
Dose-Dependent Suppression of Human Glioblastoma Xenograft Growth by Accelerator-Based Boron Neutron Capture Therapy with Simultaneous Use of Two Boron-Containing Compounds

 , , , , , ,
, , , , , ,  and
and 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Cell Cultures
2.2. Preparation of Tumor Xenografts
2.3. Boron Compounds
2.4. Irradiation Experiments
2.5. Calculation of Boron-Related Absorbed Dose
2.6. Exposure Parameters
2.7. Statistical Analysis
3. Results
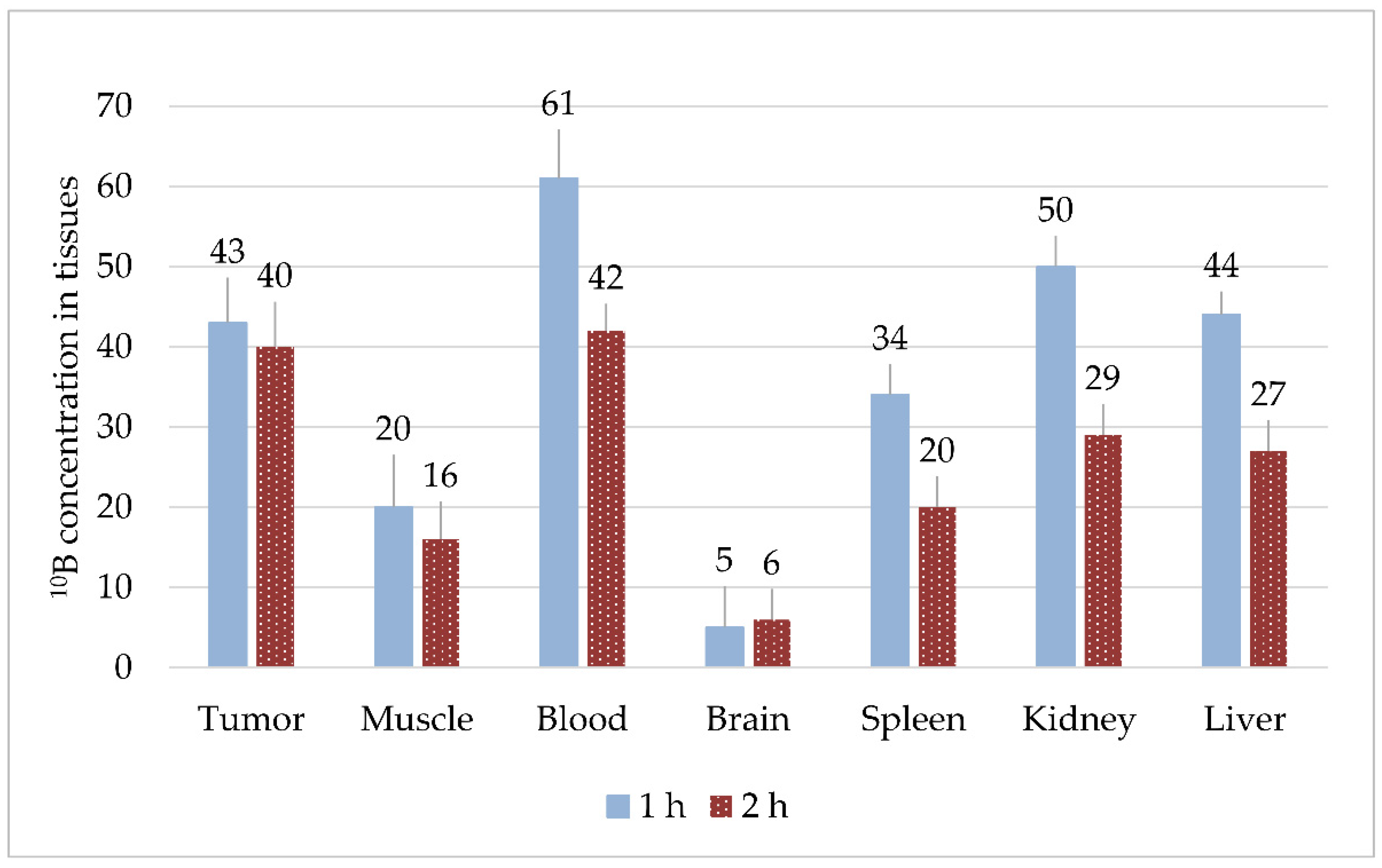
3.1. Compound Biodistribution
3.1.1. Experiment #1
3.1.2. Experiment #2
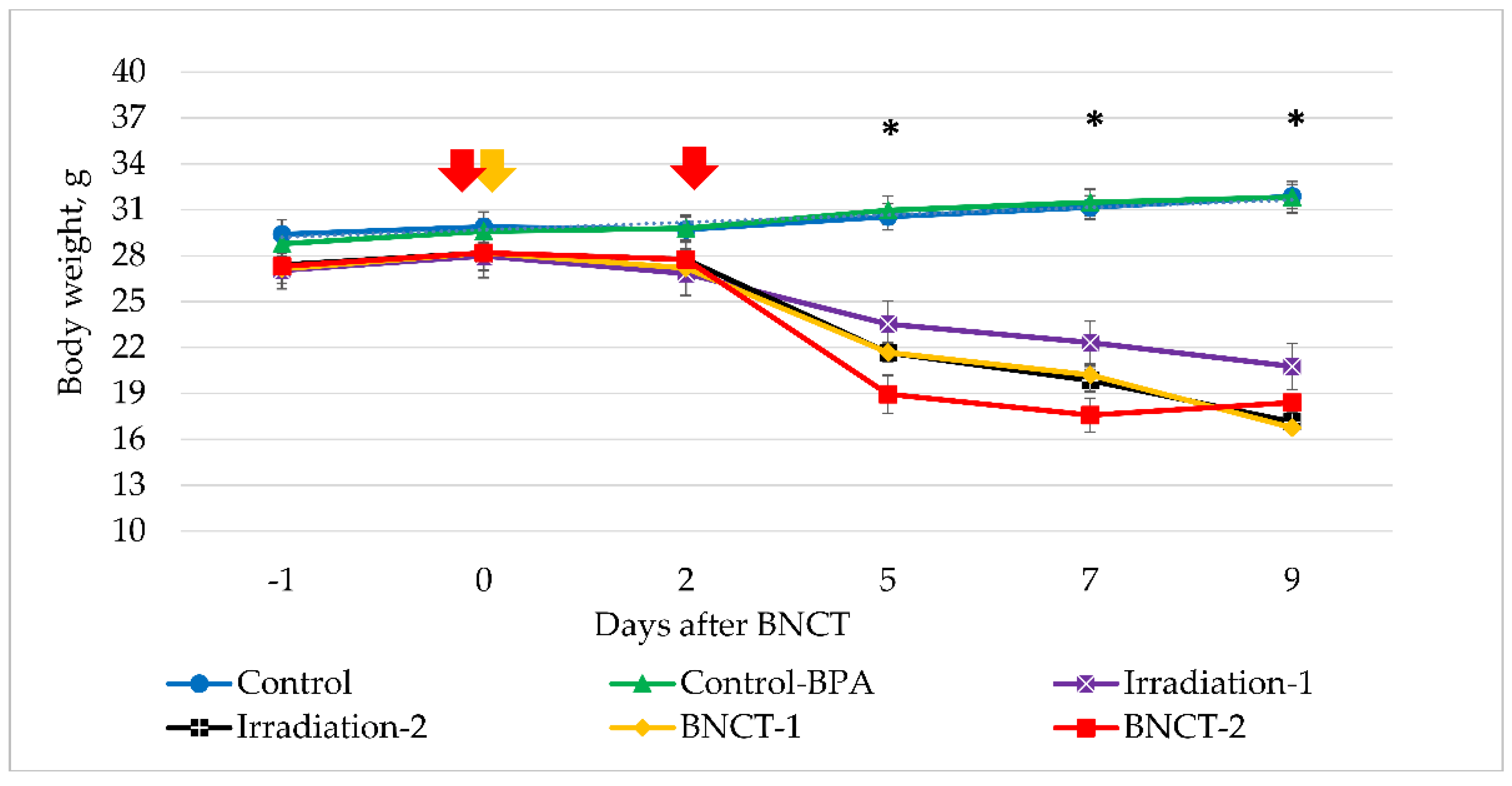
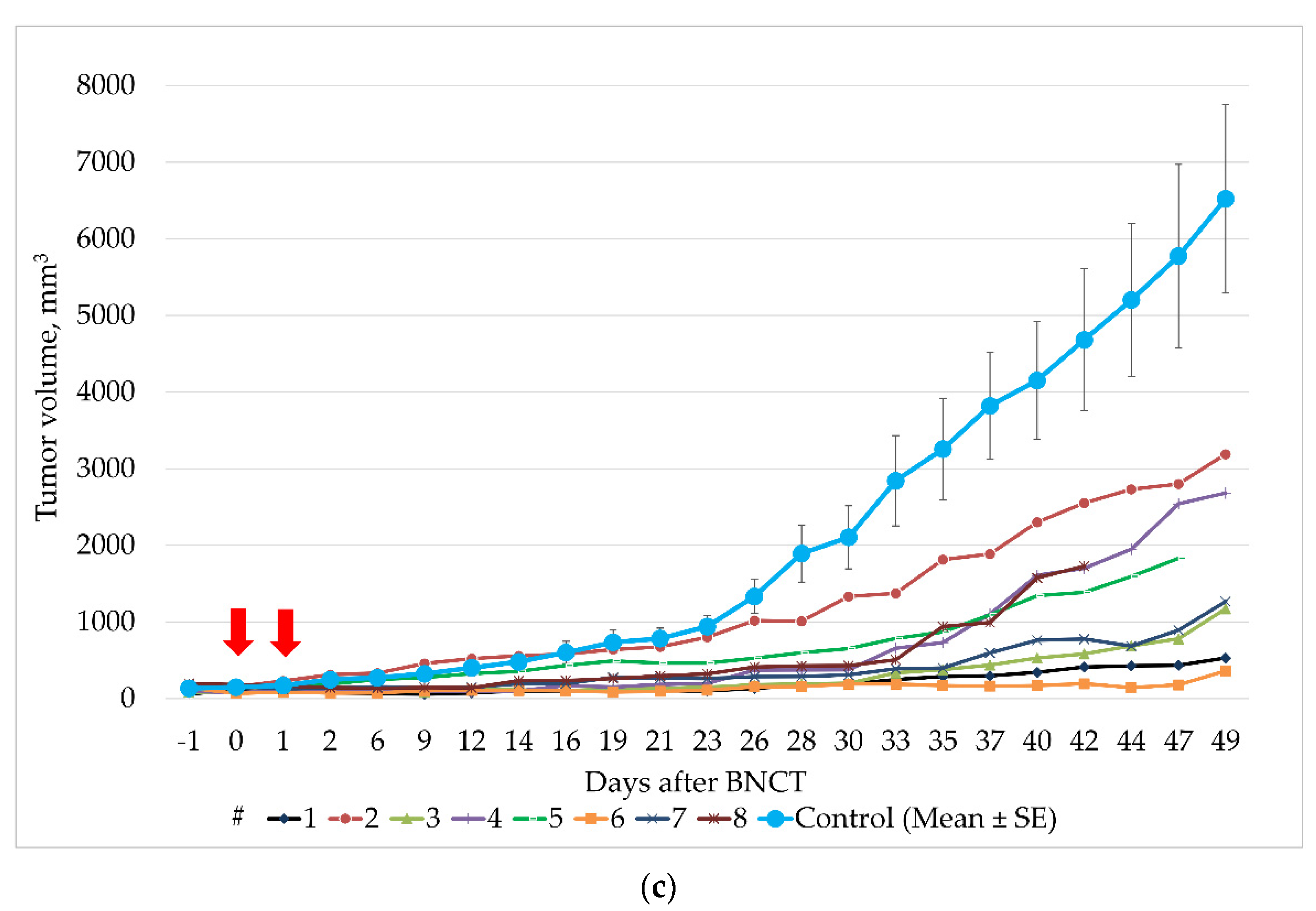
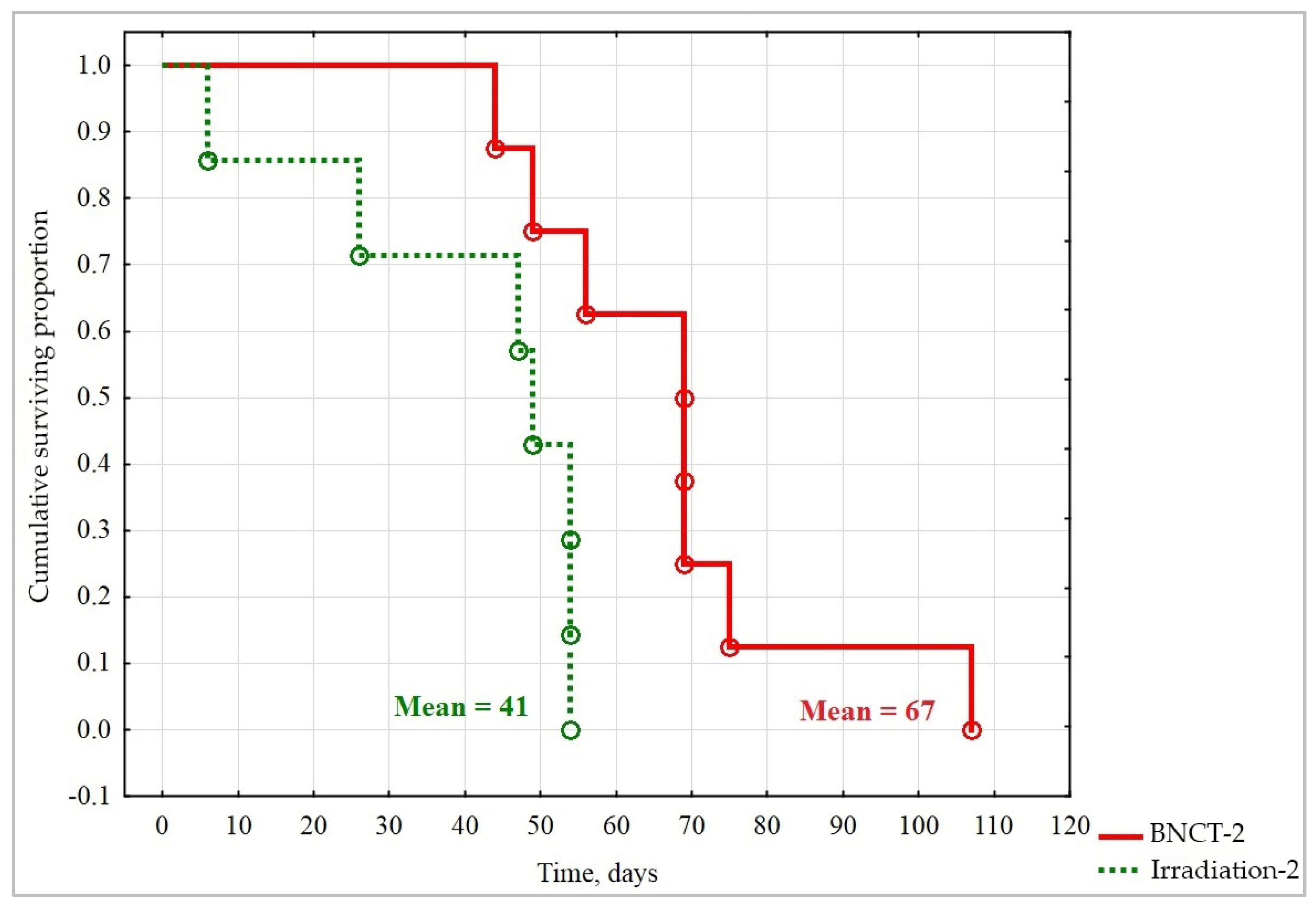
3.2. Irradiation Experiments
3.2.1. Experiment #1
3.2.2. Experiment #2
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ostrom, Q.T.; Bauchet, L.; Davis, F.G.; Deltour, I.; Fisher, J.L.; Langer, C.E.; Pekmezci, M.; Schwartzbaum, J.A.; Turner, M.C.; Walsh, K.M.; et al. The epidemiology of glioma in adults: A “state of the science” review. Neuro-Oncology 2014, 16, 896–913. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hatanaka, H. Clinical Results of Boron Neutron Capture Therapy. Basic Life Sci. 1990, 54, 15–21. [Google Scholar] [CrossRef] [PubMed]
- Nakagawa, Y.; Hatanaka, H. Boron neutron capture therapy. Clinical brain tumor studies. J. Neuro-Oncol. 1997, 33, 105–115. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, T.; Nakai, K.; Tsurubuchi, T.; Matsuda, M.; Shirakawa, M.; Zaboronok, A.; Endo, K.; Matsumura, A. Boron neutron capture therapy for newly diagnosed glioblastoma: A pilot study in Tsukuba. Appl. Radiat. Isot. 2009, 67, S25–S26. [Google Scholar] [CrossRef] [PubMed]
- Miyatake, S.-I.; Kawabata, S.; Hiramatsu, R.; Kuroiwa, T.; Suzuki, M.; Kondo, N.; Ono, K. Boron Neutron Capture Therapy for Malignant Brain Tumors. Neurol. Med. Chir. 2016, 56, 361–371. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sauerwein, W.A.G. Principles and Roots of Neutron Capture Therapy. In Neutron Capture Therapy: Principles and Applications; Sauerwein, W.A.G., Wittig, A., Moss, R., Nakagawa, Y., Eds.; Springer: Berlin/Heidelberg, Germany, 2012; pp. 1–16. [Google Scholar]
- Barth, R.F.; Zhang, Z.; Liu, T. A realistic appraisal of boron neutron capture therapy as a cancer treatment modality. Cancer Commun. 2018, 38, 36–37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sander, A.; Wosniok, W.; Gabel, D. Case numbers for a randomized clinical trial of boron neutron capture therapy for Glioblastoma multiforme. Appl. Radiat. Isot. 2014, 88, 16–19. [Google Scholar] [CrossRef] [PubMed]
- Kageji, T.; Nagahiro, S.; Mizobuchi, Y.; Matsuzaki, K.; Nakagawa, Y.; Kumada, H. Boron neutron capture therapy (BNCT) for newly-diagnosed glioblastoma: Comparison of clinical results obtained with BNCT and conventional treatment. J. Med. Investig. 2014, 61, 254–263. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dymova, M.A.; Taskaev, S.Y.; Richter, V.A.; Kuligina, E.V. Boron neutron capture therapy: Current status and future perspectives. Cancer Commun. 2020, 40, 406–421. [Google Scholar] [CrossRef]
- Taskaev, S.Y.; Kanygin, V.V. Boron Neutron Capture Therapy; SB RAS Publishing House: Novosibirsk, Russia, 2016. (In Russian) [Google Scholar]
- Sumitomo Heavy Industries. Sumitomo Heavy Industries, Ltd. Has Started to a Comprehensive Review of the SAKIGAKE Designation System in Order to Speedily Evaluate the Efficacy of Accelerator Based BNCT Systems in Japan. 2019. Available online: https://www.shi.co.jp/english/info/2019/6kgpsq0000002cez.html (accessed on 22 September 2021).
- Neutron Therapeutics. Available online: http://www.neutrontherapeutics.com/news/pr-041819/ (accessed on 22 September 2021).
- TAE Life Sciences. Available online: https://taelifesciences.com/alphabeam-neutron-system/ (accessed on 22 September 2021).
- Southern TOHOKU BNCT Research Center. Available online: http://www.sthg-jp.com/motion.asp?siteid=100511&menuid=10491&lgid=1 (accessed on 22 September 2021).
- Sumitomo Heavy Industries. Japanese BNCT Facilities Have Started Clinical Treatments under the National Health Insurance System with NeuCure™ BNCT System and NeuCure™ Dose Engine Provided by Sumitomo Heavy Industries, Ltd. 2020. Available online: https://www.shi.co.jp/english/info/2020/6kgpsq0000002p30.html (accessed on 20 October 2021).
- Stella Pharma. Available online: https://stella-pharma.co.jp/en/blog/1351/ (accessed on 20 October 2021).
- Taskaev, S.Y. Accelerator based epithermal neutron source. Phys. Part. Nucl. 2015, 46, 956–990. [Google Scholar] [CrossRef]
- Taskaev, S.Y.; Kanygin, V.; Byvaltsev, V.; Zaboronok, A.A.; Volkova, O.Y.; Mechetina, L.V.; Taranin, A.V.; Kichigin, A.I.; Iarullina, A.I.; Eliseenko, I.A.; et al. Opportunities for Using an Accelerator-Based Epithermal Neutron Source for Boron Neutron Capture Therapy. Biomed. Eng. 2018, 52, 73–76. [Google Scholar] [CrossRef]
- Taskaev, S. Development of an accelerator-based epithermal neutron source for boron neutron capture therapy. Phys. Part. Nucl. 2019, 50, 569–575. [Google Scholar] [CrossRef]
- Taskaev, S.; Berendeev, E.; Bikchurina, M.; Bykov, T.; Kasatov, D.; Kolesnikov, I.; Koshkarev, A.; Makarov, A.; Ostreinov, G.; Porosev, V.; et al. Neutron Source Based on Vacuum Insulated Tandem Accelerator and Lithium Target. Biology 2021, 10, 350. [Google Scholar] [CrossRef] [PubMed]
- Volkova, O.Y.; Mechetina, L.V.; Taranin, A.V.; Zaboronok, A.A.; Nakai, K.; Lezhnin, S.I.; Frolov, S.A.; Kasatov, D.A.; Lezhnin, S.I.; Frolov, S.A.; et al. Impact of neutron radiation on the viability of tumor cells cultured in the presence of boron-10 isotope. Vestn. Rentgenol. Radiol. 2016, 97, 283–288. (In Russian) [Google Scholar] [CrossRef] [PubMed]
- Zaboronok, A.; Byvaltsev, V.; Kanygin, V.; Iarullina, A.; Kichigin, A.; Volkova, O.; Mechetina, L.; Taskaev, S.; Muhamadiyarov, R.; Nakai, K.; et al. Boron-neutron capture therapy in Russia: Preclinical evaluation of efficacy and perspectives of its application in neurooncology. New Armen. Med. J. 2017, 11, 6–15. [Google Scholar]
- Sato, E.; Zaboronok, A.; Yamamoto, T.; Nakai, K.; Taskaev, S.; Volkova, O.; Mechetina, L.; Taranin, A.; Kanygin, V.; Isobe, T.; et al. Radiobiological response of U251MG, CHO-K1 and V79 cell lines to accelerator-based boron neutron capture therapy. J. Radiat. Res. 2017, 59, 101–107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Byvaltsev, V.A.; Zavyalov, E.L.; Kanygin, V.V.; Kasatova, A.I.; Kichigin, A.I.; Razumov, I.A.; Sycheva, T.V.; Taskaev, S.Y. Cytopathic effects of boron neutron capture therapy at the accelerator-base source of epithermal neutrons on human glioblastoma cell culture. Sib. J. Oncol. 2019, 18, 34–42. (In Russian) [Google Scholar] [CrossRef]
- Zavjalov, E.; Zaboronok, A.; Kanygin, V.; Kasatova, A.; Kichigin, A.; Mukhamadiyarov, R.; Razumov, I.; Sycheva, T.; Mathis, B.J.; Maezono, S.E.B.; et al. Accelerator-based boron neutron capture therapy for malignant glioma: A pilot neutron irradiation study using boron phenylalanine, sodium borocaptate and liposomal borocaptate with a heterotopic U87 glioblastoma model in SCID mice. Int. J. Radiat. Biol. 2020, 96, 868–878. [Google Scholar] [CrossRef] [PubMed]
- Sauerwein, W.A.G.; Bet, P.M.; Wittig, A. Drugs for BNCT: BSH and BPA. In Neutron Capture Therapy: Principles and Applications; Sauerwein, W.A.G., Wittig, A., Moss, R., Nakagawa, Y., Eds.; Springer: Berlin/Heidelberg, Germany, 2012; pp. 117–160. [Google Scholar]
- Barth, R.F.; Mi, P.; Yang, W. Boron delivery agents for neutron capture therapy of cancer. Cancer Commun. 2018, 38, 35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kabalka, G.W.; Wu, Z.; Yao, M.-L. Synthesis of a series of boronated unnatural cyclic amino acids as potential boron neutron capture therapy agents. Appl. Organomet. Chem. 2008, 22, 516–522. [Google Scholar] [CrossRef]
- Singh, B.; Kaur, G.; Singh, P.; Singh, K.; Kumar, B.; Vij, A.; Kumar, M.; Bala, R.; Meena, R.; Singh, A.; et al. Nanostructured Boron Nitride with High Water Dispersibility for Boron Neutron Capture Therapy. Sci. Rep. 2016, 6, 35535. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, J.; Yang, Q.; Liu, M.; Lin, M.; Wang, T.; Zhang, Z.; Zhong, X.; Guo, N.; Lu, Y.; Xu, J.; et al. Remarkable Boron Delivery of iRGD-Modified Polymeric Nanoparticles for Boron Neutron Capture Therapy. Int. J. Nanomed. 2019, 14, 8161–8177. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, C.-Y.; Lin, J.-J.; Chang, W.-Y.; Hsieh, C.-Y.; Wu, C.-C.; Chen, H.-S.; Hsu, H.-J.; Yang, A.-S.; Hsu, M.-H.; Kuo, W.-Y. Development of theranostic active-targeting boron-containing gold nanoparticles for boron neutron capture therapy (BNCT). Colloids Surf. B Biointerfaces 2019, 183, 110387. [Google Scholar] [CrossRef] [PubMed]
- Fukuda, H.; Hiratsuka, J.; Kobayashi, T.; Sakurai, Y.; Yoshino, K.; Karashima, H.; Turu, K.; Araki, K.; Mishima, Y.; Ichihashi, M. Boron neutron capture therapy (BNCT) for malignant melanoma with special reference to absorbed doses to the normal skin and tumor. Australas. Phys. Eng. Sci. Med. 2003, 26, 97–103. [Google Scholar] [CrossRef]
- Kato, I.; Ono, K.; Sakurai, Y.; Ohmae, M.; Maruhashi, A.; Imahori, Y.; Kirihata, M.; Nakazawa, M.; Yura, Y. Effectiveness of boron neutron capture therapy for recurrent head and neck malignancies. Appl. Radiat. Isot. 2004, 61, 1069–1073. [Google Scholar] [CrossRef]
- Wittig, A.; Malago, M.; Collette, L.; Huiskamp, R.; Bührmann, S.; Nievaart, V.; Kaiser, G.M.; Jöckel, K.-H.; Schmid, K.W.; Ortmann, U.; et al. Uptake of two 10B-compounds in liver metastases of colorectal adenocarcinoma for extracorporeal irradiation with boron neutron capture therapy (EORTC Trial 11001). Int. J. Cancer 2007, 122, 1164–1171. [Google Scholar] [CrossRef]
- Zonta, A.; Pinelli, T.; Prati, U.; Roveda, L.; Ferrari, C.; Clerici, A.; Zonta, C.; Mazzini, G.; Dionigi, P.; Altieri, S.; et al. Extra-corporeal liver BNCT for the treatment of diffuse metastases: What was learned and what is still to be learned. Appl. Radiat. Isot. 2009, 67, S67–S75. [Google Scholar] [CrossRef]
- Kankaanranta, L.; Seppälä, T.; Koivunoro, H.; Saarilahti, K.; Atula, T.; Collan, J.; Salli, E.; Kortesniemi, M.; Uusi-Simola, J.; Välimäki, P.; et al. Boron Neutron Capture Therapy in the Treatment of Locally Recurred Head-and-Neck Cancer: Final Analysis of a Phase I/II Trial. Int. J. Radiat. Oncol. Biol. Phys. 2012, 82, e67–e75. [Google Scholar] [CrossRef]
- Suzuki, M.; Kato, I.; Aihara, T.; Hiratsuka, J.; Yoshimura, K.; Niimi, M.; Kimura, Y.; Ariyoshi, Y.; Haginomori, S.-I.; Sakurai, Y.; et al. Boron neutron capture therapy outcomes for advanced or recurrent head and neck cancer. J. Radiat. Res. 2013, 55, 146–153. [Google Scholar] [CrossRef]
- Ono, K.; Masunaga, S.-I.; Suzuki, M.; Kinashi, Y.; Takagaki, M.; Akaboshi, M. The combined effect of boronophenylalanine and borocaptate in boron neutron capture therapy for SCCVII tumors in mice. Int. J. Radiat. Oncol. 1999, 43, 431–436. [Google Scholar] [CrossRef]
- Yokoyama, K.; Miyatake, S.-I.; Kajimoto, Y.; Kawabata, S.; Doi, A.; Yoshida, T.; Asano, T.; Kirihata, M.; Ono, K.; Kuroiwa, T. Pharmacokinetic study of BSH and BPA in simultaneous use for BNCT. J. Neuro-Oncol. 2006, 78, 227–232. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, M.; Sakurai, Y.; Nagata, K.; Kinashi, Y.; Masunaga, S.; Ono, K.; Maruhashi, A.; Kato, I.; Fuwa, N.; Hiratsuka, J.; et al. Impact of intra-arterial administration of boron compounds on dose–volume histograms in boron neutron capture therapy for recurrent head-and-neck tumors. Int. J. Radiat. Oncol. 2006, 66, 1523–1527. [Google Scholar] [CrossRef]
- Kawabata, S.; Miyatake, S.-I.; Kuroiwa, T.; Yokoyama, K.; Doi, A.; Iida, K.; Miyata, S.; Nonoguchi, N.; Michiue, H.; Takahashi, M.; et al. Boron neutron capture therapy for newly diagnosed glioblastoma. J. Radiat. Res. 2009, 50, 51–60. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suzuki, M. Boron neutron capture therapy (BNCT): A unique role in radiotherapy with a view to entering the accelerator-based BNCT era. Int. J. Clin. Oncol. 2019, 25, 43–50. [Google Scholar] [CrossRef]
- Khabriev, R.U. Guidelines for Experimental (Preclinical) Study of New Pharmacological Substances; Medicina: Moscow, Russia, 2005. (In Russian) [Google Scholar]
- Bikchurina, M.; Bykov, T.; Kasatov, D.; Kolesnikov, I.; Makarov, A.; Shchudlo, I.; Sokolova, E.; Taskaev, S. The Measurement of the Neutron Yield of the 7Li(p,n)7Be Reaction in Lithium Targets. Biology 2021, 10, 824. [Google Scholar] [CrossRef] [PubMed]
- Zaidi, L.; Kashaeva, E.A.; Lezhnin, S.I.; Malyshkin, G.N.; Samarin, S.I.; Sycheva, T.V.; Taskaev, S.Y.; Frolov, S.A. Neutron-beam-shaping assembly for boron neutron-capture therapy. Phys. At. Nucl. 2017, 80, 60–66. [Google Scholar] [CrossRef]
- Zaidi, L.; Belgaid, M.; Taskaev, S.; Khelifi, R. Beam shaping assembly design of 7Li(p,n)7Be neutron source for boron neutron capture therapy of deep-seated tumor. Appl. Radiat. Isot. 2018, 139, 316–324. [Google Scholar] [CrossRef]
- Taskaev, S.; Bykov, T.; Kasatov, D.; Kolesnikov, I.; Koshkarev, A.; Makarov, A.; Savinov, S.; Shchudlo, I.; Sokolova, E. Measurement of the 7Li(p,p’γ)7Li reaction cross-section and 478 keV photon yield from a thick lithium target at proton energies from 0.65 MeV to 2.225 MeV. Nucl. Instrum. Methods Phys. Res. Sect. B Beam Interact. Mater. At. 2021, 502, 85–94. [Google Scholar] [CrossRef]
- Bykov, T.; Kasatov, D.; Koshkarev, A.; Makarov, A.; Porosev, V.; Savinov, G.; Shchudlo, I.; Taskaev, S.; Verkhovod, G. Initial trials of a dose monitoring detector for boron neutron capture therapy. J. Instrum. 2021, 16, P01024. [Google Scholar] [CrossRef]
- Kanygin, V.; Tsygankova, A.; Kichigin, A.; Zavjalov, E.; Razumov, I.; Guselnikova, T.; Sibirtsev, R.; Mukhamadiyarov, R. Effectiveness of different BNCT-drug injection methods. In Proceedings of the RAP Conference Proceedings, Thessaloniki, Greece, 1 May–1 June 2020; Volume 5, pp. 33–37. [Google Scholar] [CrossRef]
- Hiratsuka, J.; Fukuda, H. Malignant melanoma. In Neutron Capture Therapy: Principles and Applications; Sauerwein, W.A.G., Wittig, A., Moss, R., Nakagawa, Y., Eds.; Springer: Berlin/Heidelberg, Germany, 2012; pp. 433–448. [Google Scholar]
- Yurov, D.; Anikeev, A.; Bagryansky, P.; Brednikhin, S.; Frolov, S.; Lezhnin, S.; Prikhodko, V. Parameters optimization in a hybrid system with a gas dynamic trap based neutron source. Fusion Eng. Des. 2012, 87, 1684–1692. [Google Scholar] [CrossRef]
- Lan, T.-L.; Chou, F.-I.; Huang, W.-S.; Lin, K.-H.; Lee, Y.-Y.; Pan, P.-S.; Kuo, Y.-C.; Hsu, S.-M.; Chang, F.-C.; Liang, M.-L.; et al. Overt tumor regression after salvage boron neutron capture therapy (BNCT) for a recurrent glioblastoma patient. Ther. Radiol. Oncol. 2018, 2, 48. [Google Scholar] [CrossRef]
- Postuma, I.; González, S.; Herrera, M.; Provenzano, L.; Ferrarini, M.; Magni, C.; Protti, N.; Fatemi, S.; Vercesi, V.; Battistoni, G.; et al. A Novel Approach to Design and Evaluate BNCT Neutron Beams Combining Physical, Radiobiological, and Dosimetric Figures of Merit. Biology 2021, 10, 174. [Google Scholar] [CrossRef] [PubMed]
- Zaboronok, A.; Taskaev, S.; Volkova, O.; Mechetina, L.; Kasatova, A.; Sycheva, T.; Nakai, K.; Kasatov, D.; Makarov, A.; Kolesnikov, I.; et al. Gold Nanoparticles Permit In Situ Absorbed Dose Evaluation in Boron Neutron Capture Therapy for Malignant Tumors. Pharmaceutics 2021, 13, 1490. [Google Scholar] [CrossRef]
- Detta, A.; Cruickshank, G.S. l-Amino Acid Transporter-1 and Boronophenylalanine-Based Boron Neutron Capture Therapy of Human Brain Tumors. Cancer Res. 2009, 69, 2126–2132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wongthai, P.; Hagiwara, K.; Miyoshi, Y.; Wiriyasermkul, P.; Wei, L.; Ohgaki, R.; Kato, I.; Hamase, K.; Nagamori, S.; Kanai, Y. Boronophenylalanine, a boron delivery agent for boron neutron capture therapy, is transported by ATB 0,+, LAT 1 and LAT. Cancer Sci. 2015, 106, 279–286. [Google Scholar] [CrossRef] [Green Version]
- Yoshida, F.; Kurita, T.; Endo, K.; Nakai, K.; Shirakawa, M.; Zaboronok, A.; Tsurubuchi, T.; Ishikawa, E.; Matsumura, A. Difference in BPA uptake between glioma stem-like cells and their cancerous cells. Appl. Radiat. Isot. 2020, 164, 109234. [Google Scholar] [CrossRef] [PubMed]
- Maeda, H.; Wu, J.; Sawa, T.; Matsumura, Y.; Hori, K. Tumor vascular permeability and the EPR effect in macromolecular therapeutics: A review. J. Control. Release 2000, 65, 271–284. [Google Scholar] [CrossRef]
- Yoshida, F.; Yamamoto, T.; Nakai, K.; Zaboronok, A.; Matsuda, M.; Akutsu, H.; Ishikawa, E.; Shirakawa, M.; Matsumura, A. Pretreatment with buthionine sulfoximine enhanced uptake and retention of BSH in brain tumor. Appl. Radiat. Isot. 2014, 88, 86–88. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barth, R.F.; Yang, W.; Bartus, R.T.; Moeschberger, M.L.; Goodman, J.H. Enhanced delivery of boronophenylalanine for neutron capture therapy of brain tumors using the bradykinin analog Cereport (Receptor-Mediated Permeabilizer-7). Neurosurgery 1999, 44, 351–359. [Google Scholar] [CrossRef] [PubMed]
- Yadrovskaya, V.A.; Ulyanenko, S.E.; Savina, E.P. Synthesis and pharmacokinetics of anion- [B12H105H] 2 labeled with iodine-131 anion- [B12H105H] 2. Chem. Pharm. J. 2001, 35, 6–7. (In Russian) [Google Scholar] [CrossRef]
- Capuani, S.; Gili, T.; Bozzali, M.; Russo, S.; Porcari, P.; Cametti, C.; D’Amore, E.; Colasanti, M.; Venturini, G.; Maraviglia, B.; et al. L-DOPA Preloading Increases the Uptake of Borophenylalanine in C6 Glioma Rat Model: A New Strategy to Improve BNCT Efficacy. Int. J. Radiat. Oncol. 2008, 72, 562–567. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Watanabe, T.; Tanaka, H.; Fukutani, S.; Suzuki, M.; Hiraoka, M.; Ono, K. L-phenylalanine preloading reduces the 10B(n, α)7Li dose to the normal brain by inhibiting the uptake of boronophenylalanine in boron neutron capture therapy for brain tumours. Cancer Lett. 2016, 370, 27–32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wittig, A.; Arlinghaus, H.F.; Kriegeskotte, C.; Moss, R.L.; Appelman, K.; Schmid, K.W.; Sauerwein, W.A. Laser postionization secondary neutral mass spectrometry in tissue: A powerful tool for elemental and molecular imaging in the development of targeted drugs. Mol. Cancer Ther. 2008, 7, 1763–1771. [Google Scholar] [CrossRef] [Green Version]
- Wittig, A.; Moss, R.L.; Sauerwein, W.A. Glioblastoma, brain metastases and soft tissue sarcoma of extremities: Candidate tumors for BNCT. Appl. Radiat. Isot. 2014, 88, 46–49. [Google Scholar] [CrossRef]
- Hideghéty, K.; Sauerwein, W.; Haselsberger, K.; Grochulla, F.; Fankhauser, H.; Moss, R.; Huiskamp, R.; Gabel, D.; De Vries, M. Postoperative treatment of glioblastoma with BNCT at the Petten irradiation facility (EORTC Protocol 11961). Strahlenther. Und Onkol. 1999, 175, 111–114. [Google Scholar] [CrossRef] [PubMed]
- Hideghéty, K.; Sauerwein, W.; Wittig, A.; Götz, C.; Paquis, P.; Grochulla, F.; Haselsberger, K.; Wolbers, J.; Moss, R.; Huiskamp, R.; et al. Tissue uptake of BSH in patients with glioblastoma in the EORTC 11961 phase I BNCT trial. J. Neuro-Oncol. 2003, 62, 145–156. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, T.; Nakai, K.; Matsumura, A. Boron neutron capture therapy for glioblastoma. Cancer Lett. 2008, 262, 143–152. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Experimental Groups | Thermal Neutrons, Gy-Eq | Fast Neutrons, Gy-Eq | Boron Dose from Neutron Capture by Boron, Gy-Eq | Gamma-Ray Dose, Gy-Eq | Average Tumor Boron Concentration, µg/g | Total Absorbed Dose, Sv |
|---|---|---|---|---|---|---|
| Experiment #1 (proton energy 2.1 MeV) | ||||||
| BNCT 1 | 1.7 | 6.2 | 15.3 | 9.7 | 15 | 32.6 |
| Irradiation 1 | 1.7 | 6.2 | 0 | 9.7 | 0 | 17.6 |
| BNCT 2 | 1.7/3.4 | 6.2/12.2 | 15.3/30.6 | 9.7/19.4 | 15 | 65.8 |
| Irradiation 2 | 1.7/3.4 | 6.2/12.2 | 0 | 9.7/19.4 | 0 | 35.2 |
| Experiment #2 (proton energy 2.05 MeV) | ||||||
| BNCT 1 | 0.9 | 2.2 | 6.6 | 5 | 42 | 21.3 |
| Irradiation 1 | 0.9 | 2.2 | 0 | 5 | 0 | 8.1 |
| BNCT 2 | 0.6/1.2 | 1.48/2.96 | 4.5/9.0 | 3.4/6.8 | 42 | 28.8 |
| Irradiation 2 | 0.6/1.2 | 1.48/2.96 | 0 | 3.4/6.8 | 0 | 11.0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kanygin, V.; Razumov, I.; Zaboronok, A.; Zavjalov, E.; Kichigin, A.; Solovieva, O.; Tsygankova, A.; Guselnikova, T.; Kasatov, D.; Sycheva, T.; et al. Dose-Dependent Suppression of Human Glioblastoma Xenograft Growth by Accelerator-Based Boron Neutron Capture Therapy with Simultaneous Use of Two Boron-Containing Compounds. Biology 2021, 10, 1124. https://doi.org/10.3390/biology10111124
Kanygin V, Razumov I, Zaboronok A, Zavjalov E, Kichigin A, Solovieva O, Tsygankova A, Guselnikova T, Kasatov D, Sycheva T, et al. Dose-Dependent Suppression of Human Glioblastoma Xenograft Growth by Accelerator-Based Boron Neutron Capture Therapy with Simultaneous Use of Two Boron-Containing Compounds. Biology. 2021; 10(11):1124. https://doi.org/10.3390/biology10111124
Chicago/Turabian StyleKanygin, Vladimir, Ivan Razumov, Alexander Zaboronok, Evgenii Zavjalov, Aleksandr Kichigin, Olga Solovieva, Alphiya Tsygankova, Tatiana Guselnikova, Dmitrii Kasatov, Tatiana Sycheva, and et al. 2021. "Dose-Dependent Suppression of Human Glioblastoma Xenograft Growth by Accelerator-Based Boron Neutron Capture Therapy with Simultaneous Use of Two Boron-Containing Compounds" Biology 10, no. 11: 1124. https://doi.org/10.3390/biology10111124