




Rat Model of Quadriceps Contracture by Joint Immobilization

Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Animals
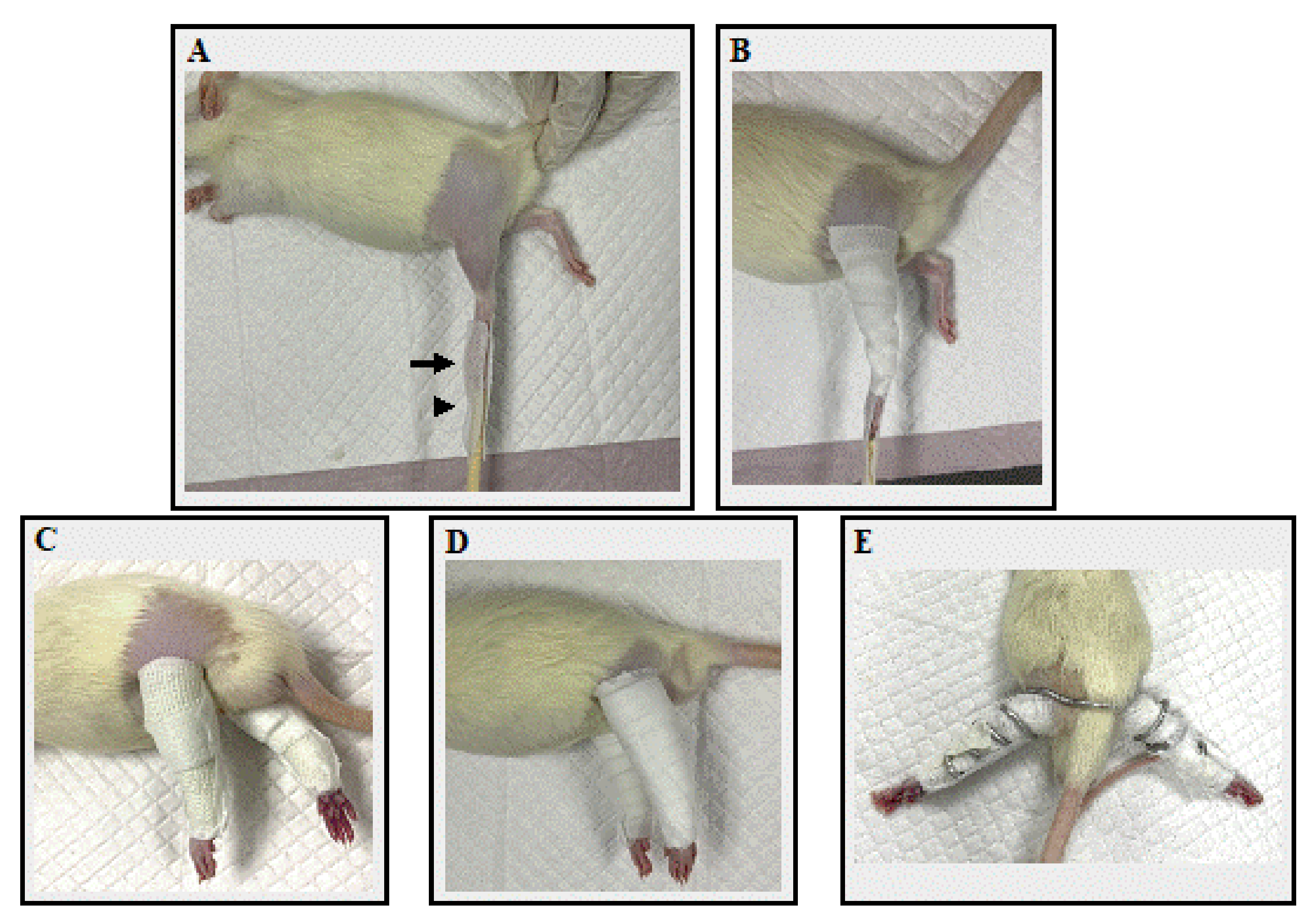
2.2. Immobilization Procedures
2.3. Body Weight and Food Intake
2.4. Measuring Joint Angles and Range of Motion
2.5. Muscle Collection and Measurement
2.6. Histopathological Examination
2.7. Statistical Analysis
3. Results
3.1. Bodyweight
3.2. Food Intake
3.3. Bandage Application Time, the Number of Rewindings, and Adverse Effects
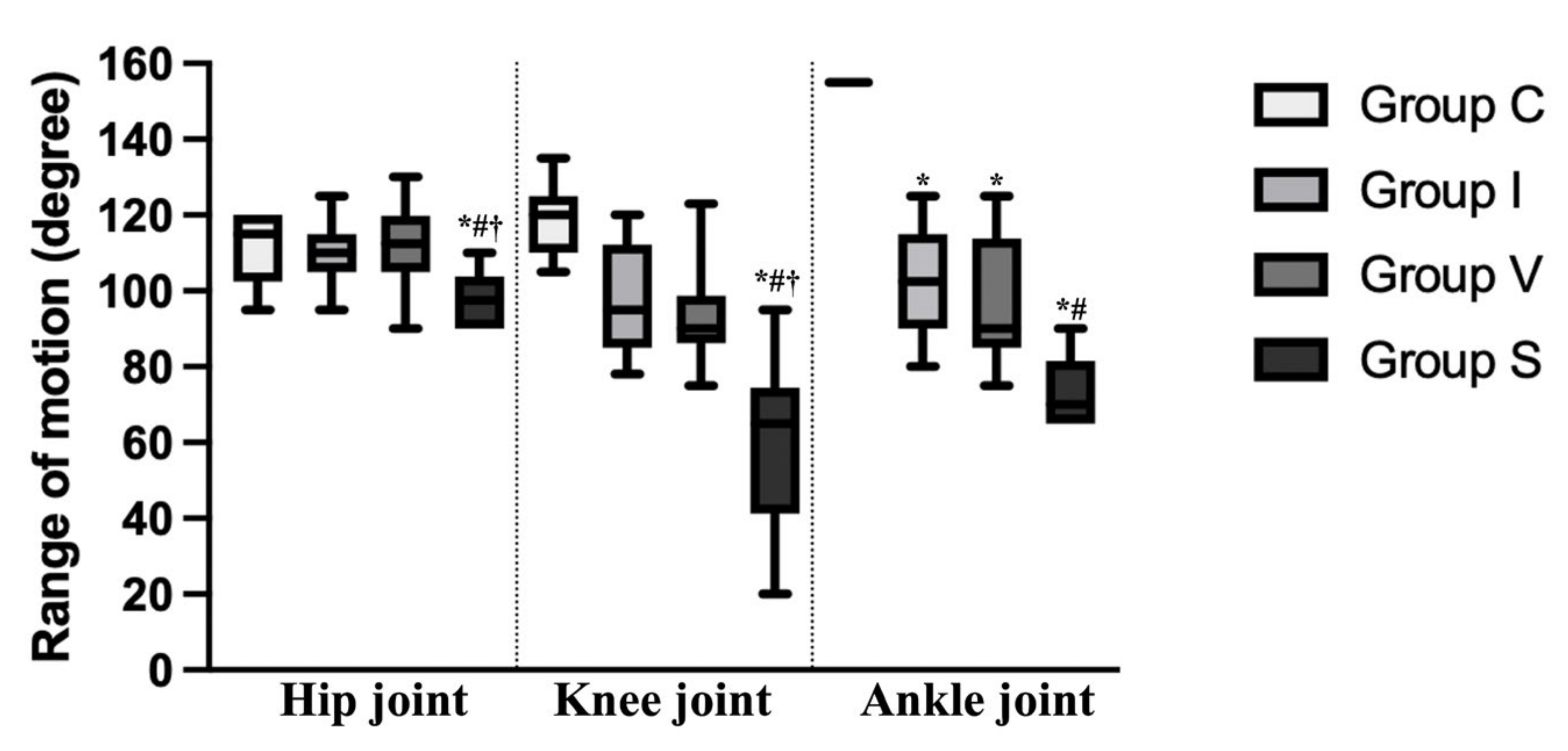
3.4. Joint Angle and Range of Motion
3.5. Muscle Weight and Measurement of Quadriceps
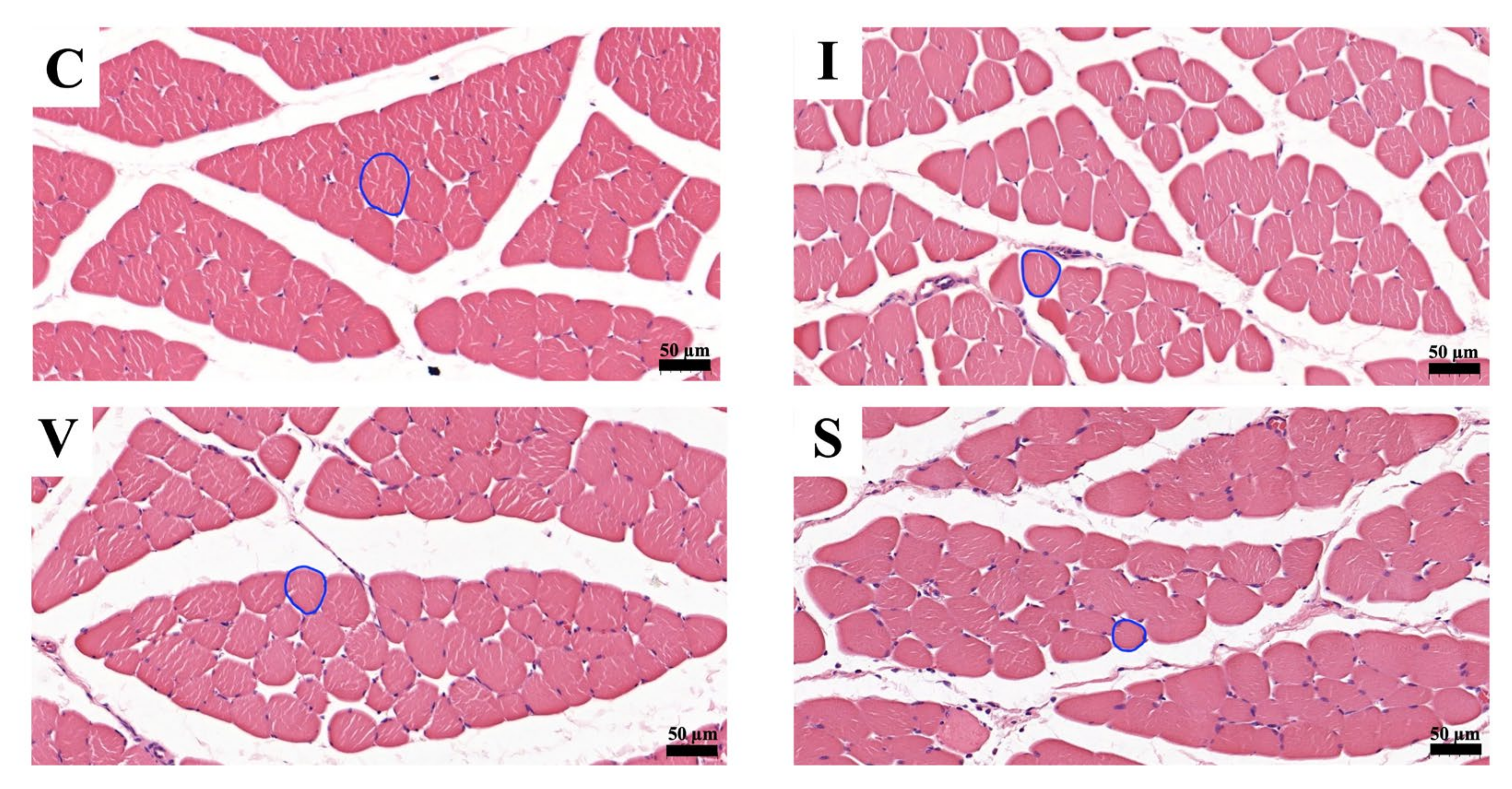
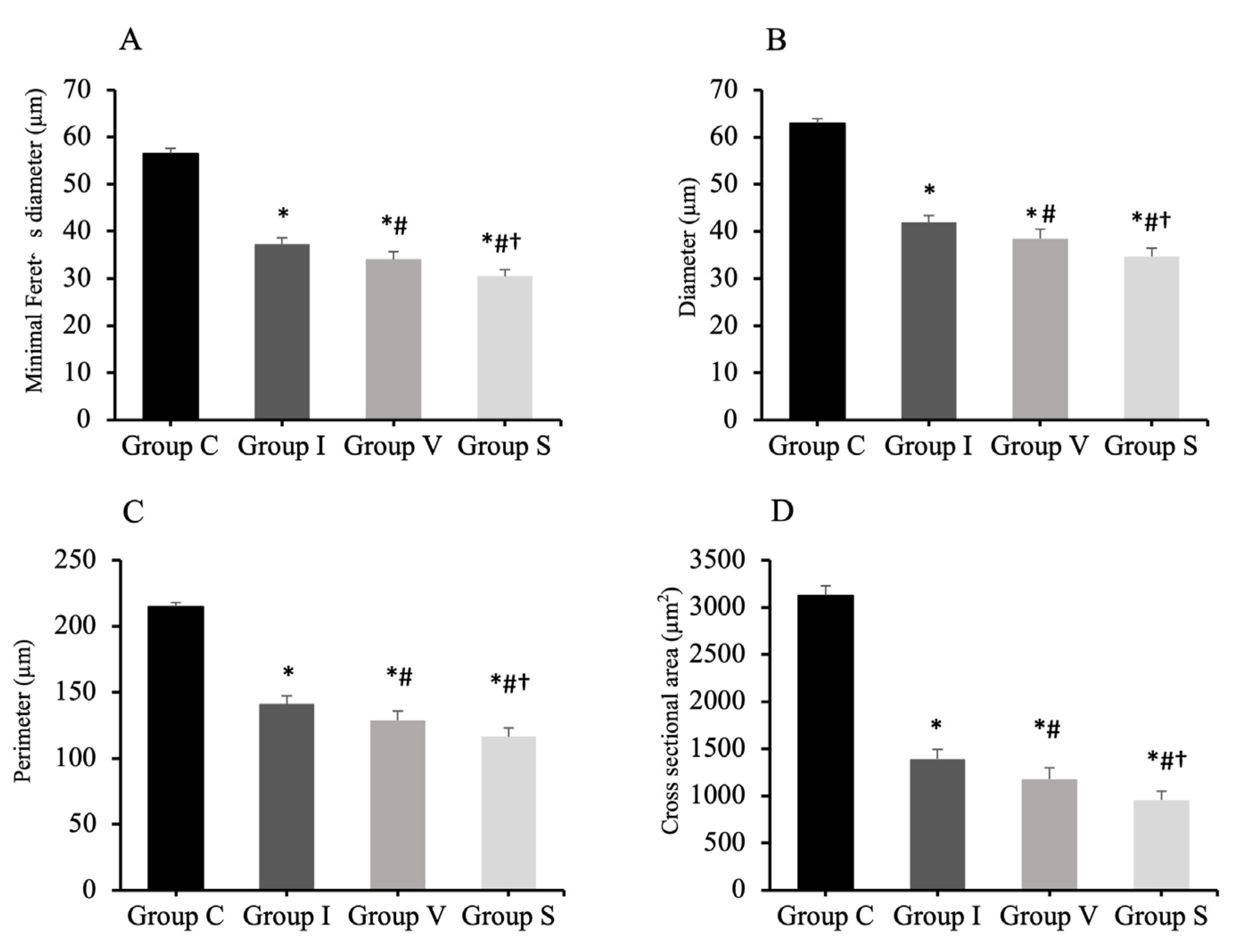
3.6. Morphological Evaluation of Quadriceps Muscle Fiber
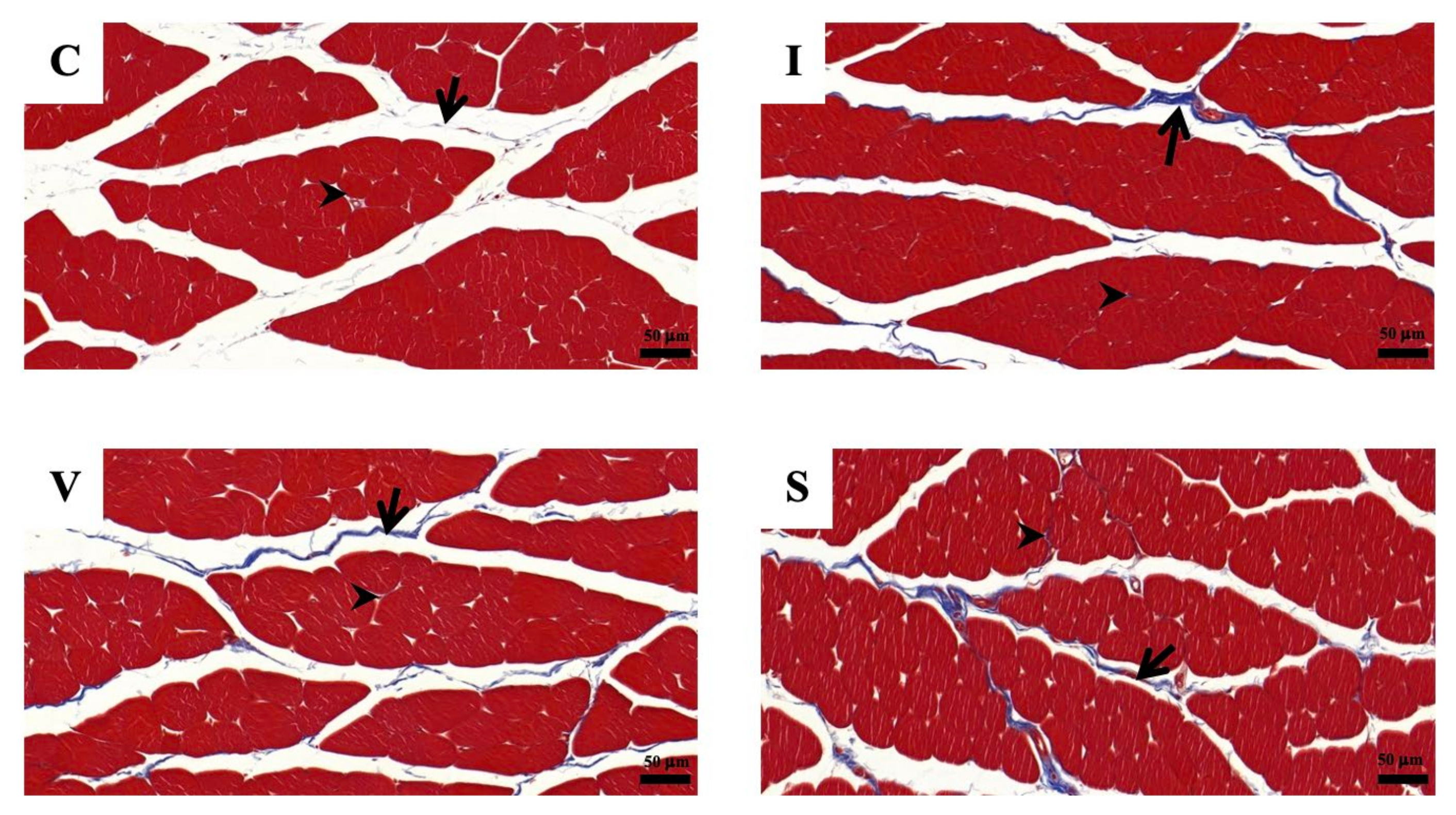
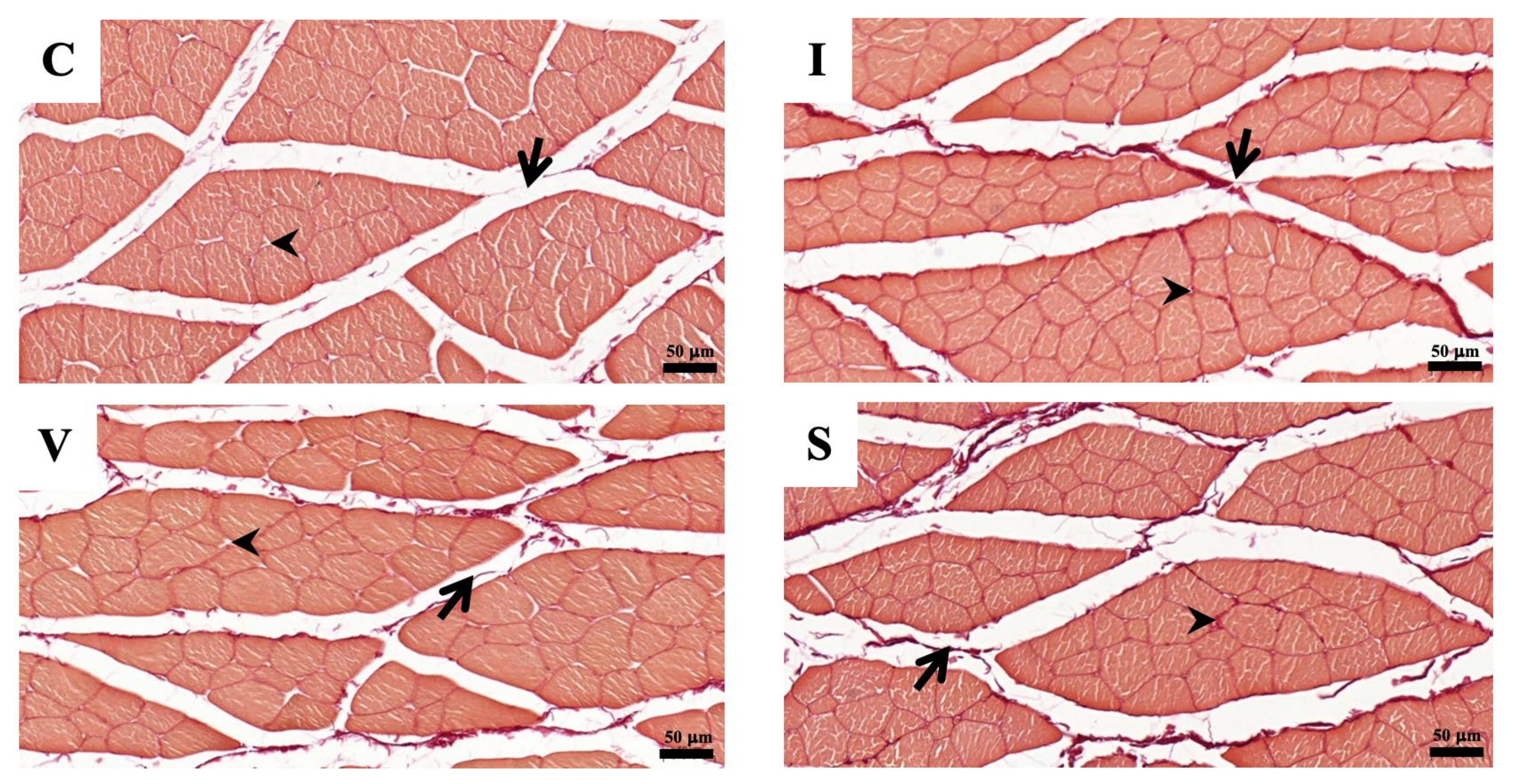
3.7. Assessment of Quadriceps Muscle Fibrosis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Canapp, S.O.; Saunders, D.G. Common conditions and physical rehabilitation of the athletic patient. In Canine Rehabilitation and Physical Therapy, 2nd ed.; Millis, D., Levine, D., Eds.; W.B. Saunders: St. Louis, MO, USA, 2014; pp. 582–608. [Google Scholar]
- Bonnie, F.F.; Frucht, S.S. Musculoskeletal system. In Medical Terminology a Living Language, 7th ed.; Pearson: New York, NY, USA, 2019; pp. 89–119. [Google Scholar]
- Lieber, R.L.; Fridén, J. Muscle contracture and passive mechanics in cerebral palsy. J. Appl. Physiol. 2019, 126, 1492–1501. [Google Scholar] [CrossRef] [PubMed]
- Ebnezar, J. Regional conditions of the lower limb. In Textbook of Orthopedics, 4th ed.; Jaypee Brothers Medical India: New Delhi, India, 2010; pp. 409–451. [Google Scholar]
- Crenshaw, A.H. Soft-tissue procedures and corrective osteotomies about the knee. In Campbell’s Operative Orthopaedics, 13th ed.; Azar, F.M., Beaty, J.H., Canale, S.T., Eds.; Elsevier: North York, ON, Canada, 2017; pp. 477–506. [Google Scholar]
- Özdemir, O.; Atalay, A.; Çeliker, R.; Kerimoğlu, Ü.; Özdemir, Ö. Congenital contracture of the quadriceps muscle: Confirming the diagnosis with magnetic resonance imaging. Jt. Bone Spine 2006, 73, 554–556. [Google Scholar] [CrossRef] [PubMed]
- Guo, R.; Xiang, X.; Qiu, L. Shear-wave elastography assessment of gluteal muscle contracture: Three case reports. Medicine 2018, 97, e13071. [Google Scholar] [CrossRef] [PubMed]
- Babhulkar, S.S. Triceps contracture caused by injections. A report of 11 cases. J. Bone Jt. Surg. Br. 1985, 67, 94–96. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Banerji, D.; De, C.; Pal, A.K.; Das, S.K.; Ghosh, S.; Dharmadevan, S. Deltoid contracture: A study of nineteen cases. Indian J Orthop. 2008, 42, 188–191. [Google Scholar] [CrossRef]
- Hagen, R. Contracture of the quadriceps muscle in children: A report of 12 cases. Acta Orthop. 1968, 39, 565–578. [Google Scholar] [CrossRef]
- Gunn, D. Contracture of the quadriceps muscle. J. Bone Joint Surg. 1964, 46, 492–497. [Google Scholar] [CrossRef] [Green Version]
- Cross, N.; McWay, D. Musculoskeletal system. In Stanfield’s Essential Medical Terminology, 5th ed.; Jones & Bartlett Learning: Burlington, MA, USA, 2020; pp. 271–298. [Google Scholar]
- Trudel, G.; Uhthoff, H.K. Contractures secondary to immobility: Is the restriction articular or muscular? An experimental longitudinal study in the rat knee. Arch. Phys. Med. Rehabil. 2000, 81, 6–13. [Google Scholar] [CrossRef]
- Chimoto, E.; Hagiwara, Y.; Ando, A.; Itoi, E. Progression of an arthrogenic motion restriction after immobilization in a rat experimental knee model. Upsala J. Med. Sci. 2007, 112, 347–355. [Google Scholar] [CrossRef]
- Trudel, G.; Laneuville, O.; Coletta, E.; Goudreau, L.; Uhthoff, H.K. Quantitative and temporal differential recovery of articular and muscular limitations of knee joint contractures; results in a rat model. J. Appl. Physiol. 2014, 117, 730–737. [Google Scholar] [CrossRef]
- Milcan, A.; Eskandari, M.M.; Öztuna, V.; Çolak, M.; Kuyurtar, F. Injection-induced contracture of the quadriceps femoris muscle in children. Orthopedics 2004, 27, 65–66. [Google Scholar] [CrossRef]
- Muteti, E.; Theuri, J.; Mead, T.; Gokcen, E. Results of surgical treatment of quadriceps femoris/contracture in children. East Afr. Orthop. J. 2009, 3, 69–72. [Google Scholar] [CrossRef]
- Wang, F.; Zhang, Q.B.; Zhou, Y.; Chen, S.; Huang, P.P.; Liu, Y.; Xu, Y.H. The mechanisms and treatments of muscular pathological changes in immobilization-induced joint contracture: A literature review. Chin. J. Traumatol. 2019, 22, 93–98. [Google Scholar] [CrossRef]
- Herbert, R.D.; Balnave, R.J. The effect of position of immobilisation on resting length, resting stiffness, and weight of the soleus muscle of the rabbit. J. Orthop. Res. 1993, 11, 358–366. [Google Scholar] [CrossRef] [PubMed]
- Okita, M.; Yoshimura, T.; Nakano, J.; Motomura, M.; Eguchi, K. Effects of reduced joint mobility on sarcomere length, collagen fibril arrangement in the endomysium, and hyaluronan in rat soleus muscle. J. Muscle Res. Cell Motil. 2004, 25, 159–166. [Google Scholar] [CrossRef]
- Shires, P.; Braund, K.; Milton, J.; Liu, W. Effect of localized trauma and temporary splinting on immature skeletal muscle and mobility of the femorotibial joint in the dog. Am. J. Vet. Res. 1982, 43, 454–460. [Google Scholar] [PubMed]
- Booth, F.W.; Kelso, J.R. Production of rat muscle atrophy by cast fixation. J. Appl. Physiol. 1973, 34, 404–406. [Google Scholar] [CrossRef] [PubMed]
- Booth, F. Time course of muscular atrophy during immobilization of hindlimbs in rats. J. Appl. Physiol. 1977, 43, 656–661. [Google Scholar] [CrossRef]
- Frimel, T.N.; Kapadia, F.; Gaidosh, G.S.; Li, Y.; Walter, G.A.; Vandenborne, K. A model of muscle atrophy using cast immobilization in mice. Muscle Nerve 2005, 32, 672–674. [Google Scholar] [CrossRef]
- Aihara, M.; Hirose, N.; Katsuta, W.; Saito, F.; Maruyama, H.; Hagiwara, H. A new model of skeletal muscle atrophy induced by immobilization using a hook-and-loop fastener in mice. J. Phys. Ther. Sci. 2017, 29, 1779–1783. [Google Scholar] [CrossRef] [PubMed]
- Onda, A.; Kono, H.; Jiao, Q.; Akimoto, T.; Miyamoto, T.; Sawada, Y.; Suzuki, K.; Kusakari, Y.; Minamisawa, S.; Fukubayashi, T. New mouse model of skeletal muscle atrophy using spiral wire immobilization. Muscle Nerve 2016, 54, 788–791. [Google Scholar] [CrossRef]
- Shivaprasad, M.; Yashavantha, K.; Ravikumar, T.; Shreel, K. Surgical management of quadriceps contracture. Int. J. Sci. Res. 2015, 4, 1919–1922. [Google Scholar]
- Trudel, G. Differentiating the myogenic and arthrogenic components of joint contractures. An experimental study on the rat knee joint. Int. J. Rehabil. Res. 1997, 20, 397–404. [Google Scholar] [CrossRef]
- Zhou, Y.; Zhou, C.X.; Wang, F.; Hua, W.; Fang, Q.Z.; Xiong, K.G.; Zhang, Q.B. A novel external immobilization method to establish a rat model of knee extension contracture. Res. Sq. 2022. [Google Scholar] [CrossRef]
- Zhou, Y.; Zhang, Q.B.; Zhong, H.Z.; Liu, Y.; Li, J.; Lv, H.; Jing, J.H. Rabbit model of extending knee joint contracture: Progression of joint motion restriction and subsequent joint capsule changes after immobilization. J. Knee Surg. 2020, 33, 15–21. [Google Scholar] [CrossRef]
- Swaim, S.F.; Renberg, W.C.; Shike, K.M. Small Animal Bandaging, Casting, and Splinting Techniques; John Wiley & Sons: Hoboken, NJ, USA, 2011; pp. 43–109. [Google Scholar]
- Jang, Y.; Park, Y.E.; Yun, C.-W.; Kim, D.-H.; Chung, H. The vest-collar as a rodent collar to prevent licking and scratching during experiments. Lab Anim. 2016, 50, 296–304. [Google Scholar] [CrossRef]
- Millis, D.; Levine, D. Joint motions and ranges. In Canine Rehabilitation and Physical Therapy; Elsevier Health Sciences: Amsterdam, The Netherlands, 2013; pp. 730–735. [Google Scholar]
- Method of Euthanasia. Available online: https://www.olac.berkeley.edu/sites/default/files/doc/adult_and_neonatal_mouse_and_rat_euthanasia.10.15.2020.pdf (accessed on 1 April 2022).
- Kawahara, Y.; Nikawa, T.; Hirasaka, K.; Miyashita, T.; Kataoka, K.; Yuge, L. Preventive effect of isometric contraction exercise on disuse muscle atrophy using tail suspension mice. J. Phys. Ther. Sci. 2008, 20, 39–44. [Google Scholar] [CrossRef] [Green Version]
- Ambrogi, L. Manual of Histologic and Special Staining Techniques; Mc Graw-Hill Book Company New York: New York, NY, USA, 1960. [Google Scholar]
- Sirius Red Staining Protocol for Collagen. Available online: http://www.ihcworld.com/_protocols/special_stains/sirius_red.htm (accessed on 11 July 2022).
- Gomes, A.R.; Coutinho, E.L.; França, C.N.; Polonio, J.; Salvini, T.F. Effect of one stretch a week applied to the immobilized soleus muscle on rat muscle fiber morphology. Braz. J. Med. Biol. Res. 2004, 37, 1473–1480. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coutinho, E.; Gomes, A.; França, C.; Oishi, J.; Salvini, T. Effect of passive stretching on the immobilized soleus muscle fiber morphology. Braz. J. Med. Biol. Res. 2004, 37, 1853–1861. [Google Scholar] [CrossRef] [Green Version]
- Akkad, H.; Corpeno, R.; Larsson, L. Masseter muscle myofibrillar protein synthesis and degradation in an experimental critical illness myopathy model. PLoS ONE 2014, 9, e92622. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Durigan, J.L.; Delfino, G.B.; Peviani, S.M.; Russo, T.L.; Ramírez, C.; Da Silva Gomes, A.D.; Salvini, T.F. Neuromuscular electrical stimulation alters gene expression and delays quadriceps muscle atrophy of rats after anterior cruciate ligament transection. Muscle Nerve 2014, 49, 120–128. [Google Scholar] [CrossRef] [PubMed]
- Cunha, D.; Nascimento, C.; Artifon, E.; Ferrari, D.; Ribeiro, L.; Fontanesi, L.; Bertolini, G. Evaluation of rats’ soleus muscle submitted to remobilization protocol with therapeutic ultrasound associated with static stretching. J. Morphol. Sci. 2012, 29, 53–57. [Google Scholar]
- Ohmichi, Y.; Sato, J.; Ohmichi, M.; Sakurai, H.; Yoshimoto, T.; Morimoto, A.; Hashimoto, T.; Eguchi, K.; Nishihara, M.; Arai, Y.C. Two-week cast immobilization induced chronic widespread hyperalgesia in rats. Eur. J. Pain 2012, 16, 338–348. [Google Scholar] [CrossRef]
- Guo, T.-Z.; Wei, T.; Li, W.-W.; Li, X.-Q.; Clark, J.D.; Kingery, W.S. Immobilization contributes to exaggerated neuropeptide signaling, inflammatory changes, and nociceptive sensitization after fracture in rats. J. Pain 2014, 15, 1033–1045. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maynard, R.L.; Downes, N. The musculature of the rat. In Anatomy and Histology of the Laboratory Rat in Toxicology and Biomedical Research; Academic Press: Cambridge, MA, USA, 2019; pp. 57–76. [Google Scholar]
- Cavalcante, J.G.T.; Marqueti, R.d.C.; Geremia, J.M.; Sousa Neto, I.V.d.; Baroni, B.M.; Silbernagel, K.G.; Bottaro, M.; Babault, N.; Durigan, J.L.Q. The effect of quadriceps muscle length on maximum neuromuscular electrical stimulation evoked contraction, muscle architecture, and tendon-aponeurosis stiffness. Front. Physiol. 2021, 12, 633589. [Google Scholar] [CrossRef] [PubMed]
- Landin, D.; Thompson, M.; Reid, M. The contribution of the rectus femoris to hip flexion. J. Athl. Enhanc. 2014, 3. [Google Scholar] [CrossRef]
- Nagai, M.; Aoyama, T.; Ito, A.; Iijima, H.; Yamaguchi, S.; Tajino, J.; Zhang, X.; Akiyama, H.; Kuroki, H. Contributions of biarticular myogenic components to the limitation of the range of motion after immobilization of rat knee joint. BMC Musculoskelet Disord. 2014, 15, 224. [Google Scholar] [CrossRef] [Green Version]
- Wong, K.; Trudel, G.; Laneuville, O. Noninflammatory joint contractures arising from immobility: Animal models to future treatments. Biomed. Res. Int. 2015, 2015, 848290. [Google Scholar] [CrossRef] [Green Version]
- Kumar, V.; Abbas, A.K.; Aster, J. Cell injury, cell death, and adaptations. In Robbins Basic Pathology, 9th ed.; Elsevier: North York, ON, Canada, 2013; pp. 1–28. [Google Scholar]
- Achouri, A.; Melizi, M.; Belbedj, H.; Azizi, A. Comparative study of histological and histo-chemical image processing in muscle fiber sections of broiler chicken. J. Appl. Poult. Res. 2021, 30, 100173. [Google Scholar] [CrossRef]
- Dumitru, A.; Radu, B.; Radu, M.; Cretoiu, S. Muscle changes during atrophy. In Muscle Atrophy; Xiao, J., Ed.; Springer: Gateway East, Singapore, 2018; pp. 73–92. [Google Scholar]
- Young, B.; Woodford, P.; O’Dowd, G. Wheater’s Functional Histology: A Text and Colour Atlas; Elsevier: Philadelphia, PA, USA, 2013; pp. 101–121. [Google Scholar]
- NTP Nonneoplastic Lesion Atlas: Skeletal Muscle-Atrophy. Available online: https://ntp.niehs.nih.gov/nnl/musculoskeletal/skel_musc/atrophy/skeletal-muscle-atrophy_508.pdf (accessed on 20 July 2022).
- Shoulders, M.D.; Raines, R.T. Collagen structure and stability. Annu. Rev. Biochem. 2009, 78, 929–958. [Google Scholar] [CrossRef] [Green Version]
- Calvi, E.N.d.C.; Nahas, F.X.; Barbosa, M.V.; Calil, J.A.; Ihara, S.S.M.; Silva, M.d.S.; Franco, M.F.d.; Ferreira, L.M. An experimental model for the study of collagen fibers in skeletal muscle. Acta Cir. Bras. 2012, 27, 681–686. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Honda, Y.; Sakamoto, J.; Nakano, J.; Kataoka, H.; Sasabe, R.; Goto, K.; Tanaka, M.; Origuchi, T.; Yoshimura, T.; Okita, M. Upregulation of interleukin-1beta/transforming growth factor-beta1 and hypoxia relate to molecular mechanisms underlying immobilization-induced muscle contracture. Muscle Nerve 2015, 52, 419–427. [Google Scholar] [CrossRef] [PubMed]
- Hibino, I.; Okita, M.; Inoue, T.; Banno, Y.; Hoso, M. Effect of immobilization on insoluble collagen concentration and type I and type III collagen isoforms of rat soleus muscle. J. Jpn. Phys. Ther. Assoc. 2008, 11, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Son, H.; Yang, J.H.; Kim, H.J.; Lee, D.K. A chronic immobilization stress protocol for inducing depression-like behavior in mice. J. Vis. Exp. 2019, 147, e59546. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kennett, G.A.; Dickinson, S.L.; Curzon, G. Enhancement of some 5-HT-dependent behavioural responses following repeated immobilization in rats. Brain Res. 1985, 330, 253–263. [Google Scholar] [CrossRef] [PubMed]
- Haque, Z.; Akbar, N.; Yasmin, F.; Haleem, M.A.; Haleem, D.J. Inhibition of immobilization stress-induced anorexia, behavioral deficits, and plasma corticosterone secretion by injected leptin in rats. Stress 2013, 16, 353–362. [Google Scholar] [CrossRef]
- Monteiro, F.; Abraham, M.; Sahakari, S.; Mascarenhas, J. Effect of immobilization stress on food intake, body weight and weights of various organs in rat. Indian J. Physiol. Pharmacol. 1989, 33, 186–190. [Google Scholar]
- Haleem, D.J.; Jabeen, B.; Parveen, T. Inhibition of restraint-induced anorexia by injected tryptophan. Life Sci. 1998, 63, 205–212. [Google Scholar] [CrossRef]
- Slimani, L.; Micol, D.; Amat, J.; Delcros, G.; Meunier, B.; Taillandier, D.; Polge, C.; Béchet, D.; Dardevet, D.; Picard, B. The worsening of tibialis anterior muscle atrophy during recovery post-immobilization correlates with enhanced connective tissue area, proteolysis, and apoptosis. Am. J. Physiol. Endocrinol. 2012, 303, 1335–1347. [Google Scholar] [CrossRef]
- Ellis, C.; Mori, M. Skin diseases of rodents and small exotic mammals. Vet. Clin. N. Am. Exot. Anim. Pract. 2001, 4, 493–542. [Google Scholar] [CrossRef]
- Flecknell, P. Analgesia and Post-operative care. In Laboratory Animal Anaesthesia, 3rd ed.; Flecknell, P., Ed.; Elsevier: New York, NY, USA, 2015; pp. 139–180. [Google Scholar]
- Glen, M.; Otto, C.L.F.; Charles, B. Clifford. Biology and Diseases of Rats. In Laboratory Animal Medicine, 3rd ed.; Fox, J.G., Ed.; Elsevier: New York, NY, USA, 2015; pp. 151–208. [Google Scholar]
- Keeble, E.; Meredith, A. BSAVA Manual of Rodents and Ferrets; British Small Animal Veterinary Association: Gloucester, UK, 2009; pp. 1–192. [Google Scholar]
- Rosa-Caldwell, M.E.; Greene, N.P. Muscle metabolism and atrophy: Let’s talk about sex. Biol. Sex Differ. 2019, 10, 43. [Google Scholar] [CrossRef] [PubMed]
- Carson, J.A.; Manolagas, S.C. Effects of sex steroids on bones and muscles: Similarities, parallels, and putative interactions in health and disease. Bone 2015, 80, 67–78. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Day | Group | |||
|---|---|---|---|---|
| C (n = 5) | I (n = 6) | V (n = 6) | S (n = 6) | |
| 1 | 211.1 ± 7.0 | 211.9 ± 9.6 | 216.6 ± 8.4 | 212.6 ± 7.3 |
| 2 | 221.2 ± 8.0 a | 210.8 ± 10.6 | 210.2 ± 10.2 a | 223.1 ± 9.5 a |
| 5 | 239.0 ± 9.1 ab | 207.1 ± 10.5 * | 211.2 ± 6.4 * | 215.5 ± 6.7 * |
| 8 | 259.9 ± 14.9 abc | 214.4 ± 14.0 * | 215.4 ± 6.8 * | 222.7 ± 8.8 * |
| 11 | 279.7 ± 14.3 abcd | 213.7 ± 9.2 * | 217.2 ± 11.0 * | 227.1 ± 11.6 *c |
| 14 | 297.1 ± 15.0 abcde | 219.4 ± 15.4 * | 220.2 ± 9.9 * | 237.4 ± 11.6 *abc |
| 15 | 299.4 ± 14.6 abcde | 218.1 ± 18.8 * | 222.9 ± 12.4 * | 234.5 ± 11.4 *abc |
| Day | Group | |||
|---|---|---|---|---|
| C (n = 5) | I (n = 6) | V (n = 6) | S (n = 6) | |
| 2 | 19.0 ± 2.2 | 11.6 ± 5.4 | 15.2 ± 5.9 | 17.3 ± 3.5 |
| 5 | 22.2 ± 1.1 | 17.4 ± 2.7 * | 17.9 ± 1.7 * | 18.2 ± 1.3 * |
| 8 | 22.8 ± 1.7 | 20.1 ± 2.3 | 19.1 ± 1.3 * | 20.4 ± 2.2 |
| 11 | 23.7 ± 0.9 | 19.6 ± 1.6 *a | 20.5 ± 3.3 | 21.2 ± 3.0 |
| 14 | 23.2 ± 0.8 a | 19.8 ± 2.6 a | 20.4 ± 1.3 * | 23.0 ± 2.7 a |
| Measurements | Group | ||
|---|---|---|---|
| I (n = 6) | V (n = 6) | S (n = 6) | |
| Application time (minutes) | 4.6 (4.0–5.5) | 7.5 (6.3–8.8) | 12.6 * (9.9–13.0) |
| Frequency of rewinding (times) | 1.0 (0.8–1.0) | 2.5 # (1.8–4.3) | 1.5 (0.8–2.0) |
| Joint and Position | Group | ||||
|---|---|---|---|---|---|
| C (n = 10) | I (n = 12) | V (n = 12) | S (n = 12) | ||
| Hip | Extension | 150.0 (147.5–155.0) | 157.5 (155.0–165.0) | 157.5 (150.0–163.8) | 147.5 (145.0–155.0) |
| Flexion | 41.5 (27.5–51.3) | 45.0 (41.3–50.0) | 45.0 (40.0–45.0) | 55 ac (45.0–55.0) | |
| Knee | Extension | 160.0 (155.0–161.3) | 170.0 a (165.0–173.8) | 160.0 (160.0–165.0) | 169.0 a (165.0–170.0) |
| Flexion | 40.0 (35.0–42.5) | 72.5 a (60.0–80.0) | 72.5 a (61.3–75.0) | 97.5 abc (90.0–133.8) | |
| Ankle | Extension | 160.0 (160.0–160.0) | 170.0 a (165.0–170.0) | 160.0 (160.0–165.0) | 172.5 a (170.0–175.0) |
| Flexion | 5.0 (5.0–5.0) | 65.0 a (55.0–80.0) | 70.0 a (55.0–75.0) | 95.0 abc (88.5–107.3) | |
| Quadriceps Muscle | Group | |||
|---|---|---|---|---|
| C (n = 10) | I (n = 12) | V (n = 12) | S (n = 12) | |
| Muscle weight (g) | 2.1 (1.8–2.2) | 1.2 (1.1–1.3) | 1.3 (1.2–1.3) | 1.0 abc (1.0–1.1) |
| Muscle weight/Body weight (mg/g) | 7.1 (5.7–7.4) | 5.5 (5.1–5.8) | 5.7 (5.5–5.9) | 4.4 abc (4.2–4.6) |
| Muscle measurement (mm) | ||||
| Width | 14.3 (14.1–15.2) | 11.6 a (11.2–11.9) | 12.5 a (11.6–13.4) | 11.8 a (11.0–12.7) |
| Length | 26.0 (24.4–26.9) | 23.8 (22.6–24.9) | 24.1 (23.6–25.1) | 22.8 a (22.4–23.5) |
| Height | 9.3 (8.2–9.7) | 7.3 a (6.9–7.6) | 7.5 a (6.8–8.3) | 7.1 a (6.1–7.8) |
| Collagen Amount (%) | Group | |||
|---|---|---|---|---|
| C (n = 10) | I (n = 12) | V (n = 12) | S (n = 12) | |
| Masson’s trichrome Collagen percentage | 0.5 (0.4–0.7) | 1.0* (0.8–1.5) | 1.1 * (0.9–1.4) | 1.5 * (1.3–1.7) |
| Picrosirius red Collagen percentage | 0.9 (0.6–1.2) | 2.1 * (1.7–2.4) | 2.0 * (1.5–2.5) | 2.9 * (2.3–3.3) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Suwankanit, K.; Shimizu, M. Rat Model of Quadriceps Contracture by Joint Immobilization. Biology 2022, 11, 1781. https://doi.org/10.3390/biology11121781
Suwankanit K, Shimizu M. Rat Model of Quadriceps Contracture by Joint Immobilization. Biology. 2022; 11(12):1781. https://doi.org/10.3390/biology11121781
Chicago/Turabian StyleSuwankanit, Kanokwan, and Miki Shimizu. 2022. "Rat Model of Quadriceps Contracture by Joint Immobilization" Biology 11, no. 12: 1781. https://doi.org/10.3390/biology11121781