
The Effects of EMMPRIN/CD147 on Late Function and Histopathological Lesions of the Renal Graft

 , ,
, ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Patients and Methods
2.1. Patients
2.2. Methods
2.3. Statistical Analysis
3. Results
4. Discussion
4.1. EMMPRIN/CD147
4.2. CD147/AKI
4.3. CKD/EMT
4.4. EMT/CD147/EMMPRIN
4.5. Future Perspectives
5. Conclusions
6. Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zhou, D.; Liu, Y. Renal Fibrosis in 2015: Understanding the Mechanisms of Kidney Fibrosis. Nat. Rev. Nephrol. 2016, 12, 68–70. [Google Scholar] [CrossRef] [PubMed]
- Sun, Y.B.Y.; Qu, X.; Caruana, G.; Li, J. The Origin of Renal Fibroblasts/Myofibroblasts and the Signals That Trigger Fibrosis. Differentiation 2016, 92, 102–107. [Google Scholar] [CrossRef] [PubMed]
- Grass, G.D.; Toole, B.P. How, with Whom and When: An Overview of CD147-Mediated Regulatory Networks Influencing Matrix Metalloproteinase Activity. Biosci. Rep. 2016, 36, e00283. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, Y. New Insights into Epithelial-Mesenchymal Transition in Kidney Fibrosis. J. Am. Soc. Nephrol. 2010, 21, 212–222. [Google Scholar] [CrossRef] [Green Version]
- Sheng, L.; Zhuang, S. New Insights Into the Role and Mechanism of Partial Epithelial-Mesenchymal Transition in Kidney Fibrosis. Front. Physiol. 2020, 11, 569322. [Google Scholar] [CrossRef]
- Kemmner, S.; Schulte, C.; Hann von Weyhern, C.; Schmidt, R.; Baumann, M.; Heemann, U.; Renders, L.; Schmaderer, C. EMMPRIN Expression Is Involved in the Development of Interstitial Fibrosis and Tubular Atrophy in Human Kidney Allografts. Clin. Transplant. 2016, 30, 218–225. [Google Scholar] [CrossRef]
- Earley, A.; Miskulin, D.; Lamb, E.J.; Levey, A.S.; Uhlig, K. Estimating Equations for Glomerular Filtration Rate in the Era of Creatinine Standardization: A Systematic Review. Ann. Intern. Med. 2012, 156, 785–795. [Google Scholar] [CrossRef]
- Rognant, N.; Lemoine, S.; Laville, M.; Hadj-Aïssa, A.; Dubourg, L. Performance of the Chronic Kidney Disease Epidemiology Collaboration Equation to Estimate Glomerular Filtration Rate in Diabetic Patients. Diabetes Care 2011, 34, 1320–1322. [Google Scholar] [CrossRef] [Green Version]
- Schwandt, A.; Denkinger, M.; Fasching, P.; Pfeifer, M.; Wagner, C.; Weiland, J.; Zeyfang, A.; Holl, R.W. Comparison of MDRD, CKD-EPI, and Cockcroft-Gault Equation in Relation to Measured Glomerular Filtration Rate among a Large Cohort with Diabetes. J. Diabetes Complicat. 2017, 31, 1376–1383. [Google Scholar] [CrossRef]
- Guindolet, D.; Gabison, E.E. Role of CD147 (EMMPRIN/Basigin) in Tissue Remodeling. Anat. Rec. 2020, 303, 1584–1589. [Google Scholar] [CrossRef]
- Ryzhakova, O.S.; Solov’eva, N.I. Matrix Metalloproteinases (MMP)–MMP-1,-2,-9 and Its Endogenous Activity Regulators in Transformed by E7 Oncogene HPV16 and HPV18 Cervical Carcinoma Cell Lines. Biomeditsinskaya Khimiya 2013, 59, 530–540. [Google Scholar] [CrossRef] [Green Version]
- Kato, N.; Yuzawa, Y.; Kosugi, T.; Hobo, A.; Sato, W.; Miwa, Y.; Sakamoto, K.; Matsuo, S.; Kadomatsu, K. The E-Selectin Ligand Basigin/CD147 Is Responsible for Neutrophil Recruitment in Renal Ischemia/Reperfusion. J. Am. Soc. Nephrol. 2009, 20, 1565–1576. [Google Scholar] [CrossRef] [Green Version]
- Seizer, P.; Ochmann, C.; Schönberger, T.; Zach, S.; Rose, M.; Borst, O.; Klingel, K.; Kandolf, R.; MacDonald, H.R.; Nowak, R.A.; et al. Disrupting the EMMPRIN (CD147)-Cyclophilin a Interaction Reduces Infarct Size and Preserves Systolic Function after Myocardial Ischemia and Reperfusion. Arterioscler. Thromb. Vasc. Biol. 2011, 31, 1377–1386. [Google Scholar] [CrossRef] [Green Version]
- Kosugi, T.; Maeda, K.; Sato, W.; Maruyama, S.; Kadomatsu, K. CD147 (EMMPRIN/Basigin) in Kidney Diseases: From an Inflammation and Immune System Viewpoint. Nephrol. Dial. Transplant. 2015, 30, 1097–1103. [Google Scholar] [CrossRef] [Green Version]
- Nagaya, H.; Kosugi, T.; Maeda-Hori, M.; Maeda, K.; Sato, Y.; Kojima, H.; Hayashi, H.; Kato, N.; Ishimoto, T.; Sato, W.; et al. CD147/Basigin Reflects Renal Dysfunction in Patients with Acute Kidney Injury. Clin. Exp. Nephrol. 2014, 18, 746–754. [Google Scholar] [CrossRef]
- Mannon, R.B. Delayed Graft Function: The AKI of Kidney Transplantation. Nephron 2018, 140, 94–98. [Google Scholar] [CrossRef]
- Cruz-Solbes, A.S.; Youker, K. Epithelial to Mesenchymal Transition (EMT) and Endothelial to Mesenchymal Transition (EndMT): Role and Implications in Kidney Fibrosis. In Kidney Development and Disease; Results and Problems in Cell Differentiation book series 60; Springer: Cham, Switzerland, 2017; pp. 345–372. [Google Scholar] [CrossRef]
- Arora, K.; Gwinn, W.M.; Bower, M.A.; Watson, A.; Okwumabua, I.; MacDonald, H.R.; Bukrinsky, M.I.; Constant, S.L. Extracellular Cyclophilins Contribute to the Regulation of Inflammatory Responses. J. Immunol. 2005, 175, 517–522. [Google Scholar] [CrossRef] [Green Version]
- Lange-Sperandio, B.; Cachat, F.; Thornhill, B.A.; Chevalier, R.L. Selectins Mediate Macrophage Infiltration in Obstructive Nephropathy in Newborn Mice. Kidney Int. 2002, 61, 516–524. [Google Scholar] [CrossRef] [Green Version]
- Mori, Y.; Masuda, T.; Kosugi, T.; Yoshioka, T.; Hori, M.; Nagaya, H.; Maeda, K.; Sato, Y.; Kojima, H.; Kato, N.; et al. The Clinical Relevance of Plasma CD147/Basigin in Biopsy-Proven Kidney Diseases. Clin. Exp. Nephrol. 2018, 22, 815–824. [Google Scholar] [CrossRef]
- Wu, J.; Ru, N.Y.; Zhang, Y.; Li, Y.; Wei, D.; Ren, Z.; Huang, X.F.; Chen, Z.N.; Bian, H. HAb18G/CD147 Promotes Epithelial-Mesenchymal Transition through TGF-β Signaling and Is Transcriptionally Regulated by Slug. Oncogene 2011, 30, 4410–4427. [Google Scholar] [CrossRef]
- Guillot, S.; Delaval, P.; Brinchault, G.; Caulet-Maugendre, S.; Depince, A.; Lena, H.; Delatour, B.; Lagente, V.; Martin-Chouly, C. Increased Extracellular Matrix Metalloproteinase Inducer (EMMPRIN) Expression in Pulmonary Fibrosis. Exp. Lung Res. 2006, 32, 81–97. [Google Scholar] [CrossRef]
- Sun, S.; Zhao, A.; Li, R.; Du, R.; He, L.; Sun, W.; Wang, H.; Huang, C. CD147 Renal Expression as a Biomarker for Progressive IgAN. J. Nephrol. 2015, 28, 307–314. [Google Scholar] [CrossRef]
- Qu, X.; Wang, C.; Zhang, J.; Qie, G.; Zhou, J. The Roles of CD147 and/or Cyclophilin a in Kidney Diseases. Mediat. Inflamm. 2014, 2014, 728673. [Google Scholar] [CrossRef]
- Zakiyanov, O.; Kalousová, M.; Zima, T.; Tesař, V. Matrix Metalloproteinases in Renal Diseases: A Critical Appraisal. Kidney Blood Press. Res. 2019, 44, 298–330. [Google Scholar] [CrossRef]
- Roufosse, C.; Simmonds, N.; Clahsen-Van Groningen, M.; Haas, M.; Henriksen, K.J.; Horsfield, C.; Loupy, A.; Mengel, M.; Perkowska-Ptasińska, A.; Rabant, M.; et al. A 2018 Reference Guide to the Banff Classification of Renal Allograft Pathology. Transplantation 2018, 102, 1795–1814. [Google Scholar] [CrossRef]
- Webster, A.C.; Nagler, E.V.; Morton, R.L.; Masson, P. Chronic Kidney Disease. Lancet 2017, 389, 1238–1252. [Google Scholar] [CrossRef]
- Zhong, J.; Yang, H.C.; Fogo, A.B. A Perspective on Chronic Kidney Disease Progression. Am. J. Physiol. Ren. Physiol. 2017, 312, F375–F384. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Naesens, M.; Lerut, E.; Emonds, M.P.; Herelixka, A.; Evenepoel, P.; Claes, K.; Bammens, B.; Sprangers, B.; Meijers, B.; Jochmans, I.; et al. Proteinuria as a Noninvasive Marker for Renal Allograft Histology and Failure: An Observational Cohort Study. J. Am. Soc. Nephrol. 2016, 27, 281–292. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yoshioka, T.; Kosugi, T.; Masuda, T.; Watanabe, T.; Ryuge, A.; Nagaya, H.; Maeda, K.; Sato, Y.; Katsuno, T.; Kato, N.; et al. CD147/Basigin Deficiency Prevents the Development of Podocyte Injury through FAK Signaling. Am. J. Pathol. 2019, 189, 1338–1350. [Google Scholar] [CrossRef] [PubMed]
- Ntrinias, T.; Papasotiriou, M.; Balta, L.; Kalavrizioti, D.; Vamvakas, S.; Papachristou, E.; Goumenos, D.S. Biomarkers in Progressive Chronic Kidney Disease. Still a Long Way to Go. Prilozi 2019, 40, 27–39. [Google Scholar] [CrossRef] [Green Version]
- Kwiatkowska, E.; Domanski, L.; Bober, J.; Safranow, K.; Romanowski, M.; Pawlik, A.; Kwiatkowski, S.; Ciechanowski, K. Urinary Metalloproteinases-9 and -2 and Their Inhibitors TIMP-1 and TIMP-2 Are Markers of Early and Long-Term Graft Function after Renal Transplantation. Kidney Blood Press. Res. 2016, 41, 288–297. [Google Scholar] [CrossRef]
- Hörstrup, J.H.; Gehrmann, M.; Schneider, B.; Plöger, A.; Froese, P.; Schirop, T.; Kampf, D.; Frei, U.; Neumann, R.; Eckardt, K.U. Elevation of Serum and Urine Levels of TIMP-1 and Tenascin in Patients with Renal Disease. Nephrol. Dial. Transplant. 2002, 17, 1005–1013. [Google Scholar] [CrossRef] [Green Version]
- Musiał, K.; Zwolińska, D. Matrix Metalloproteinases (MMP-2,9) and Their Tissue Inhibitors (TIMP-1,2) as Novel Markers of Stress Response and Atherogenesis in Children with Chronic Kidney Disease (CKD) on Conservative Treatment. Cell Stress Chaperones 2011, 16, 97–103. [Google Scholar] [CrossRef] [Green Version]
- Mansour, S.G.; Puthumana, J.; Coca, S.G.; Gentry, M.; Parikh, C.R. Biomarkers for the Detection of Renal Fibrosis and Prediction of Renal Outcomes: A Systematic Review. BMC Nephrol. 2017, 18, 72. [Google Scholar] [CrossRef] [Green Version]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Banff Lesion | Abbreviation | 0 | 1 | 2 | 3 |
|---|---|---|---|---|---|
| Interstitial inflammation | I | <10% | 10–25% | 26–50% | >50% |
| Tubulitis | T | none | 1–4/tubular cross section or 10 tubular epithelial cells | 5–10 | >10 or foci of tubular basement membrane destruction with i ≥ 2 and t2 elsewhere |
| Glomerulitis | G | none | <25% | 25–75% | >75% |
| Peritubular capillaritis | PTC | <3 leukocytes/PTC | ≥1 leukocyte in ≥10% of PTCs with max. of 3–4/PTCS | ≥1 leukocyte in ≥10% of PTCs with max. of 5–10/PTCS | ≥1 leukocyte in ≥10% of PTCs with max. of >10/PTCS |
| C4d | C4d | none | <10% | 10–50% | >50% |
| Interstitial fibrosis | CI | ≤5% | 6–25% | 26–50% | >50% |
| Tubular atrophy | CT | none | ≤25% | 26–50% | >50% |
| Vascular fibrous Intimal thickening | CV | none | ≤25% | 26–50% | >50% |
| double contours of GBM | CG | none | 1 a: only by EM 1 b: ≤25% by LM | 26–50% | >50% |
| Mesangial matrix expansion | MM | none | ≤25% | 26–50% | >50% |
| Arteriolar hyalinosis | AA | none | Mild to moderate ≥1 | Moderate to severe in >1 | Severe in many |
| Hyaline arteriolar thickening | AAH | none | 1 without circumferential | ≥1 without circumferential | Severe in many circumferenial |
| N | ME | MIN | MAX | MEAN | SD | |
|---|---|---|---|---|---|---|
| Time from Tx (months) | 49 | 69 | 12 | 182 | 75.7 | 52.3 |
| Recipient age (years) | 49 | 42 | 24 | 71 | 45.7 | 13.6 |
| BMI at Tx | 49 | 23.8 | 16.1 | 34.8 | 24.4 | 4 |
| BMI at last appointment | 49 | 25.4 | 18.1 | 34 | 25.9 | 4.3 |
| eGFR at last appointment (mL/min/1.73 m2) | 49 | 36 | 15 | 89 | 38.6 | 19.1 |
| Urine protein (mg/dL) | 49 | 0 | 0 | 865.7 | 78.7 | 165 |
| Duration of dialysis prior to Tx (months) | 49 | 15 | 0 | 102 | 23.9 | 23.8 |
| CIT (min) | 49 | 1260 | 72 | 2100 | 1116.7 | 555 |
| PRA(%) | 49 | 3 | 0 | 56 | 8 | 15.9 |
| ZENITH eGFR (mL/min/1.73 m2) | 49 | 31.0 | 98.0 | 118.0 | 58 | 17 |
| eGFR at 1 year (mL/min/1.73 m2) | 49 | 45 | 9 | 96.0 | 47.7 | 17.9 |
| eGFR at 2 years (mL/min/1.73 m2) | 48 | 49 | 15 | 85 | 48 | 17.1 |
| eGFR at 3 years (mL/min/1.73 m2) | 43 | 47 | 17 | 87 | 47.3 | 15.4 |
| eGFR at 4 years (mL/min/1.73 m2) | 38 | 46 | 19 | 98 | 48 | 18.9 |
| eGFR at 5 years (mL/min/1.73 m2) | 35 | 41 | 17 | 109 | 45.5 | 20.1 |
| eGFR at 10 years (mL/min/1.73 m2) | 13 | 44 | 23 | 82 | 47.8 | 18.7 |
| EMMPRIN (pg/mL) | 49 | 6623.2 | 643.36 | 59,861.6 | 9419.67 | 9678.712 |
| sex | 49 (23 W,26 M) |
| Group without Chronic Changes N = 23 | Group with Chronic Changes N = 26 | ||||||
|---|---|---|---|---|---|---|---|
| ME | MIN | MAX | ME | MIN | MAX | p | |
| Time from Tx (months) | 44.9 | 3.16 | 162.1 | 82.7 | 9.53 | 181 | 0.004 |
| Recipient age (years) | 43 | 24 | 71 | 40,5 | 26 | 70 | NS |
| BMI at last appointment (kg/m2) | 26.2 | 18.7 | 33.7 | 24.4 | 18.1 | 34 | NS |
| eGFR at last appointment (mL/min/1.73 m2) | 41.9 | 6.1 | 88.9 | 33.7 | 6.02 | 71.62 | NS |
| ZENITH eGFR (mL/min/1.73 m2) | 64 | 34.17 | 92.38 | 53.85 | 31.1 | 97.76 | 0.03 |
| G | 0 | 0 | 2 | 0 | 0 | 0 | NS |
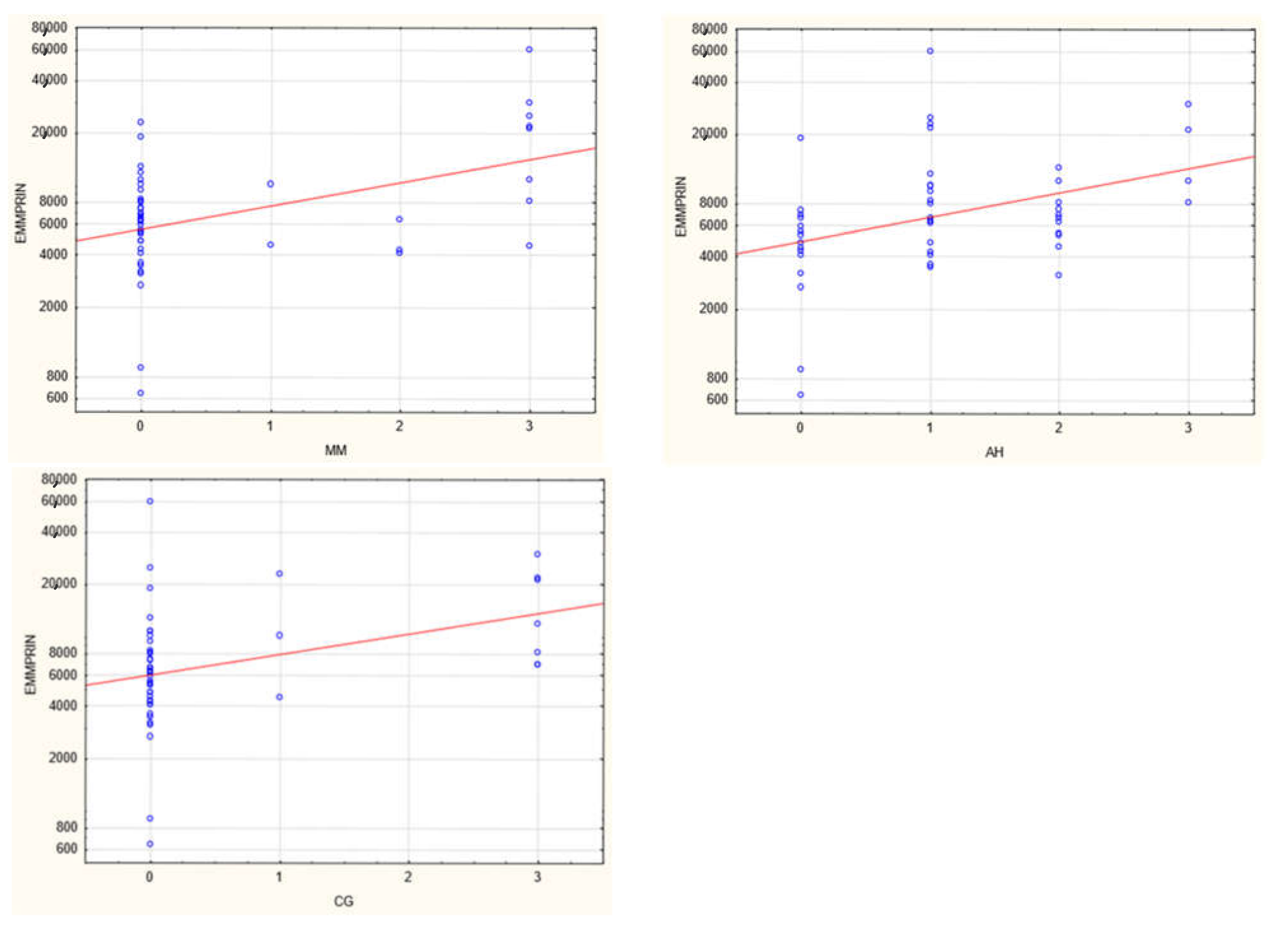
| CG | 0 | 0 | 3 | 0 | 0 | 3 | NS |
| MM | 0 | 0 | 3 | 0 | 0 | 3 | 0.013 |
| I | 0 | 0 | 3 | 1 | 0 | 3 | 0.007 |
| T | 0 | 0 | 2 | 0 | 0 | 3 | NS |
| PTC | 0 | 0 | 10 | 0 | 0 | 3 | NS |
| CV | 0 | 0 | 3 | 0 | 0 | 2 | NS |
| AH | 1 | 0 | 3 | 1 | 0 | 3 | 0.027 |
| CI | 0 | 0 | 1 | 2 | 0 | 3 | 3.32 × 10−6 |
| CT | 1 | 0 | 1 | 2 | 0 | 3 | 4.06 × 10−8 |
| DGF Positive | DGF Negative | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| ME | MIN | MAX | MEAN | SD | ME | MIN | MAX | MEAN | SD | p | |
| EMMPRIN(pg/mL) | 7729.9 | 643.4 | 29,709.47 | 11,658.36 | 8370.301 | 5348.1 | 897.4 | 59,861.6 | 8047.789 | 10,064.92 | 0.00896 |
| N | 16 | 33 | |||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nalewajska, M.; Opara-Bajerowicz, M.; Safranow, K.; Pawlik, A.; Ciechanowski, K.; Kwiatkowski, S.; Kwiatkowska, E. The Effects of EMMPRIN/CD147 on Late Function and Histopathological Lesions of the Renal Graft. Biology 2022, 11, 232. https://doi.org/10.3390/biology11020232
Nalewajska M, Opara-Bajerowicz M, Safranow K, Pawlik A, Ciechanowski K, Kwiatkowski S, Kwiatkowska E. The Effects of EMMPRIN/CD147 on Late Function and Histopathological Lesions of the Renal Graft. Biology. 2022; 11(2):232. https://doi.org/10.3390/biology11020232
Chicago/Turabian StyleNalewajska, Magdalena, Martyna Opara-Bajerowicz, Krzysztof Safranow, Andrzej Pawlik, Kazimierz Ciechanowski, Sebastian Kwiatkowski, and Ewa Kwiatkowska. 2022. "The Effects of EMMPRIN/CD147 on Late Function and Histopathological Lesions of the Renal Graft" Biology 11, no. 2: 232. https://doi.org/10.3390/biology11020232