
Efficacy and Safety of Filgrastim and Its Biosimilars to Prevent Febrile Neutropenia in Cancer Patients: A Prospective Study and Meta-Analysis


 and
and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Methods
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Outcome Measures
2.4. Data Abstraction and Analysis
3. Results
3.1. Description of Studies
3.2. Outcome of FIL versus PCT/NT by Indication
3.2.1. CIN Indication
3.2.2. AML Indication
3.2.3. SCN Indication
3.2.4. BMT Indication
3.3. Outcome of FIL versus PEG-F by Indication
3.3.1. CIN Indication
3.3.2. AML Indication
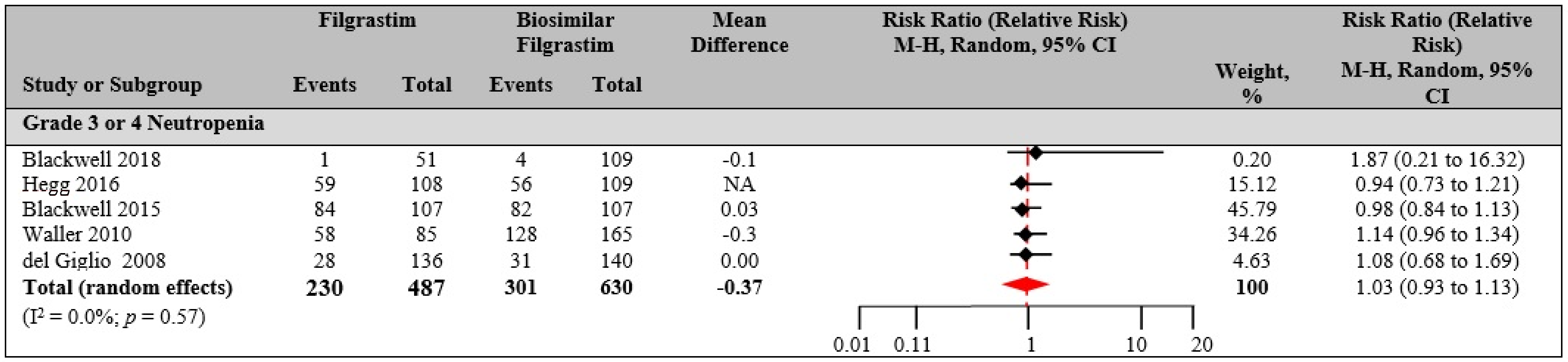
3.4. Outcome of FIL versus Bio-F
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kuderer, N.M.; Dale, D.C.; Crawford, J.; Cosler, L.E.; Lyman, G.H. Mortality, morbidity, and cost associated with febrile neutropenia in adult cancer patients. Cancer 2006, 106, 2258–2266. [Google Scholar] [CrossRef]
- Rossi, L.; Tomao, F.; Russo, G.L.; Papa, A.; Zoratto, F.; Marzano, R.; Basso, E.; Giordani, E.; Verrico, M.; Ricci, F.; et al. Efficacy and safety analysis of once per cycle pegfilgrastim and daily lenograstim in patients with breast cancer receiving adjuvant myelosuppressive chemotherapy FEC 100: A pilot study. Ther. Clin. Risk Manag. 2013, 9, 457–462. [Google Scholar] [CrossRef] [Green Version]
- Lyman, G.H.; Morrison, V.A.; Dale, D.C.; Crawford, J.; Delgado, D.J.; Fridman, M. Risk of febrile neutropenia among patients with intermediate-grade non-Hodgkin’s lymphoma receiving CHOP chemotherapy. Leuk. Lymphoma 2003, 44, 2069–2076. [Google Scholar] [CrossRef]
- Wildiers, H.; Reiser, M. Relative dose intensity of chemotherapy and its impact on outcomes in patients with early breast cancer or aggressive lymphoma. Crit. Rev. Oncol. 2011, 77, 221–240. [Google Scholar] [CrossRef]
- Chatta, G.S.; Price, T.H.; Allen, R.C.; Dale, D.C. Effects of In Vivo recombinant methionyl human granulocyte colony-stimulating factor on the neutrophil response and peripheral blood colony-forming cells in healthy young and elderly adult volunteers. Blood 1994, 84, 2923–2929. [Google Scholar] [CrossRef] [Green Version]
- Groopman, J.E.; Molina, J.-M.; Scadden, D.T. Hematopoietic growth factors. N. Engl. J. Med. 1989, 321, 1449–1459. [Google Scholar] [CrossRef]
- Crawford, J.; Ozer, H.; Stoller, R.; Johnson, D.; Lyman, G.; Tabbara, I.; Kris, M.; Grous, J.; Picozzi, V.; Rausch, G.; et al. Reduction by granulocyte colony-stimulating factor of fever and neutropenia induced by chemotherapy in patients with small-cell lung cancer. N. Engl. J. Med. 1991, 325, 164–170. [Google Scholar] [CrossRef]
- Green, M.; Koelbl, H.; Baselga, J.; Galid, A.; Guillem, V.; Gascon, P.; Siena, S.; Lalisang, R.; Samonigg, H.; Clemens, M. A randomized double-blind multicenter phase III study of fixed-dose single-administration pegfilgrastim versus daily filgrastim in patients receiving myelosuppressive chemotherapy. Ann. Oncol. 2003, 14, 29–35. [Google Scholar] [CrossRef]
- Holmes, F.; O’shaughnessy, J.; Vukelja, S.; Jones, S.; Shogan, J.; Savin, M.; Glaspy, J.; Moore, M.; Meza, L.; Wiznitzer, I. Blinded, randomized, multicenter study to evaluate single administration pegfilgrastim once per cycle versus daily filgrastim as an adjunct to chemotherapy in patients with high-risk stage II or stage III/IV breast cancer. J. Clin. Oncol. 2002, 20, 727–731. [Google Scholar] [CrossRef] [PubMed]
- Crawford, J.; Althaus, B.; Armitage, J.; Balducci, L.; Bennett, C.; Blayney, D.W.; Cataland, S.R.; Dale, D.C.; Demetri, G.D.; Erba, H.P. Myeloid growth factors: Clinical practice guidelines in oncology™. J. Natl. Compr. Cancer Netw. 2007, 5, 188–202. [Google Scholar]
- Carmona-Bayonas, A.; Jimenez-Fonseca, P.; De Castro, E.M.; Mata, E.; Biosca, M.; Custodio, A.; Espinosa, J.; Vázquez, E.G.; Henao, F.; De La Peña, F.A. SEOM clinical practice guideline: Management and prevention of febrile neutropenia in adults with solid tumors (2018). Clin. Transl. Oncol. 2018, 21, 75–86. [Google Scholar] [CrossRef] [Green Version]
- Taplitz, R.A.; Kennedy, E.B.; Bow, E.J.; Crews, J.; Gleason, C.; Hawley, D.K.; Langston, A.A.; Nastoupil, L.J.; Rajotte, M.; Rolston, K.; et al. Outpatient management of fever and neutropenia in adults treated for malignancy: American society of clinical oncology and infectious diseases society of America clinical practice guideline update. J. Clin. Oncol. 2018, 36, 1443–1453. [Google Scholar] [CrossRef] [Green Version]
- Klastersky, J.; de Naurois, J.; Rolston, K.; Rapoport, B.; Maschmeyer, G.; Aapro, M.; Herrstedt, J. Management of febrile neutropaenia: ESMO clinical practice guidelines. Ann. Oncol. 2016, 27, v111–v118. [Google Scholar] [CrossRef]
- Baden, L.R.; Swaminathan, S.; Angarone, M.; Blouin, G.; Camins, B.C.; Casper, C.; Cooper, B.; Dubberke, E.R.; Engemann, A.M.; Freifeld, A.G.; et al. Prevention and treatment of cancer-related infections, version 2.2016, NCCN clinical practice guidelines in oncology. J. Natl. Compr. Cancer Netw. 2016, 14, 882–913. [Google Scholar] [CrossRef]
- Clark, O.A.; Lyman, G.H.; Castro, A.A.; Clark, L.G.; Djulbegovic, B. Colony-stimulating factors for chemotherapy-induced febrile neutropenia: A meta-analysis of randomized controlled trials. J. Clin. Oncol. 2005, 23, 4198–4214. [Google Scholar] [CrossRef] [Green Version]
- Welte, K.; Gabrilove, J.; Bronchud, M.H.; Platzer, E.; Morstyn, G. Filgrastim (r-metHuG-CSF): The first 10 years. Blood 1996, 88, 1907–1929. [Google Scholar] [CrossRef] [Green Version]
- Amgen Inc. Neupogen (Filgrastim) Prescribing Information; Amgen Inc: Thousand Oaks, CA, USA, 2000. [Google Scholar]
- Yang, B.-B.; Savin, M.A.; Green, M. Prevention of chemotherapy-induced neutropenia with pegfilgrastim: Pharmacokinetics and patient outcomes. Chemotherapy 2012, 58, 387–398. [Google Scholar] [CrossRef]
- Holmes, F.; Jones, S.; O’shaughnessy, J.; Vukelja, S.; George, T.; Savin, M.; Richards, D.; Glaspy, J.; Meza, L.; Cohen, G. Comparable efficacy and safety profiles of once-per-cycle pegfilgrastim and daily injection filgrastim in chemotherapy-induced neutropenia: A multicenter dose-finding study in women with breast cancer. Ann. Oncol. 2002, 13, 903–909. [Google Scholar] [CrossRef] [PubMed]
- Pinto, L.; Liu, Z.; Doan, Q.; Bernal, M.; Dubois, R.; Lyman, G. Comparison of pegfilgrastim with filgrastim on febrile neutropenia, grade IV neutropenia and bone pain: A meta-analysis of randomized controlled trials. Curr. Med Res. Opin. 2007, 23, 2283–2295. [Google Scholar] [CrossRef] [PubMed]
- Rastogi, S.; Shukla, S.; Sharma, A.K.; Sarwat, M.; Srivastava, P.; Katiyar, T.; Kalaiselvan, V.; Singh, G.N. Towards a comprehensive safety understanding of granulocyte-colony stimulating factor biosimilars in treating chemotherapy associated febrile neutropenia: Trends from decades of data. Toxicol. Appl. Pharmacol. 2020, 395, 114976. [Google Scholar] [CrossRef] [PubMed]
- He, K.; Chen, H.; Gwise, T.; Casak, S.; Lemery, S.; Keegan, P.; Pazdur, R.; Sridhara, R. Statistical considerations in evaluating a biosimilar product in an oncology clinical study. Clin. Cancer Res. 2016, 22, 5167–5170. [Google Scholar] [CrossRef] [Green Version]
- Daller, J. Biosimilars: A consideration of the regulations in the United States and European union. Regul. Toxicol. Pharmacol. 2016, 76, 199–208. [Google Scholar] [CrossRef]
- Kuderer, N.M.; Dale, D.C.; Crawford, J.; Lyman, G.H. Impact of primary prophylaxis with granulocyte colony-stimulating factor on febrile neutropenia and mortality in adult cancer patients receiving chemotherapy: A systematic review. J. Clin. Oncol. 2007, 25, 3158–3167. [Google Scholar] [CrossRef]
- Lyman, G.H.; Dale, D.C.; Culakova, E.; Poniewierski, M.S.; Wolff, D.A.; Kuderer, N.M.; Huang, M.; Crawford, J. The impact of the granulocyte colony-stimulating factor on chemotherapy dose intensity and cancer survival: A systematic review and meta-analysis of randomized controlled trials. Ann. Oncol. 2013, 24, 2475–2484. [Google Scholar] [CrossRef]
- Almenar Cubells, D.; Bosch Roig, C.; Jimenez Orozco, E.; Alvarez, R.; Cuervo, J.; Diaz Fernandez, N.; Sanchez Heras, A.; Galan Brotons, A.; Giner Marco, V.; Codes, M.; et al. Effectiveness of daily versus non-daily granulocyte colony-stimulating factors in patients with solid tumours undergoing chemotherapy: A multivariate analysis of data from current practice. Eur. J. Cancer Care 2013, 22, 400–412. [Google Scholar] [CrossRef]
- Morrison, V.A.; Wong, M.; Hershman, D.; Campos, L.T.; Ding, B.; Malin, J. Observational study of the prevalence of febrile neutropenia in patients who received filgrastim or pegfilgrastim associated with 3–4 week chemotherapy regimens in community oncology practices. J. Manag. Care Pharm. 2007, 13, 337–348. [Google Scholar] [CrossRef] [Green Version]
- Naeim, A.; Henk, H.J.; Becker, L.; Chia, V.; Badre, S.; Deeter, R.G. Pegfilgrastim use associated with lower risk of hospitalization than filgrastim use: A retrospective US claims analysis. Blood 2010, 116, 3801. [Google Scholar] [CrossRef]
- Naeim, A.; Henk, H.J.; Becker, L.; Chia, V.; Badre, S.; Li, X.; Deeter, R. Pegfilgrastim prophylaxis is associated with a lower risk of hospitalization of cancer patients than filgrastim prophylaxis: A retrospective United States claims analysis of granulocyte colony-stimulating factors (G-CSF). BMC Cancer 2013, 13, 11. [Google Scholar] [CrossRef] [Green Version]
- Brito, M.; Esteves, S.; André, R.; Isidoro, M.; Moreira, A. Comparison of effectiveness of biosimilar filgrastim (Nivestim™), reference Amgen filgrastim and pegfilgrastim in febrile neutropenia primary prevention in breast cancer patients treated with neo (adjuvant) TAC: A non-interventional cohort study. Support. Care Cancer 2016, 24, 597–603. [Google Scholar] [CrossRef]
- Dale, D.C.; Crawford, J.; Klippel, Z.; Reiner, M.; Osslund, T.; Fan, E.; Morrow, P.K.; Allcott, K.; Lyman, G.H. A systematic literature review of the efficacy, effectiveness, and safety of filgrastim. Support. Care Cancer 2018, 26, 7–20. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.-Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, 14898. [Google Scholar] [CrossRef] [Green Version]
- Crawford, J.; Glaspy, J.A.; Stoller, R.G.; Tomita, D.K.; Vincent, M.E.; McGuire, B.W.; Ozer, H. Final results of a placebo-controlled study of filgrastim in small-cell lung cancer: Exploration of risk factors for febrile neutropenia. Support. Cancer Ther. 2005, 3, 36–46. [Google Scholar] [CrossRef]
- Doorduijn, J.; Van Der Holt, B.; Van Imhoff, G.; Van Der Hem, K.; Kramer, M.; Van Oers, M.; Ossenkoppele, G.; Schaafsma, M.; Verdonck, L.; Verhoef, G.; et al. CHOP compared with CHOP plus granulocyte colony-stimulating factor in elderly patients with aggressive non-hodgkin’s lymphoma. J. Clin. Oncol. 2003, 21, 3041–3050. [Google Scholar] [CrossRef]
- Osby, E.; Hagberg, H.; Kvaløy, S.; Teerenhovi, L.; Anderson, H.; Cavallin-Ståhl, E.; Holte, H.; Myhre, J.; Pertovaara, H.; Björkholm, M. CHOP is superior to CNOP in elderly patients with aggressive lymphoma while outcome is unaffected by filgrastim treatment: Results of a Nordic lymphoma group randomized trial. Blood J. Am. Soc. Hematol. 2003, 101, 3840–3848. [Google Scholar] [CrossRef] [Green Version]
- Timmer-Bonte, J.N.; De Boo, T.M.; Smit, H.J.; Biesma, B.; Wilschut, F.A.; Cheragwandi, S.A.; Termeer, A.; Hensing, C.A.; Akkermans, J.; Adang, E.M.; et al. Prevention of chemotherapy-induced febrile neutropenia by prophylactic antibiotics plus or minus granulocyte colony-stimulating factor in small-cell lung cancer: A Dutch randomized phase III study. J. Clin. Oncol. 2005, 23, 7974–7984. [Google Scholar] [CrossRef]
- Fosså, S.D.; Kaye, S.B.; Mead, G.M.; Cullen, M.; De Wit, R.; Bodrogi, I.; Van Groeningen, C.J.; De Mulder, P.H.; Stenning, S.; Lallemand, E.; et al. Filgrastim during combination chemotherapy of patients with poor-prognosis metastatic germ cell malignancy. J. Clin. Oncol. 1998, 16, 716–724. [Google Scholar] [CrossRef]
- Larson, R.A.; Dodge, R.K.; Linker, C.A.; Stone, R.M.; Powell, B.L.; Lee, E.J.; Schulman, P.; Davey, F.R.; Frankel, S.R.; Bloomfield, C.D.; et al. A randomized controlled trial of filgrastim during remission induction and consolidation chemotherapy for adults with acute lymphoblastic leukemia: CALGB study 9111. Blood 1998, 92, 1556–1564. [Google Scholar]
- Papaldo, P.; Lopez, M.; Cortesi, E.; Cammilluzzi, E.; Antimi, M.; Terzoli, E.; Lepidini, G.; Vici, P.; Barone, C.; Ferretti, G.; et al. Addition of either lonidamine or granulocyte colony-stimulating factor does not improve survival in early breast cancer patients treated with high-dose epirubicin and cyclophosphamide. J. Clin. Oncol. 2003, 21, 3462–3468. [Google Scholar] [CrossRef] [PubMed]
- Geissler, K.; Koller, E.; Hubmann, E.; Niederwieser, D.; Hinterberger, W.; Geissler, D.; Kyrle, P.; Knöbl, P.; Pabinger, I.; Thalhammer, R. Granulocyte colony-stimulating factor as an adjunct to induction chemotherapy for adult acute lymphoblastic leukemia—a randomized phase-III study. Blood J. Am. Soc. Hematol. 1997, 90, 590–596. [Google Scholar]
- Michon, J.; Hartmann, O.; Bouffet, E.; Meresse, V.; Coze, C.; Rubie, H.; Bordigoni, P.; Cattiaux, E.; Ward, N.; Bernard, J.-L.; et al. An open-label, multicentre, randomised phase 2 study of recombinant human granulocyte colony-stimulating factor (filgrastim) as an adjunct to combination chemotherapy in paediatric patients with metastatic neuroblastoma. Eur. J. Cancer 1998, 34, 1063–1069. [Google Scholar] [CrossRef]
- Zinzani, P.L.; Pavone, E.; Storti, S.; Moretti, L.; Fattori, P.P.; Guardigni, L.; Falini, B.; Gobbi, M.; Gentilini, P.; Lauta, V.M. Randomized trial with or without granulocyte colony-stimulating factor as adjunct to induction VNCOP-B treatment of elderly high-grade non-Hodgkin’s lymphoma. Blood J. Am. Soc. Hematol. 1997, 89, 3974–3979. [Google Scholar]
- Pui, C.-H.; Boyett, J.M.; Hughes, W.T.; Rivera, G.K.; Hancock, M.L.; Sandlund, J.T.; Synold, T.; Relling, M.V.; Ribeiro, R.C.; Crist, W.M.; et al. Human granulocyte colony-stimulating factor after induction chemotherapy in children with acute lymphoblastic leukemia. N. Engl. J. Med. 1997, 336, 1781–1787. [Google Scholar] [CrossRef]
- Maher, D.W.; Lieschke, G.J.; Green, M.; Bishop, J.; Stuart-Harris, R.; Wolf, M.; Sheridan, W.P.; Kefford, R.F.; Cebon, J.; Olver, I.; et al. Filgrastim in patients with chemotherapy-induced febrile neutropenia: A double-blind, placebo-controlled trial. Ann. Intern. Med. 1994, 121, 492–501. [Google Scholar] [CrossRef]
- Trillet-Lenoir, V.; Green, J.; Manegold, C.; Von Pawel, J.; Gatzemeier, U.; Lebeau, B.; Depierre, A.; Johnson, P.; Decoster, G.; Tomita, D.; et al. Recombinant granulocyte colony stimulating factor reduces the infectious complications of cytotoxic chemotherapy. Eur. J. Cancer 1993, 29, 319–324. [Google Scholar] [CrossRef]
- Blayney, D.W.; McGuire, B.W.; Cruickshank, S.E.; Johnson, D.H. Increasing chemotherapy dose density and intensity: Phase I trials in non-small cell lung cancer and non-Hodgkin’s lymphoma. Oncologist 2005, 10, 138–149. [Google Scholar] [CrossRef]
- Altwairgi, A.; Hopman, W.; Mates, M. Real-world impact of granulocyte-colony stimulating factor on febrile neutropenia. Curr. Oncol. 2013, 20, 171–179. [Google Scholar] [CrossRef] [Green Version]
- Chen, J.; Pan, Y. The safety and clinical efficacy of recombinant human granulocyte colony stimulating factor injection for colon cancer patients undergoing chemotherapy. Rev. Assoc. Méd. Bras. 2017, 63, 1061–1064. [Google Scholar] [CrossRef]
- Hershman, D.; Hurley, D.; Wong, M.; Morrison, V.A.; Malin, J.L. Impact of primary prophylaxis on febrile neutropenia within community practices in the US. J. Med. Econ. 2009, 12, 203–210. [Google Scholar] [CrossRef]
- Gilad, J.; Riesenberg, K.; Mermershtain, W.; Borer, A.; Porath, A.; Schlaeffer, F. Granulocyte-colony stimulating factor for the prevention of chemotherapy-induced febrile neutropenia in the adult cancer patient population of Southern Israel. Support. Care Cancer 1999, 7, 260–264. [Google Scholar] [CrossRef]
- Gebbia, V.; Testa, A.; Valenza, R.; Borsellino, N.; Cipolla, C.; Cannata, G.; Curto, G.; Latteri, M.; Florena, M.; Gebbia, N. A prospective evaluation of the activity of human granulocyte-colony stimulating factor on the prevention of chemotherapy-related neutropenia in patients with advanced carcinoma. J. Chemother. 1993, 5, 186–190. [Google Scholar] [CrossRef]
- Ottmann, O.; Hoelzer, D.; Gracien, E.; Ganser, A.; Kelly, K.; Reutzel, R.; Lipp, T.; Busch, F.; Schwonzen, M.; Heil, G. Concomitant granulocyte colony-stimulating factor and induction chemoradiotherapy in adult acute lymphoblastic leukemia: A randomized phase III trial. Blood 1995, 86, 444–450. [Google Scholar] [CrossRef] [PubMed]
- Usuki, K.; Urabe, A.; Masaoka, T.; Ohno, R.; Mizoguchi, H.; Hamajima, N.; Miyazaki, T.; Niitsu, Y.; Yoshida, Y.; Miura, A.; et al. Efficacy of granulocyte colony-stimulating factor in the treatment of acute myelogenous leukaemia: A multicentre randomized study. Br. J. Haematol. 2002, 116, 103–112. [Google Scholar] [CrossRef] [PubMed]
- Beksac, M.; Ali, R.; Ozcelik, T.; Özcan, M.; Ozcebe, O.; Bayık, M.; Paydas, S.; Büyükasik, Y.; Ilhan, O.; Ozkalemkas, F.; et al. Short and long term effects of granulocyte colony-stimulating factor during induction therapy in acute myeloid leukemia patients younger than 65: Results of a randomized multicenter phase III trial. Leuk. Res. 2011, 35, 340–345. [Google Scholar] [CrossRef] [PubMed]
- Heil, G.; Hoelzer, D.; Sanz, M.A.; Lechner, K.; Noens, L.; Szer, J.; Ganser, A.; Matcham, J.; Renwick, J. Long-term survival data from a phase 3 study of filgrastim as an adjunct to chemotherapy in adults with de novo acute myeloid leukemia. Leukemia 2006, 20, 404–409. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Godwin, J.E.; Kopecky, K.J.; Head, D.R.; Willman, C.L.; Leith, C.P.; Hynes, H.E.; Balcerzak, S.P.; Appelbaum, F.R. A double-blind placebo-controlled trial of granulocyte colony-stimulating factor in elderly patients with previously untreated acute myeloid leukemia: A Southwest oncology group study (9031). Blood J. Am. Soc. Hematol. 1998, 91, 3607–3615. [Google Scholar]
- Harousseau, J.; Witz, B.; Lioure, B.; Hunault-Berger, M.; Desablens, B.; Delain, M.; Guilhot, F.; Le Prise, P.; Abgrall, J.; Deconinck, E.; et al. Granulocyte colony-stimulating factor after intensive consolidation chemotherapy in acute myeloid leukemia: Results of a randomized trial of the groupe ouest-est leucémies aigues myeloblastiques. J. Clin. Oncol. 2000, 18, 780. [Google Scholar] [CrossRef]
- Heil, G.; Hoelzer, D.; Sanz, M.A.; Lechner, K.; Liu Yin, J.A.; Papa, G.; Noens, L.; Szer, J.; Ganser, A.; O’Brien, C. A randomized, double-blind, placebo-controlled, phase III study of filgrastim in remission induction and consolidation therapy for adults with de novo acute myeloid leukemia. Blood J. Am. Soc. Hematol. 1997, 90, 4710–4718. [Google Scholar]
- Moore, J.O.; Dodge, R.K.; Amrein, P.C.; Kolitz, J.; Lee, E.J.; Powell, B.; Godfrey, S.; Robert, F.; Schiffer, C.A. Granulocyte colony-stimulating factor (filgrastim) accelerates granulocyte recovery after intensive postremission chemotherapy for acute myeloid leukemia with aziridinyl benzoquinone and mitoxantrone: Cancer and leukemia group B study 9022. Blood 1997, 89, 780–788. [Google Scholar] [CrossRef]
- Dale, D.C.; Bonilla, M.A.; Davis, M.W.; Nakanishi, A.M.; Hammond, W.P.; Kurtzberg, J.; Wang, W.; Jakubowski, A.; Winton, E.; Lalezari, P. A randomized controlled phase III trial of recombinant human granulocyte colony-stimulating factor (filgrastim) for treatment of severe chronic neutropenia. Blood 1993, 81, 2496–2502. [Google Scholar] [CrossRef] [Green Version]
- Yilmaz, D.; Ritchey, A.K. Severe neutropenia in children: A single institutional experience. J. Pediatric Hematol. Oncol. 2007, 29, 513–518. [Google Scholar] [CrossRef]
- González-Vicent, M.; Madero, L.; Sevilla, J.; Ramirez, M.; Diaz, M.; Gonz, L.M.M. A prospective randomized study of clinical and economic consequences of using G-CSF following autologous peripheral blood progenitor cell (PBPC) transplantation in children. Bone Marrow Transplant. 2004, 34, 1077–1081. [Google Scholar] [CrossRef]
- Stahel, R.A.; Jost, L.M.; Honegger, H.; Betts, E.; Goebel, M.E.; Nagler, A. Randomized trial showing equivalent efficacy of filgrastim 5 μg/kg/d and 10 μg/kg/d following high-dose chemotherapy and autologous bone marrow transplantation in high-risk lymphomas. J. Clin. Oncol. 1997, 15, 1730–1735. [Google Scholar] [CrossRef] [PubMed]
- Damiani, D.; Fanin, R.; Silvestri, F.; Grimaz, S.; Infanti, L.; Geromin, A.; Cerno, M.; Michieli, M.; Rinaldi, C.; Savignano, C. Randomized trial of autologous filgrastim-primed bone marrow transplantation versus filgrastim-mobilized peripheral blood stem cell transplantation in lymphoma patients. Blood J. Am. Soc. Hematol. 1997, 90, 36–42. [Google Scholar]
- Gertz, M.A.; Gastineau, D.A.; Lacy, M.Q.; Dispenzieri, A.; Hayman, S.R.; Kumar, S.K.; Dingli, D.; Leung, N.; Wolf, R.C.; Hogan, W.J.; et al. SCT without growth factor in multiple myeloma: Engraftment kinetics, bacteremia and hospitalization. Bone Marrow Transplant. 2010, 46, 956–961. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, K.H.; Park, J.H.; Kang, S.Y.; Kim, H.Y.; Park, I.H.; Park, Y.H.; Im, Y.H.; Lee, H.J.; Park, S.; Lee, S.; et al. A randomized, multi-center, open-label, phase III study of once-per-cycle DA-3031, a pegylated G-CSF, in comparison with daily filgrastim in patients receiving TAC chemotherapy for breast cancer. Support. Care Cancer 2016, 25, 505–511. [Google Scholar] [CrossRef] [PubMed]
- Park, K.H.; Sohn, J.; Lee, S.; Kang, S.Y.; Kim, H.Y.; Im, Y.H.; Lee, H.J.; Hong, D.S.; Park, S.; Shin, S.H.; et al. A randomized, multi-center, open-label, phase II study of once-per-cycle DA-3031, a biosimilar pegylated G-CSF, compared with daily filgrastim in patients receiving TAC chemotherapy for early-stage breast cancer. Investig. New Drugs 2013, 31, 1300–1306. [Google Scholar] [CrossRef]
- Zhang, W.; Jiang, Z.; Wang, L.; Li, C.; Xia, J. An open-label, randomized, multicenter dose-finding study of once-per-cycle pegfilgrastim versus daily filgrastim in Chinese breast cancer patients receiving TAC chemotherapy. Med. Oncol. 2015, 32, 147. [Google Scholar] [CrossRef]
- Xu, F.; Zhang, Y.; Miao, Z.; Zeng, X.; Wu, B.; Cai, L.; Liu, J.; Wang, S.; Hu, X.; Zheng, W.; et al. Efficacy and safety of mecapegfilgrastim for prophylaxis of chemotherapy-induced neutropenia in patients with breast cancer: A randomized, multicenter, active-controlled phase III trial. Ann. Transl. Med. 2019, 7, 482. [Google Scholar] [CrossRef]
- Kubo, K.; Miyazaki, Y.; Murayama, T.; Shimazaki, R.; Usui, N.; Urabe, A.; Hotta, T.; Tamura, K. A randomized, double-blind trial of pegfilgrastim versus filgrastim for the management of neutropenia during CHASE (R) chemotherapy for malignant lymphoma. Br. J. Haematol. 2016, 174, 563–570. [Google Scholar] [CrossRef]
- Filon, O.; Nechaeva, M.; Burdaeva, O.; Vladimirov, V.I.; Lifirenko, I.; Kovalenko, N.V.; Kopp, M.V.; Matrosova, M.; Mukhametsina, G.; Panchenko, S. Efficacy and safety of empegfilgrastim, a novel pegylated G-CSF: Results of complete analysis after 4 cycles of myelosuppressive chemotherapy in phase III double-dummy randomized clinical study. Am. Soc. Clin. Oncol. 2015, 33 (Suppl. 15), e20735. [Google Scholar] [CrossRef]
- Salafet, O.V.; Chernovskaya, T.V.; Sheveleva, L.P.; Khorinko, A.V.; Prokopenko, T.I.; Nechaeva, M.P.; Burdaeva, O.N.; Matrosova, M.P.; Kovalenko, N.V.; Ovchinnikova, E.G.; et al. Efficacy and safety of BCD-017, a novel pegylated filgrastim: Results of open-label controlled phase II study in patients with breast cancer receiving myelosuppressive chemotherapy. J. Clin. Oncol. 2013, 31, e20593. [Google Scholar] [CrossRef]
- Grigg, A.; Solal-Celigny, P.; Hoskin, P.; Taylor, K. Open-label, randomized study of pegfilgrastim vs. daily filgrastim as an adjunct to chemotherapy in elderly patients with non-Hodgkin’s lymphoma. Leuk. Lymphoma 2003, 44, 1503–1508. [Google Scholar] [CrossRef]
- Vose, J.; Crump, M.; Lazarus, H.; Emmanouilides, C.; Schenkein, D.; Moore, J.; Frankel, S.; Flinn, I.; Lovelace, W.; Hackett, J.; et al. Randomized, multicenter, open-label study of pegfilgrastim compared with daily filgrastim after chemotherapy for lymphoma. J. Clin. Oncol. 2003, 21, 514–519. [Google Scholar] [CrossRef] [PubMed]
- Sierra, J.; Szer, J.; Kassis, J.; Herrmann, R.; Lazzarino, M.; Thomas, X.; Noga, S.J.; Baker, N.; Dansey, R.; Bosi, A. A single dose of pegfilgrastim compared with daily filgrastim for supporting neutrophil recovery in patients treated for low-to-intermediate risk acute myeloid leukemia: Results from a randomized, double-blind, phase 2 trial. BMC Cancer 2008, 8, 195. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blackwell, K.; Gascon, P.; Krendyukov, A.; Gattu, S.; Li, Y.; Harbeck, N. Safety and efficacy of alternating treatment with EP2006, a filgrastim biosimilar, and reference filgrastim: A phase III, randomised, double-blind clinical study in the prevention of severe neutropenia in patients with breast cancer receiving myelosuppressive chemotherapy. Ann. Oncol. 2018, 29, 244–249. [Google Scholar] [CrossRef]
- Blackwell, K.; Semiglazov, V.; Krasnozhon, D.; Davidenko, I.; Nelyubina, L.; Nakov, R.; Stiegler, G.; Singh, P.; Schwebig, A.; Kramer, S.; et al. Comparison of EP2006, a filgrastim biosimilar, to the reference: A phase III, randomized, double-blind clinical study in the prevention of severe neutropenia in patients with breast cancer receiving myelosuppressive chemotherapy. Ann. Oncol. 2015, 26, 1948–1953. [Google Scholar] [CrossRef]
- Del Giglio, A.; Eniu, A.; Ganea-Motan, D.; Topuzov, E.; Lubenau, H. XM02 is superior to placebo and equivalent to Neupogen™ in reducing the duration of severe neutropenia and the incidence of febrile neutropenia in cycle 1 in breast cancer patients receiving docetaxel/doxorubicin chemotherapy. BMC Cancer 2008, 8, 332. [Google Scholar] [CrossRef] [Green Version]
- Engert, A.; Griskevicius, L.; Zyuzgin, Y.; Lubenau, H.; Del Giglio, A. XM02, the first granulocyte colony-stimulating factor biosimilar, is safe and effective in reducing the duration of severe neutropenia and incidence of febrile neutropenia in patients with non-Hodgkin lymphoma receiving chemotherapy. Leuk. Lymphoma 2009, 50, 374–379. [Google Scholar] [CrossRef]
- Hegg, R.; Mattar, A.; Matos-Neto, J.N.D.; Pedrini, J.L.; Aleixo, S.B.; Rocha, R.O.; Cramer-Junior, R.P.; van-Eyll-Rocha, S. A phase III, randomized, non-inferiority study comparing the efficacy and safety of biosimilar filgrastim versus originator filgrastim for chemotherapy-induced neutropenia in breast cancer patients. Clinics 2016, 71, 586–592. [Google Scholar] [CrossRef]
- Waller, C.F.; Semiglazov, V.F.; Tjulandin, S.; Bentsion, D.; Chan, S.; Challand, R. A Phase III randomized equivalence study of biosimilar filgrastim versus amgen filgrastim in patients receiving myelosuppressive chemotherapy for breast cancer. Oncol. Res. Treat. 2010, 33, 504–511. [Google Scholar] [CrossRef]
- Sivgin, S.; Karakus, E.; Keklik, M.; Zararsiz, G.; Solmaz, M.; Kaynar, L.; Eser, B.; Cetin, M.; Unal, A. Evaluation of the efficacy and safety of original filgrastim (Neupogen®), biosimilar filgrastim (Leucostim®) and Lenograstim (Granocyte®) in CD34+ peripheral hematopoietic stem cell mobilization procedures for allogeneic hematopoietic stem cell transplant donors. Transfus. Apher. Sci. 2016, 54, 410–415. [Google Scholar] [CrossRef]
- Skopec, B.; Skerget, M.; Zontar, D.; Zadnik, V.; Zver, S. Filgrastim-alone versus pegylated filgrastim-alone for autologous peripheral blood stem cells mobilization in newly diagnosed multiple myeloma patients. Wien. Klin. Wochenschr. 2017, 129, 545–551. [Google Scholar] [CrossRef]
- Yoshimura, H.; Hotta, M.; Nakanishi, T.; Fujita, S.; Nakaya, A.; Satake, A.; Ito, T.; Ishii, K.; Nomura, S. Evaluation of a biosimilar granulocyte colony-stimulating factor (filgrastim XM02) for peripheral blood stem cell mobilization and transplantation: A single center experience in Japan. J. Blood Med. 2017, 8, 5–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Y.; Chen, L.; Liu, F.; Zhao, N.; Xu, L.; Fu, B.; Li, Y. Efficacy and tolerability of granulocyte colony-stimulating factors in cancer patients after chemotherapy: A systematic review and Bayesian network meta-analysis. Sci. Rep. 2019, 9, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Lyman, G.H.; Reiner, M.; Morrow, P.K.; Crawford, J. The effect of filgrastim or pegfilgrastim on survival outcomes of patients with cancer receiving myelosuppressive chemotherapy. Ann. Oncol. 2015, 26, 1452–1458. [Google Scholar] [CrossRef]
- Bradley, A.M.; Deal, A.M.; Buie, L.W.; Van Deventer, H. Neutropenia-associated outcomes in adults with acute myeloid leukemia receiving cytarabine consolidation chemotherapy with or without granulocyte colony-stimulating factor. Pharmacother. J. Hum. Pharmacol. Drug Ther. 2012, 32, 1070–1077. [Google Scholar] [CrossRef]
- Dale, D.C.; Cottle, T.E.; Fier, C.J.; Bolyard, A.A.; Bonilla, M.A.; Boxer, L.A.; Cham, B.; Freedman, M.H.; Kannourakis, G.; Kinsey, S.E.; et al. Severe chronic neutropenia: Treatment and follow-up of patients in the severe chronic neutropenia international registry. Am. J. Hematol. 2003, 72, 82–93. [Google Scholar] [CrossRef] [PubMed]
- Sehouli, J.; Goertz, A.; Steinle, T.; Dubois, R.; Plesnila-Frank, C.; Lalla, A.; von Minckwitz, G. Pegfilgrastim vs. filgrastim in primary prophylaxis of febrile neutropenia in patients with breast cancer after chemotherapy: A cost-effectiveness analysis for Germany. Dtsch. Med. Wochenschr. 2010, 135, 385–389. [Google Scholar] [CrossRef]
- Botteri, E.; Krendyukov, A.; Curigliano, G. Comparing granulocyte colony-stimulating factor filgrastim and pegfilgrastim to its biosimilars in terms of efficacy and safety: A meta-analysis of randomised clinical trials in breast cancer patients. Eur. J. Cancer 2018, 89, 49–55. [Google Scholar] [CrossRef] [PubMed]
- Aitken, M. Delivering on the Potential of Biosimilar Medicines. The Role of Functioning Competitive Markets; IMS Institute for Healthcare Informatics: Singapore, 2016. [Google Scholar]
- Aapro, M.; Cornes, P.; Abraham, I. Comparative cost-efficiency across the european G5 countries of various regimens of filgrastim, biosimilar filgrastim, and pegfilgrastim to reduce the incidence of chemotherapy-induced febrile neutropenia. J. Oncol. Pharm. Pract. 2012, 18, 171–179. [Google Scholar] [CrossRef] [PubMed]
- Sun, D.; Andayani, T.M.; Altyar, A.; MacDonald, K.; Abraham, I. Potential cost savings from chemotherapy-induced febrile neutropenia with biosimilar filgrastim and expanded access to targeted antineoplastic treatment across the european union G5 countries: A simulation study. Clin. Ther. 2015, 37, 842–857. [Google Scholar] [CrossRef] [PubMed]
- Tabernero, J.; Vyas, M.; Giuliani, R.; Arnold, D.; Cardoso, F.; Casali, P.G.; Cervantes, A.; Eggermont, A.M.; Eniu, A.; Jassem, J.; et al. Biosimilars: A position paper of the European Society for Medical Oncology, with particular reference to oncology prescribers. ESMO Open 2016, 1, e000142. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abboud, C.N.; Lang, N.; Fung, H.; Lammerich, A.; Buchner, A.; Liu, P.; Mueller, U.; Pettengell, R.; Diel, I.J.; Link, H.; et al. Real-world safety experience of tevagrastim/ratiograstim/biograstim and tbo-filgrastim, short-acting recombinant human granulocyte colony-stimulating factors. Support. Care Cancer 2018, 27, 2569–2577. [Google Scholar] [CrossRef]
- Yang, J.; Yu, S.; Yang, Z.; Yan, Y.; Chen, Y.; Zeng, H.; Ma, F.; Shi, Y.; Shi, Y.; Zhang, Z.; et al. Efficacy and safety of supportive care biosimilars among cancer patients: A systematic review and meta-analysis. BioDrugs 2019, 33, 373–389. [Google Scholar] [CrossRef]
- Te Poele, E.M.; Kamps, W.A.; Tamminga, R.Y.; Leeuw, J.A.; Postma, A.; de Bont, E.S. Pegfilgrastim in pediatric cancer patients. J. Pediatric Hematol. Oncol. 2005, 27, 627–629. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Tumor Type | Filgrastim Intervention and Patient Number | FN Incidence | Grade 3 or 4 Neutropenia Incidence | Definition of FN |
|---|---|---|---|---|---|
| FIL vs. PCT/NT | |||||
| Crawford et al., 2005 [33] | SCLC | N = 231 Filgrastim = 111 Placebo = 120 | Incidence of FN 38% vs. 74% p = 0.001 | Grade 4 neutropenia incidence in cycle 1 82% vs. 97% | ≥38.2 °C |
| Timmer-Bonte et al., 2005 [36] | SCLC | N = 175 Filgrastim = 90 Placebo = 85 | Incidence of FN in cycle 1:10% vs. 24% Incidence of FN 2 to 5 cycles: 11% vs. 17% p = 0.001 | NR | ≥38.2 °C |
| Doorduijun et al., 2003 [34] | NHL | N = 389 Filgrastim = 197 Placebo = 192 | Incidence of FN 36.5% vs. 44.8% p = 0.04 | NR | ≥38.2 °C |
| Obsy et al., 2003 [35] | NHL | N = 455 Filgrastim = 226 Placebo = 229 | Granulocytopenic fever (<0.5 × 109/L) CHOP arms 34% vs. 50% p = not reported | Granulocytopenia (<0.5 × 109/L) CHOP arms 55% vs. 89% | >38.5 °C once or >38.0 °C twice in 4 h |
| Obsy et al., 2003 [35] | NHL | N = 455 Filgrastim = 226 Placebo = 229 | Granulocytopenic fever (<0.5 × 109/L) CNOP arms 32% vs. 50% p = not reported | Granulocytopenia (<0.5 × 109/L) CNOP arms 64% vs. 86% | >38.5 °C once or >38.0 °C twice in 4 h |
| Papaldo et al., 2003 [39] | Breast Cancer | N = 503 Filgrastim = 254 No Filgrastim = 249 | Incidence of FN 1.2% vs. 6.6% p = 0.004 | Grade 3/4 neutropenia: 28.6 vs. 81.6% p < 0.00001 | NR |
| Fossa et al., 1998 [37] | Germ Cell | N = 259 Filgrastim = 129 No Filgrastim = 130 | Incidence of FN 20% vs. 30% p < 0.052 | NR | NR |
| Geissler et al., 1997 [40] | ALL | N = 51 Filgrastim = 25 Placebo = 26 | Incidence of FN 12% vs. 42% p = not reported | NR | >38.0 °C |
| Ottmann et al., 1995 [52] | ALL | N = 76 Filgrastim = 37 No filgrastim = 39 | Duration of prolonged neutropenia incidence 22% vs. 42% p = not reported | NR | >38.0 °C |
| Zinzani et al., 1997 [42] | NHL | N = 149 Filgrastim = 77 No filgrastim = 72 | NR | Grade 4 neutropenia incidence 23.0% vs. 55.5% p = 0.00005 | NR |
| Gebbia et al., 1993 [51] | Breast cancer | N = 86 Filgrastim = 43 Placebo = 43 | Incidence of FN 12% vs. 32% p < 0.05 | Grade 3 and 4 neutropenia 18% vs. 42% p < 0.05 | >38.0 °C |
| Trillet-Lenoir et al., 1993 [45] | SCLC | N = 129 Filgrastim = 65 Placebo = 64 | Incidence of FN 26% vs. 53% p = 0.002 | NR | ≥38.2 °C |
| Crawford et al., 1991 [7] | SCLC | N = 199 Filgrastim = 95 Placebo = 104 | Incidence of FN in cycle 1 28% vs. 57% p < 0.001 FN incidence across 6 cycles 40% vs. 77% p < 0.001 | Grade 4 neutropenia incidence in cycle 1 84% vs. 98% p = 0.001 | ≥38.2 °C |
| FIL vs. PEG-F | |||||
| Park et al., 2017 [66] | Breast Cancer | N = 74 Filgrastim = 38 DA 3031 = 36 | Incidence of FN 7.9% vs. 17.1% | NR | NR |
| Kubo et al., 2016 [70] | NHL | N = 111 Filgrastim = 56 Pegfilgrastim = 55 | Incidence of FN 55.6% vs. 56.6% p = not reported | NR | <37.5 °C |
| Zhang et al., 2015 [68] | Breast Cancer | N = 171 Filgrastim = 43 PEG 60 μg/kg = 43 PEG 100 μg/kg = 43 PEG 120 μg/kg = 42 | Incidence of FN 11.63% vs. 6.98% vs. 4.65% vs. 11.90% | NR | ≥38.2 °C |
| Park et al., 2013 [67] | Breast Cancer | N = 61 Filgrastim = 21 DA-3031 3.6 mg = 20 DA-3031 6 mg = 20 | Incidence of FN9.5% vs. 15% vs. 5% | NR | NR |
| Green et al., 2003 [8] | Breast Cancer | N = 152 Filgrastim: 75 Pegfilgrastim: 77 | Incidence of FN 15% vs. 9% | NR | ≥38.2 °C |
| Grigg et al., 2003 [73] | NHL | N = 50 Filgrastim: 22 Pegfilgrastim: 27 | Incidence of FN in cycle 1 was 0% vs. 15% | NR | ≥38.2 °C |
| Vose et al., 2003 [74] | NHL | N = 60 Filgrastim: 31 Pegfilgrastim: 29 | Incidence of FN 19% vs. 21% | Incidence of grade 4 neutropenia 68% vs. 69% | ≥38.2 °C |
| Holmes et al., 2002 [9] | Breast Cancer | N = 296 Filgrastim: 147 Pegfilgrastim: 149 | Incidence of FN 18% vs. 9% | Incidence of grade 4 neutropenia in cycle 1 79% vs. 77% | ≥38.2 °C |
| Holmes et al., 2002 [19] | Breast Cancer | N = 125 Filgrastim = 25 PEG 30 μg/kg = 19 PEG 60 μg/kg = 60 PEG 100 μg/kg = 46 | Incidence of FN 4% vs. 21% vs. 8% vs. 7% | Incidence of grade 4 neutropenia 76% vs. 95% vs. 90% vs. 74% | ≥38.2 °C |
| FIL vs. Bio-F | |||||
| Blackwell et al., 2018 [76] | Breast Cancer | N = 213 Filgrastim: 51 Switched biosimilar: 109 EP2006: 53 | Incidence of FN across cycles 2–6 0% vs. 3.4% | NR | ≥38.3 °C |
| Hegg et al., 2016 [80] | Breast Cancer | N = 217 Filgrastim: 108 Biosimilar filgrastim: 109 | NR | NR | ≥38.2 °C |
| Blackwell et al., 2015 [77] | Breast Cancer | N = 214 Filgrastim: 107 EP 2006: 107 | NR | NR | ≥38.3 °C |
| Waller et al., 2010 [81] | Breast Cancer | N = 278 Filgrastim: 95 Biosimilar filgrastim: 183 | Incidence of FN in cycle 1–3 2.4% vs. 2.4% | NR | ≥38.5 °C |
| del Giglio et al., 2008 [78] | Breast Cancer | N = 348 Filgrastim: n = 136 XM02: n = 140 Placebo/XM02: n = 72 | FN incidence 20.7% vs. 22.1% vs. 41.7% | NR | >38.5 °C |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rastogi, S.; Kalaiselvan, V.; Ali, S.; Ahmad, A.; Guru, S.A.; Sarwat, M. Efficacy and Safety of Filgrastim and Its Biosimilars to Prevent Febrile Neutropenia in Cancer Patients: A Prospective Study and Meta-Analysis. Biology 2021, 10, 1069. https://doi.org/10.3390/biology10101069
Rastogi S, Kalaiselvan V, Ali S, Ahmad A, Guru SA, Sarwat M. Efficacy and Safety of Filgrastim and Its Biosimilars to Prevent Febrile Neutropenia in Cancer Patients: A Prospective Study and Meta-Analysis. Biology. 2021; 10(10):1069. https://doi.org/10.3390/biology10101069
Chicago/Turabian StyleRastogi, Shruti, Vivekananda Kalaiselvan, Sher Ali, Ajaz Ahmad, Sameer Ahmad Guru, and Maryam Sarwat. 2021. "Efficacy and Safety of Filgrastim and Its Biosimilars to Prevent Febrile Neutropenia in Cancer Patients: A Prospective Study and Meta-Analysis" Biology 10, no. 10: 1069. https://doi.org/10.3390/biology10101069