 20.7 | (0.0–70.0) | 1.000 |
| 3 months | 35.6 ± 18.4 | (0.0–90.0) | 37.5 ± 19.7 | (0.0–90.0) | 1.000 |
| 6 months | 44.8 ± 18.0 | (10.0–90.0) | 45.8 ± 19.0 | (10.0–85.0) | 1.000 |
| 2 years | 52.0 ± 13.6 | (0.0–90.0) | 53.2 ± 13.4 | (10.0–85.0) | 1.000 |
| Pain on VAS | |||||
| Baseline | 57.3 ± 18.3 | (10.0–86.7) | 57.3 ± 20.0 | (6.0–100.0) | 1.000 |
| 6 weeks | 32.7 ± 18.2 | (10.0–90.0) | 38.3 ± 21.3 | (0.0–97.0) | 0.928 |
| 3 months | 22.8 ± 14.3 | (0.0–60.0) | 25.3 ± 16.3 | (0.0–67.0) | 1.000 |
| 6 months | 15.2 ± 14.9 | (0.0–60.0) | 14.4 ± 15.1 | (0.0–53.0) | 1.000 |
| 2 years | 8.9 ± 11.7 | (0.0–40.0) | 9.8 ± 14.0 | (0.0–60.0) | 1.000 |
| SANE score | |||||
| Baseline | 55.6 ± 24.9 | (10.0–95.0) | 37.9 ± 23.6 | (0.0–85.0) | 0.019 |
| 6 weeks | 39.2 ± 16.7 | (10.0–80.0) | 46.6 ± 18.0 | (5.0–80.0) | 0.306 |
| 3 months | 62.0 ± 19.2 | (20.0–95.0) | 62.4 ± 14.4 | (20.0–90.0) | 1.000 |
| 6 months | 78.4 ± 15.3 | (45.0–100.0) | 81.2 ± 14.0 | (50.0–100.0) | 1.000 |
| 2 years | 90.5 ± 15.8 | (10.0–100.0) | 89.3 ± 17.1 | (20.0–100.0) | 1.000 |
| Constant score | |||||
| Baseline | 57.8 ± 16.8 | (21.0–90.0) | 57.1 ± 16.0 | (30.0–87.5) | 1.000 |
| 6 weeks | 36.2 ± 11.3 | (17.0–61.0) | 39.8 ± 13.6 | (20.0–74.0) | 1.000 |
| 3 months | 56.0 ± 13.4 | (25.0–79.0) | 54.8 ± 12.5 | (31.0–81.0) | 1.000 |
| 6 months | 75.0 ± 12.5 | (40.0–100.0) | 74.9 ± 12.9 | (44.0–94.0) | 1.000 |
| 2 years | 80.1 ± 15.0 | (18.0–100.0) | 80.8 ± 16.3 | (17.0–100.0) | 1.000 |
| ASES Score at 2 years | 88.9 ± 16.0 | (10.0–100.0) | 88.4 ± 14.9 | (33.0–100.0) | 0.864 |
| SST score at 2 years | 10.0 ± 2.2 | (3.0–12.0) | 9.9 ± 2.4 | (1.0–12.0) | 0.846 |
| Workstop (weeks) | 11.9 ± 8.4 | (0.0–28.0) | 15.3 ± 13.1 | (0.0–48.0) | 0.585 |
| Standard (n = 42 Patients) | Aquatic Therapy (n = 44 Patients) | p-Value | |||
|---|---|---|---|---|---|
| N | (%) | N | (%) | ||
| Sugaya classification | 0.443 | ||||
| Type 1 | 32 | (76.2%) | 39 | (88.6%) | |
| Type 2 | 5 | (11.9%) | 4 | (9.1%) | |
| Type 3 | 3 | (7.1%) | 1 | (2.3%) | |
| Type 4 | 1 | (2.4%) | 0 | (0.0%) | |
| Type 5 | 1 | (2.4%) | 0 | (0.0%) | |
| Satisfaction | 0.663 | ||||
| Very satisfied | 32 | (76.2%) | 36 | (81.8%) | |
| Satisfied | 5 | (11.9%) | 6 | (13.6%) | |
| Unsatisfied | 4 | (9.5%) | 2 | (4.5%) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dufournet, A.; Chong, X.L.; Schwitzguébel, A.; Bernimoulin, C.; Carvalho, M.; Bothorel, H.; Lädermann, A. Aquatic Therapy versus Standard Rehabilitation after Surgical Rotator Cuff Repair: A Randomized Prospective Study. Biology 2022, 11, 610. https://doi.org/10.3390/biology11040610
Dufournet A, Chong XL, Schwitzguébel A, Bernimoulin C, Carvalho M, Bothorel H, Lädermann A. Aquatic Therapy versus Standard Rehabilitation after Surgical Rotator Cuff Repair: A Randomized Prospective Study. Biology. 2022; 11(4):610. https://doi.org/10.3390/biology11040610
Chicago/Turabian StyleDufournet, Adrien, Xue Ling Chong, Adrien Schwitzguébel, Corinne Bernimoulin, Myriam Carvalho, Hugo Bothorel, and Alexandre Lädermann. 2022. "Aquatic Therapy versus Standard Rehabilitation after Surgical Rotator Cuff Repair: A Randomized Prospective Study" Biology 11, no. 4: 610. https://doi.org/10.3390/biology11040610