
Comparative Assessment of the Functional Parameters for Metal-Ceramic and All-Ceramic Teeth Restorations in Prosthetic Dentistry—A Literature Review

 ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
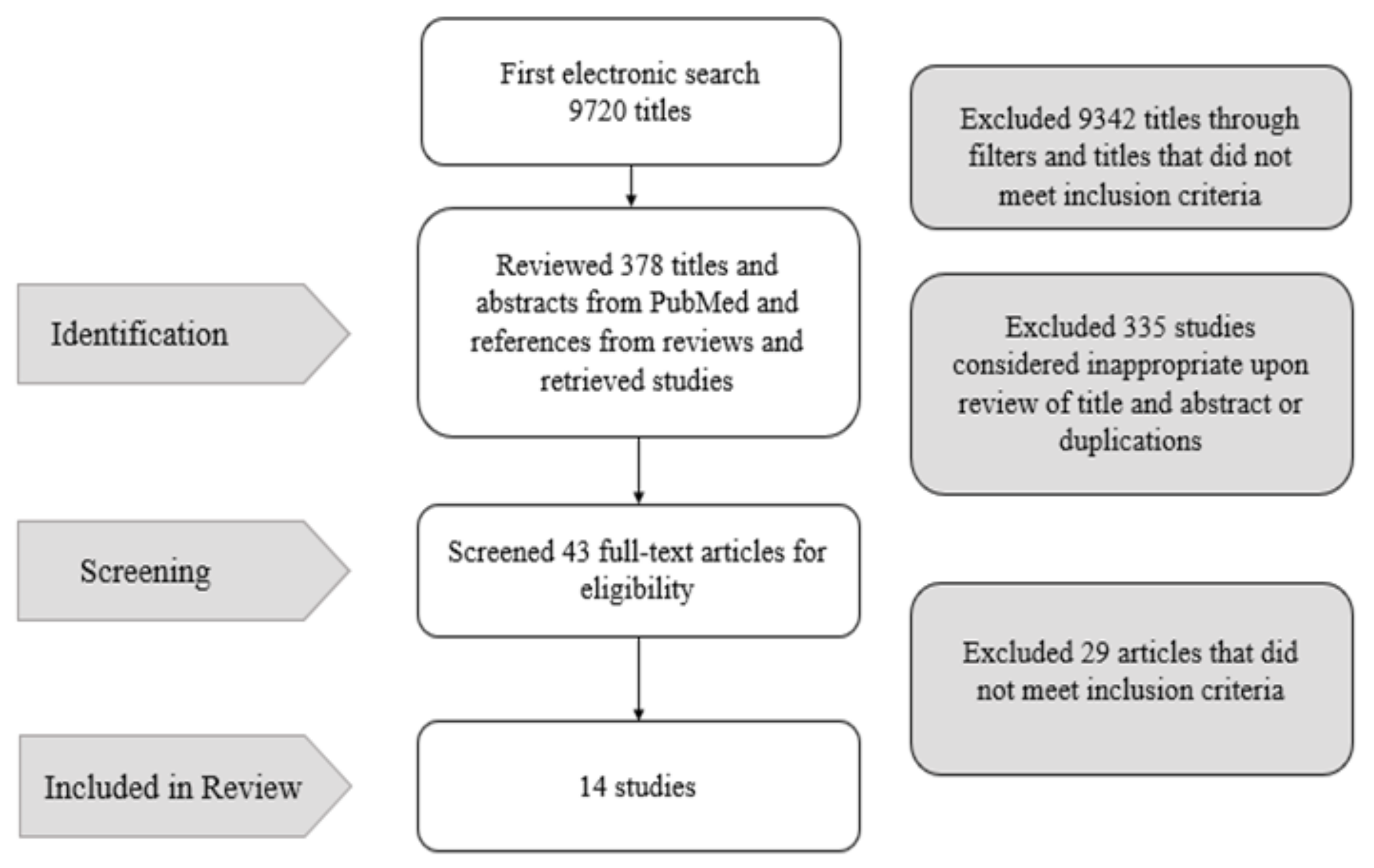
2. Materials and Methods
3. Results
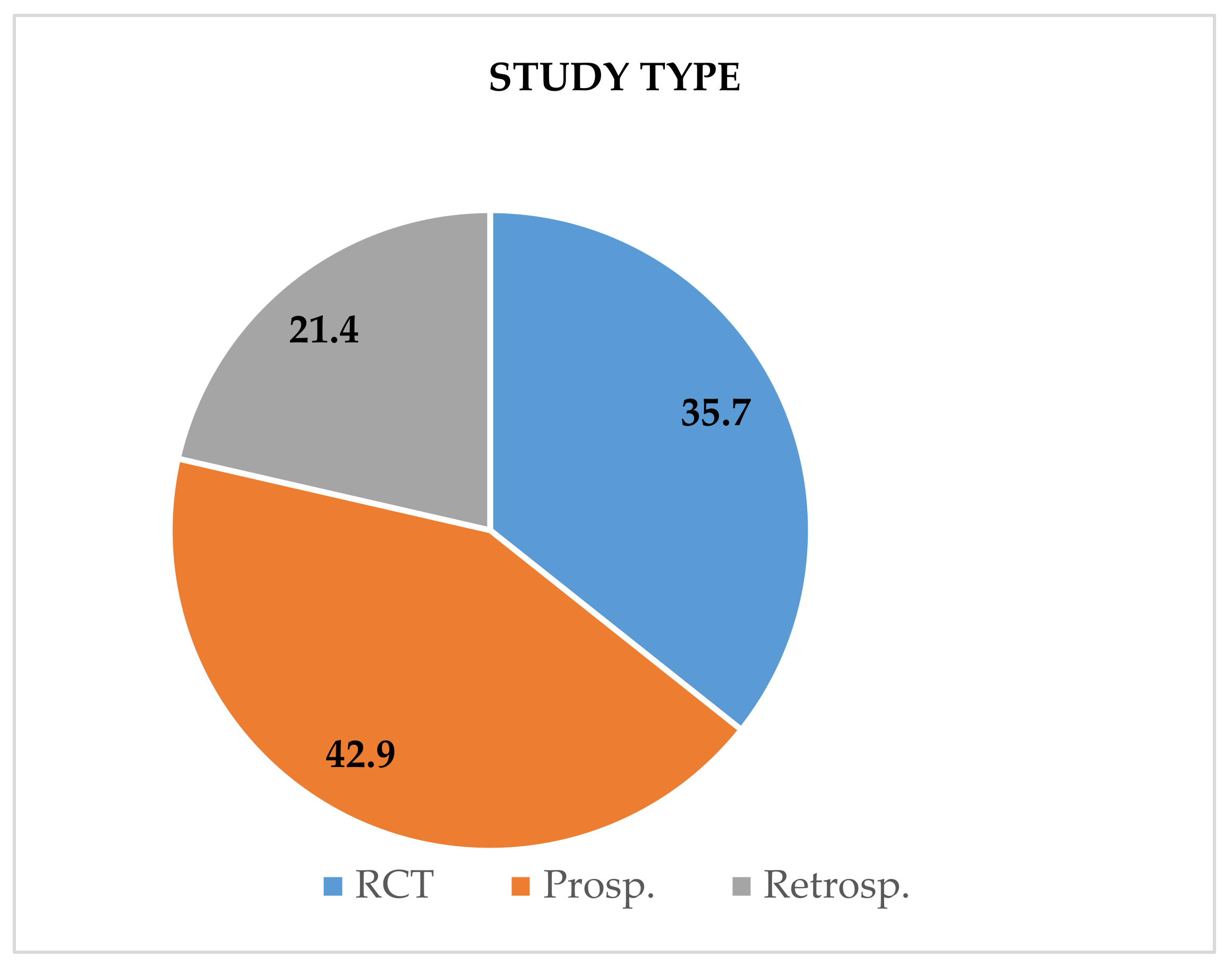
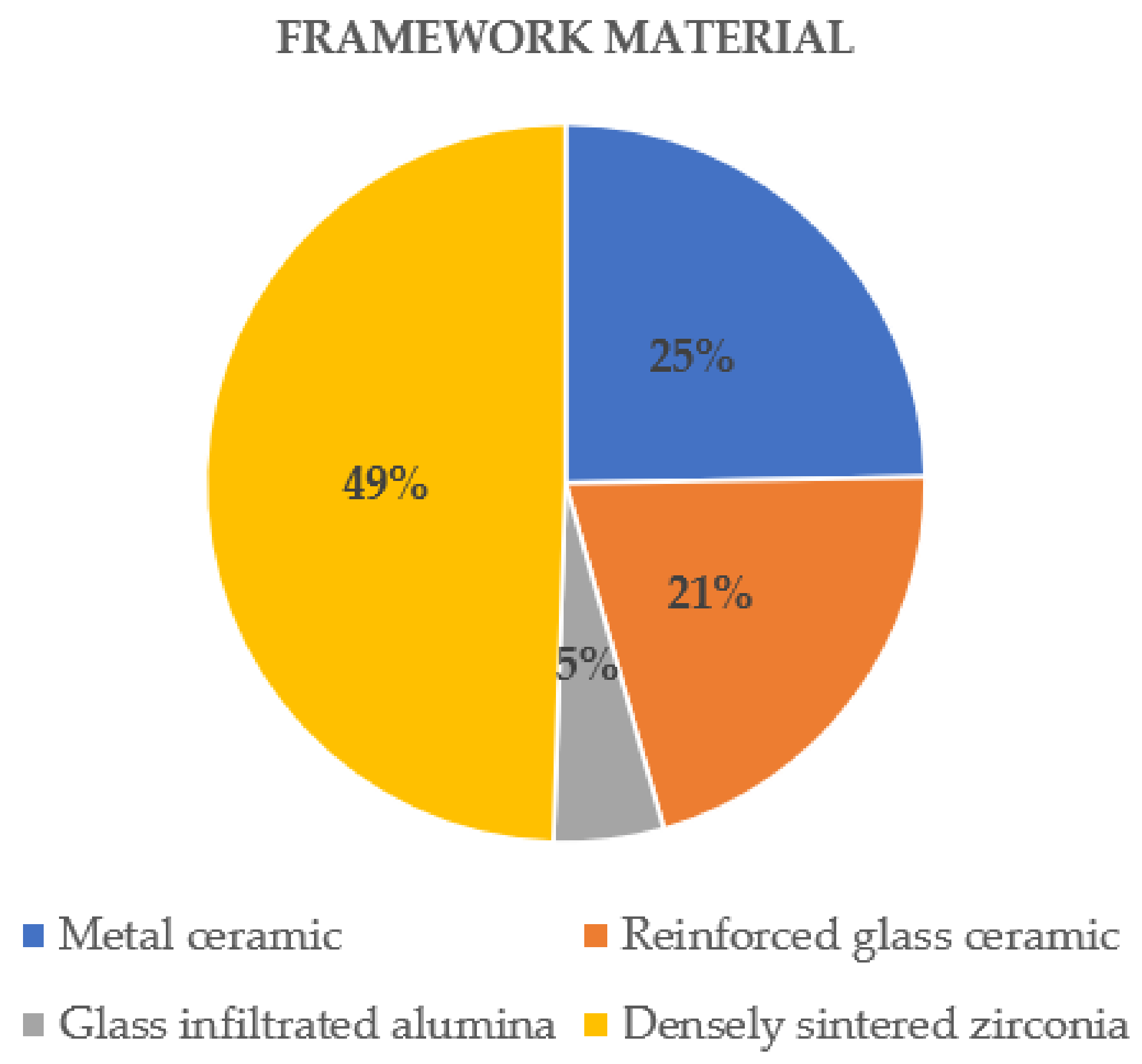
3.1. Characteristics of the Studies
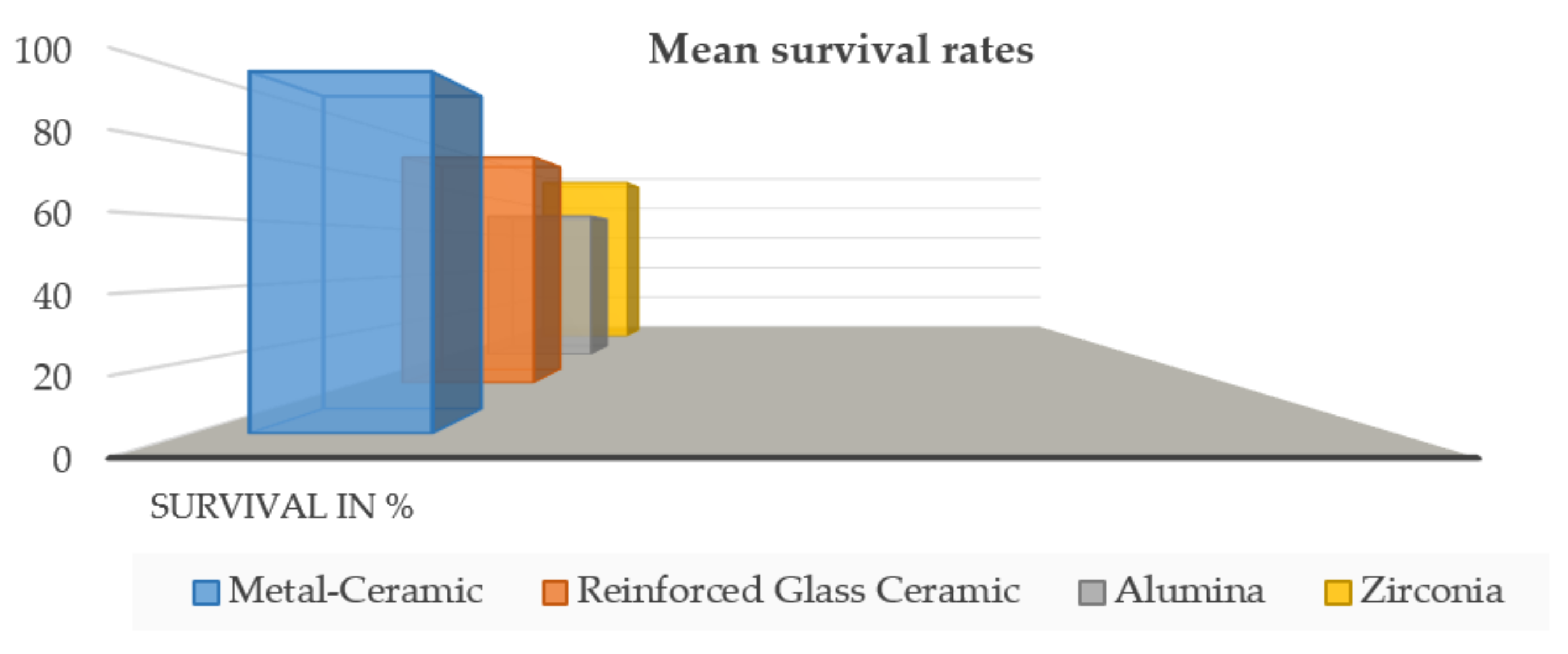
3.2. Survival of Fixed Partial Dentures
3.3. Biological Complications
3.3.1. Secondary Caries
3.3.2. Periodontal Disease
3.3.3. Abutment Tooth Fracture
3.4. Technical Complications
3.4.1. Framework or Core Fracture
3.4.2. Chipping
3.4.3. Ceramic Fracture
3.4.4. Loss of Retention
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Guess, P.; Schultheis, S.; Bonfante, E.; Coelho, P.; Ferencz, J.; Silva, N. All-ceramic systems: Laboratory and clinical performance. Dent. Clin. N. Am. 2011, 55, 333–352. [Google Scholar] [CrossRef] [PubMed]
- Monaco, C.; Rosentritt, M.; Llukacej, A.; Baldissara, P.; Scotti, R. Marginal adaptation, gap width, and fracture strength of teeth restored with different all-ceramic vs metal ceramic crown systems: An in vitro study. Eur. J. Prosthodont. Restor. Dent. 2016, 24, 130–137. [Google Scholar] [PubMed]
- Pjetursson, B.E.; Valente, N.A.; Strasding, M.; Zwahlen, M.; Liu, S.; Sailer, I. A Systematic Review of the Survival and Complication Rates of Zirconia-Ceramic and Metal-Ceramic Single Crowns. Clin. Oral Implant. Res. 2018, 29 (Suppl. 16), 199–214. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miura, S.; Yamauchi, S.; Kasahara, S.; Katsuda, Y.; Fujisawa, M.; Egusa, H. Clinical evaluation of monolithic zirconiacrowns: A failure analysis of clinically obtained cases from a 3.5-year study. J. Prosthodont. Res. 2020, 65, 148–154. [Google Scholar] [CrossRef]
- Zhang, Y.; Kelly, J.R. Dental Ceramics for Restoration and Metal Veneering. Dent. Clin. N. Am. 2017, 61, 797–819. [Google Scholar] [CrossRef]
- Saravi, B.; Vollmer, A.; Hartmann, M.; Lang, G.; Kohal, R.-J.; Boeker, M.; Patzelt, S.B.M. Clinical Performance of CAD/CAM All-Ceramic Tooth-Supported Fixed Dental Prostheses: A Systematic Review and Meta-Analysis. Materials 2021, 14, 2672. [Google Scholar] [CrossRef]
- Rosentritt, M.; Hahnel, S.; Engelhardt, F.; Behr, M.; Preis, V. In vitro performance and fracture resistance of CAD/CAM-fabricated implant supported molar crowns. Clin. Oral Investig. 2017, 21, 1213–1219. [Google Scholar] [CrossRef]
- Malament, K.A.; Natto, Z.S.; Thompson, V.; Rekow, D.; Eckert, S.; Weber, H.-P. Ten-Year Survival of Pressed, Acid-Etched e.Max Lithium Disilicate Monolithic and Bilayered Complete-Coverage Restorations: Performance and Outcomes as a Function of Tooth Position and Age. J. Pros. Dent. 2019, 121, 782–790. [Google Scholar] [CrossRef] [Green Version]
- Pahncke, E.; Hahnel, S.; Schierz, O.; Schmidt, M.B.; Schmutzler, A.; Rauch, A. Two-Year Longevity of Posterior Zirconia Multi-Unit Fixed Dental Prostheses with Monolithic Occlusal Surface. Appl. Sci. 2021, 11, 4449. [Google Scholar] [CrossRef]
- Jang, Y.-S.; Noh, H.-R.; Lee, M.-H.; Lim, M.-J.; Bae, T.-S. Effect of Lithium Disilicate Reinforced Liner Treatment on Bond and Fracture Strengths of Bilayered Zirconia All-Ceramic Crown. Materials 2018, 11, 77. [Google Scholar] [CrossRef] [Green Version]
- Poticny, D.J.; Klim, J. CAD/CAM in-Office Technology: Innovations after 25 Years for Predictable, Esthetic Outcomes. J. Am. Dent. Assoc. 2010, 141 (Suppl. 2), 5S–9S. [Google Scholar] [CrossRef]
- Reich, S.; Schierz, O. Chair-side generated posterior lithium disilicate crowns after 4 years. Clin. Oral Investig. 2013, 17, 1765–1772. [Google Scholar] [CrossRef]
- Cooper, L.F.; Stanford, C.; Feine, J.; McGuire, M. Prospective assessment of CAD/CAM zirconia abutment and lithium disilicate crown restorations: 2.4 year results. J. Prosth. Dent. 2016, 116, 33–39. [Google Scholar] [CrossRef]
- Baldi, A.; Comba, A.; Michelotto Tempesta, R.; Carossa, M.; Pereira, G.K.R.; Valandro, L.F.; Paolone, G.; Vichi, A.; Goracci, C.; Scotti, N. External Marginal Gap Variation and Residual Fracture Resistance of Composite and Lithium-Silicate CAD/CAM Overlays after Cyclic Fatigue over Endodontically-Treated Molars. Polymers 2021, 13, 3002. [Google Scholar] [CrossRef]
- Christensen, G.J. Indirect restoration use: A changing paradigm. J. Am. Dent. Assoc. 2012, 143, 398–400. [Google Scholar] [CrossRef]
- Beuer, F.; Schweiger, J.; Edelhoff, D. Digital Dentistry: An Overview of Recent Developments for CAD/CAM Generated Restorations. Br. Dent. J. 2008, 204, 505–551. [Google Scholar] [CrossRef]
- Fasbinder, D.J.; Dennison, J.B.; Heys, D.; Neiva, G. A clinical evaluation of chairside lithium disilicate CAD/CAM crowns: A two-year report. J. Am. Dent. Assoc. 2010, 141 (Suppl. 2), 10S–14S. [Google Scholar] [CrossRef]
- Anusavice, K.J.; Philips, R.W. Phillips’ Science of Dental Materials, 11th ed.; Elsevier/Saunders: St. Louis, MO, USA, 2003; Volume 48, pp. 421–423. [Google Scholar]
- Elsaka, S.E.; Einaghy, A.M. Mechanical properties of zirconia reinforced lithium silicate glass-ceramic. Dent. Mater. 2016, 32, 908–914. [Google Scholar] [CrossRef]
- Sen, N.; Us, Y.O. Mechanical and optical properties of monolithic CAD-CAM restorative materials. J. Prosthet. Dent. 2018, 119, 593–599. [Google Scholar] [CrossRef]
- Lops, D.; Mosca, D.; Casentini, P.; Ghisolfi, M.; Romeo, E. Prognosis of Zirconia Ceramic Fixed Partial Dentures: A 7-Year Prospective Study. Int. J. Prosthodont. 2012, 25, 21–23. [Google Scholar]
- Marchesi, G.; Camurri Piloni, A.; Nicolin, V.; Turco, G.; Di Lenarda, R. Chairside CAD/CAM Materials: Current Trends of Clinical Uses. Biology 2021, 10, 1170. [Google Scholar] [CrossRef]
- Iosif, L.; Barbinta-Patrascu, M.E.; Ispas, A. Zirconia, from optoelectronics to oral environment applicability. Optoelectron. Adv. Mat. 2020, 22, 635–646. [Google Scholar]
- Heintze, S.D.; Rousson, V. Survival of Zirconia- and Metal-Supported Fixed Dental Prostheses: A Systematic Review. Int. J. Prosthodont. 2010, 23, 493–502. [Google Scholar]
- Bahat, Z.; Mahmood, D.J.; Vult von Steyern, P. Fracture strength of three-unit fixed partial denture cores (Y-TZP) with different connector dimension and design. Swed. Dent. J. 2009, 33, 149–159. [Google Scholar]
- Nakai, H.; Inokoshi, M.; Nozaki, K.; Komatsu, K.; Kamijo, S.; Liu, H.; Shimizubata, M.; Minakuchi, S.; Van Meerbeek, B.; Vleugels, J.; et al. Additively Manufactured Zirconia for Dental Applications. Materials 2021, 14, 3694. [Google Scholar] [CrossRef] [PubMed]
- Lughi, V.; Sergo, V. Low temperature degradation -aging-of zirconia: A critical review of the relevant aspects in dentistry. Dent. Mater. 2010, 26, 807–820. [Google Scholar] [CrossRef]
- Anusavice, K.J. Standardizing failure, success, and survival decisions in clinical studies of ceramic and metal-ceramic fixed dental prostheses. Dent. Mater. 2012, 28, 102–111. [Google Scholar] [CrossRef] [Green Version]
- Tartaglia, G.M.; Sidoti, E.; Sforza, C. Seven-year prospective clinical study on zirconia-based single crowns and fixed dental prostheses. Clin. Oral Investig. 2015, 19, 1137–1145. [Google Scholar] [CrossRef]
- Sax, C.; Hammerle, C.H.; Sailer, I. 10-year clinical outcomes of fixed dental prostheses with zirconia frameworks. Int. J. Comput. Dent. 2011, 14, 183–202. [Google Scholar]
- Naenni, N.; Bindl, A.; Sax, C.; Hämmerle, C.; Sailer, I. A Randomized Controlled Clinical Trial of 3-Unit Posterior Zirconia-Ceramic Fixed Dental Prostheses (FDP) with Layered or Pressed Veneering Ceramics: 3-Year Results. J. Dent. 2015, 43, 1365–1370. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perry, R.D.; Kugel, G.; Sharma, S.; Ferreira, S.; Magnuson, B. Two-Year Evaluation Indicates Zirconia Bridges Acceptable Alternative to PFMs. Compend. Contin. Educ. Dent. 2012, 33, e1–e5. [Google Scholar]
- Selz, C.F.; Bogler, J.; Vach, K.; Strub, J.R.; Guess, P.C. Veneered Anatomically Designed Zirconia FDPs Resulting from Digital Intraoral Scans: Preliminary Results of a Prospective Clinical Study. J. Dent. 2015, 43, 1428–1435. [Google Scholar] [CrossRef]
- Sorrentino, R.; De Simone, G.; Tetè, S.; Russo, S.; Zarone, F. Five-Year Prospective Clinical Study of Posterior Three-Unit Zirconia-Based Fixed Dental Prostheses. Clin. Oral Investig. 2012, 16, 977–985. [Google Scholar] [CrossRef]
- Belli, R.; Petschelt, A.; Hofner, B.; Hajtó, J.; Scherrer, S.S.; Lohbauer, U. Fracture Rates and Lifetime Estimations of CAD/CAM All-Ceramic Restorations. J. Dent. Res. 2016, 95, 67–73. [Google Scholar] [CrossRef] [Green Version]
- Chaar, M.S.; Passia, N.; Kern, M. Ten-Year Clinical Outcome of Three-Unit Posterior FDPs Made from a Glass-Infiltrated Zirconia Reinforced Alumina Ceramic (In-Ceram Zirconia). J. Dent. 2015, 43, 512–517. [Google Scholar] [CrossRef]
- Makarouna, M.; Ullmann, K.; Lazarek, K.; Boening, K.W. Six-year clinical performance of lithium disilicate fixed partial dentures. Int. J. Prosthodont. 2011, 24, 204–206. [Google Scholar]
- Kern, M.; Sasse, M.; Wolfart, S. Ten-year outcome of three-unit fixed dental prostheses made from monolithic lithium disilicate ceramic. J. Am. Dent. Assoc. 2012, 143, 234–240. [Google Scholar] [CrossRef]
- Sola-Ruiz, M.F.; Lagos-Flores, E.; Roman-Rodriguez, J.L.; Highsmith Jdel, R.; Fons-Font, A.; Granell-Ruiz, M. Survival rates of a lithium disilicate-based core ceramic for three-unit esthetic fixed partial dentures: A 10-year prospective study. Int. J. Prosthodont. 2013, 26, 175–180. [Google Scholar] [CrossRef] [Green Version]
- Koenig, V.; Vanheusden, A.; Le Goff, S.; Mainjot, A. Clinical risk factors related to failures with zirconia-based restorations: An up to 9-year retrospective study. J. Dent. 2013, 41, 1164–1174. [Google Scholar] [CrossRef]
- Rinke, S.; Gersdorff, N.; Lange, K.; Roedinger, M. Prospective Evaluation of Zirconia Posterior Fixed Partial Dentures: 7-Year Clinical Results. Int. J. Prosthodont. 2013, 26, 164–171. [Google Scholar] [CrossRef] [Green Version]
- Christensen, R.P.; Ploeger, B.J. A Clinical Comparison of Zirconia, Metal and Alumina Fixed-Prosthesis Frameworks Veneered with Layered or Pressed Ceramic: A Three-Year Report. J. Am. Dent. Assoc. 2010, 141, 1317–1329. [Google Scholar] [CrossRef]
- Håff, A.; Löf, H.; Gunne, J.; Sjörgen, G. A retrospective evaluation of zirconia-fixed partial dentures in general practices: An up to 13-year study. Dent. Mater. 2015, 31, 162–170. [Google Scholar] [CrossRef]
- Ioannidis, A.; Bindl, A. Clinical prospective evaluation of zirconia-based three-unit posterior fixed dental prostheses: Up-to ten-year results. J. Dent. 2016, 47, 80–85. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nicolaisen, M.; Bahrami, G.; Schropp, L.; Isidor, F. Functional and Esthetic Comparison of Metal-Ceramic and All-Ceramic Posterior Three-Unit Fixed Dental Prostheses. Int. J. Prosthodont. 2016, 29, 473–481. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sailer, I.; Balmer, M.; Hüsler, J.; Hämmerle, C.; Känel, S.; Thoma, D. 10-year randomized trial (RCT) of zirconia-ceramic and metal-ceramic fixed dental prostheses. J. Dent. 2018, 76, 32–39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suarez, M.; Perez, C.; Pelaez, J.; Lopez-Suarez, C.; Gonzalo, E. A Randomized Clinical Trial Comparing Zirconia and Metal-Ceramic Three-Unit Posterior Fixed Partial Dentures: A 5-Year Follow-Up. J. Prosthodont. 2019, 28, 750–756. [Google Scholar] [CrossRef] [PubMed]
- Koenig, V.; Wulfman, C.; Bekaert, S.; Dupont, N.; Le Goff, S.; Eldafrawy, M.; Vanheusden, A.; Mainjot, A. Clinical behavior of second-generation zirconia monolithic posterior restorations: Two-year results of a prospective study with Ex vivo analyses including patients with clinical signs of bruxism. J. Dent. 2019, 91, 103229. [Google Scholar] [CrossRef]
- Brandt, S.; Winter, A.; Lauer, H.-C.; Kollmar, F.; Portscher-Kim, S.-J.; Romanos, G.E. IPS e.max for All-Ceramic Restorations: Clinical Survival and Success Rates of Full-Coverage Crowns and Fixed Partial Dentures. Materials 2019, 12, 462. [Google Scholar] [CrossRef] [Green Version]
- Forrer, F.; Schnider, N.; Brägger, U.; Yilmaz, B.; Hicklin, S. Clinical performance and patient satisfaction obtained with tooth-supported ceramic crowns and fixed partial dentures. J. Prost. Dent. 2020, 124, 446–453. [Google Scholar] [CrossRef]
- Baldi, A.; Comba, A.; Ferrero, G.; Italia, E.; Michelotto Tempesta, R.; Paolone, G.; Mazzoni, A.; Breschi, L.; Scotti, N. External gap progression after cyclic fatigue of adhesive overlays and crowns made with high translucency zirconia or lithium silicate. J. Esthet. Restor. Dent. 2021, 1–8. [Google Scholar] [CrossRef]
- Sailer, I.; Gottnerb, J.; Kanelb, S.; Hammerle, C.H. Randomized controlled clinical trial of zirconia-ceramic and metal-ceramic posterior fixed dental prostheses:a 3-year follow-up. Int. J. Prosthodont. 2009, 22, 553–560. [Google Scholar]
- Pjetursson, B.E.; Sailer, I.; Makarov, N.A.; Zwahlen, M.; Thoma, D.S. All ceramic or metal-ceramic tooth-supported fixed dental prostheses (FDPs)? A systematic review of the survival and complication rates. Part II: Multiple-unit FDPs. Dent. Mater. 2015, 31, 624–639. [Google Scholar]
- Layton, D. A critical appraisal of the survival and complication rates of tooth-supported all-ceramic and metal-ceramic fixed dental prostheses: The application of evidence-based dentistry. Int. J. Prosthodont. 2011, 24, 417–427. [Google Scholar]
- Raigrodski, A.J.; Yu, A.; Chiche, G.J.; Hochstedler, J.L.; Mancl, L.A.; Mohamed, S.E. Clinical efficacy of veneered zirconium dioxide-based posterior partial fixed dental prostheses: Five-year results. J. Prosthet. Dent. 2012, 108, 214–222. [Google Scholar] [CrossRef]
- Pelaez, J.; Cogolludo, P.G.; Serrano, B.; Serrano, J.F.; Suarez, M.J. A four-year prospective clinical evaluation of zirconia and metal-ceramic posterior fixed dental prostheses. Int. J. Prosthodont. 2012, 25, 451–458. [Google Scholar]
- Sulaiman, T.A.; Abdulmajeed, A.A.; Delgado, A.; Donovan, T.E. Fracture Rate of 188695 Lithium Disilicate and Zirconia Ceramic Restorations after up to 7.5 Years of Clinical Service: A Dental Laboratory Survey. J. Pros. Dent. 2020, 123, 807–810. [Google Scholar] [CrossRef]
- Chrisp, R.J.; Cowan, A.J.; Lamb, J.; Thompson, O.; Tulloch, N.; Burke, F.J.T. A clinical evaluation of all-ceramic bridges placed inpatients attending UK general dental practices: Three-year results. Dent. Mater. 2012, 28, 229–236. [Google Scholar] [CrossRef]
- Hooshmand, T.; Rostami, G.; Behroozibakhsh, M.; Fatemi, M.; Keshvad, A.; van Noort, R. Interfacial fracture toughness of different resin cements bonded to a lithium disilicate glass ceramic. J. Dent. 2012, 40, 139–145. [Google Scholar] [CrossRef]
- Lekesiz, H. Reliability estimation for single-unit ceramic crown restorations. J. Dent. Res. 2014, 93, 923–928. [Google Scholar] [CrossRef] [Green Version]
- Pospiech, P. All-ceramic crowns: Bonding or cementing? Clin. Oral Investig. 2002, 6, 189–197. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Year | Framework Material | Study Design | Observation Period (Y) | No. of Patients in Study | Age Range | Mean Age | Setting |
|---|---|---|---|---|---|---|---|---|
| Christensen et al. [37] | 2010 | Zirconia, metal, and alumina | RCT | 3 | 266 | 16–89 | 50 | Specialists and private practice |
| Makarouna et al. [38] | 2011 | Lithium disilicate | RCT | 6 | 18 | n.r. | 47 | University |
| Kem et al. [39] | 2012 | Lithium disilicate | Prosp. | 10 | 36 | n.r. | 47.5 | University |
| Sola-Ruiz et al. [40] | 2013 | Lithium disilicate | Prosp. | 10 | 21 | n.r. | 49 | University |
| Koenig et al. [41] | 2013 | Zirconia | Retrosp. | 9 | 30 | 25–79 | 54.6 | University |
| Rinke et al. [42] | 2013 | Zirconia | Prosp. | 7 | 99 | 26–76 | 49.4 | University |
| Haff et al. [43] | 2015 | Zirconia | Retrosp. | 13 | 33 | 35–87 | 68 ± 11 | Specialists and private practice |
| Ioannidis et al. [44] | 2016 | Zirconia | Prosp. | 10 | 57 | n.r. | 52.6 ± 10.1 | University |
| Nicolaisen et al. [45] | 2016 | Zirconia, high-noble metal | RCT | 3 | 34 | 36–66 | 51 | University |
| Sailer et al. [46] | 2018 | Zirconia, high-noble metal | RCT | 10 | 53 | 36.5–86.9 | 60.9 | University |
| Suarez et al. [47] | 2019 | Zirconia, Co-Cr metal | RCT | 5 | 40 | 24–70 | n.r. | University |
| Koenig et al. [48] | 2019 | Zirconia | Prosp. | 3 | 10 | n.r. | 54.34 | University |
| Brandt et al. [49] | 2019 | Zirconia, lithium disilicate | Retrosp. | 5 | 136 | 30–70 | 57.84 | Specialists and private practice |
| Forrer et al. [50] | 2020 | Zirconia, high-noble metal | Prosp. | 5 | 83 | n.r. | n.r. | University |
| Study | Year | Total No. of FPDs | Mean Follow-Up Time | No. of Failures | Estimated Annual Failures | Estimated Survival in % after (N) = Years |
|---|---|---|---|---|---|---|
| Metal-ceramic | ||||||
| Chirstensen et al. [37] | 2010 | 69 | n.r. | 0 | 1.6 | (3) 95% |
| Nicolaisen et al. [45] | 2016 | 17 | n.r. | 0 | 0 | (3) 100% |
| Sailer et al. [46] | 2018 | 24 | 10.0 | 1 | 0 | (10) 100% |
| Suarez et al. [47] | 2019 | 20 | 5.25 ± 0.2 | 0 | 0 | (5) 100% |
| Forrer et al. [50] | 2020 | 30 | 6.44 ± 1.14 | 1 | 0.72 | (5) 96.4% |
| Reinforced glass-ceramic | ||||||
| Makarouna et al. [38] | 2011 | 18 | 4.7 | 6 | 7.14 | (5) 70% |
| Kem et al. [39] | 2012 | 36 | 10.1 | 4 | 1.10 | (5) 94.6% |
| Sola-Ruiz et al. [40] | 2013 | 21 | 10.0 | 6 | 2.86 | (5) 86.7% |
| Brandt et al. [49] | 2019 | 136 | 3.10 ± 1.5 | 8 | 0.93 | (5) 9.35% |
| Glass-infiltrated alumina | ||||||
| Christensen et al. [37] | 2010 | 34 | n.r. | 11 | 10.6 | (3) 68% |
| Zirconia | ||||||
| Christensen et al. [37] | 2010 | 163 | n.r. | 2 | 4.66 | (3) 86% |
| Koenig et al. [41] | 2013 | 30 | 3.96 ± 2.7 | 1 | 2.04 | (9) 81.6% |
| Rinke at al. [42] | 2013 | 99 | 6.3 | 19 | 3.03 | (5) 85.9% |
| Haff et al. [43] | 2015 | 33 | 9.6 ± 1.6 | 2 | 0.6 | (10) 94% |
| Ioannidis et al. [44] | 2016 | 57 | 6.3 ± 1.9 | 3 | 1.5 | (10) 85% |
| Nicolaisen et al. [45] | 2016 | 17 | n.r. | 0 | 0 | (3) 100% |
| Sailer et al. [46] | 2018 | 29 | 10.3 | 5 | 0.87 | (10) 91.3% |
| Saurez et al. [47] | 2019 | 20 | 5.25 ± 0.2 | 0 | 0 | (5) 100% |
| Koenig et al. [48] | 2019 | 10 | n.r. | 1 | 0 | (3) 100% |
| Forrer et al. [50] | 2020 | 53 | 6.44 ± 1.14 | 2 | 0.42 | (5) 97.9% |
| FPD Type | Total Number of FPDs | Total Number of Abutments Affected Due to: | |||
|---|---|---|---|---|---|
| a. Secondary Caries | b. Periodontal Disease | c. Loss of Vitality | d. Abutment Fracture | ||
| All FPDs | 916 | 26 | 9 | 19 | 9 |
| MC-FPDS | 160 | 3 | 3 | 1 | 0 |
| AC-FPDs | 756 | 23 | 6 | 18 | 9 |
| a. Densely sintered Zirconia | 511 | 20 | 5 | 15 | 7 |
| b. Reinforced Glass Ceramic | 211 | 3 | 1 | 3 | 2 |
| c. Alumina | 34 | 0 | 0 | 0 | 0 |
| Items | Total Number of FPDs | Framework or Core Fractures | Chipping | Ceramic Fractures | Loss of Retention |
|---|---|---|---|---|---|
| All FPDs | 916 | 32 | 194 | 62 | 21 |
| MC-FP Ds | 160 | 0 | 30 | 4 | 3 |
| AC-FPDs | 756 | 32 | 164 | 58 | 19 |
| a. Zirconia | 511 | 16 | 141 | 51 | 15 |
| b. Reinforced Glass Ceramic | 211 | 5 | 6 | 6 | 4 |
| c. Alumina | 34 | 11 | 17 | 1 | 0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ispas, A.; Iosif, L.; Popa, D.; Negucioiu, M.; Constantiniuc, M.; Bacali, C.; Buduru, S. Comparative Assessment of the Functional Parameters for Metal-Ceramic and All-Ceramic Teeth Restorations in Prosthetic Dentistry—A Literature Review. Biology 2022, 11, 556. https://doi.org/10.3390/biology11040556
Ispas A, Iosif L, Popa D, Negucioiu M, Constantiniuc M, Bacali C, Buduru S. Comparative Assessment of the Functional Parameters for Metal-Ceramic and All-Ceramic Teeth Restorations in Prosthetic Dentistry—A Literature Review. Biology. 2022; 11(4):556. https://doi.org/10.3390/biology11040556
Chicago/Turabian StyleIspas, Ana, Laura Iosif, Daniela Popa, Marius Negucioiu, Mariana Constantiniuc, Cecilia Bacali, and Smaranda Buduru. 2022. "Comparative Assessment of the Functional Parameters for Metal-Ceramic and All-Ceramic Teeth Restorations in Prosthetic Dentistry—A Literature Review" Biology 11, no. 4: 556. https://doi.org/10.3390/biology11040556