
Studying the Accuracy and Function of Different Thermometry Techniques for Measuring Body Temperature

 and
and 
Abstract
:Simple Summary
Abstract
1. Introduction
Objectives
2. Methods
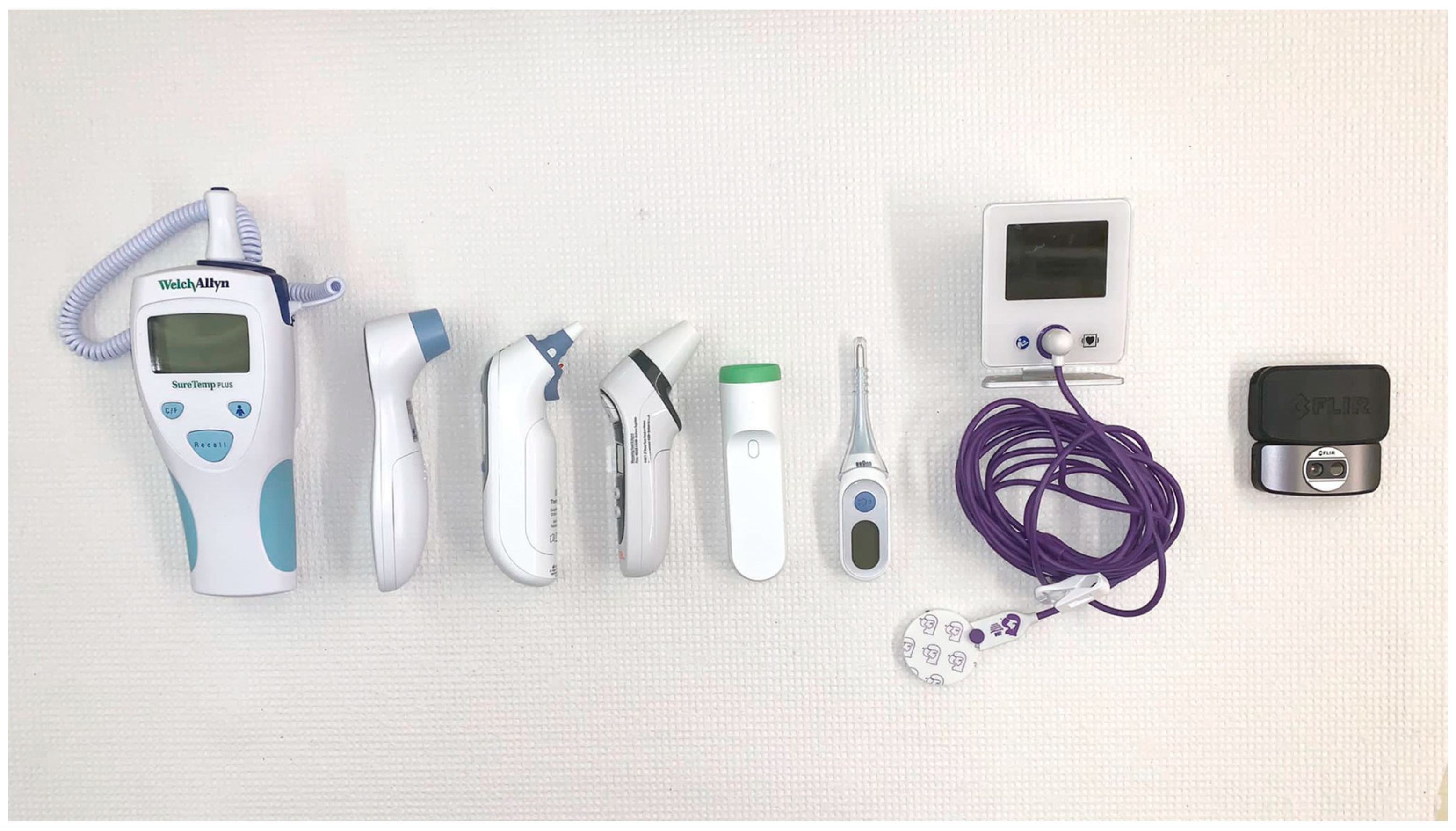
2.1. Selected Thermometer Systems
2.1.1. Infrared Forehead Thermometer
2.1.2. Infrared Tympanic Thermometer
2.1.3. Infrared Temporal Artery Thermometer
2.1.4. Digital Sublingual Thermometer
2.1.5. Zero Heat Flux Thermometer
2.1.6. Infrared Thermal Imaging Camera
2.2. Participants
2.3. Experimental Protocol
2.4. Statistical Methods
3. Results
3.1. Mean Temperature Difference
3.2. Statistical Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Robinson, J.L. Body temperature measurement in paediatrics: Which gadget should we believe? Paediatr. Child Health 2004, 9, 457–459. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khan, S.; Saultry, B.; Adams, S.; Kouzani, A.Z.; Decker, K.; Digby, R.; Bucknall, T. Comparative accuracy testing of non-contact infrared thermometers and temporal artery thermometers in an adult hospital setting. Am. J. Infect. Control 2021, 49, 597–602. [Google Scholar] [CrossRef] [PubMed]
- Jefferies, S.; Weatherall, M.; Young, P.; Beasley, R. A systematic review of the accuracy of peripheral thermometry in estimating core temperatures among febrile critically ill patients. Crit. Care Resusc. J. Australas. Acad. Crit. Care Med. 2011. Available online: https://pubmed.ncbi.nlm.nih.gov/21880009/ (accessed on 10 September 2021).
- Crawford, D.C.; Hicks, B.; Thompson, M.J. Which thermometer? Factors influencing best choice for intermittent clinical temperature assessment. J. Med. Eng. Technol. 2006, 30, 199–211. [Google Scholar] [CrossRef]
- Eshraghi, Y.; Nasr, V.; Parra-Sanchez, I.; Van Duren, A.; Botham, M.; Santoscoy, T.; Sessler, D.I. An evaluation of a zero-heat-flux cutaneous thermometer in cardiac surgical patients. Anesth. Analg. 2014, 119, 543–549. [Google Scholar] [CrossRef] [Green Version]
- Lim, C.L.; Byrne, C.; Lee, J. Human Thermoregulation and Measurement of Body Temperature in Exercise and Clinical Settings; Annals of the Academy of Medicine: Singapore, 2008. Available online: https://pubmed.ncbi.nlm.nih.gov/18461221/ (accessed on 10 September 2021).
- Uslu, S.; Ozdemir, H.; Bulbul, A.; Comert, S.; Bolat, F.; Can, E.; Nuhoglu, A. A comparison of different methods of temperature measurements in sick newborns. J. Trop. Pediatr. 2011, 57, 418–423. [Google Scholar] [CrossRef] [Green Version]
- Fitzgerald, E. Accuracy Study for the Welch Allyn® Model 692/690 SureTemp® Plus Oral, Adult Axillary, and Rectal Thermometer. 2003. Available online: https://emeai.welchallyn.com/content/dam/welchallyn/documents/upload-docs/Research/Case-Study/Suretempplus_Accuracy_CaseStudy.pdf (accessed on 13 September 2021).
- Mangat, J.; Standley, T.; Prevost, A.; Vasconcelos, J.; White, P. A comparison of technologies used for estimation of body temperature. Physiol. Meas. 2010, 31, 1105–1118. [Google Scholar] [CrossRef]
- Kiekkas, P.; Stefanopoulos, N.; Bakalis, N.; Kefaliakos, A.; Karanikolas, M. Agreement of infrared temporal artery thermometry with other thermometry methods in adults: Systematic review. J. Clin. Nurs. 2016, 25, 894–905. [Google Scholar] [CrossRef] [PubMed]
- Hooper, V.D.; Andrews, J.O. Accuracy of noninvasive core temperature measurement in acutely ill adults: The state of the science. Biol. Res. Nurs. 2006, 8, 24–34. [Google Scholar] [CrossRef]
- Guschlbauer, M.; Maul, A.C.; Yan, X.; Herff, H.; Annecke, T.; Sterner-Kock, A.; Böttiger, B.W.; Schroeder, D.C. Zero-Heat-Flux thermometry for Non-invasive measurement of core body temperature in pigs. PLoS ONE 2016, 11, e0150759. [Google Scholar] [CrossRef]
- Ng, E.Y.K.; Kawb, G.J.L.; Chang, W.M. Analysis of ir thermal imager for mass blind fever screening. Microvasc. Res. 2004, 68, 104–109. [Google Scholar] [CrossRef]
- Khaksari, K.; Nguyen, T.; Hill, B.Y.; Perrault, J.; Gorti, V.; Blick, E.; Gonzalez Cano, T.; Shadgan, B.; Quang, T.; Malpani, R.; et al. Review of the efficacy of infrared thermography for screening infectious diseases with applications to covid-19. J. Med. Imaging 2021, 8, 010901. [Google Scholar] [CrossRef] [PubMed]
- Peiffer, J.J.; Abbiss, C.R.; Nosaka, K.; Peake, J.M.; Laursen, P.B. Effect of cold water immersion after exercise in the heat on muscle function, body temperatures, and vessel diameter. J. Sci. Med. Sport 2009, 12, 91–96. [Google Scholar] [CrossRef]
- Jacobsen, F.L. Surface Temperature, Body Temperature, and Heart Rate as Affected by Immersing the Feet of Conditioned Basketball Players in Cold Water Bath. Master’s Thesis, Dakota State University, Madison, SD, USA, 1968. [Google Scholar]
- Kim, P.S.; Read, S.W.; Fauci, A.S. Therapy for early COVID-19. JAMA 2020, 324, 2149. [Google Scholar] [CrossRef]
- Aggarwal, N.; Garg, M.; Dwarakanathan, V.; Gautam, N.; Kumar, S.S.; Jadon, R.S.; Gupta, M.; Ray, A. Diagnostic accuracy of non-contact infrared thermometers and thermal scanners: A systematic review and meta-analysis. J. Travel Med. 2020, 27, taaa193. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.-Y.; Chen, A.; Chen, C. Investigation of the impact of infrared sensors on core body temperature monitoring by comparing measurement sites. Sensors 2020, 20, 2885. [Google Scholar] [CrossRef]
- Moran, D.S.; Mendal, L. Core temperature measurement. Sports Med. 2002, 32, 879–885. [Google Scholar] [CrossRef] [PubMed]
- Erickson, R.S.; Kirklin, S.K. Comparison of ear-based, bladder, oral, and axillary methods for core temperature measurement. Crit. Care Med. 1993, 21, 1528–1534. [Google Scholar] [CrossRef] [PubMed]
- White, N.; Baird, S.; Anderson, D.L. A comparison of tympanic thermometer readings to pulmonary artery catheter core temperature recordings. Appl. Nurs. Res. 1994, 7, 165–169. [Google Scholar] [CrossRef]
- Haugan, B.; Langerud, A.K.; Kalvøy, H.; Frøslie, K.F.; Riise, E.; Kapstad, H. Can we trust the new generation of infrared tympanic thermometers in clinical practice? J. Clin. Nurs. 2013, 22, 698–709. [Google Scholar] [CrossRef]
- Childs, C.; Harrison, R.; Hodkinson, C. Tympanic membrane temperature as a measure of core temperature. Arch. Dis. Child. 1999, 80, 262–266. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fulbrook, P. Core body temperature measurement: A comparison of axilla, tympanic membrane and pulmonary artery blood temperature. Intensive Crit. Care Nurs. 1997, 13, 266–272. [Google Scholar] [CrossRef]
- Yaron, M.; Lowenstein, S.R.; Koziol-McLain, J. Measuring the accuracy of the infrared tympanic thermometer: Correlation does not signify agreement. J. Emerg. Med. 1995, 13, 617–621. [Google Scholar] [CrossRef]
- Barnett, B.J.; Nunberg, S.; Tai, J.; Lesser, M.L.; Fridman, V.; Nichols, P.; Powell, R.; Silverman, R. Oral and tympanic membrane temperatures are inaccurate to identify Fever in emergency department adults. West. J. Emerg. Med. 2011, 12, 505–511. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jensen, B.N.; Jensen, F.S.; Madsen, S.N.; Løssl, K. Accuracy of digital tympanic, oral, axillary, and rectal thermometers compared with standard rectal mercury thermometers. Eur. J. Surg. Acta Chir. 2000, 166, 848–851. [Google Scholar] [CrossRef]
- Mazerolle, S.M.; Ganio, M.S.; Casa, D.J.; Vingren, J.; Klau, J. Is oral temperature an accurate measurement of deep body temperature? A systematic review. J. Athl. Train. 2011, 46, 566–573. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bijur, P.E.; Shah, P.D.; Esses, D. Temperature measurement in the adult emergency department: Oral, tympanic membrane and temporal artery temperatures versus rectal temperature. Emerg. Med. J. EMJ 2016, 33, 843–847. [Google Scholar] [CrossRef] [PubMed]
- Duncan, A.L.; Bell, A.J.; Chu, K.; Greenslade, J.H. Can a non-contact infrared thermometer be used interchangeably with other thermometers in an adult Emergency department? Australas. Emerg. Nurs. J. 2008, 11, 130–134. [Google Scholar] [CrossRef]
- Liu, C.C.; Chang, R.E.; Chang, W.C. Limitations of forehead infrared body temperature detection for fever screening for severe acute respiratory syndrome. Infect. Control Hosp. Epidemiol. 2004, 25, 1109–1111. [Google Scholar] [CrossRef]
- Hausfater, P.; Zhao, Y.; Defrenne, S.; Bonnet, P.; Riou, B. Cutaneous infrared thermometry for detecting febrile patients. Emerg. Infect. Dis. 2008, 14, 1255–1258. [Google Scholar] [CrossRef]
- Niven, D.J.; Gaudet, J.E.; Laupland, K.B.; Mrklas, K.J.; Roberts, D.J.; Stelfox, H.T. Accuracy of peripheral thermometers for estimating temperature: A systematic review and meta-analysis. Ann. Intern. Med. 2015, 163, 768–777. [Google Scholar] [CrossRef] [PubMed]
- Hart, D.; Rischall, M.; Durgin, K.; Donoghue, M.; Pham, T.; Wyatt, T.; Stang, J.; DeVries, P.; Driver, B. Non-invasive zero-heat-flux technology compared with traditional core temperature measurements in the emergency department. Am. J. Emerg. Med. 2020, 38, 2383–2386. [Google Scholar] [CrossRef]
- Bräuer, A.; Fazliu, A.; Perl, T.; Heise, D.; Meissner, K.; Brandes, I.F. Accuracy of zero-heat-flux thermometry and bladder temperature measurement in critically ill patients. Sci. Rep. 2020, 10, 21746. [Google Scholar] [CrossRef] [PubMed]
- Morettini, E.; Turchini, F.; Tofani, L.; Villa, G.; Ricci, Z.; Romagnoli, S. Intraoperative core temperature monitoring: Accuracy and precision of zero-heat flux heated controlled servo sensor compared with esophageal temperature during major surgery; the ESOSPOT study. J. Clin. Monit. Comput. 2020, 34, 1111–1119. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Device | Company | Model Number | Meas. Site | Meas. Distance | Meas. Speed | Data Recordability | Clinical Accuracy | Price (CAD) |
|---|---|---|---|---|---|---|---|---|
| SureTemp Plus * | Welch-Allyn | 692 | Oral | Contact | 6 s | No | ±0.1 °C | $501 |
| Temporal Artery | Withings | SCT01 | Forehead | 2–5 cm | 3 s | Yes | ±0.2 °C | $130 |
| Infrared Forehead | Wellworks | FDIR-V16 | Forehead | 2–5 cm | 1 s | No | ±0.3 °C | $50 |
| Infrared Tympanic | Braun | IRT6520 | Ear | Contact | 1 s | No | ±0.2 °C | $58 |
| Digital Sublingual | Braun | PRT2000 | Oral | Contact | 8 s | No | ±0.1 °C | $24 |
| Infrared Forehead | MOBI | 70121 | Forehead | 2–5 cm | 1 s | No | ±0.2 °C | $29 |
| Zero Heat Flux | 3M | 3700 | Forehead | Contact | Continuous (After equilibrium) | No | ±0.23 °C | $1100 |
| Thermal Imaging Camera | FLIR One | FLIR One Pro | Face | 10 cm/50 cm | 1 s | Yes | ±3 °C | $530 |
| Withings | Wellworks | Braun Tympanic (R) | Braun Tympanic (L) | Braun Sublingual | MOBI | 3M | FLIR One (10 cm) | FLIR One (50 cm) | |
|---|---|---|---|---|---|---|---|---|---|
| Mean Difference | +0.429 | +0.237 | −0.106 | −0.044 | −0.189 | −0.184 | +0.342 | +0.443 | +0.522 |
| SD | 0.359 | 0.315 | 0.301 | 0.279 | 0.331 | 0.283 | 0.311 | 1.333 | 1.334 |
| CI95 | ±0.129 | ±0.113 | ±0.108 | ±0.099 | ±0.119 | ±0.101 | ±0.111 | ±0.477 | ±0.478 |
| Withings | Wellworks | Braun Tympanic (R) | Braun Tympanic (L) | Braun Sublingual | MOBI | 3M | FLIR One (10 cm) | FLIR One (50 cm) | |
|---|---|---|---|---|---|---|---|---|---|
| p value | 0.0000 | 0.0000 | 0.000 | 0.1747 * | 0.0000 | 0.0000 | 0.0000 | 0.0000 | 0.0000 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mah, A.J.; Ghazi Zadeh, L.; Khoshnam Tehrani, M.; Askari, S.; Gandjbakhche, A.H.; Shadgan, B. Studying the Accuracy and Function of Different Thermometry Techniques for Measuring Body Temperature. Biology 2021, 10, 1327. https://doi.org/10.3390/biology10121327
Mah AJ, Ghazi Zadeh L, Khoshnam Tehrani M, Askari S, Gandjbakhche AH, Shadgan B. Studying the Accuracy and Function of Different Thermometry Techniques for Measuring Body Temperature. Biology. 2021; 10(12):1327. https://doi.org/10.3390/biology10121327
Chicago/Turabian StyleMah, Aaron James, Leili Ghazi Zadeh, Mahta Khoshnam Tehrani, Shahbaz Askari, Amir H. Gandjbakhche, and Babak Shadgan. 2021. "Studying the Accuracy and Function of Different Thermometry Techniques for Measuring Body Temperature" Biology 10, no. 12: 1327. https://doi.org/10.3390/biology10121327