
The Theoretical Framework of the Clinical Pilates Exercise Method in Managing Non-Specific Chronic Low Back Pain: A Narrative Review



Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
3. Practical Considerations
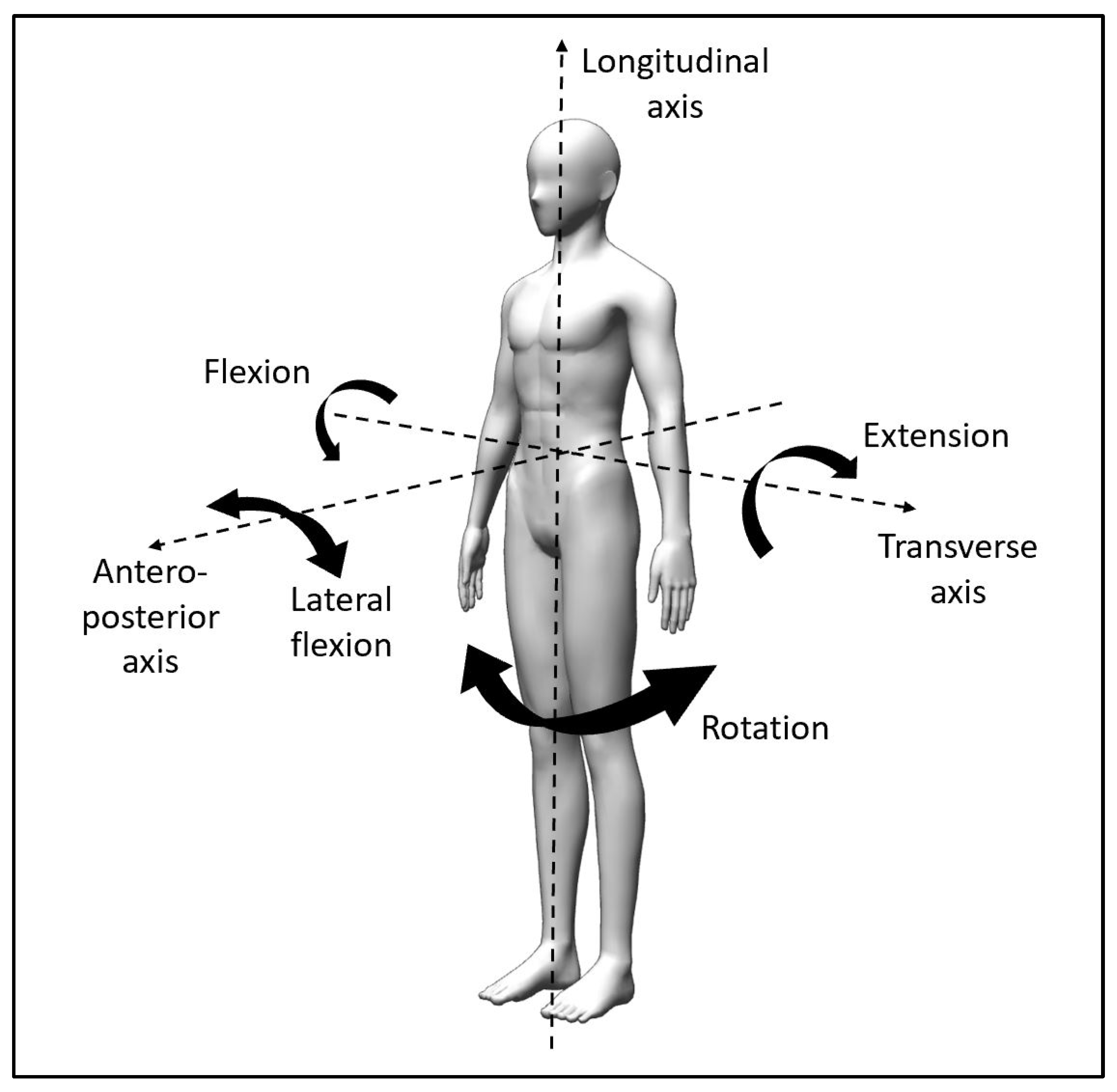
3.1. Directional Trauma—Clinical History Taking
3.1.1. Transverse Axis Trauma
3.1.2. Anteroposterior Axis Trauma
3.1.3. Longitudinal Axis Trauma
3.2. Directional Preference—Movement Assessment
3.3. Assessment Algorithms
4. Recommendations
4.1. Exercise Principles
4.1.1. Exercise Type
4.1.2. Exercise Frequency
4.1.3. Exercise Intensity
4.1.4. Exercise Duration
4.2. Safety Considerations
5. Discussion
6. Conclusions
7. Patents
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Nakamura, M.; Toyama, Y.; Nishiwaki, Y.; Ushida, T. Prevalence and characteristics of chronic musculoskeletal pain in Japan. J. Orthop. Sci. 2011, 16, 424–432. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Henschke, N.; Maher, C.G.; Refshauge, K.M.; Herbert, R.D.; Cumming, R.G.; Bleasel, J.; York, J.; Das, A.; McAuley, J.H. Prevalence of and screening for serious spinal pathology in patients presenting to primary care settings with acute low back pain. Arthritis Rheum. 2009, 60, 3072–3080. [Google Scholar] [CrossRef]
- Koes, B.W.; van Tulder, M.; Thomas, S. Diagnosis and treatment of low back pain. BMJ 2006, 332, 1430–1434. [Google Scholar] [CrossRef] [Green Version]
- Maher, C.; Underwood, M.; Buchbinder, R. Non-specific low back pain. Lancet 2017, 389, 736–747. [Google Scholar] [CrossRef] [Green Version]
- Comerford, M.; Mottram, S. Movement and stability dysfunction—Contemporary developments. Man. Ther. 2001, 6, 15–26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chou, R.; Deyo, R.; Friedly, J.; Skelly, A.; Hashimoto, R.; Weimer, M.; Fu, R.; Dana, T.; Kraegel, P.; Griffin, J.; et al. Nonpharmacologic Therapies for Low Back Pain: A Systematic Review for an American College of Physicians Clinical Practice Guideline. Ann. Intern. Med. 2017, 166, 493–505. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qaseem, A.; Wilt, T.J.; McLean, R.M.; Forciea, M.A.; Denberg, T.D.; Barry, M.J.; Boyd, C.; Chow, R.D.; Fitterman, N.; Clinical Guidelines Committee of the American College of Physicians; et al. Noninvasive treatments for acute, subacute, and chronic low back pain: A clinical practice guideline from the american college of physicians. Ann. Intern. Med. 2017, 166, 514–530. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aladro-Gonzalvo, A.R.; Araya-Vargas, G.A.; Machado-Díaz, M.; Salazar-Rojas, W. Pilates-based exercise for persistent, non-specific low back pain and associated functional disability: A meta-analysis with meta-regression. J. Bodyw. Mov. Ther. 2013, 17, 125–136. [Google Scholar] [CrossRef]
- Pereira, L.M.; Obara, K.; Dias, J.M.; Menacho, M.O.; Guariglia, D.A.; Schiavoni, D.; Pereira, H.M.; Cardoso, J. Comparing the Pilates method with no exercise or lumbar stabilization for pain and functionality in patients with chronic low back pain: Systematic review and meta-analysis. Clin. Rehabil. 2012, 26, 10–20. [Google Scholar] [CrossRef] [PubMed]
- Owen, P.J.; Miller, C.T.; Mundell, N.L.; Verswijveren, S.J.J.M.; Tagliaferri, S.D.; Brisby, H.; Bowe, S.J.; Belavy, D.L. Which specific modes of exercise training are most effective for treating low back pain? Network meta-analysis. Br. J. Sports Med. 2020, 54, 1279–1287. [Google Scholar] [CrossRef] [PubMed]
- Wajswelner, H.; Metcalf, B.; Bennell, K. Clinical pilates versus general exercise for chronic low back pain: Randomized trial. Med. Sci. Sports Exerc. 2012, 44, 1197–1205. [Google Scholar] [CrossRef]
- Donzelli, S.; Di Domenica, E.; Cova, A.M.; Galletti, R.; Giunta, N. Two different techniques in the rehabilitation treatment of low back pain: A randomized controlled trial. Eur. Med. 2006, 42, 205–210. [Google Scholar]
- Stieglitz, D.D.; Vinson, D.R.; Hampton, M.D.C. Equipment-based Pilates reduces work-related chronic low back pain and disability: A pilot study. J. Bodyw. Mov. Ther. 2016, 20, 74–82. [Google Scholar] [CrossRef] [PubMed]
- Ganesh, G.S.; Kaur, P.; Meena, S. Systematic reviews evaluating the effectiveness of motor control exercises in patients with non-specific low back pain do not consider its principles—A review. J. Bodyw. Mov. Ther. 2020, 26, 374–393. [Google Scholar] [CrossRef]
- Wells, C.; Kolt, G.; Marshall, P.; Bialocerkowski, A. The Definition and Application of Pilates Exercise to Treat People with Chronic Low Back Pain: A Delphi Survey of Australian Physical Therapists. Phys. Ther. 2014, 94, 792–805. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barton, C.; King, M.; Dascombe, B.; Taylor, N.; Silva, D.D.O.; Holden, S.; Goff, A.; Takarangi, K.; Shields, N. Many physiotherapists lack preparedness to prescribe physical activity and exercise to people with musculoskeletal pain: A multi-national survey. Phys. Ther. Sport 2021, 49, 98–105. [Google Scholar] [CrossRef]
- Tulloch, E.; Phillips, C.; Sole, G.; Carman, A.; Abbott, J.H. DMA Clinical Pilates Directional-Bias Assessment: Reliability and Predictive Validity. J. Orthop. Sports Phys. Ther. 2012, 42, 676–687. [Google Scholar] [CrossRef] [Green Version]
- Taylor, L.; Hay-Smith, E.; Dean, S. Can clinical pilates decrease pain and improve function in people complaining of non-specific chronic low back pain? A pilot study. N. Z. J. Physiother. 2011, 39, 30–38. [Google Scholar]
- Hayden, J.A.; Ellis, J.; Ogilvie, R.; Stewart, S.A.; Bagg, M.K.; Stanojevic, S.; Yamato, T.P.; Saragiotto, B.T. Some types of exercise are more effective than others in people with chronic low back pain: A network meta-analysis. J. Physiother. 2021, 67, 252–262. [Google Scholar] [CrossRef]
- Devasahayam, A.J.; Ho, D.R.Y.; Leung, E.Y.S.; Goh, M.R.; Koh, P. The effects of a novel pilates exercise prescription method on people with non-specific unilateral musculoskeletal pain: A randomised pilot trial. Proc. Singap. Healthc. 2016, 25, 201–206. [Google Scholar] [CrossRef] [Green Version]
- Meier, M.L.; Vrana, A.; Schweinhardt, P. Low Back Pain: The Potential Contribution of Supraspinal Motor Control and Proprioception. Neuroscientist 2019, 25, 583–596. [Google Scholar] [CrossRef]
- Clarkson, H.M. Musculoskeletal Assessment: Joint Range of Motion and Manual Muscle Strength; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2000. [Google Scholar]
- Colloca, C.J.; Hinrichs, R.N. The Biomechanical and Clinical Significance of the Lumbar Erector Spinae Flexion-Relaxation Phenomenon: A Review of Literature. J. Manip. Physiol. Ther. 2005, 28, 623–631. [Google Scholar] [CrossRef]
- Golding, J.S. Electromyography of the erector spinal in low back pain. Postgrad. Med. J. 1952, 28, 401–406. [Google Scholar] [CrossRef] [Green Version]
- Shirado, O.; Ito, T.; Kaneda, K.; Strax, E.T. Flexion-relaxation phenomenon in the back muscles. A comparative study between healthy subjects and patients with chronic low back pain. Am. J. Phys. Med. Rehabil. 1995, 74, 139–144. [Google Scholar]
- Hashemirad, F.; Talebian, S.; Hatef, B.; Kahlaee, A.H. The relationship between flexibility and EMG activity pattern of the erector spinae muscles during trunk flexion–extension. J. Electromyogr. Kinesiol. 2009, 19, 746–753. [Google Scholar] [CrossRef]
- Gomez, T.T. Symmetry of Lumbar Rotation and Lateral Flexion Range of Motion and Isometric Strength in Subjects with and without Low Back Pain. J. Orthop. Sports Phys. Ther. 1994, 19, 42–48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rose-Dulcina, K.; Genevay, S.; Dominguez, D.; Armand, S.; Vuillerme, N. Flexion-Relaxation Ratio Asymmetry and Its Relation with Trunk Lateral ROM in Individuals with and without Chronic Nonspecific Low Back Pain. Spine 2020, 45, E1–E9. [Google Scholar] [CrossRef] [PubMed]
- Larivière, C.; Gagnon, D.; Loisel, P. The effect of load on the coordination of the trunk for subjects with and without chronic low back pain during flexion–extension and lateral bending tasks. Clin. Biomech. 2000, 15, 407–416. [Google Scholar] [CrossRef]
- Kumar, S.; Narayan, Y.; Stein, R.B.; Snijders, C. Muscle fatigue in axial rotation of the trunk. Int. J. Ind. Ergon. 2001, 28, 113–125. [Google Scholar] [CrossRef]
- Maquirriain, J.; Ghisi, J.P. Uncommon abdominal muscle injury in a tennis player: Internal oblique strain. Br. J. Sports Med. 2006, 40, 462–463. [Google Scholar] [CrossRef]
- Johnson, R. Abdominal wall injuries: Rectus abdominis strains, oblique strains, rectus sheath hematoma. Curr. Sports Med. Rep. 2006, 5, 99–103. [Google Scholar] [CrossRef] [PubMed]
- da Fonseca, J.L.; Magini, M.; de Freitas, T.H. Laboratory gait analysis in patients with low back pain before and after a pilates intervention. J. Sport Rehabil. 2009, 18, 269–282. [Google Scholar] [CrossRef] [PubMed]
- Brooks, C.; Kennedy, S.; Marshall, P.W. Specific trunk and general exercise elicit similar changes in anticipatory postural adjustments in patients with chronic low back pain: A randomized controlled trial. Spine 2012, 37, E1543–E1550. [Google Scholar] [CrossRef]
- Docking, S.I.; Cook, J.; Rio, E. The diagnostic dartboard: Is the bullseye a correct pathoanatomical diagnosis or to guide treatment? Br. J. Sports Med. 2016, 50, 959–960. [Google Scholar] [CrossRef]
- Phillips, C. DMA Clinical Pilates Unit B Manual; DMA: Melbourne, Australia, 2015. [Google Scholar]
- Hayden, J.; van Tulder, M.; Malmivaara, A.; Koes, B. Exercise therapy for treatment of non-specific low back pain. Cochrane Database Syst. Rev. 2005, 20, CD000335. [Google Scholar] [CrossRef] [PubMed]
- Macadam, P.; Cronin, J.; Contreras, B. An Examination of the Gluteal Muscle Activity Associated with Dynamic Hip Abduction and Hip External Rotation Exercise: A Systematic Review. Int. J. Sports Phys. Ther. 2015, 10, 573–591. [Google Scholar]
- Cooper, N.A.; Scavo, K.M.; Strickland, K.J.; Tipayamongkol, N.; Nicholson, J.D.; Bewyer, D.C.; Sluka, K. Prevalence of gluteus medius weakness in people with chronic low back pain compared to healthy controls. Eur. Spine J. 2016, 25, 1258–1265. [Google Scholar] [CrossRef] [PubMed]
- Willcox, E.L.; Burden, A.M. The Influence of Varying Hip Angle and Pelvis Position on Muscle Recruitment Patterns of the Hip Abductor Muscles during the Clam Exercise. J. Orthop. Sports Phys. Ther. 2013, 43, 325–331. [Google Scholar] [CrossRef]
- Tarnanen, S.P.; Siekkinen, K.M.; Häkkinen, A.H.; Mälkiä, E.A.; Kautiainen, H.J.; Ylinen, J.J. Core Muscle Activation during Dynamic Upper Limb Exercises in Women. J. Strength Cond. Res. 2012, 26, 3217–3224. [Google Scholar] [CrossRef]
- Miyamoto, G.C.; Franco, K.; Van Dongen, J.M.; Franco, Y.R.D.S.; De Oliveira, N.T.B.; Amaral, D.D.V.; Branco, A.N.C.; Da Silva, M.L.; van Tulder, M.; Cabral, C. Different doses of Pilates-based exercise therapy for chronic low back pain: A randomised controlled trial with economic evaluation. Br. J. Sports Med. 2018, 52, 859–868. [Google Scholar] [CrossRef] [PubMed]
- Bhattacharyya, K.B. The stretch reflex and the contributions of C David Marsden. Ann. Indian Acad. Neurol. 2017, 20, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Moore, J.C. The Golgi Tendon Organ: A Review and Update. Am. J. Occup. Ther. 1984, 38, 227–236. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Dierendonck, D. Servant Leadership: A Review and Synthesis. J. Manag. 2011, 37, 1228–1261. [Google Scholar] [CrossRef] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Exercises | Directional Preference Assessed (Axes) | Descriptions |
|---|---|---|
Roll-up Variations: (i) With one side knee bend; (ii) With trunk lateral flexion to one side; (iii) Combination of (i) and (ii). | Flexion or mid-range flexion (transverse axis). Variations: (i) Unilateral flexion (transverse axis); (ii) Unilateral flexion or mid-range flexion with lateral flexion (transverse and anteroposterior axes); (iii) Unilateral flexion with lateral flexion (transverse and anteroposterior axes). | 1. Person lies flat on back with arms stretched out overhead [Starting pose]. 2. Person lifts arms up while flexing head and neck (looking at toes). 3. Person curves upper back (slouch) to lift off from the flat surface with fingers reaching for the toes. 4. Person curves lower back (slouch) to lift off from the flat surface with fingers reaching for the toes. 5. At terminal fingers to toes reach [Ending pose], the person rolls back to the flat surface by reversing the steps described. |
Bug leg Variation: With trunk lateral flexion to one side. | Unilateral flexion (transverse axis). Variation: Unilateral flexion with lateral flexion (transverse and anteroposterior axes). | 1. Person lies flat on back with arms by the side of body and hip/knee flexed to 90 degrees [Starting pose]. 2. Person straightens knee of one leg to between 45 to 60 degrees hip flexion. 3. At terminal knee extension [Ending pose], the person bends hip/knee to the starting pose. Assessor can palpate for abdominal contractions. |
Crook-lying leg Variation: With trunk lateral flexion to one side. | Unilateral mid-range flexion (transverse axis). Variation: Unilateral mid-range flexion with lateral flexion (transverse and anteroposterior axes). | 1. Person lies flat on back with arms by the side of body and hip knee/knee bent with feet firmly placed on flat surface [Starting pose]. 2. Person straightens knee of one leg to between 45 to 60 degrees hip flexion. 3. At terminal knee extension [Ending pose], the person bends hip/knee to the starting pose. Assessor can palpate for abdominal contractions. |
Prone single-leg kick Variation: With trunk lateral flexion to one side. | Unilateral extension (transverse axis). Variation: Unilateral extension with lateral flexion (transverse and anteroposterior axes). | 1. Person lies prone on flat surface with back of hands supporting forehead [Starting/Ending pose]. 2. Person bends knee of one leg to 90 degrees. 3. Person lifts bent leg off the flat surface without trunk compensatory movement. 4. Person straightens knee of lifted leg fully. 5. Person lowers leg onto the flat surface gently [Starting/Ending pose]. This test is not applicable in person who is unable to extend hip pass neutral, e.g., with tight hip flexors. Assessor can palpate for muscle contraction near posterior superior iliac spine. |
Side-lying clamshell Hip flexion angles: (a) 90 degrees; (b) 60 degrees; (c) 30 degrees; (d) 0 degree. Variations: (i) With trunk lateral flexion (Mermaid); (ii) With trunk rotation; (iii) Combination of (i) and (ii). | Lateral flexion (anteroposterior axis) coupled with: (a) Unilateral flexion (transverse axis);. (b) Unilateral mid-range flexion (transverse axis); (c) Unilateral mid-range extension (transverse axis); (d) Unilateral extension (transverse axis). Variations: (i) As above; (ii) Lateral flexion (anteroposterior axis) with rotation (longitudinal axis) and respective hip flexion angle (transverse axis); (iii) Similar to (ii). | 1. Person lies on non-tested side on flat surface with knees bent at 90 degrees and hip flexed at the assessed angle. The palm of one hand supports the head and the other hand on the hip (pelvic crest) [Starting pose]. 2. Person abducts the above knee (hip external rotation as well) to about pelvic level [Ending pose]. 3. Assessor applies break test of the manual muscle testing technique or with handheld dynamometry at the distal thigh of the abducted leg. 4. Repeat the testing at other hip flexion angles to identify the hip flexion angle that produced the peak force (directional preference confirmation) or weakest force (directional trauma identification). |
Bug roll * Variations: (i) Hands cupped at ears (reduce base of support); (ii) Arms crossed on chest (minimal base of support). | Flexion and unilateral rotation (transverse and longitudinal axes). | 1. Person lies flat on back with arms stretched out from side of body and hip/knee flexed to 90 degrees [Starting pose]. 2. Roll knees about 30 to 45 degrees to one side [Ending pose]. 3. Return knees to starting pose. Assessor can palpate for abdominal contractions. |
Knee/lumbar roll * Variation: Arms crossed on chest (minimal base of support). | Mid-range flexion and unilateral rotation (transverse and longitudinal axes). | 1. Person lies flat on back with arms by the side of body and hip knee/knee bent with feet firmly placed on flat surface [Starting pose]. 2. Roll knees about 30 to 45 degrees to one side [Ending pose]. 3. Return knees to starting pose. Assessor can palpate for abdominal contractions. |
Prone attitude rotation Variation: With arms stretched out from side of body (increase base of support). | Extension and unilateral rotation (transverse and longitudinal axes). | 1. Person lies prone on flat surface with back of hands supporting forehead [Starting pose]. 2. Person bends knee of one leg to 90 degrees. 3. Person lifts bent leg off the flat surface and twist to the contralateral side [Ending pose]. 4. Reverse the movement steps to return to the starting pose. Assessor can palpate for muscle contraction near posterior superior iliac spine. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kwok, B.C.; Lim, J.X.L.; Kong, P.W. The Theoretical Framework of the Clinical Pilates Exercise Method in Managing Non-Specific Chronic Low Back Pain: A Narrative Review. Biology 2021, 10, 1096. https://doi.org/10.3390/biology10111096
Kwok BC, Lim JXL, Kong PW. The Theoretical Framework of the Clinical Pilates Exercise Method in Managing Non-Specific Chronic Low Back Pain: A Narrative Review. Biology. 2021; 10(11):1096. https://doi.org/10.3390/biology10111096
Chicago/Turabian StyleKwok, Boon Chong, Justin Xuan Li Lim, and Pui Wah Kong. 2021. "The Theoretical Framework of the Clinical Pilates Exercise Method in Managing Non-Specific Chronic Low Back Pain: A Narrative Review" Biology 10, no. 11: 1096. https://doi.org/10.3390/biology10111096