
BreastNet18: A High Accuracy Fine-Tuned VGG16 Model Evaluated Using Ablation Study for Diagnosing Breast Cancer from Enhanced Mammography Images

 , , ,
, , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Research Aim and Scope
- Initially, artefacts and noise presented in raw mammograms are removed by applying noise reduction and data pre-processing algorithms, the quality of the mammograms is improved and the breast lesion emphasized with different data enhancement methods.
- Preprocessing algorithms and their parameter values which result in the best outcome, after experimentation with our dataset, are selected.
- Statistical analysis such as MSE, PSNR, SSIM, RMSE, and histogram analysis is performed on the pre-processed images to ensure the quality and pixel information has not deteriorated.
- The number of mammograms is increased eight times using seven data augmentation techniques to deal with overfitting issues and the dataset is split into train, validation, and test sets.
- Pre-trained networks namely VGGNet16, VGGNet19, ResNet50, InceptionV3, MobileNetV2, and DenseNet201 are modified by fine-tuning the model’s final layers to determine the best classifier for the augmented dataset.
- BreastNet18 model is proposed based on a fine-tuned VGG16 architecture after thorough experimentation with our dataset as it yields the highest accuracy among the pre-trained models.
- An ablation study is conducted on the proposed model in order to improve its classification performance.
- To avoid the possibility of overfitting, the model is evaluated by employing k-fold cross validation technique.
- Once the model offers adequate performance, to further investigate the robustness, it is tested on a noise induced dataset.
3. Literature Review
4. Dataset
5. Image Preprocessing Techniques
5.1. Artefacts Removal
5.1.1. Binary Masking
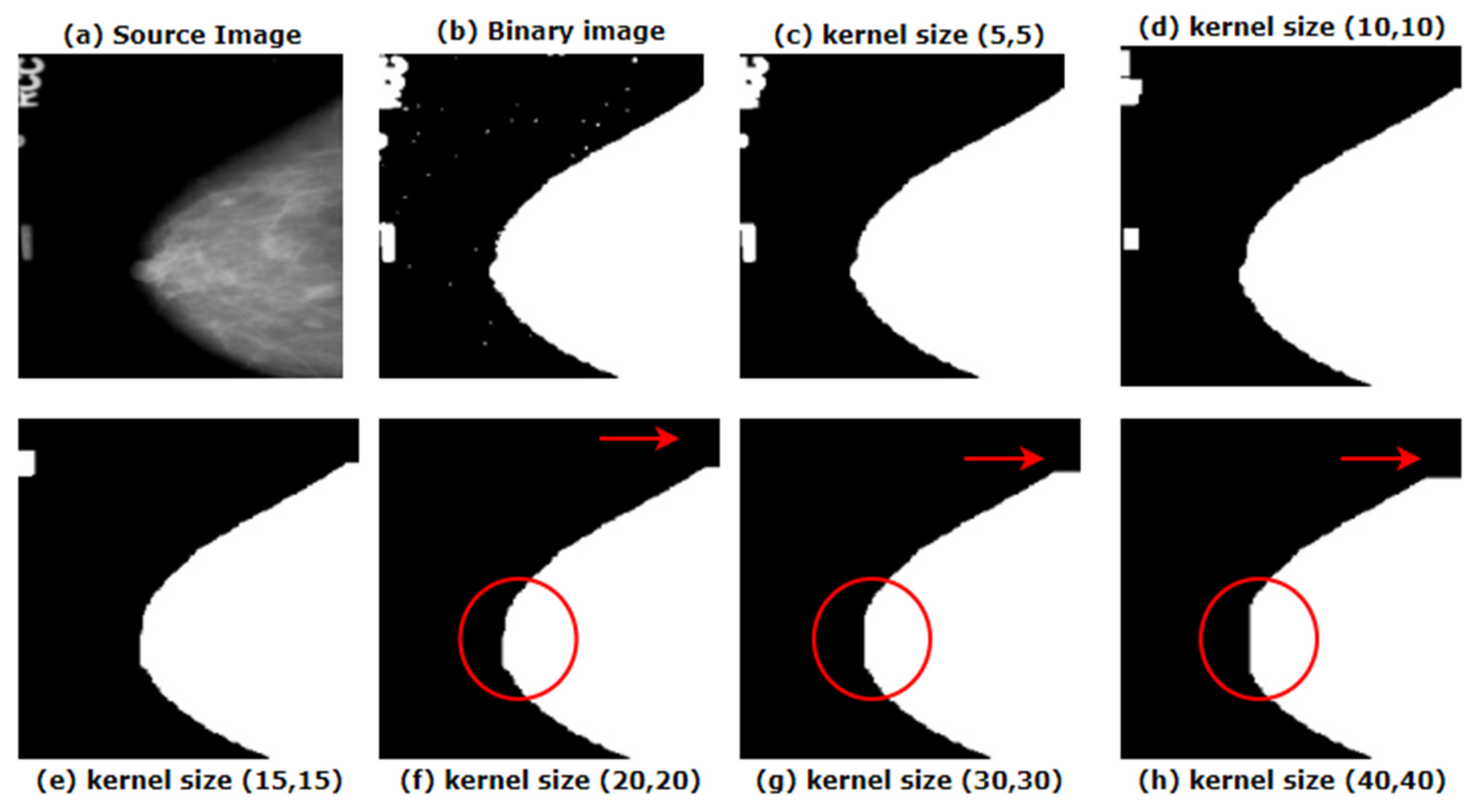
5.1.2. Morphological Opening
| Algorithm 1 Binary thresholding |
| 1. START |
| 2. READ source image, s(x,y) where x and y denotes the pixel coordinates |
| 3. threshold value, t = 127 |
| 4. maximum value, m = 255 |
| 5. FOR pixel in s(x,y): |
| 6. IF s[pixel] < t: |
| 7. s[pixel] = 0 |
| 8. ELSE |
| 9. s[pixel] = 255 |
| 10. END IF |
| 11. END FOR |
| 12. END |
| Algorithm 2 Morphological opening |
| 1. BEGIN |
| 2. VOID open1d(image,u) { |
| 3. FOR i in 1,length(image.lines) do |
| 4. line = image.lines[i] |
| 5. filtered = [] |
| 6. FOR j in 1,length(line.runs) do |
| 7. if runs[j].width() >= u then |
| 8. filtered.append(line.runs[j]) |
| 9. ENDFOR |
| 10. image.lines[i] = filtered |
| 11. ENDFOR |
| 12. END |
5.1.3. Largest Contour Detection
5.2. Remove Line
5.2.1. InRange Operation
5.2.2. Gabor Filter
| Algorithm 3 Pseudo-code of Gabor feature extraction |
| 1. BEGIN |
| 2. FOR each frequency f in the frequency list f_list: |
| 3. FOR each orientation φ in the orientation list o_list DO |
| 4. Construct a gabor filter g(f, φ), |
| 5. Convolve g(f, φ) with original image I, get response image R, |
| 6. Compute the mean (m) response in R, |
| 7. Count the # of pixels Np that have a larger value than m, |
| 8. Divide R into X x Y frames, |
| 9. FOR i in range(1,X); |
| 10. FOR j in range(1,Y): |
| 11. Count the # of strong response Ni,j and Compute the ratio r: |
| 12. r = Ni,j/Nr; |
| 13. Append r to the feature vector z: |
| 14. Finally, z = [r1,r2,…r|f_list|*|o_list|*X*Y]. |
| 15. END |
5.2.3. Morphological Operations
Opening
Dilation
5.2.4. Inverse Mask
5.3. Image Enhancement
5.3.1. Gamma Correction
- g = 1 means no effect.
- g < 1 means darkening the details.
5.3.2. Results of the First CLAHE
| Algorithm 4 CLAHE |
| Input: Image after gamma correction I; |
| 1. Resizing l to N × N; Decompose l—(n) tiles; (n)—N × N/n × n |
| 2. Hm—histogram(m); // histogram of a n × n tile; |
| 3. Clip limit: CL—Ncl × Navg of Hn using CL; |
| 4. pixels—distribution over the remaining pixels; |
| 5. CLAHE(n)—equalization of contrast limited the histogram tile histogram for the image(l) |
| 6. bc—bilinear interpolation of CLAHE |
| Output: CLAHE processed image bc |
5.3.3. Outputs after Applying CLAHE a Second Time
5.3.4. Green Fire Blue
5.4. Verification
5.4.1. MSE
5.4.2. PSNR
5.4.3. SSIM
5.4.4. RMSE
5.4.5. Histogram Analysis
6. Data Augmentation
6.1. Data Augmentation
6.2. Data Split
7. Proposed Model
7.1. Transfer Learning and ImageNet
7.2. Transfer Learning Model and Finetuning
7.2.1. MobileNetV2
7.2.2. ResNet50
7.2.3. InceptionV3
7.2.4. DenseNet201
7.2.5. VGG16
7.2.6. VGG19
7.3. Training Approach
7.4. BreastNet18
7.5. Ablation Study
8. Results and Discussion
8.1. Evaluation Matrix
8.2. Results of Transfer Learning Models
8.2.1. Statistical Analysis of the Models
8.2.2. Comparison among the Models Based on Layer Depth and Trainable Parameters
8.3. Results of Ablation Study
8.3.1. Ablation Study 1: Changing Flatten Layer
8.3.2. Ablation Study 2: Changing Batch Size
8.3.3. Ablation Study 3: Changing Loss Functions
8.3.4. Ablation Study 4: Changing Optimizer and Learning Rates
8.3.5. Ablation Study Based on Different ImageJ Filters
8.3.6. Ablation Study Based on Image Processing Algorithms
8.4. Performance Analysis of Best Model
8.5. Check on Overfitting
8.6. Evaluation on Noise Induced Test Set
8.7. Comparison with Previous Literature
9. Limitations
10. Contribution of This Study
11. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2017. CA Cancer J. Clin. 2017, 67, 7–30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Torre, L.A.; Bray, F.; Siegel, R.L.; Ferlay, J.; Lortet-Tieulent, J.; Jemal, A. Global cancer statistics, 2012. CA Cancer J. Clin. 2015, 65, 87–108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barbieri, R.L.; Strauss, J.F. Yen Jaffe’s Reproductive Endocrinology: Physiology, Pathophysiology, and Clinical Management, 8th ed.; Elsevier: Amsterdam, The Netherlands, 2019; Volume 419, pp. 248–255.e3. [Google Scholar] [CrossRef]
- Ragab, D.A.; Sharkas, M.; Marshall, S.; Ren, J. Breast cancer detection using deep convolutional neural networks and support vector machines. Peer. J 2019, 7, e6201. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Zhuang, S.; Li, D.-A.; Zhao, J.; Ma, Y. Benign and malignant classification of mammogram images based on deep learning. Biomed. Signal. Process. Control. 2019, 51, 347–354. [Google Scholar] [CrossRef]
- Ghosh, P.; Karim, A.; Azam, S.; Jonkman, M.; Hasib, K.M.; Anwar, A. A performance based study on deep learning algorithms in the effective prediction of breast cancer. In Proceedings of the 2021 International Joint Conference on Neural Networks (IJCNN), Shenzhen, China, 18–22 July 2021; pp. 1–8. [Google Scholar] [CrossRef]
- Labrèche, F.; Goldberg, M.S.; Hashim, D.; Weiderpass, E. Breast Cancer. Occup. Cancers 2020, 417–438. [Google Scholar] [CrossRef]
- Friedberg, E.B.; Corn, D.; Prologo, J.D.; Fleishon, H.; Pyatt, R.; Duszak, R.; Cook, P. Access to Interventional Radiology Services in Small Hospitals and Rural Communities: An ACR Membership Intercommission Survey. J. Am. Coll. Radiol. 2019, 16, 185–193. [Google Scholar] [CrossRef]
- Beeravolu, A.R.; Azam, S.; Jonkman, M.; Shanmugam, B.; Kannoorpatti, K.; Anwar, A. Preprocessing of Breast Cancer Images to Create Datasets for Deep-CNN. IEEE Access 2021, 9, 33438–33463. [Google Scholar] [CrossRef]
- Sickles, E.A. Breast Cancer Screening Outcomes in Women Ages 40-49: Clinical Experience with Service Screening Using Modern Mammography. J. Natl. Cancer Inst. Monogr. 1997, 1997, 99–104. [Google Scholar] [CrossRef] [PubMed]
- Tang, J.; Rangayyan, R.; Xu, J.; El Naqa, I.; Yang, Y. Computer-Aided Detection and Diagnosis of Breast Cancer with Mammography: Recent Advances. IEEE Trans. Inf. Technol. Biomed. 2009, 13, 236–251. [Google Scholar] [CrossRef]
- Rangayyan, R.M.; Banik, S.; Desautels, J.E.L. Computer-Aided Detection of Architectural Distortion in Prior Mammograms of Interval Cancer. J. Digit. Imaging 2010, 23, 611–631. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Africano, G.; Arponen, O.; Sassi, A.; Rinta-Kiikka, I.; Laaperi, A.L.; Pertuz, S. A new benchmark and method for the evaluation of chest wall detection in digital mammography. In Proceedings of the 2020 42nd Annual International Conference of the IEEE Engineering in Medicine & Biology Society (EMBC), Montreal, QC, Canada, 20–24 July 2020; pp. 1132–1135. [Google Scholar] [CrossRef]
- Ferrari, R.J.; Rangayyan, R.; Desautels, J.; Borges, R.; Frere, A. Automatic Identification of the Pectoral Muscle in Mammograms. IEEE Trans. Med. Imaging 2004, 23, 232–245. [Google Scholar] [CrossRef]
- Comelli, A.; Bruno, A.; Di Vittorio, M.L.; Ienzi, F.; Lagalla, R.; Vitabile, S.; Ardizzone, E. Automatic Multi-seed Detection for MR Breast Image Segmentation. Lect. Notes Compu. Sci. 2017, 10484, 706–717. [Google Scholar] [CrossRef]
- Burt, J.R.; Torosdagli, N.; Khosravan, N.; Raviprakash, H.; Mortazi, A.; Tissavirasingham, F.; Hussein, S.; Bagci, U. Deep learning beyond cats and dogs: Recent advances in diagnosing breast cancer with deep neural networks. Br. J. Radiol. 2018, 91, 20170545. [Google Scholar] [CrossRef] [PubMed]
- Shuyue, G.; Murray, L. Breast cancer detection using transfer learning in convolutional neural networks. In Proceedings of the 2017 IEEE Applied Imagery Pattern Recognition Workshop (AIPR), Washington, DC, USA, 10–12 October 2017; pp. 1–8. [Google Scholar] [CrossRef]
- Khamparia, A.; Bharati, S.; Podder, P.; Gupta, D.; Khanna, A.; Phung, T.K.; Thanh, D.N.H. Diagnosis of breast cancer based on modern mammography using hybrid transfer learning. Multidimens. Syst. Signal. Process. 2021, 32, 747–765. [Google Scholar] [CrossRef] [PubMed]
- Mahmood, T.; Li, J.; Pei, Y.; Akhtar, F. An Automated In-Depth Feature Learning Algorithm for Breast Abnormality Prognosis and Robust Characterization from Mammography Images Using Deep Transfer Learning. Biology 2021, 10, 859. [Google Scholar] [CrossRef] [PubMed]
- Wang, P.; Wang, J.; Li, Y.; Li, P.; Li, L.; Jiang, M. Automatic classification of breast cancer histopathological images based on deep feature fusion and enhanced routing. Biomed. Signal. Process. Control 2021, 65, 102341. [Google Scholar] [CrossRef]
- Song, R.; Li, T.; Wang, Y. Mammographic Classification Based on XGBoost and DCNN with Multi Features. IEEE Access 2020, 8, 75011–75021. [Google Scholar] [CrossRef]
- Hameed, Z.; Zahia, S.; Garcia-Zapirain, B.; Javier Aguirre, J.; María Vanegas, A. Breast Cancer Histopathology Image Classification Using an Ensemble of Deep Learning Models. Sensors 2020, 20, 4373. [Google Scholar] [CrossRef]
- Khan, H.N.; Shahid, A.R.; Raza, B.; Dar, A.H.; Alquhayz, H. Multi-View Feature Fusion Based Four Views Model for Mammogram Classification Using Convolutional Neural Network. IEEE Access 2019, 7, 165724–165733. [Google Scholar] [CrossRef]
- Wang, Z.; Li, M.; Wang, H.; Jiang, H.; Yao, Y.; Zhang, H.; Xin, J. Breast Cancer Detection Using Extreme Learning Machine Based on Feature Fusion with CNN Deep Features. IEEE Access 2019, 7, 105146–105158. [Google Scholar] [CrossRef]
- Shallu; Mehra, R. Breast cancer histology images classification: Training from scratch or transfer learning? ICT Express 2018, 4, 247–254. [Google Scholar] [CrossRef]
- Ribli, D.; Horváth, A.; Unger, Z.; Pollner, P.; Csabai, I. Detecting and classifying lesions in mammograms with Deep Learning. Sci. Rep. 2018, 8, 4165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kooi, T.; Litjens, G.; van Ginneken, B.; Gubern-Mérida, A.; Sánchez, C.I.; Mann, R.; Heeten, A.D.; Karssemeijer, N. Large scale deep learning for computer aided detection of mammographic lesions. Med. Image Anal. 2017, 35, 303–312. [Google Scholar] [CrossRef] [PubMed]
- Al-Antari, M.A.; Al-Masni, M.A.; Choi, M.-T.; Han, S.-M.; Kim, T.-S. A fully integrated computer-aided diagnosis system for digital X-ray mammograms via deep learning detection, segmentation, and classification. Int. J. Med. Inf. 2018, 117, 44–54. [Google Scholar] [CrossRef] [PubMed]
- Jiao, Z.; Gao, X.; Wang, Y.; Li, J. A deep feature based framework for breast masses classification. Neurocomputing 2016, 197, 221–231. [Google Scholar] [CrossRef]
- Wang, X.; Liang, G.; Zhang, Y.; Blanton, H.; Bessinger, Z.; Jacobs, N. Inconsistent Performance of Deep Learning Models on Mammogram Classification. J. Am. Coll. Radiol. 2020, 17, 796–803. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paquin, F.; Rivnay, J.; Salleo, A.; Stingelin, N.; Silva, C. Multi-phase semicrystalline microstructures drive exciton dissociation in neat plastic semiconductors. J. Mater. Chem. C 2015, 3, 10715–10722. [Google Scholar] [CrossRef] [Green Version]
- Jadoon, M.M.; Zhang, Q.; Haq, I.U.; Butt, S.; Jadoon, A. Three-Class Mammogram Classification Based on Descriptive CNN Features. BioMed Res. Int. 2017, 2017, 3640901. [Google Scholar] [CrossRef] [Green Version]
- Gardezi, S.J.S.; Awais, M.; Faye, I.; Meriaudeau, F. Mammogram classification using deep learning features. In Proceedings of the 2017 IEEE International Conference on Signal and Image Processing Applications (ICSIPA), Kuching, Malaysia, 12–14 September 2017; pp. 485–488. [Google Scholar] [CrossRef]
- Bruno, A.; Ardizzone, E.; Vitabile, S.; Midiri, M. A Novel Solution Based on Scale Invariant Feature Transform Descriptors and Deep Learning for the Detection of Suspicious Regions in Mammogram Images. J. Med. Signals Sens. 2020, 10, 158–173. [Google Scholar] [CrossRef]
- The Cancer Imaging Archive (TCIA) Public Access, URL. Available online: https://wiki.cancerimagingarchive.net/display/Public/CBIS-DDSM (accessed on 11 December 2021).
- Breuel, T.M. Efficient Binary and Run Length Morphology and its Application to Document Image Processing. arXiv 2007, arXiv:0712.0121. [Google Scholar]
- Gong, X.Y.; Su, H.; Xu, D.; Zhang, Z.T.; Shen, F.; Yang, H. Bin an Overview of Contour Detection Approaches. Int. J. Autom. Comput. 2018, 15, 656–672. [Google Scholar] [CrossRef]
- Nikolskaia, K.; Ezhova, N.; Sinkov, A.; Medvedev, M. Skin Detection Technique Based on HSV Color Model and SLIC Segmentation Method. In Proceedings of the 4th Ural Workshop on Parallel, Distributed and Cloud Computing for Young Scientists (Ural-PDC), Yekaterinburg, Russia, 15 November 2018; Volume 2281, pp. 123–135. [Google Scholar]
- Zheng, Y. Breast Cancer Detection with Gabor Features from Digital Mammograms. Algorithms 2010, 3, 44–62. [Google Scholar] [CrossRef]
- Van Droogenbroeck, M.; Buckley, M.J. Morphological Erosions and Openings: Fast Algorithms Based on Anchors. J. Math. Imaging Vis. 2005, 22, 121–142. [Google Scholar] [CrossRef]
- Dhar, P. A Method to Detect Breast Cancer Based on Morphological Operation. Int. J. Educ. Manag. Eng. 2021, 11, 25–31. [Google Scholar] [CrossRef]
- Hassan, N.; Ullah, S.; Bhatti, N.; Mahmood, H.; Zia, M. The Retinex based improved underwater image enhancement. Multimed. Tools Appl. 2021, 80, 1839–1857. [Google Scholar] [CrossRef]
- Ahmed, N.; Yigit, A.; Isik, Z.; Alpkocak, A. Identification of Leukemia Subtypes from Microscopic Images Using Convolutional Neural Network. Diagnostics 2019, 9, 104. [Google Scholar] [CrossRef] [Green Version]
- Chen, J.; Cao, H.; Prasad, R.; Bhardwaj, A.; Natarajan, P. Gabor features for offline Arabic handwriting recognition. In Proceedings of the DAS ‘10: Proceedings of the 9th IAPR International Workshop on Document Analysis Systems, Boston, MA, USA, 9–11 June 2010; pp. 53–58. [Google Scholar] [CrossRef]
- Abbas, A.H.; Kareem, A.A.; Kamil, M.Y. Breast Cancer Image Segmentation Using Morphological Operations. Int. J. Electron. Commun. Eng. Technol. 2015, 6, 8–14. [Google Scholar]
- Lestari, W.; Sumarlinda, S. Application of Mathematical Morphology Algorithm for Image Enhancement of Breast Cancer Detection. In Proceedings of the 1st International Conference of Health, Science & Technology (ICOHETECH), Solo, Indonesia, 16 November 2019; pp. 187–189. [Google Scholar]
- Gupta, S.; Sinha, N.; Sudha, R.; Babu, C. Breast Cancer Detection Using Image Processing Techniques. In Proceedings of the IEEE 2019 Innovations in Power and Advanced Computing Technologies (i-PACT), Vellore, India, 22–23 March 2019. [Google Scholar]
- Menon, L.T.; Laurensi, I.A.; Penna, M.C.; Oliveira, L.E.S.; Britto, A.S. Data Augmentation and Transfer Learning Applied to Charcoal Image Classification. In Proceedings of the 2019 International Conference on Systems, Signals and Image Processing (IWSSIP), Osijek, Croatia, 5–7 June 2019; pp. 69–74. [Google Scholar] [CrossRef]
- Falconi, L.G.; Perez, M.; Aguilar, W.G.; Conci, A. Transfer Learning and Fine Tuning in Breast Mammogram Abnormalities Classification on CBIS-DDSM Database. Adv. Sci. Technol. Eng. Syst. J. 2020, 5, 154–165. [Google Scholar] [CrossRef] [Green Version]
- Erhan, D.; Manzagol, P.-A.; Bengio, Y.; Bengio, S.; Vincent, P. The Difficulty of Training Deep Architectures and the Effect of Unsupervised Pre-Training. In Proceedings of the Twelfth International Conference on Artificial Intelligence and Statistics, Clearwater Beach, FL, USA, 16–18 April 2009; Volume 5, pp. 153–160. [Google Scholar]
- Shin, H.-C.; Roth, H.R.; Gao, M.; Lu, L.; Xu, Z.; Nogues, I.; Yao, J.; Mollura, D.; Summers, R.M. Deep Convolutional Neural Networks for Computer-Aided Detection: CNN Architectures, Dataset Characteristics and Transfer Learning. IEEE Trans. Med. Imaging 2016, 35, 1285–1298. [Google Scholar] [CrossRef] [Green Version]
- Esteva, A.; Kuprel, B.; Novoa, R.A.; Ko, J.; Swetter, S.M.; Blau, H.M.; Thrun, S. Dermatologist-level classification of skin cancer with deep neural networks. Nature 2017, 542, 115–118. [Google Scholar] [CrossRef]
- Weiss, K.; Khoshgoftaar, T.M.; Wang, D. A survey of transfer learning. J. Big. Data 2016, 3, 1. [Google Scholar] [CrossRef] [Green Version]
- Huh, M.; Agrawal, P.; Efros, A.A. What Makes ImageNet Good for Transfer Learning? arXiv 2016, arXiv:1608.08614. [Google Scholar]
- Simonyan, K.; Zisserman, A. Very deep convolutional networks for large-scale image recognition. arXiv 2014, arXiv:1409.1556. [Google Scholar]
- Lorencin, I.; Šegota, S.B.; Anđelić, N.; Mrzljak, V.; Ćabov, T.; Španjol, J.; Car, Z. On Urinary Bladder Cancer Diagnosis: Utilization of Deep Convolutional Generative Adversarial Networks for Data Augmentation. Biology 2021, 10, 175. [Google Scholar] [CrossRef]
- Rodríguez, J.D.; Pérez, A.; Lozano, J.A. Sensitivity Analysis of k-Fold Cross Validation in Prediction Error Estimation. IEEE Trans. Pattern Anal. Mach. Intell. 2010, 32, 569–575. [Google Scholar] [CrossRef] [PubMed]
- Wong, T.-T.; Yang, N.-Y. Dependency Analysis of Accuracy Estimates in k-Fold Cross Validation. IEEE Trans. Knowl. Data Eng. 2017, 29, 2417–2427. [Google Scholar] [CrossRef]
- Moreno-Barea, F.J.; Strazzera, F.; Jerez, J.M.; Urda, D.; Franco, L. Forward noise adjustment scheme for data augmentation. In Proceedings of the 2018 IEEE Symposium Series on Computational Intelligence (SSCI), Bangalore, India, 18–21 November 2018; pp. 728–734. [Google Scholar] [CrossRef]
- Wang, S.; Tang, C.; Sun, J.; Yang, J.; Huang, C.; Phillips, P.; Zhang, Y.-D. Multiple Sclerosis Identification by 14-Layer Convolutional Neural Network With Batch Normalization, Dropout, and Stochastic Pooling. Front. Neurosci. 2018, 12, 818. [Google Scholar] [CrossRef] [PubMed]
- Wang, F.; Liu, X.; Yuan, N.; Qian, B.; Ruan, L.; Yin, C.; Jin, C. Study on automatic detection and classification of breast nodule using deep convolutional neural network system. J. Thorac. Dis. 2020, 12, 4690–4701. [Google Scholar] [CrossRef] [PubMed]
- Matheus, B.R.N.; Schiabel, H. A CADx scheme in mammography: Considerations on a novel approach. In Proceedings of the ADVCOMP 2013: The Seventh International Conference on Advanced Engineering Computing and Applications in Sciences, Porto, Portugal, 29 September–4 October 2013; pp. 15–18. [Google Scholar]


























{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Name | Description |
|---|---|
| Total Number of Images | 1459 |
| Dimension | 224 × 224 |
| Color Grading | RGB |
| Benign Mass | 417 |
| Benign Calcification | 398 |
| Malignant Calcification | 300 |
| Malignant Mass | 344 |
| Process | Algorithm | Function/Method | Parameter Value |
|---|---|---|---|
| Binary masking | cv2.rectangle() | Thickness = 5 | |
| Morphological opening | cv2.threshold() | Threshold = 127, maximum = 255, type = cv2.THRESH_BINARY | |
| cv2.morphologyEx() | Type = cv2.MORPH_OPEN, kernel size = (20, 20) | ||
| Artefacts removal | cv2.threshold() | Threshold = 127, maximum = 255, type = cv2.THRESH_BINARY | |
| Largest contour detection | cv2.findContours() | Contour retrieval mode = cv2. RETR_EXTERNAL, contour approximation method = cv2.CHAIN_APPROX_SIMPLE | |
| max() | key = cv2.contourArea | ||
| cv2.drawContours() | Index = −1, border color = (255, 255, 255), thickness = 1 | ||
| inRange Operation | cv2.inRange() | Lowest = (0, 0, 200), highest = (255, 255, 255) | |
| Gabor Filter | cv2.getGaborKernel() | Kernel size = (5, 5), sigma = 3, theta = 1*np.pi/1, lambd = 1*np. Pi/4, gamma = 0.5, phi = 20 and ktype=cv2.CV_32F | |
| Remove line | cv2.filter2D() | Source image, kernel | |
| Morphological opening | cv2.getStructuringElement() | Structuring element = cv2.MORPH_RECT, kernelSize = (1, 30) | |
| cv2.morphologyEx() | morphological operation = cv2.MORPH_OPEN | ||
| Morphological dilation | cv2.dilate() | kernelSize = (5, 5) | |
| Image enhancement | Gamma correction | np.array() | Gamma value = 2.0 |
| CLAHE | cv2.createCLAHE() | clipLimit =1.0, tileGridSize = (8, 8) |
| Image | MSE | PSNR | SSIM | RMSE |
|---|---|---|---|---|
| Image_1 | 15.37 | 37.67 | 0.962 | 0.13 |
| Image_2 | 15.63 | 37.29 | 0.961 | 0.13 |
| Image_3 | 14.25 | 38.28 | 0.964 | 0.12 |
| Image_4 | 13.31 | 37.31 | 0.962 | 0.13 |
| Image_5 | 13.37 | 39.67 | 0.967 | 0.11 |
| Image_6 | 11.53 | 41.29 | 0.973 | 0.09 |
| Image_7 | 13.63 | 39.28 | 0.963 | 0.11 |
| Image_8 | 12.47 | 40.36 | 0.969 | 0.10 |
| Image_9 | 15.21 | 37.79 | 0.963 | 0.13 |
| Image_10 | 13.82 | 39.31 | 0.966 | 0.11 |
| Classifier Name | Pre (%) | Recall (%) | F1 (%) | Spe (%) | Sen (%) | Tr_Acc (%) | Tr_Loss (%) | Val_Acc (%) | Val_Loss (%) | Ts_Acc (%) | Ts_Loss (%) |
|---|---|---|---|---|---|---|---|---|---|---|---|
| MobileNetV2 | 77.93 | 77.78 | 77.85 | 78.15 | 77.91 | 78.72 | 0.327 | 77.62 | 0.375 | 77.84 | 0.366 |
| ResNet50 | 80.12 | 79.91 | 80.01 | 81.21 | 81.35 | 80.43 | 0.380 | 79.81 | 0.324 | 79.98 | 0.301 |
| DenseNet201 | 87.06 | 86.83 | 86.94 | 88.21 | 88.63 | 88.03 | 0.292 | 86.77 | 0.284 | 86.92 | 0.271 |
| InceptionV3 | 76.74 | 76.84 | 76.78 | 78.85 | 79.91 | 76.91 | 0.421 | 76.21 | 0.392 | 76.87 | 0.384 |
| VGG16 | 97.29 | 97.02 | 97.15 | 98.03 | 98.14 | 97.79 | 0.182 | 96.83 | 0.115 | 97.13 | 0.081 |
| VGGNet19 | 96.33 | 96.27 | 96.29 | 97.33 | 97.17 | 96.63 | 0.221 | 95.63 | 0.205 | 96.24 | 0.197 |
| Classifier Name | FPR (%) | FNR (%) | FDR (%) | KC (%) | MCC (%) |
|---|---|---|---|---|---|
| MobileNetV2 | 21.15 | 22.22 | 22.07 | 78.65 | 68.56 |
| ResNet50 | 18.79 | 20.09 | 19.88 | 80.63 | 70.48 |
| DenseNet201 | 11.79 | 13.17 | 12.94 | 86.27 | 77.25 |
| InceptionV3 | 21.85 | 23.16 | 23.26 | 75.81 | 67.02 |
| VGG16 | 1.97 | 2.98 | 2.71 | 98.52 | 88.62 |
| VGGNet19 | 2.67 | 3.73 | 3.67 | 97.46 | 86.50 |
| Classifier Name | MAE | RMSE |
|---|---|---|
| MobileNetV2 | 17.09 | 32.57 |
| ResNet50 | 15.37 | 36.51 |
| DenseNet201 | 11.78 | 26.65 |
| InceptionV3 | 19.32 | 44.36 |
| VGG16 | 2.44 | 7.20 |
| VGGNet19 | 3.16 | 12.51 |
| Model | Layer Depth | Trainable Parameters |
|---|---|---|
| VGG19 | 19 | 50,178 |
| Mobilenetv2 | 53 | 125,442 |
| ResNet50 | 50 | 200,706 |
| InceptionV3 | 48 | 102,402 |
| DenseNet201 | 201 | 188,162 |
| VGG16 | 16 | 50,178 |
| Case Study | Layer Name | Val_Acc (%) | Val_Loss (%) | Ts_Acc (%) | Ts_Loss (%) | AUC (%) | Finding |
|---|---|---|---|---|---|---|---|
| Flatten | 96.98 | 0.12 | 97.13 | 0.12 | 97.57 | Identical performance | |
| 1 | GlobalAveragePooling2D | 96.98 | 0.12 | 97.13 | 0.12 | 97.57 | Identical performance |
| GlobalMaxPooling2D | 96.02 | 0.19 | 96.56 | 0.19 | 97.34 | Accuracy dropped |
| Case Study | Batch Size | Val_Acc (%) | Val_Loss (%) | Ts_Acc (%) | Ts_Loss (%) | AUC (%) | Finding |
|---|---|---|---|---|---|---|---|
| 16 | 96.98 | 0.16 | 97.44 | 0.197 | 97.72 | Accuracy increased | |
| 2 | 32 | 97.03 | 0.09 | 97.57 | 0.064 | 97.98 | Accuracy increased |
| 64 | 96.83 | 0.11 | 97.13 | 0.081 | 97.57 | Identical accuracy |
| Case Study | Loss Function | Val_Acc (%) | Val_Loss (%) | Ts_Acc (%) | Ts_Loss (%) | AUC (%) | Finding |
|---|---|---|---|---|---|---|---|
| Categorical Crossentropy | 97.03 | 0.09 | 97.57 | 0.064 | 97.98 | Identical accuracy | |
| 3 | Cosine similarity | 96.86 | 0.12 | 96.93 | 0.05 | 96.94 | Identical accuracy |
| Mean Squared Error | 95.64 | 0.18 | 96.72 | 0.08 | 96.86 | Accuracy dropped |
| Case Study | OP | LR | Val_Loss (%) | Val_Acc (%) | Ts_Loss (%) | Ts_Acc (%) | AUC (%) | Findings |
|---|---|---|---|---|---|---|---|---|
| Adam | 0.006 | 0.56 | 94.89 | 0.3110 | 95.0997 | 95.63 | Accuracy dropped | |
| 0.001 | 0.09 | 97.03 | 0.06 | 97.57 | 97.98 | Identical accuracy | ||
| 4 | 0.0008 | 0.14 | 97.03 | 0.05 | 98.02 | 98.27 | Accuracy increased | |
| Nadam | 0.006 | 0.42 | 95.15 | 0.26 | 96.18 | 96.94 | Accuracy dropped | |
| 0.001 | 0.14 | 96.62 | 0.08 | 97.31 | 97.67 | Accuracy dropped | ||
| 0.0008 | 0.14 | 96.19 | 0.08 | 97.48 | 98.15 | Accuracy dropped | ||
| Adamax | 0.006 | 0.18 | 95.50 | 0.10 | 96.61 | 96.82 | Accuracy dropped | |
| 0.001 | 0.18 | 94.89 | 0.14 | 95.35 | 95.46 | Accuracy dropped | ||
| 0.0008 | 0.19 | 94.29 | 0.15 | 94.96 | 95.27 | Accuracy dropped | ||
| RMSprop | 0.006 | 0.83 | 93.94 | 0.44 | 95.35 | 95.53 | Accuracy dropped | |
| 0.001 | 0.20 | 94.46 | 0.14 | 94.27 | 94.65 | Accuracy dropped | ||
| 0.0008 | 0.22 | 94.24 | 0.12 | 94.10 | 95.68 | Accuracy dropped |
| Filter | Val_Acc (%) | Test_Acc (%) | F1_score (%) |
|---|---|---|---|
| Green fire blue | 97.03 | 98.02 | 98.15 |
| Blue orange icb | 94.78 | 95.23 | 95.27 |
| 6 shades | 94.42 | 94.11 | 94.25 |
| 16 colors | 95.43 | 95.87 | 95.93 |
| Experiment | Test Accuracy (%) | Validation Accuracy (%) | F1_Score (%) |
|---|---|---|---|
| Raw image | 79.32 | 72.86 | 79.36 |
| Artefact removal | 88.45 | 87.38 | 88.62 |
| CLAHE 1ST | 94.63 | 91.67 | 94.74 |
| CLAHE 2ND | 95.21 | 93.07 | 93.28 |
| Green fire blue | 98.02. | 97.03 | 98.15 |
| Configuration | Value |
|---|---|
| Image size | 224 × 224 |
| Epochs | 90 |
| Optimization function | Adam |
| Learning rate | 0.001 |
| Batch size | 32 |
| Weight decay | 0.0001 |
| Activation function | Softmax |
| Dropout | 0.5 |
| Momentum | 0.9 |
| Accuracy | Fold 1 | Fold 2 | Fold 3 | Fold 4 | Fold 5 | Average Validation Accuracy |
|---|---|---|---|---|---|---|
| Training | 97.93 | 99.35 | 98.83 | 98.57 | 99.06 | |
| Validation | 96.85 | 98.71 | 97.74 | 98.26 | 98.53 | 98.01 |
| Accuracy | Fold 1 | Fold 2 | Fold 3 | Fold 4 | Fold 5 | Fold 6 | Fold 7 | Fold 8 | Fold 9 | Fold 10 | Average Validation Accuracy |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Training | 97.34 | 99.06 | 97.40 | 99.15 | 98.83 | 98.72 | 98.86 | 99.07 | 98.47 | 98.60 | |
| Validation | 97.48 | 98.63 | 96.81 | 98.72 | 97.95 | 97.64 | 98.54 | 98.26 | 96.88 | 98.15 | 97.90 |
| Noise | Amount | Optimizer | Learning Rate | Test Accuracy (%) | F1_Score (%) |
|---|---|---|---|---|---|
| Gaussian | 0.1 | Adam | 0.001 | 95.87 | 95.44 |
| Work | Model | Dataset | Batch | Epoch | Optimizer | Learning Rate | Accuracy |
|---|---|---|---|---|---|---|---|
| Nasir Khan et al. (2019) [23] | MVFF CADx | CBIS-DDSM: 3568 mammograms & MIAS: 322 mammograms | 32 | 100 | SGD | 0.001 | 93.73% |
| Al-antari et al. (2018) [28] | Fully Integrated CAD | INbreast Toward a Full-field Digital Mammographic Database: 410 mammograms After augmentation: 896 | 24 | 100 | Adam | 0.0001 | 95.64% |
| Hameed et al. (2020) [22] | Full trained VGG16 + VGG19 Fine-tuned VGG16 + VGG19 | Pathology department of Colsanitas Colombia University provided 544 image of breast cancer. | 32 | 200 | Adam | 0.0001 | 93.53% 95.29% |
| Khamparia et al. (2021) [18] | Hybrid MVGG16 ImageNet | Digital Database for Screening Mammography (DDSM) containing 2620 mammograms. | 32 | 15 | - | - | 94.3% |
| Institute of Electrical and Electronics Engineers, n.d. [17] | Pre-trained VGG16 with 1 FC layer | Digital Database for Screening Mammography (DDSM) containing 2620 mammograms. Mammographic Image Analysis Society containing 332 mammograms. | 20 15 | 500 500 | Nadam RMSprop | - | 90.5% 91.2% |
| Shallu and Mehra, (2018) [25] | VGG16 + LR VGG19 + LR ResNet50 + LR | BreakHis dataset used in collaboration with the Prognostic and Diagnostic Laboratory containing 7909 breast cancer images. | - | - | - | - | 92.60% 90.40% 79.40% |
| Li et al. (2019) [5] | AlexNet VGGNet GoogLeNet DenseNet DenseNet-II | The First Hospital of Shanxi Medical University provided 2042 full-field digital mammograms. With augmentation the data set was increased to 30,630 images | - | - | - | 0.01 | 92.70% 92.78% 93.54% 93.87% 94.55% |
| Our work | BreastNet18 | Pre trained on ImageNet dataset consisting of over 14 million images. CBIS-DDSM dataset: 1442 mammograms. After augmentation: 11,536 mammograms. | 32 | 350 | Adam | 0.0008 | 98.02% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Montaha, S.; Azam, S.; Rafid, A.K.M.R.H.; Ghosh, P.; Hasan, M.Z.; Jonkman, M.; De Boer, F. BreastNet18: A High Accuracy Fine-Tuned VGG16 Model Evaluated Using Ablation Study for Diagnosing Breast Cancer from Enhanced Mammography Images. Biology 2021, 10, 1347. https://doi.org/10.3390/biology10121347
Montaha S, Azam S, Rafid AKMRH, Ghosh P, Hasan MZ, Jonkman M, De Boer F. BreastNet18: A High Accuracy Fine-Tuned VGG16 Model Evaluated Using Ablation Study for Diagnosing Breast Cancer from Enhanced Mammography Images. Biology. 2021; 10(12):1347. https://doi.org/10.3390/biology10121347
Chicago/Turabian StyleMontaha, Sidratul, Sami Azam, Abul Kalam Muhammad Rakibul Haque Rafid, Pronab Ghosh, Md. Zahid Hasan, Mirjam Jonkman, and Friso De Boer. 2021. "BreastNet18: A High Accuracy Fine-Tuned VGG16 Model Evaluated Using Ablation Study for Diagnosing Breast Cancer from Enhanced Mammography Images" Biology 10, no. 12: 1347. https://doi.org/10.3390/biology10121347