
A Modelization of the Propagation of COVID-19 in Regions of Spain and Italy with Evaluation of the Transmission Rates Related to the Intervention Measures

 ,
,  , ,
, ,  ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. The Models
2.1. Non-Delayed Model
2.2. Delayed Model
3. Estimation of the Infectivity Rate
- In Italy, the lockdown began on 8 March in Lombardia and 14 provinces while on 10 March in the rest of the country, and it ended at 4 May.
- The lockdown in Spain took place from 15 March to 4 May.
- On 23 March there was a tightening of the measures, but we considered that the habits and the social contact were not altered enough to add another phase.
- Italy has a criteria for establishing the dates of de-escalating stages following the lockdown determined nationally, so in 18 May the whole country was in the phase 2, on 25 May in the phase 3, on 3 June in the phase 4 and on 15 June the normality was reached. However, in Spain it was independently chosen at each Autonomous Community until 21 June when the final phase ended in all the country.
4. Results
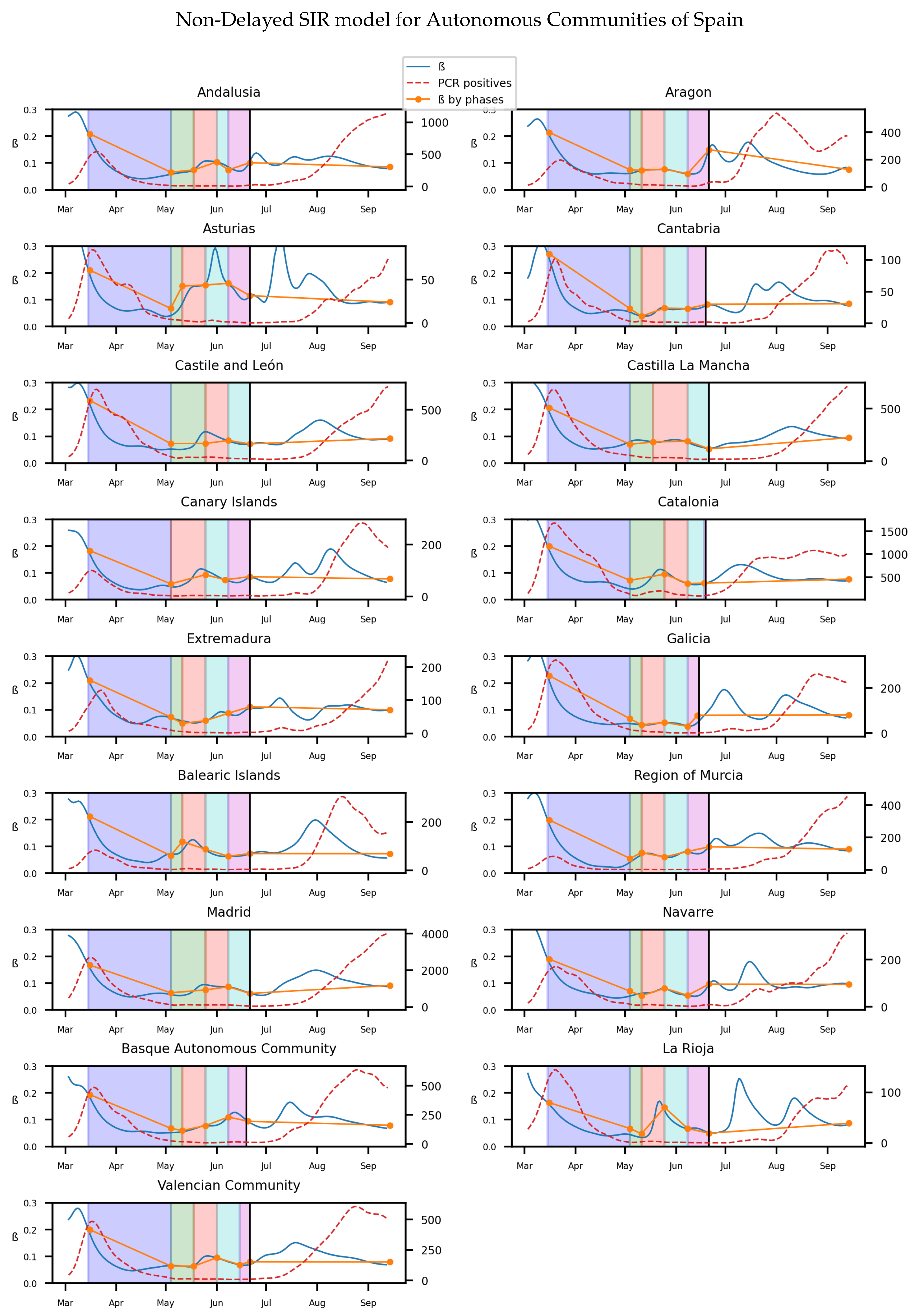
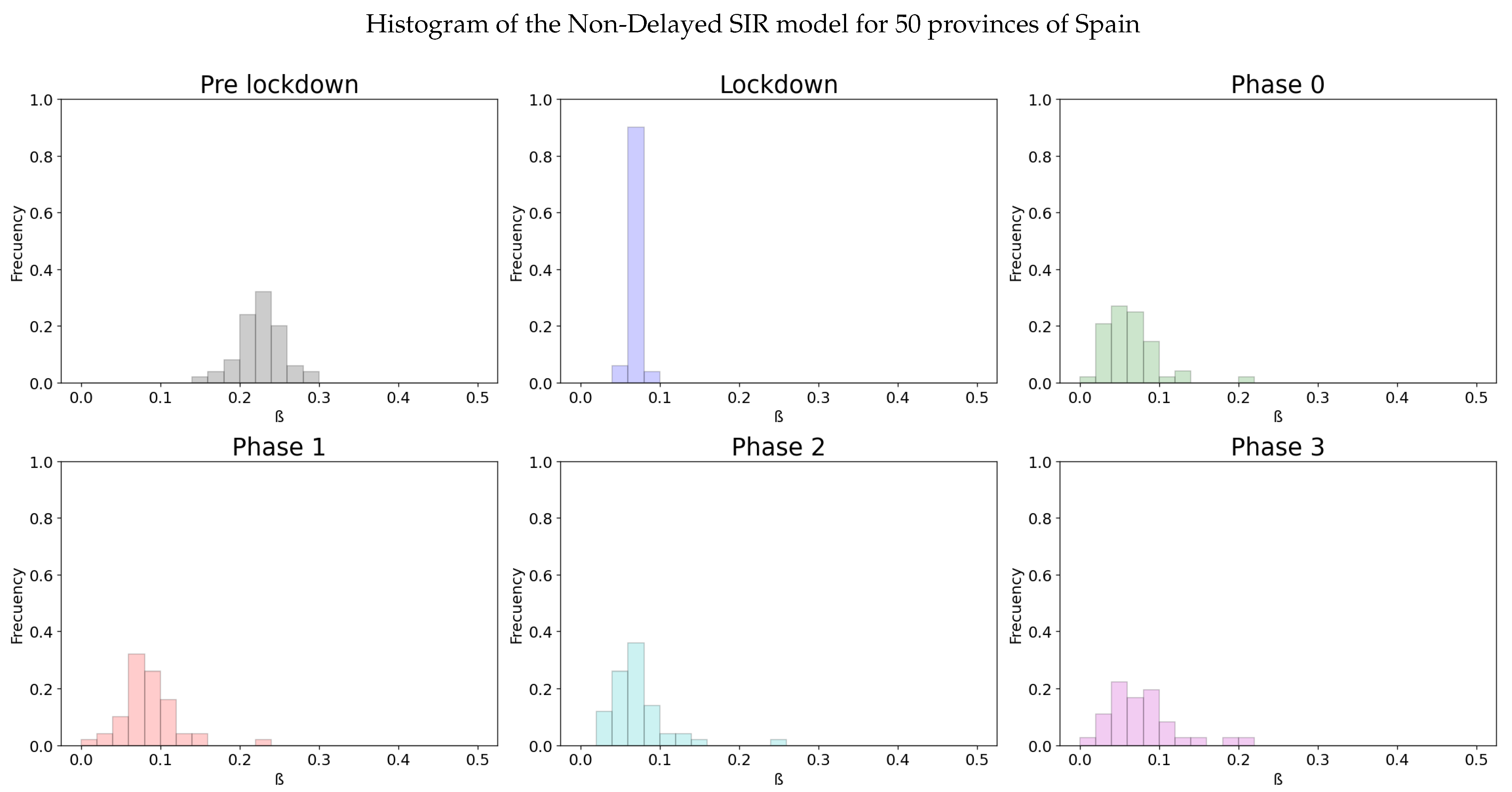
4.1. Non-Delayed SIR Model
4.2. Delayed SIR Model
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Singh, R.K.; Rani, M.; Bhagavathula, A.S.; Sah, R.; Rodriguez-Morales, A.J.; Kalita, H.; Nanda, C.; Sharma, S.; Sharma, Y.D.; Rabaan, A.A.; et al. Prediction of the COVID-19 Pandemic for the Top 15 Affected Countries: Advanced Autoregressive Integrated Moving Average (ARIMA) Model. JMIR Public Health Surveill 2020, 6, e19115. [Google Scholar] [CrossRef] [PubMed]
- Cotta, R.M.; NAveira-Cotta, C.P.; Magal, P. Mathematical Parameters of the COVID-19 Epidemic in Brazil and Evaluation of the Impact of Different Public Health Measures. Biology 2020, 9, 220. [Google Scholar] [CrossRef]
- Singh, R.K.; Drews, M.; De la Sen, M.; Kumar, M.; Singh, S.S.; Pandey, A.K.; Srivastava, P.K.; Dobriyal, M.; Rani, M.; Kumari, P.; et al. Short -Term Statistical forecasts of COVID-19 infections in India. IEEE Access 2020, 8, 186932–186938. [Google Scholar] [CrossRef]
- Li, M.Y.; Graef, J.R.; Wang, L.; Karsai, J. Global dynamics of a SEIR model with varying total population size. Math. Biosci. 1999, 160, 191–213. [Google Scholar] [CrossRef] [Green Version]
- Nistal, R.; De la Sen, M.; Alonso-Quesada, S.; Ibeas, A. On a New Discrete SEIADR Model with Mixed Controls: Study of Its Properties. Mathematics 2019, 7, 18. [Google Scholar] [CrossRef] [Green Version]
- Wang, X.; Wang, Z.; Shen, H. Dynamical analysis of a discrete-time SIS epidemic model on complex networks. Appl. Math. Lett. 2019, 94, 292–299. [Google Scholar] [CrossRef]
- Koide, C.; Seno, H. Sex ratio features of two-group SIR model for asymmetric transmission of heterosexual disease. Math. Comput. Model. 1996, 23, 67–91. [Google Scholar] [CrossRef]
- De la Sen, M.; Ibeas, A.; Alonso-Quesada, S.; Nistal, R. On a SIR Model in a Patchy Environment Under Constant and Feedback Decentralized Controls with Asymmetric Parameterizations. Symmetry 2019, 11, 430. [Google Scholar] [CrossRef] [Green Version]
- Bjørnstad, O.N.; Finkenstädt, B.F.; Grenfell, B.T. Dynamics of measles epidemics: Estimating scaling of transmission rates using a time series SIR model. Ecol. Monogr. 2002, 72, 169–184. [Google Scholar] [CrossRef] [Green Version]
- Berge, T.; Lubuma, J.S.; Moremedi, G.M.; Morris, N.; Kondera-Shava, R. A simple mathematical model for ebola in Africa. J. Biol. Dyn. 2017, 11, 42–74. [Google Scholar] [CrossRef] [Green Version]
- Shulgin, B.; Stone, L.; Agur, Z. Pulse vaccination strategy in the SIR epidemic model. Bull. Math. Biol. 1998, 60, 1123–1148. [Google Scholar] [CrossRef]
- Ambrosio, B.; Aziz-Alaoui, M.A. On a coupled time-dependent SIR models fiting with New York and New-Jersey states COVID-19 Data. Biology 2020, 9, 135. [Google Scholar] [CrossRef]
- McCallum, J.H. Barlow, N. How should pathogen transmission be modeled? Trends Ecol. Evol. 2001, 16, 295–300. [Google Scholar] [CrossRef]
- Rohani, P.; Keeling, M.J. Modeling Infectious Diseases in Humans and Animals; Princeton University Press: Princeton, NJ, USA, 2008. [Google Scholar]
- D’Onofrio, A. Stability properties of pulse vaccination strategy in SEIR epidemic model. Math. Biosci. 2002, 179, 57–72. [Google Scholar] [CrossRef]
- Shend, Q.; Zhang, X.; Fan, B.; Wang, C.; Zeng, B.; Li, Z.; Li, X.; Li, H.; Long, C.; Xuc, H. Diagnosis of the Coronavirus disease (covid-19): RRT-PCR or CT? Eur. J. Radiol. 2020, 126, 108961. [Google Scholar]
- Rohrer, K.; Bajnoczki, C.; Socha, A.; Voss, M.; Nicod, M.; Ridde, V.; Koonin, J.; Rajan, D.; Koch, K. Governance of the Covid-19 response: A call for more inclusive and transparent decision-making. BMJ Glob. Health 2020, 5, e002655. Available online: https://gh.bmj.com/content/5/5/e002655 (accessed on 5 October 2020).
- Barton, C.M.; Alberti, M.; Ames, D.; Atkinson, J.A.; Bales, J.; Burke, E.; Chen, M.; Diallo, S.Y.; Earn, D.J.; Fath, B.; et al. Call for transparency of COVID-19 models. Science 2020, 368, 482–483. [Google Scholar] [PubMed]
- Stokes, L.S.; Pierce, R.; Aronoff, D.M.; McPheeters, M.L.; Omary, R.A.; Spalluto, L.B.; Planz, V.B. Transparency and trust during the Coronavirus disease 2019 (Covid-19) Pandemic. J. Am. Coll. Radiol. 2020, 17, 909–912. [Google Scholar]
- De la Sen, M.; Ibeas, A.; Alonso-Quesada, S. On vaccination controls for the SEIR epidemic model. Commun. Nonlinear Sci. Numer. Simul. 2012, 17, 2637–2658. [Google Scholar] [CrossRef]
- Tang, B.; Scarabel, F.; Bragazzi, N.L.; McCarthy, Z.; Glazer, M.; Xiao, Y.; Heffernan, J.M.; Asgary, A.; Ogden, N.H.; Wu, J. De-Escalation by reversing the escalation with a stronger synergistic package of contact tracing, quarantine, isolation and personal protection: Feasibility of preventing a COVID-19 rebound in Ontario, Canada, as case study. Biology 2020, 9, 100. [Google Scholar] [CrossRef]
- Roussel, L. La famille en Europe occidentale: Divergences et convergences. Population 1992, 47, 133–152. [Google Scholar] [CrossRef]
- Rhodes, A.; Ferdinande, P.; Flaatten, H.; Guidet, B.; Metnitz, P.G.; Moreno, R.P. The variability of critical care bed numbers in Europe. Intensive Care Med. 2012, 38, 1647–1653. [Google Scholar] [CrossRef] [Green Version]
- Available online: https://www.ine.es/covid/piramides.htm (accessed on 5 October 2020).
- Available online: https://www.tuttitalia.it/statistiche/indici-demografici-struttura-popolazione/ (accessed on 5 October 2020).
- Gandhi, R.T.; Lynch, J.B.; Del Rio, C. Mild or moderate Covid-19. N. Engl. J. Med. 2020, 383, 1757–1766. [Google Scholar] [CrossRef]
- Tang, B.; Wang, X.; Li, Q.; Bragazzi, N.L.; Tang, S.; Xiao, Y.; Wu, J. Estimation of the transmission risk of the 2019- Covid and its implication for public health interventions. J. Clin. Med. 2020, 9, 462. [Google Scholar] [CrossRef] [Green Version]
- Tang, B.; Bragazzi, N.L.; Li, Q.; Tang, S.; Xiao, Y.; Wu, J. An updated estimation of the risk of transmission of the novel Coronavirus (2019-nCov). Infect. Dis. Model. 2020, 5, 248–255. [Google Scholar] [CrossRef] [PubMed]
- Chen, N.; Zhou, M.; Dong, X.; Qu, J.; Gong, F.; Han, Y.; Qiu, Y.; Wang, J.; Liu, Y.; Wei, Y.; et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: A descriptive study. Lancet 2020, 395, 507–513. [Google Scholar] [CrossRef] [Green Version]
- Lauer, S.A.; Grantz, K.H.; Bi, Q.; Jones, F.K.; Zheng, Q.; Meredith, H.R.; Azman, A.S.; Reich, N.G.; Lessler, J. The Incubation Period of Coronavirus Disease 2019 (COVID-19) From Publicly Reported Confirmed Cases: Estimation and Application. Ann Intern Med. 2020, 172, 577–582. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spanish Database. Available online: https://cnecovid.isciii.es/covid19 (accessed on 5 October 2020).
- Italian Database. Available online: https://github.com/pcm-dpc/covid-19 (accessed on 5 October 2020).
- Bassetti, S.; Bischoff, W.E.; Sheretz, R.J. Are SARS superspreaders cloud adults? Emerg. Inf. Dis. 2005, 11, 637–638. [Google Scholar] [CrossRef]
- Lowen, A.C.; Mubareka, S.; Steel, J.; Palese, P. Influenza Virus Transm. Is Depend. Relat. Humidity Temp. PLoS Pathog. 2007, 3, e151. [Google Scholar] [CrossRef] [PubMed]
- Spain Lockdown Plan. Available online: https://www.ecestaticos.com/file/586e3fe4193e6c9f05dca2c2e757b0c7/1588103416-plan-de-transicion-hacia-la-nueva-normalidad.pdf (accessed on 5 October 2020).
- Available online: https://www.unipd.it/sites/unipd.it/files/2020/DPCM-1-marzo-2020.pdf (accessed on 5 October 2020).
- Marcus, B.P. The weighted moving average technique. In Wiley Encyclopedia of Operations Research and Management Science; Wiley Online Library: Hoboken, NJ, USA, 2010. [Google Scholar]
- Italian Official Repository. Available online: http://www.salute.gov.it/portale/news/p3_2_1_1_1.jsp?lingua=italiano&menu=notizie&p=dalministero&id=5077 (accessed on 5 October 2020).
- Montgomery, D.C.; Runger, G.C. Applied Statistics and Probability for Engineers; John Wiley & Sons: Hoboken, NJ, USA, 2010. [Google Scholar]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Phase | Mean | Variance | CI 95% | p-Value |
|---|---|---|---|---|
| Pre-lockdown | 0.36727 | 0.03821 | (0.33023, 0.40431) | |
| Lockdown | 0.07599 | 0.00004 | (0.07482, 0.07716) | 0.0 |
| Phase 1 | 0.05348 | 0.00059 | (0.04889, 0.05807) | 0.0 |
| Phase 2 | 0.08338 | 0.03196 | (0.04951, 0.11726) | 0.10092 |
| Phase 3 | 0.06078 | 0.00447 | (0.04811, 0.07344) | 0.23762 |
| Phase 4 | 0.08749 | 0.00973 | (0.06881, 0.10618) | 0.01099 |
| Normality | 0.09013 | 0.00093 | (0.08435, 0.09591) | 0.26908 |
| Phase | Mean | Variance | CI 95% | p-Value |
|---|---|---|---|---|
| Pre-lockdown | 0.22883 | 0.00078 | (0.22111, 0.23655) | |
| Lockdown | 0.071 | 0.00004 | (0.06936, 0.07264) | 0.0 |
| Phase 0 | 0.07945 | 0.01179 | (0.04935, 0.10954) | 0.92041 |
| Phase 1 | 0.08555 | 0.00125 | (0.07574, 0.09536) | 0.66039 |
| Phase 2 | 0.07239 | 0.0013 | (0.06239, 0.08239) | 0.68447 |
| Phase 3 | 0.07887 | 0.00192 | (0.06672, 0.09102) | 0.71008 |
| Normality | 0.11245 | 0.00291 | (0.09749, 0.12741) | 0.00067 |
| Phase | Mean | Variance | CI 95% | p-Value |
|---|---|---|---|---|
| Pre-lockdown | 0.83841 | 0.30304 | (0.7341, 0.94272) | |
| Lockdown | 0.07157 | 0.00007 | (0.06995, 0.0732) | 0.0 |
| Phase 1 | 0.04437 | 0.00062 | (0.03965, 0.04908) | 0.0 |
| Phase 2 | 0.07041 | 0.00927 | (0.05216, 0.08865) | 0.00865 |
| Phase 3 | 0.05583 | 0.00558 | (0.04168, 0.06999) | 0.21103 |
| Phase 4 | 0.07355 | 0.008 | (0.05661, 0.0905) | 0.06891 |
| Normality | 0.09549 | 0.00226 | (0.08649, 0.1045) | 0.00093 |
| Phase | Mean | Variance | CI 95% | p-Value |
|---|---|---|---|---|
| Pre-lockdown | 0.40061 | 0.00508 | (0.38086, 0.42037) | |
| Lockdown | 0.06661 | 0.00004 | (0.06477, 0.06844) | 0.0 |
| Phase 0 | 0.06163 | 0.00401 | (0.04407, 0.0792) | 0.2545 |
| Phase 1 | 0.0791 | 0.00123 | (0.06938, 0.08882) | 0.11963 |
| Phase 2 | 0.06847 | 0.00152 | (0.05766, 0.07929) | 0.59498 |
| Phase 3 | 0.07881 | 0.00315 | (0.06326, 0.09436) | 0.30296 |
| Normality | 0.13141 | 0.00821 | (0.1063, 0.15652) | 0.00033 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nistal, R.; de la Sen, M.; Gabirondo, J.; Alonso-Quesada, S.; Garrido, A.J.; Garrido, I. A Modelization of the Propagation of COVID-19 in Regions of Spain and Italy with Evaluation of the Transmission Rates Related to the Intervention Measures. Biology 2021, 10, 121. https://doi.org/10.3390/biology10020121
Nistal R, de la Sen M, Gabirondo J, Alonso-Quesada S, Garrido AJ, Garrido I. A Modelization of the Propagation of COVID-19 in Regions of Spain and Italy with Evaluation of the Transmission Rates Related to the Intervention Measures. Biology. 2021; 10(2):121. https://doi.org/10.3390/biology10020121
Chicago/Turabian StyleNistal, Raul, Manuel de la Sen, Jon Gabirondo, Santiago Alonso-Quesada, Aitor J. Garrido, and Izaskun Garrido. 2021. "A Modelization of the Propagation of COVID-19 in Regions of Spain and Italy with Evaluation of the Transmission Rates Related to the Intervention Measures" Biology 10, no. 2: 121. https://doi.org/10.3390/biology10020121