
Comparative Analysis of Periodontal Pain According to the Type of Precision Orthodontic Appliances: Vestibular, Lingual and Aligners. A Prospective Clinical Study

 ,
,  ,
,  , ,
, ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Characteristics of the Participants
3.2. Analysis of the Periodontal Location of Pain
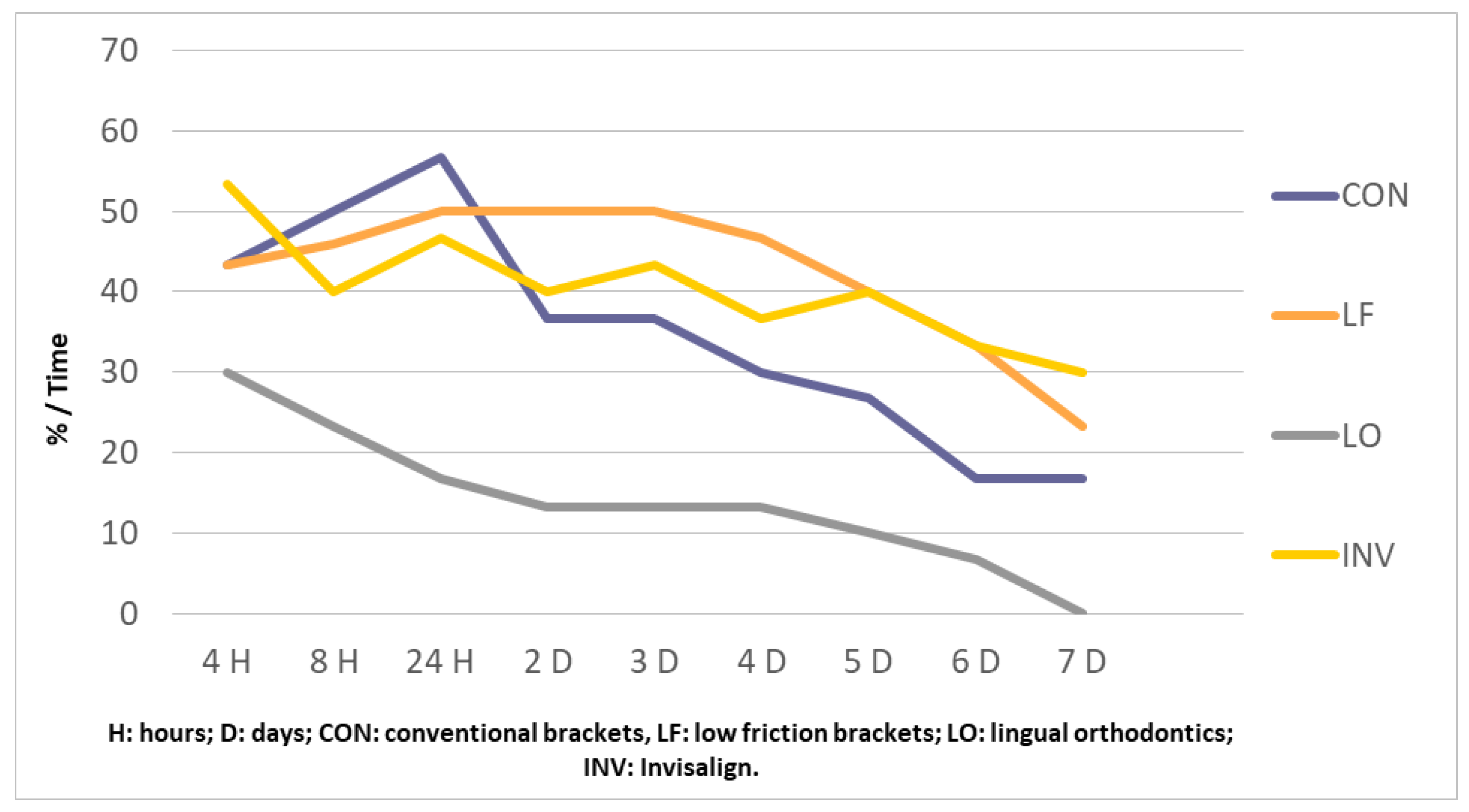
3.2.1. Evolution of Pain in Both Anterior Arches
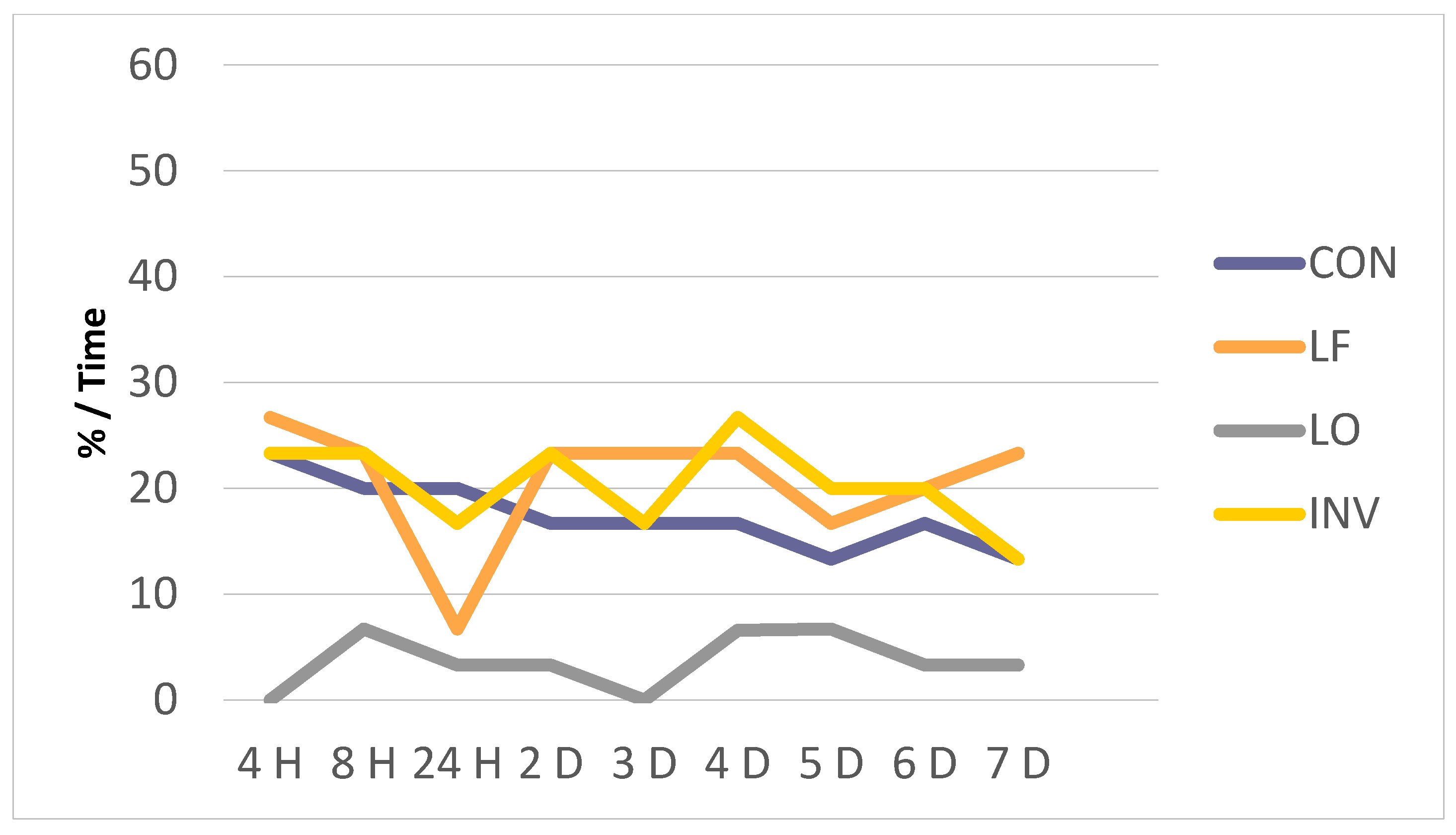
3.2.2. Evolution of Pain in the Anterior Maxillary Location
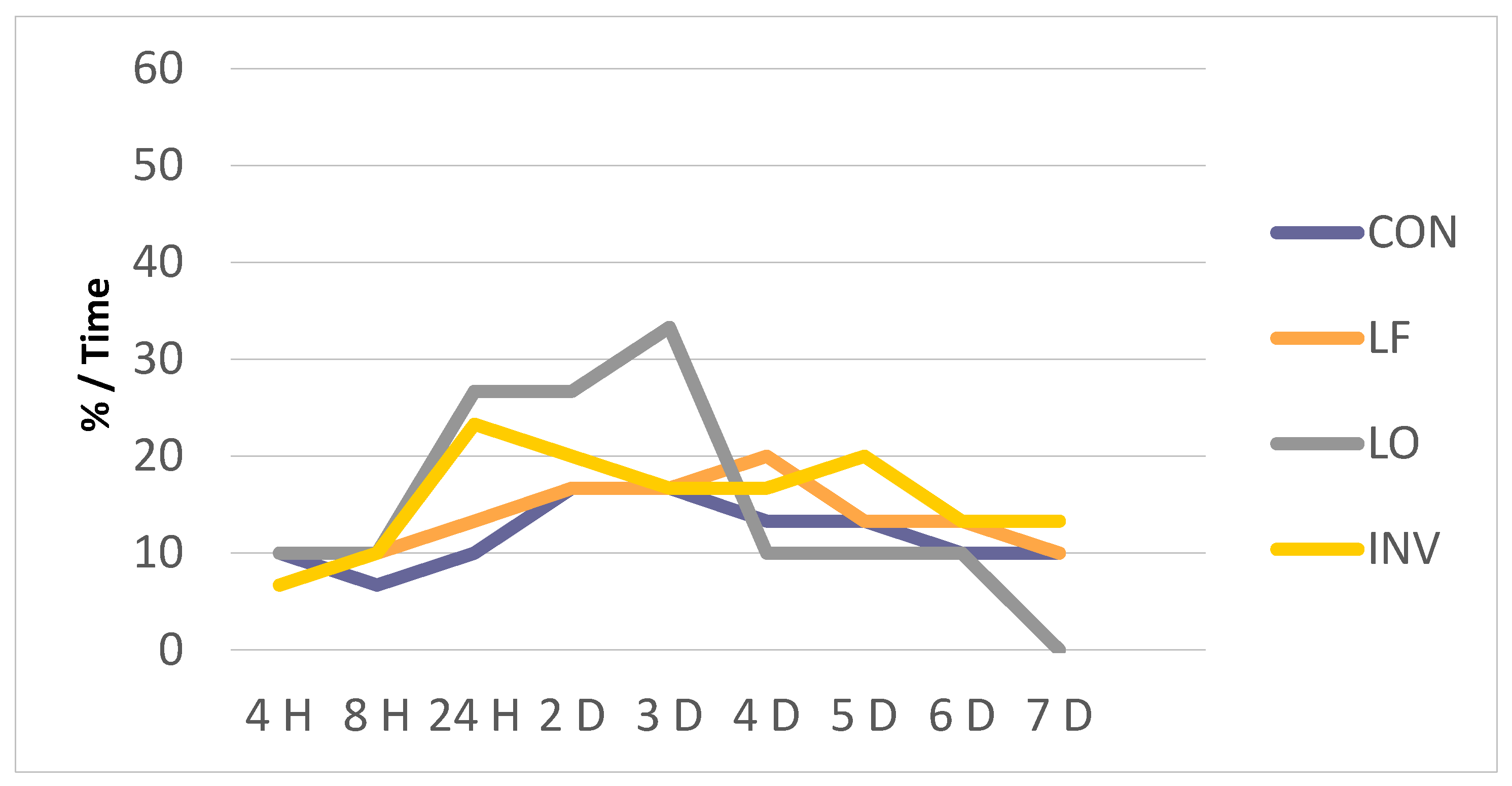
3.2.3. Evolution of Pain in the Anterior Mandibular Location
3.3. Analysis of the Degree of Pain by Groups
3.4. Analysis of the Type of Pain by Groups
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Klepac, R.K.; Dowling, J.; Hauge, G. Reports of pain after dental treatment, electrical tooth pulp stimulation and cutaneous shock. J. Am. Dent. Assoc. 1980, 100, 692–695. [Google Scholar] [CrossRef] [PubMed]
- Vassend, O. Anxiety, pain and discomfort associated with dental treatment. Behav. Res. Ther. 1993, 31, 659–666. [Google Scholar] [CrossRef]
- Carter, A.E.; Carter, G.; Boschen, M.; AlShwaimi, E.; George, R. Pathways of fear and anxiety in dentistry: A review. World J. Clin. Cases 2014, 2, 642–653. [Google Scholar] [CrossRef]
- Barlet, B.; Firestone, A.; Vig, K.; Beck, M.; Maruchae, P. The influence of a structured telephone call on orthodontic pain and anxiety. Am. J. Orthod. Dentofac. Orthop. 2005, 128, 435–441. [Google Scholar] [CrossRef] [PubMed]
- Sawada, A.; Usui, N.; Shimazaki, K.; Taira, M.; Ono, T. The effects of cognitive behavioral therapy on experimental orthodontic pain. Orthod. Waves 2015, 74, 10–14. [Google Scholar] [CrossRef]
- Ngan, P.; Kess, B.; Wilson, S. Perception of discomfort by patients undergoing orthodontic treatment. Am. J. Orthod. Dentofac. Orthop. 1989, 961, 47–53. [Google Scholar] [CrossRef]
- Bergius, M.; Kiliaridis, S.; Berggren, U. Pain in orthodontics. A review and discussion of the literature. J. Orofac. Orthop. 2000, 61, 125–137. [Google Scholar] [CrossRef]
- Feldmann, I.; List, T.; Bondemark, L. Orthodontic anchoring techniques and its influence on pain, discomfort, and jaw function—A randomized controlled trial. Eur. J. Orthod. 2012, 34, 102–108. [Google Scholar] [CrossRef] [Green Version]
- Polat-Ozsoy, O. Pain and Discomfort after Orthodontic Appointments. Semin. Orthod. 2007, 13, 292–300. [Google Scholar] [CrossRef]
- Krishnan, V. Orthodontic pain: From causes to management—A review. Eur. J. Orthod. 2007, 29, 170–179. [Google Scholar] [CrossRef] [Green Version]
- Kluemper, G.T.; Hiser, D.G.; Rayens, M.K.; Jay, M.J. Efficacy of a wax containing benzocaine in the relief of oral mucosal pain caused by orthodontic appliances. Am. J. Orthod. Dentofac. Orthop. 2002, 122, 359–365. [Google Scholar] [CrossRef] [PubMed]
- O’Connor, P.J. Patients’ perceptions before, during, and after orthodontic treatment. J. Clin. Orthod. 2000, 34, 591–592. [Google Scholar] [PubMed]
- Antonio-Zancajo, L.; Montero, J.; Albaladejo, A.; Oteo-Calatayud, M.D.; Alvarado-Lorenzo, A. Pain and Oral-Health-Related Quality of Life in Orthodontic Patients During Initial Therapy with Conventional, Low-Friction, and Lingual Brackets and Aligners (Invisalign): A Prospective Clinical Study. J. Clin. Med. 2020, 9, 2088. [Google Scholar] [CrossRef] [PubMed]
- Scott, P.; Sherriff, M.; DiBiase, A.T.; Cobourne, M.T. Perception of discomfort during initial orthodontic tooth alignment using a self-ligating or conventional bracket system: A randomized clinical trial. Eur. J. Orthod. 2008, 30, 227–232. [Google Scholar] [CrossRef] [Green Version]
- Tecco, S.; D’Attilio, M.; Tetè, S.; Festa, F. Prevalence and type of pain during conventional and self-ligating orthodontic treatment. Eur. J. Orthod. 2009, 31, 380–384. [Google Scholar] [CrossRef] [PubMed]
- Jones, M.; Chan, C. The pain and discomfort experienced during orthodontic treatment: A randomized controlled clinical trial of two initial aligning arch wires. Am. J. Orthod. Dentofac. Orthop. 1992, 102, 373–381. [Google Scholar] [CrossRef]
- Bernhardt, M.; Southard, K.; Batterson, K.; Logan, H.; Baker, K.; Pharm, B.S.; Pharm, M.S.; Jakobsen, J. The effect of preemptive and/or ibuprofen therapy for orthodontic pain postoperative. Am. J. Orthod. Dentofac. Orthop. 2001, 120, 20–27. [Google Scholar] [CrossRef] [Green Version]
- Bird, S.E.; Williams, K.; Kula, K. Preoperative acetaminophen vs ibuprofen for control of pain after orthodontic separator placement. Am. J. Orthod. Dentofac. Orthop. 2007, 132, 504–510. [Google Scholar] [CrossRef]
- Rakhshan, H.; Rakhshan, V. Pain and discomfort perceived during the initial stage of active fixed orthodontic treatment. Saudi Dent. J. 2015, 27, 81–87. [Google Scholar] [CrossRef] [Green Version]
- Lew, K.K. Attitudes and perceptions of adults towards orthodontic treatment in an Asian community. Community Dent. Oral Epidemiol. 1993, 21, 31–35. [Google Scholar] [CrossRef] [PubMed]
- Sergl, H.G.; Klages, U.; Zentner, A. Functional and social discomfort during orthodontic treatment effects on compliance and prediction of patients’ adaptation by personality variables. Eur. J. Orthod. 2000, 22, 307–315. [Google Scholar] [CrossRef]
- Otasevic, M.; Naini, F.B.; Gill, D.S.; Lee, R.T. Prospective randomized clinical trial comparing the effects of a masticatory bite wafer and avoidance of hard food on pain associated with initial orthodontic tooth movement. Am. J. Orthod. Dentofac. Orthop. 2006, 130, 6.e9–6.e15. [Google Scholar] [CrossRef] [PubMed]
- Wiedel, A.P.; Bondemark, L. A randomized controlled trial of self-perceived pain, discomfort, and impairment of jaw function in children undergoing orthodontic treatment with fixed or removable appliances. Angle Orthod. 2016, 86, 324–330. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hixon, E.H.; Aitikian, H.; Callow, G.; McDonald, H.; Tacy, R.J. Optimal force, differential force and anchorage. Am. J. Orthod. 1968, 55, 437–451. [Google Scholar] [CrossRef]
- Ogura, M.; Kamimura, H.; Al-Kalaly, A.; Nagayama, K.; Taira, K.; Nagata, J.; Miyawaki, S. Pain intensity during the first 7 days following the application of light and heavy continuous forces. Eur. J. Orthod. 2009, 31, 314–319. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johal, A.; Ashari, A.B.; AlAmiri, N.; Fleming, P.S.; Qureshi, U.; Cox, S.; Pandis, N. Pain experience in adults undergoing treatment: A longitudinal evaluation. Angle Orthod. 2018, 88, 292–298. [Google Scholar] [CrossRef] [Green Version]
- Miller, K.B.; McGorray, S.P.; Womack, R.; Quintero, J.C.; Perelmuter, M.; Gibson, J.; Dolan, T.A.; Wheeler, T.T. A comparison of treatment impacts between Invisalign aligner and fixed appliance therapy during the first week of treatment. Am. J. Orthod. Dentofac. Orthop. 2007, 131, 302.e1–302.e9. [Google Scholar] [CrossRef]
- Bergius, M.; Broberg, A.; Hakeberg, M.; Berggrend, U. Prediction of prolonged pain experiences during orthodontic treatment. Am. J. Orthod. Dentofac. Orthop. 2008, 133, 339.e1–339.e8. [Google Scholar] [CrossRef]
- Johal, A.; Fleming, P.S.; Al Jawad, F.A. A prospective longitudinal controlled assessment of pain experience and oral health-related quality of life in adolescents undergoing fixed appliance treatment. Orthod. Craniofacial Res. 2014, 17, 178–186. [Google Scholar] [CrossRef]
- Caniklioglu, C.; Oztürk, Y. Patient discomfort: A comparison between lingual and labial fixed appliances. Angle Orthod. 2005, 75, 86–91. [Google Scholar]
- Wu, A.K.Y.; McGrath, C.P.J.; Wong, R.; Wiechmann, D.; Rabie, A.B.M. A comparison of pain experienced by patients treated with labial and lingual orthodontic appliances. Eur. J. Orthod. 2009, 32, 403–407. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Melzack, R. The McGill Pain Questionnaire: Major properties and scoring methods. Pain 1975, 1, 277–299. [Google Scholar] [CrossRef]
- Sandhu, S.S. Validating the factor structure and testing measurement invariance of modified Short-Form McGill Pain Questionnaire (Ortho-SF-MPQ) for orthodontic pain assessment. J. Orthod. 2017, 44, 34–43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scuzzo, G.; Takemoto, K.; Takemoto, Y.; Takemoto, A.; Lombardo, L. A new lingual straight-wire technique. J. Clin. Orthod. 2010, 44, 114–123. [Google Scholar] [PubMed]
- Warren, J.J.; Bishara, S.E.; Yonezu, T. Tooth size-arch length relationships in the deciduous dentition: A comparison between contemporary and historical samples. Am. J. Orthod. Dentofac. Orthop. 2003, 123, 614–619. [Google Scholar] [CrossRef]
- Caton, J.G.; Armitage, G.; Berglundh, T.; Chapple, I.L.C.; Jepsen, S.; Kornman, K.S.; Mealey, B.L.; Papapanou, P.N.; Sanz, M.; Tonetti, M.S. A new classification scheme for periodontal and periimplant diseases and conditions—Introduction and key changes from the 1999 classification. J. Clin. Periodontol. 2018, 45, S1–S8. [Google Scholar] [CrossRef] [PubMed]
- Iwasaki, L.R.; Freytag, L.E.; Schumacher, C.A.; Walker, M.P.; Williams, K.B. Validation of a modified McGill Pain Questionnaire for orthodontic patients. Angle Orthod. 2013, 83, 906–912. [Google Scholar] [CrossRef]
- Dworkin, R.H.; Turk, D.C.; Trudeau, J.; Benson, C.; Biondi, D.M.; Katz, N.P.; Kim, M. Validation of the Short-Form McGill Pain Questionnaire-2 (SF-MPQ-2) in Acute Low Back Pain. J. Pain 2015, 16, 357–366. [Google Scholar] [CrossRef]
- Kane, R.L.; Bershadsky, B.; Rockwood, T.; Saleh, K.; Islam, N.C. Visual Analog Scale pain reporting was standardized. J. Clin. Epidemiol. 2005, 58, 618–623. [Google Scholar] [CrossRef]
- Shalish, M.; Cooper-Kazaz, R.; Ivgi, I.; Canetti, L.; Tsur, B.; Bachar, E.; Chaushu, S. Adult Patients’ Adjustability to Orthodontic Appliances. Part I: A Comparison between Labial, Lingual, and Invisalign™. Eur. J. Orthod. 2012, 34, 724–730. [Google Scholar] [CrossRef] [Green Version]
- Liao, L.; Long, H.; Zhang, L.; Chen, H.; Zhou, Y.; Ye, N.; Lai, W. Evaluation of pain in rats through facial expression following experimental tooth movement. Eur. J. Oral Sci. 2014, 122, 121–124. [Google Scholar] [CrossRef]
- Schumacher, H.A.; Bourauel, C.; Drescher, D. The deactivation behavior and effectiveness of different orthodontic leveling arches—A dynamic analysis of the force. Fortschr. Kieferorthop. 1992, 53, 273–285. [Google Scholar] [CrossRef] [PubMed]
- Abdelrahman, R.S.; Al-Nimri, K.S.; Al Maaitah, E.F. Pain experience during initial alignment with three types of nickel-titanium archwires: A prospective clinical trial. Angle Orthod. 2015, 85, 1021–1026. [Google Scholar] [CrossRef]
- Cioffi, I.; Piccolo, A.; Tagliaferri, R.; Paduano, S.; Galeotti, A.; Martina, R. Pain perception following first orthodontic archwire placement--thermoelastic vs superelastic alloys: A randomized controlled trial. Quintessence Int. 2012, 43, 61–69. [Google Scholar] [PubMed]
- Jian, F.; Lai, W.; Furness, S.; McIntyre, G.; Millett, D.T.; Hickman, J.; Wang, Y. Initial arch wires for tooth alignment during orthodontic treatment with fixed appliances. Cochrane Database Syst. Rev. 2013, CD007859. [Google Scholar] [CrossRef] [PubMed]
- Scheurer, P.A.; Firestone, A.R.; Burbin, W.B. Perception of pain as a result of orthodontic treatment with fixed appliances. Eur. J. Orthod. 1996, 18, 349–357. [Google Scholar] [CrossRef] [PubMed]
- Ngan, P.; Wilson, S.; Shanfeld, J.; Amini, H. The effect of ibuprofen on the level of discomfort in patients undergoing orthodontic treatment. Am. J. Orthod. Dentofac. Orthop. 1995, 106, 88–95. [Google Scholar] [CrossRef]
- Erdinç, A.M.E.; Dinçer, B. Perception of pain during orthodontic treatment with fixed appliances. Eur. J. Orthod. 2004, 26, 79–85. [Google Scholar] [CrossRef]
- Fernandes, L.M.; Ogaard, B.; Skoglund, L. Pain and discomfort experienced after placement of a conventional or a superelastic NiTi aligning archwire. A randomized clinical trial. J. Orofac. Orthop. 1998, 59, 331–339. [Google Scholar] [CrossRef]
- Long, H.; Zhou, Y.; Pyakurel, U.; Liao, L.; Jian, F.; Xue, J.; Ye, N.; Yang, X.; Wang, Y.; Lai, W. Comparison of adverse effects between lingual and labial orthodontic treatment: A systematic review. Angle Orthod. 2013, 83, 1066–1073. [Google Scholar] [CrossRef] [Green Version]
- Casteluci, C.E.V.F.; Oltramari, P.V.P.; Conti, P.C.R.; Bonjardim, L.R.; de Almeida-Pedrin, R.R.; Fernandes, T.M.F.; de Almeida, M.R.; de Castro Ferreira Conti, A.C. Evaluation of pain intensity in patients treated with aligners and conventional fixed appliances: Randomized clinical trial. Randomized Control. Trial 2021, 24, 268–276. [Google Scholar] [CrossRef] [PubMed]
- Lai, T.T.; Chiou, J.Y.; Lai, T.C.; Chen, T.; Wang, H.Y.; Li, C.H.; Chen, M.H. Perceived pain for orthodontic patients with conventional brackets or self-ligating brackets over 1 month period: A single-center, randomized controlled clinical trial. J. Med. Assoc. 2020, 119, 282–289. [Google Scholar] [CrossRef] [PubMed]
- Diddige, R.; Negi, G.; Kiran, K.; Chitra, P. Comparision of pain levels in patients treated with 3 different orthodontic appliances—A randomized trial. Med. Pharm. Rep. 2020, 93, 81–88. [Google Scholar] [PubMed]
- Cardoso, P.C.; Espinosa, D.G.; Mecenas, P.; Flores-Mir, C.; Normando, D. Pain level between clear aligners and fixed appliances: A systematic review. Prog. Orthod. 2020, 21, 3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mheissen, S.; Khan, H.; Aldandan, M. Limited evidence on differences between fixed appliances and clear aligners regarding pain level. Evid. Based Dent. 2020, 21, 144–145. [Google Scholar] [CrossRef] [PubMed]
- Gao, M.; Yan, X.; Zhao, R.; Shan, Y.; Chen, Y.; Jian, F.; Long, H.; Lai, W. Comparison of pain perception, anxiety, and impacts on oral health-related quality of life between patients receiving clear aligners and fixed appliances during the initial stage of orthodontic treatment. Eur. J. Orthod. 2020, 2, cjaa037. [Google Scholar] [CrossRef]
- Brown, D.; Moerenhout, R. The pain experience and psychological adjustment to orthodontic treatment of preadolescents, adolescents and adults. Am. J. Orthod. Dentofac. Orthop. 1991, 19, 349–356. [Google Scholar] [CrossRef]
- Jawaid, M.; Qadeer, T.A.; Fahim, M.F. Pain perception of orthodontic treatment—A cross-sectional study. Pak. J. Med. Sci. 2020, 36, 160–165. [Google Scholar] [CrossRef] [Green Version]
- Patini, R.; Staderini, E.; Camodeca, A.; Guglielmi, F.; Gallenzi, P. Case Reports in Pediatric Dentistry Journals: A Systematic Review about Their Effect on Impact Factor and Future Investigations. Dent. J. 2019, 7, 103. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Age (Years) | Sex | TSALD | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | Men | Woman | Upper | Lower | |||||
| N | % | N | % | Mean | SD. | Mean | SD. | |||
| Conventional Brackets (CON) (n = 30) | 24.7 | 4.1 | 13 | 43.3 | 17 | 56.7 | −3.1 | 1.0 | −3.3 | 1.3 |
| Low-Friction Brackets (LF) (n = 30) | 28 | 9.7 | 12 | 40 | 18 | 60 | −3.1 | 0.7 | −2.7 | 1.2 |
| Lingual Brackets (LO) (n = 30) | 33.8 | 8.2 | 13 | 43.3 | 17 | 56.7 | −3.0 | 1.6 | −3.4 | 1.5 |
| Invisalign (INV) (n = 30) | 33.4 | 5.1 | 16 | 53.3 | 14 | 46.6 | −2.6 | 1.6 | −2.6 | 1.7 |
| Time | Groups | No Pain | Both Arches | Mandible | Maxilla | Whole Mouth | Lower Arch | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Anterior | Posterior | Anterior | Posterior | Anterior | Posterior | ||||||||||||||
| N | % | N | % | N | % | N | % | N | % | N | % | N | % | N | % | N | % | ||
| T4h (4 h) ** | CON | 0 | 0.0 | 13 | 43.3 | 3 | 10.0 | 3 | 10.0 | 2 | 6.7 | 7 | 23.3 | 2 | 6.7 | 0 | 0.0 | 0 | 0.0 |
| LF | 5 | 16.7 | 13 | 43.3 | 0 | 0.0 | 2 | 6.7 | 1 | 3.3 | 8 | 26.7 | 1 | 3.3 | 0 | 0.0 | 0 | 0.0 | |
| LO | 8 | 26.7 | 9 | 30.0 | 4 | 13.3 | 3 | 10.0 | 0 | 0.0 | 0 | 0.0 | 1 | 3.3 | 0 | 0.0 | 0 | 0.0 | |
| INV | 1 | 3.3 | 16 | 53.3 | 4 | 13.3 | 2 | 6.7 | 0 | 0.0 | 7 | 23.3 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | |
| Chi: 46.09, fd: 24; p-value: 0.004 | |||||||||||||||||||
| T8h (8 h) * | CON | 0 | 0.0 | 15 | 50.0 | 3 | 10.0 | 2 | 6.7 | 2 | 6.7 | 6 | 20.0 | 2 | 6.7 | 0 | 0.0 | 0 | 0.0 |
| LF | 3 | 10.0 | 14 | 46.7 | 1 | 3.3 | 3 | 10.0 | 1 | 3.3 | 7 | 23.3 | 1 | 3.3 | 0 | 0.0 | 0 | 0.0 | |
| LO | 3 | 10.0 | 7 | 23.3 | 4 | 13.3 | 3 | 10.0 | 2 | 6.7 | 2 | 6.7 | 1 | 3.3 | 3 | 10.0 | 5 | 16.7 | |
| INV | 1 | 3.3 | 12 | 40.0 | 3 | 10.0 | 6 | 20.0 | 0 | 0.0 | 7 | 23.3 | 1 | 3.3 | 0 | 0.0 | 0 | 0.0 | |
| Chi: 41.21; fd: 24; p-value: 0.016 | |||||||||||||||||||
| T1 (24 h) ** | CON | 0 | 0.0 | 17 | 56.7 | 1 | 3.3 | 3 | 10.0 | 1 | 3.3 | 6 | 20.0 | 2 | 6.7 | 0 | 0.0 | 0 | 0.0 |
| LF | 0 | 0.0 | 15 | 50.0 | 2 | 6.7 | 4 | 13.3 | 1 | 3.3 | 8 | 6.7 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | |
| LO | 4 | 13.3 | 5 | 16.7 | 2 | 6.7 | 8 | 26.7 | 2 | 6.7 | 1 | 3.3 | 1 | 3.3 | 4 | 13.3 | 3 | 10.0 | |
| INV | 0 | 0.0 | 14 | 46.7 | 3 | 10.0 | 7 | 23.3 | 1 | 3.3 | 5 | 16.7 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | |
| Chi: 53.21; fd: 24; p-value: 0.001 | |||||||||||||||||||
| T2 (2 days) ** | CON | 1 | 3.3 | 11 | 36.7 | 4 | 13.3 | 5 | 16.7 | 2 | 6.7 | 5 | 16.7 | 2 | 6.7 | 0 | 0.0 | 0 | 0.0 |
| LF | 1 | 3.3 | 15 | 50.0 | 1 | 3.3 | 5 | 16.7 | 1 | 3.3 | 7 | 23.2 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | |
| LO | 7 | 23.3 | 4 | 13.3 | 2 | 6.7 | 8 | 26.7 | 1 | 3.3 | 1 | 3.3 | 1 | 3.3 | 3 | 10.0 | 3 | 10.0 | |
| INV | 2 | 6.7 | 12 | 40.0 | 3 | 10.0 | 6 | 20.0 | 0 | 0.0 | 7 | 23.3 | 0 | 0.0 | 0 | 0.0 | 0 | 0..0 | |
| Chi: 53.73; fd: 24; p-value: 0.00 | |||||||||||||||||||
| T3 (3 days) ** | CON | 1 | 3.3 | 11 | 36.7 | 4 | 13.3 | 5 | 16.7 | 2 | 6.7 | 5 | 16.7 | 2 | 6.7 | 0 | 0,0 | 0 | 0,0 |
| LF | 1 | 3.3 | 15 | 50.0 | 1 | 3.3 | 5 | 16.7 | 1 | 3.3 | 7 | 23.3 | 0 | 0.0 | 0 | 0,0 | 0 | 0,0 | |
| LO | 9 | 30.0 | 4 | 13.3 | 3 | 10.0 | 10 | 33.3 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 1 | 3.3 | 3 | 10.0 | |
| INV | 3 | 10.0 | 13 | 43.3 | 3 | 10.0 | 5 | 16.7 | 1 | 3.3 | 5 | 16.7 | 0 | 0.0 | 0 | 0,0 | 0 | 0,0 | |
| Chi: 49.7; fd: 24; p-value: 0.002 | |||||||||||||||||||
| T4 (4 days) ** | CON | 5 | 16.7 | 9 | 30.0 | 4 | 13.3 | 4 | 13.3 | 1 | 3.3 | 5 | 16.7 | 2 | 6.7 | 0 | 0.0 | 0 | 0.0 |
| LF | 2 | 6.7 | 14 | 46.7 | 0 | 0.0 | 6 | 20.0 | 1 | 3.3 | 7 | 23.3 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | |
| LO | 16 | 53.3 | 4 | 13.3 | 1. | 3.3 | 3 | 10.0 | 0 | 0.0 | 2 | 6.7 | 0 | 0.0 | 0 | 0.0 | 4 | 13.3 | |
| INV | 3 | 10.0 | 11 | 36.7 | 1 | 3.3 | 5 | 16.7 | 2 | 6.7 | 8 | 26.7 | 0 | 0.0 | 0 | 0,0 | 0 | 0.0 | |
| Chi: 55.74; fd: 21; p-value: 0.00 | |||||||||||||||||||
| T5 (5 days) ** | CON | 8 | 26.7 | 8 | 26.7 | 4 | 13.3 | 4 | 13.3 | 2 | 6.7 | 4 | 13.3 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 |
| LF | 7 | 23.3 | 12 | 40.0 | 0 | 0.0 | 4 | 13.3 | 1 | 3.3 | 5 | 16.7 | 1 | 3.3 | 0 | 0.0 | 0 | 0.0 | |
| LO | 19 | 63.3 | 3 | 10.0 | 0 | 0.0 | 3 | 10.0 | 0 | 0.0 | 2 | 6.7 | 0 | 0.0 | 0 | 0.0 | 3 | 10.0 | |
| INV | 3 | 10.0 | 12 | 40.0 | 1 | 3.3 | 6 | 20.0 | 2 | 6.7 | 6 | 20.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | |
| Chi: 47.45; fd: 21; p-value: 0.001 | |||||||||||||||||||
| T6 (6 days) ** | CON | 12 | 40.0 | 5 | 16.7 | 3 | 10.0 | 3 | 10.0 | 2 | 6.7 | 5 | 16.7 | 0 | 0.0 | 0 | 0,0 | 0 | 0,0 |
| LF | 8 | 26.7 | 10 | 33.3 | 0 | 0.0 | 4 | 13.3 | 1 | 3.3 | 6 | 20.0 | 1 | 3.3 | 0 | 0.0 | 0 | 0.0 | |
| LO | 24 | 80.0 | 2 | 6.7 | 0 | 0.0 | 3 | 10.0 | 0 | 0.0 | 1 | 3.3 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | |
| INV | 9 | 30.0 | 10 | 33.3 | 0 | 0.0 | 4 | 13.3 | 0 | 0.0 | 6 | 20.0 | 1 | 3.3 | 0 | 0.0 | 0 | 0.0 | |
| Chi: 37.94; fd: 18; p-value: 0.004 | |||||||||||||||||||
| T7 (7 days) ** | CON | 14 | 46.7 | 5 | 16.7 | 2 | 6.7 | 3 | 10.0 | 1 | 3.3 | 4 | 13.3 | 1 | 3.3 | 0 | 0.0 | 0 | 0.0 |
| LF | 11 | 36.7 | 7 | 23.3 | 0 | 0.0 | 3 | 10.0 | 1 | 3.3 | 7 | 23.3 | 1 | 3.3 | 0 | 0.0 | 0 | 0.0 | |
| LO | 29 | 96.7 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 1 | 3.3 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | |
| INV | 12 | 40.0 | 9 | 30.0 | 0 | 0.0 | 4 | 13.3 | 0 | 0.0 | 4 | 13.3 | 1 | 3.3 | 0 | 0.0 | 0 | 0.0 | |
| Chi: 38.53; fd: 18; p-value: 0.003 | |||||||||||||||||||
| Time | Pain Intensity | Conventional (n = 30) | Low Friction (n = 30) | Lingual (n = 30) | Invisalign (n = 30) | ||||
|---|---|---|---|---|---|---|---|---|---|
| T4h * | N | % | N | % | N | % | N | % | |
| No pain | 0 | 0.0 | 6 | 20.0 | 7 | 23.3 | 1 | 3.3 | |
| Mild | 14 | 46.7 | 18 | 60.0 | 18 | 60.0 | 20 | 66.7 | |
| Moderate | 12 | 40.0 | 4 | 13.3 | 4 | 13.3 | 8 | 26.7 | |
| Intense | 4 | 13.3 | 2 | 6.7 | 1 | 3.3 | 1 | 3.3 | |
| Chi: 20.94; fd: 9; p-value: 0.013 | |||||||||
| T8h | No pain | 0 | 0.0 | 3 | 10.0 | 1 | 3.3 | 1 | 3.3 |
| Mild | 8 | 26.7 | 16 | 53.3 | 13 | 43.3 | 16 | 53.3 | |
| Moderate | 17 | 57.7 | 9 | 30.0 | 14 | 46.7 | 11 | 36.7 | |
| Intense | 5 | 16.7 | 2 | 6.7 | 2 | 6.7 | 2 | 6.7 | |
| Chi: 12.36; fd: 9; p-value: 0.19 | |||||||||
| T24h | No pain | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 |
| Mild | 8 | 26.7 | 12 | 40.0 | 11 | 36.7 | 11 | 36.7 | |
| Moderate | 18 | 60.0 | 10 | 33.3 | 18 | 60.0 | 16 | 53.3 | |
| Intense | 4 | 13.3 | 8 | 26.7 | 1 | 3.3 | 3 | 10.0 | |
| Chi: 10.13; fd: 6; p-value: 0.12 | |||||||||
| T2 | No pain | 0 | 0.0 | 0 | 0.0 | 4 | 13.3 | 2 | 6.7 |
| Mild | 13 | 43.3 | 10 | 33.3 | 14 | 46.7 | 12 | 40.0 | |
| Moderate | 12 | 40.0 | 13 | 43.3 | 11 | 36.7 | 14 | 46.7 | |
| Intense | 5 | 16.7 | 7 | 23.3 | 1 | 3.3 | 2 | 6.7 | |
| Chi: 14.55; fd: 9; p-value: 0.11 | |||||||||
| T3 ** | No pain | 1 | 3.3 | 3 | 3.3 | 10 | 3.3 | 3 | 10.0 |
| Mild | 16 | 53.3 | 18 | 60.0 | 17 | 56.7 | 14 | 46.7 | |
| Moderate | 9 | 30.0 | 6 | 20.0 | 3 | 10 | 11 | 36.7 | |
| Intense | 4 | 13.3 | 5 | 16.7 | 0 | 0.0 | 2 | 6.7 | |
| Chi: 25.57; fd: 9; p-value: 0.002 | |||||||||
| T4 ** | No pain | 5 | 16.7 | 2 | 6.7 | 14 | 46.7 | 3 | 10.0 |
| Mild | 15 | 50.0 | 18 | 60.0 | 15 | 50.0 | 22 | 73.3 | |
| Moderate | 6 | 20.0 | 8 | 26.7 | 1 | 3.3 | 4 | 13.3 | |
| Intense | 4 | 13.3 | 1 | 3.3 | 0 | 0.0 | 1 | 3.3 | |
| Chi: 31.52; fd: 12; p-value: 0.002 | |||||||||
| T5 ** | No pain | 7 | 23.3 | 7 | 23.3 | 19 | 63.3 | 3 | 10.0 |
| Mild | 16 | 53.3 | 18 | 60.0 | 11 | 36.7 | 23 | 76.7 | |
| Moderate | 17 | 23.3 | 5 | 16.7 | 0 | 0.0 | 0 | 0.0 | |
| Intense | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | |
| Chi: 26.85; fd: 6; p-valor: 0.00 | |||||||||
| T6 ** | No pain | 11 | 36.7 | 8 | 26.7 | 24 | 83.3 | 10 | 33.3 |
| Mild | 13 | 43.3 | 19 | 63.3 | 5 | 16.7 | 19 | 63.3 | |
| Moderate | 6 | 20.0 | 3 | 10 | 0 | 0.0 | 1 | 3.3 | |
| Intense | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | |
| Chi: 31.24; fd: 6; p-value: 0.00 | |||||||||
| T7 ** | No pain | 13 | 43.3 | 11 | 36.7 | 27 | 90.0 | 13 | 43.3 |
| Mild | 14 | 46.7 | 18 | 60.0 | 3 | 10.0 | 16 | 53.3 | |
| Moderate | 3 | 10 | 1 | 3.3 | 0 | 0.0 | 1 | 3.3 | |
| Intense | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | |
| Chi: 24.62; fd: 6; p-value: 0.00 | |||||||||
| Time | Type of Pain | Conventional (n = 30) | Low Friction (n = 30) | Lingual (n = 30) | Invisalign (n = 30) | ||||
|---|---|---|---|---|---|---|---|---|---|
| T4h ** | N | % | N | % | N | % | N | % | |
| No pain | 1 | 3.3 | 6 | 20,0 | 7 | 23.3 | 1 | 3.3 | |
| Acute | 2 A | 6.7 | 8 A,C | 26.7 | 13 C | 43.3 | 8 A,C | 26.7 | |
| Dull | 1 | 3.3 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | |
| Sensitive | 11 A,D | 36.7 | 3 A | 10.0 | 8 A,D | 26.7 | 13 D | 43.3 | |
| Throbbing | 6 | 20.0 | 4 | 13.3 | 1 | 3.3 | 4 | 13.3 | |
| Stabbing | 5 | 16.7 | 5 | 16.7 | 0 | 0.0 | 0 | 0.0 | |
| Other types of pain | 4 | 13.3 | 4 | 13.3 | 1 | 3.3 | 4 | 13.3 | |
| Chi: 49.16; fd: 27; p-value: 0.006 | |||||||||
| T8h ** | No pain | 0 | 0.0 | 3 | 10.0 | 1 | 3.3 | 0 | 0.0 |
| Acute | 4 | 13.3 | 12 | 40.0 | 13 | 43.3 | 7 | 23.3 | |
| Dull | 1 | 3.3 | 2 | 6.7 | 1 | 3.3 | 0 | 0.0 | |
| Sensitive | 11 B,D | 36.7 | 3 B | 10.0 | 10 B,D | 33.3 | 14 D | 46.7 | |
| Throbbing | 6 | 20.0 | 2 | 6.7 | 2 | 6.7 | 6 | 20.0 | |
| Stabbing | 6 | 20.0 | 5 | 16.7 | 0 | 0.0 | 0 | 0.0 | |
| Other types of pain | 2 | 6.7 | 3 | 10.0 | 3 | 10.0 | 3 | 10.0 | |
| Chi: 44.26; fd: 24; p-value: 0.007 | |||||||||
| T24h ** | No pain | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 |
| Acute | 4 A | 13.3 | 18C | 60.0 | 14 C | 46.7 | 10 A,C | 33.3 | |
| Dull | 1 | 3.3 | 3 | 10.0 | 1 | 3.3 | 2 | 6.7 | |
| Sensitive | 9 C | 30.0 | 0 B | 0.0 | 12 C | 40.0 | 11 C | 36.7 | |
| Throbbing | 8 | 26.7 | 1 | 3.3 | 2 | 6.7 | 4 | 13.3 | |
| Stabbing | 5 | 16.7 | 4 | 13.3 | 0 | 0.0 | 1 | 3.3 | |
| Other types of pain | 3 | 10.0 | 4 | 13.3 | 1 | 3.3 | 2 | 6.7 | |
| Chi: 48.59; fd: 24; p-value: 0.002 | |||||||||
| T2 ** | No pain | 0 | 0.0 | 0 | 0.0 | 4 | 13.3 | 2 | 6.7 |
| Acute | 3 A | 10.0 | 17 B | 56.7 | 10 A,B | 33.3 | 13 B | 43.3 | |
| Dull | 1 | 3.3 | 3 | 10.0 | 0 | 0.0 | 0 | 0.0 | |
| Sensitive | 8 B,C | 26.7 | 1 B | 3.3 | 13 C | 43.3 | 10 C | 33.3 | |
| Throbbing | 11 A | 36.7 | 1 C | 3.3 | 1 C | 3.3 | 4 A,C | 13.3 | |
| Stabbing | 4 | 13.3 | 4 | 13.3 | 1 | 3.3 | 0 | 0.0 | |
| Other types of pain | 3 | 10.0 | 4 | 13.3 | 1 | 3.3 | 1 | 3.3 | |
| Chi: 63.87; fd: 27; p-value: 0.000 | |||||||||
| T3 ** | No pain | 1 | 3.3 | 1 | 3.3 | 10 | 33.3 | 3 | 10.0 |
| Acute | 3 | 10.0 | 12 | 40.0 | 10 | 33.3 | 12 | 40.0 | |
| Dull | 1 | 3.3 | 9 | 30.0 | 0 | 0.0 | 0 | 0.0 | |
| Sensitive | 8 | 26.7 | 1 | 3.3 | 8 | 26.7 | 10 | 33.3 | |
| Throbbing | 9 | 30.0 | 0 | 0.0 | 1 | 3.3 | 3 | 10.0 | |
| Stabbing | 4 | 13.3 | 3 | 10.0 | 0 | 0.0 | 1 | 3.3 | |
| Other types of pain | 4 | 13.3 | 4 | 13.3 | 1 | 3.3 | 1 | 3.3 | |
| Chi: 89.91; fd: 30; p-value: 0.000 | |||||||||
| T4 ** | No pain | 5 A | 16.7 | 2 A | 6.7 | 14 C | 46.7 | 3 A,C | 10.0 |
| Acute | 2 A | 6.7 | 10 B | 33.3 | 7 A,B | 23.3 | 12 B | 40.0 | |
| Dull | 1 A | 3.3 | 9 B | 30.0 | 0 A | 0.0 | 0 A | 0.0 | |
| Sensitive | 8 B,D | 26.7 | 3 B | 10.0 | 7 B,D | 23.3 | 11 D | 36.7 | |
| Throbbing | 8 A | 26.7 | 0 C | 0.0 | 1 C | 3.3 | 2 A,C | 6.7 | |
| Stabbing | 5 | 16.7 | 4 | 13.3 | 1 | 3.3 | 0 | 0.0 | |
| Other types of pain | 1 | 3.3 | 2 | 6.7 | 0 | 0.0 | 2 | 6.7 | |
| Chi: 80.19; fd: 24; p-value: 0.000 | |||||||||
| T5 ** | No pain | 6 A | 20.0 | 7 C | 23.3 | 19 C | 63.3 | 3 A | 10.0 |
| Acute | 2 A | 6.7 | 8 A,D | 26.7 | 4 A,D | 13.3 | 12 D | 40.0 | |
| Dull | 1 B,C | 3.3 | 7 B | 23.3 | 0 C | 0.0 | 0 C | 0.0 | |
| Sensitive | 8 | 26.7 | 3 | 10.0 | 5 | 16.7 | 11 | 36.7 | |
| Throbbing | 9 A | 30.0 | 0 C | 0.0 | 1 C | 3.3 | 2 A,C | 6.7 | |
| Stabbing | 3 | 10.0 | 1 | 3.3 | 1 | 3.3 | 0 | 0.0 | |
| Other types of pain | 1 | 3.3 | 4 | 13.3 | 0 | 0.0 | 2 | 6.7 | |
| Chi: 79.99; fd: 24; p-value: 0.000 | |||||||||
| T6 ** | No pain | 11 A | 36.7 | 8 A | 26.7 | 25 C | 83.3 | 10 A | 33.3 |
| Acute | 3 | 10.0 | 8 | 26.7 | 2 | 6.7 | 6 | 20.0 | |
| Dull | 0 | 0.0 | 6 | 20.0 | 0 | 0.0 | 0 | 0.0 | |
| Sensitive | 6 B,D | 20.0 | 2 B | 6.7 | 2 B | 6.7 | 11 D | 36.7 | |
| Throbbing | 4 | 13.3 | 1 | 3.3 | 0 | 0.0 | 1 | 3.3 | |
| Stabbing | 2 | 6.7 | 2 | 6.7 | 1 | 3.3 | 1 | 3.3 | |
| Other types of pain | 4 | 13.3 | 3 | 10.0 | 0 | 0.0 | 1 | 3.3 | |
| Chi: 59.16; fd: 21; p-value: 0.000 | |||||||||
| T7 ** | No pain | 14 A | 46.7 | 12 A | 40.0 | 27 C | 90.0 | 13 A | 43.3 |
| Acute | 4 | 13.3 | 7 | 23.3 | 1 | 3.3 | 6 | 20.0 | |
| Dull | 0 | 0.0 | 4 | 13.3 | 0 | 0.0 | 0 | 0.0 | |
| Sensitive | 6 C,D | 20.0 | 1 C | 3.3 | 1 C | 3.3 | 9 D | 30.0 | |
| Throbbing | 4 | 13.3 | 1 | 3.3 | 0 | 0.0 | 1 | 3.3 | |
| Stabbing | 1 | 3.3 | 1 | 3.3 | 0 | 0.0 | 0 | 0.0 | |
| Other types of pain | 1 | 3.3 | 4 | 13.3 | 1 | 3.3 | 1 | 3.3 | |
| Chi: 50.36; fd: 21; p-value: 0.000 | |||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Antonio-Zancajo, L.; Montero, J.; Garcovich, D.; Alvarado-Lorenzo, M.; Albaladejo, A.; Alvarado-Lorenzo, A. Comparative Analysis of Periodontal Pain According to the Type of Precision Orthodontic Appliances: Vestibular, Lingual and Aligners. A Prospective Clinical Study. Biology 2021, 10, 379. https://doi.org/10.3390/biology10050379
Antonio-Zancajo L, Montero J, Garcovich D, Alvarado-Lorenzo M, Albaladejo A, Alvarado-Lorenzo A. Comparative Analysis of Periodontal Pain According to the Type of Precision Orthodontic Appliances: Vestibular, Lingual and Aligners. A Prospective Clinical Study. Biology. 2021; 10(5):379. https://doi.org/10.3390/biology10050379
Chicago/Turabian StyleAntonio-Zancajo, Laura, Javier Montero, Daniele Garcovich, Mario Alvarado-Lorenzo, Alberto Albaladejo, and Alfonso Alvarado-Lorenzo. 2021. "Comparative Analysis of Periodontal Pain According to the Type of Precision Orthodontic Appliances: Vestibular, Lingual and Aligners. A Prospective Clinical Study" Biology 10, no. 5: 379. https://doi.org/10.3390/biology10050379