
A Cross-Sectional Study for Association between Periodontitis and Benign Prostatic Hyperplasia Using the Korean Genome and Epidemiology Study Data

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population and Data Collection
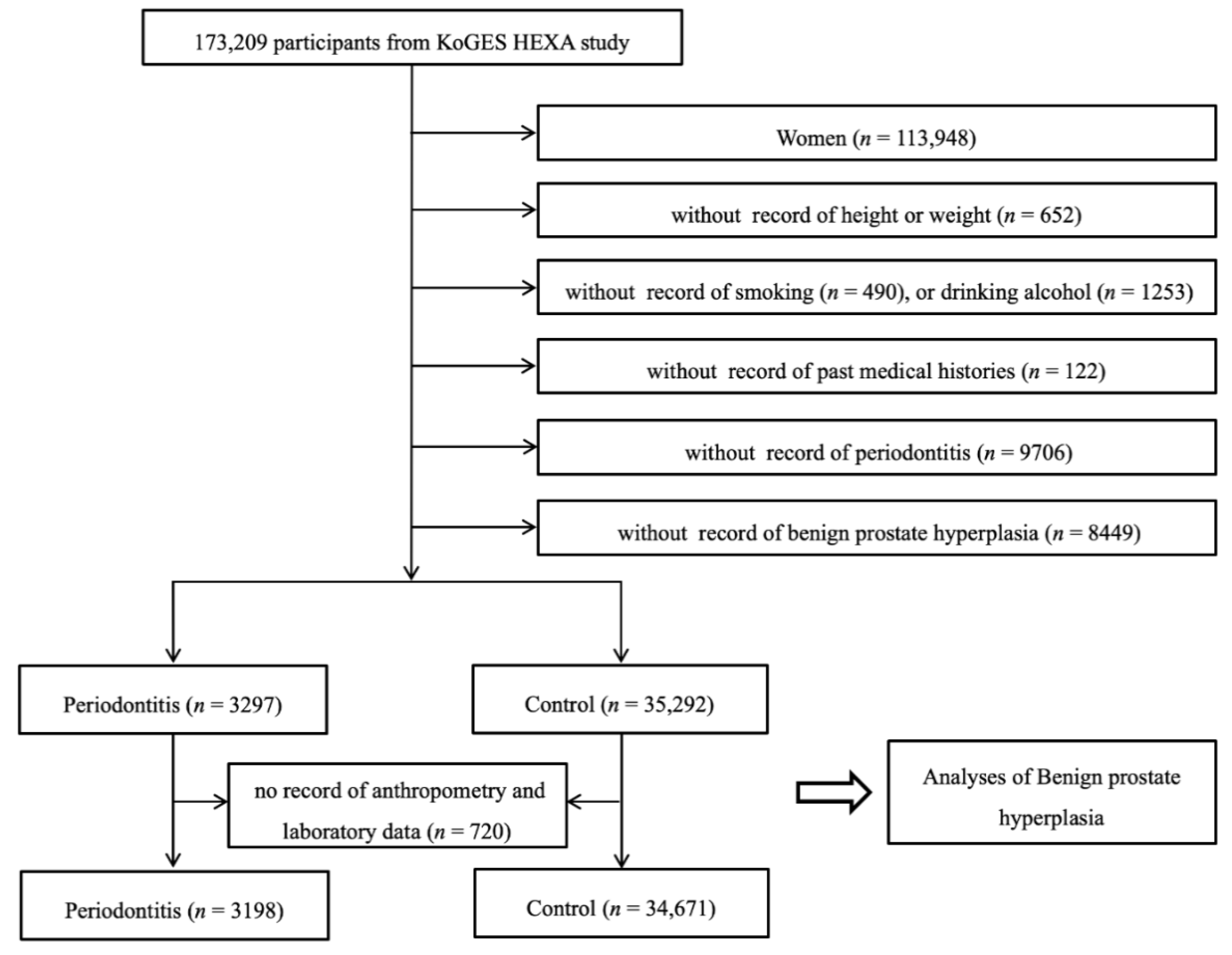
2.2. Participants Selection
2.3. Survey
2.4. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kinane, D.F.; Stathopoulou, P.G.; Papapanou, P.N. Periodontal diseases. Nat. Rev. Dis. Primers 2017, 3, 17038. [Google Scholar] [CrossRef]
- Dentino, A.; Lee, S.; Mailhot, J.; Hefti, A.F. Principles of periodontology. Periodontol. 2000 2013, 61, 16–53. [Google Scholar] [CrossRef] [Green Version]
- Eke, P.I.; Wei, L.; Thornton-Evans, G.O.; Borrell, L.N.; Borgnakke, W.S.; Dye, B.; Genco, R.J. Risk Indicators for Periodontitis in US Adults: NHANES 2009 to 2012. J. Periodontol. 2016, 87, 1174–1185. [Google Scholar] [CrossRef] [Green Version]
- Isola, G.; Polizzi, A.; Santonocito, S.; Alibrandi, A.; Ferlito, S. Expression of Salivary and Serum Malondialdehyde and Lipid Profile of Patients with Periodontitis and Coronary Heart Disease. Int. J. Mol. Sci. 2019, 20, 6061. [Google Scholar] [CrossRef] [Green Version]
- Vidal, F.; Figueredo, C.M.; Cordovil, I.; Fischer, R.G. Periodontal therapy reduces plasma levels of interleukin-6, C-reactive protein, and fibrinogen in patients with severe periodontitis and refractory arterial hypertension. J. Periodontol. 2009, 80, 786–791. [Google Scholar] [CrossRef]
- Wirth, R.; Pap, B.; Maróti, G.; Vályi, P.; Komlósi, L.; Barta, N.; Strang, O.; Minárovits, J.; Kovács, K.L. Toward Personalized Oral Diagnosis: Distinct Microbiome Clusters in Periodontitis Biofilms. Front. Cell. Infect. Microbiol. 2021, 11, 747814. [Google Scholar] [CrossRef] [PubMed]
- Slots, J. Low-Cost periodontal therapy. Periodontol. 2000 2012, 60, 110–137. [Google Scholar] [CrossRef]
- Nagarajan, R.; Miller, C.S.; Dawson, D., 3rd; Al-Sabbagh, M.; Ebersole, J.L. Cross-Talk between clinical and host-response parameters of periodontitis in smokers. J. Periodontal Res. 2017, 52, 342–352. [Google Scholar] [CrossRef] [PubMed]
- Leite, F.R.M.; Nascimento, G.G.; Scheutz, F.; López, R. Effect of Smoking on Periodontitis: A Systematic Review and Meta-regression. Am. J. Prev. Med. 2018, 54, 831–841. [Google Scholar] [CrossRef]
- Wilt, T.J.; N’Dow, J. Benign prostatic hyperplasia. Part 2—Management. BMJ 2008, 336, 206–210. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Madersbacher, S.; Sampson, N.; Culig, Z. Pathophysiology of Benign Prostatic Hyperplasia and Benign Prostatic Enlargement: A Mini-Review. Gerontology 2019, 65, 458–464. [Google Scholar] [CrossRef]
- Kim, E.H.; Larson, J.A.; Andriole, G.L. Management of Benign Prostatic Hyperplasia. Annu. Rev. Med. 2016, 67, 137–151. [Google Scholar] [CrossRef] [Green Version]
- Jokisch, J.F.; Herlemann, A.; Weinhold, P.; Magistro, G.; Stief, C.G.; Gratzke, C. Management of benign prostatic hyperplasia (BPH). MMW Fortschr. Med. 2017, 159, 58–64. [Google Scholar] [CrossRef] [PubMed]
- Nicholson, T.M.; Ricke, W.A. Androgens and estrogens in benign prostatic hyperplasia: Past, present and future. Differentiation 2011, 82, 184–199. [Google Scholar] [CrossRef] [Green Version]
- Kim, M.S.; Jung, S.I. The Urinary Tract Microbiome in Male Genitourinary Diseases: Focusing on Benign Prostate Hyperplasia and Lower Urinary Tract Symptoms. Int. Neurourol. J. 2021, 25, 3–11. [Google Scholar] [CrossRef]
- Soler, R.; Andersson, K.E.; Chancellor, M.B.; Chapple, C.R.; de Groat, W.C.; Drake, M.J.; Gratzke, C.; Lee, R.; Cruz, F. Future direction in pharmacotherapy for non-neurogenic male lower urinary tract symptoms. Eur. Urol. 2013, 64, 610–621. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.Y.; Wang, J.W.; Juan, Y.S.; Li, C.C.; Liu, C.J.; Cho, S.Y.; Yeh, H.C.; Chueh, K.S.; Wu, W.J.; Wu, D.C. The impact of urine microbiota in patients with lower urinary tract symptoms. Ann. Clin. Microbiol. Antimicrob. 2021, 20, 23. [Google Scholar] [CrossRef] [PubMed]
- Yu, H.; Meng, H.; Zhou, F.; Ni, X.; Shen, S.; Das, U.N. Urinary microbiota in patients with prostate cancer and benign prostatic hyperplasia. Arch. Med. Sci. 2015, 11, 385–394. [Google Scholar] [CrossRef] [PubMed]
- Ebersole, J.L.; Graves, C.L.; Gonzalez, O.A.; Dawson, D., 3rd; Morford, L.A.; Huja, P.E.; Hartsfield, J.K., Jr.; Huja, S.S.; Pandruvada, S.; Wallet, S.M. Aging, inflammation, immunity and periodontal disease. Periodontol. 2000 2016, 72, 54–75. [Google Scholar] [CrossRef]
- Martin, S.A.; Haren, M.T.; Marshall, V.R.; Lange, K.; Wittert, G.A.; Members of the Florey Adelaide Male Ageing, S. Prevalence and factors associated with uncomplicated storage and voiding lower urinary tract symptoms in community-dwelling Australian men. World J. Urol. 2011, 29, 179–184. [Google Scholar] [CrossRef]
- Breyer, B.N.; Sarma, A.V. Hyperglycemia and insulin resistance and the risk of BPH/LUTS: An update of recent literature. Curr. Urol. Rep. 2014, 15, 462. [Google Scholar] [CrossRef] [Green Version]
- Zeng, X.T.; Weng, H.; Jin, Y.H.; Liu, T.Z.; Liu, M.Y.; Wang, X.H. Association between Diabetes Mellitus and Hypertension in Benign Prostatic Hyperplasia Patients. Chin. Med. J. Engl. 2018, 131, 1120–1121. [Google Scholar] [CrossRef]
- Parsons, J.K.; Carter, H.B.; Partin, A.W.; Windham, B.G.; Metter, E.J.; Ferrucci, L.; Landis, P.; Platz, E.A. Metabolic factors associated with benign prostatic hyperplasia. J. Clin. Endocrinol. Metab. 2006, 91, 2562–2568. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oelke, M.; Baard, J.; Wijkstra, H.; de la Rosette, J.J.; Jonas, U.; Hofner, K. Age and bladder outlet obstruction are independently associated with detrusor overactivity in patients with benign prostatic hyperplasia. Eur. Urol. 2008, 54, 419–426. [Google Scholar] [CrossRef]
- Sebastianelli, A.; Gacci, M. Current Status of the Relationship Between Metabolic Syndrome and Lower Urinary Tract Symptoms. Eur. Urol. Focus 2018, 4, 25–27. [Google Scholar] [CrossRef] [PubMed]
- Hyun, H.; Park, Y.W.; Kwon, Y.C.; Cho, B.K.; Lee, J.H. Relationship Between Chronic Periodontitis and Lower Urinary Tract Symptoms/Benign Prostatic Hyperplasia. Int. Neurourol. J. 2021, 25, 77–83. [Google Scholar] [CrossRef] [PubMed]
- Townes, C.L.; Ali, A.; Gross, N.; Pal, D.; Williamson, S.; Heer, R.; Robson, C.N.; Pickard, R.S.; Hall, J. Prostate specific antigen enhances the innate defence of prostatic epithelium against Escherichia coli infection. Prostate 2013, 73, 1529–1537. [Google Scholar] [CrossRef] [PubMed]
- Joshi, N.; Bissada, N.F.; Bodner, D.; Maclennan, G.T.; Narendran, S.; Jurevic, R.; Skillicorn, R. Association between periodontal disease and prostate-specific antigen levels in chronic prostatitis patients. J. Periodontol. 2010, 81, 864–869. [Google Scholar] [CrossRef] [PubMed]
- Genco, R.J.; Borgnakke, W.S. Risk factors for periodontal disease. Periodontol. 2000 2013, 62, 59–94. [Google Scholar] [CrossRef]
- Vignozzi, L.; Rastrelli, G.; Corona, G.; Gacci, M.; Forti, G.; Maggi, M. Benign prostatic hyperplasia: A new metabolic disease? J. Endocrinol. Investig. 2014, 37, 313–322. [Google Scholar] [CrossRef]
- Hegde, R.; Awan, K.H. Effects of periodontal disease on systemic health. Dis. Mon. 2019, 65, 185–192. [Google Scholar] [CrossRef]
- Bajic, P.; Dornbier, R.A.; Doshi, C.P.; Wolfe, A.J.; Farooq, A.V.; Bresler, L. Implications of the Genitourinary Microbiota in Prostatic Disease. Curr. Urol. Rep. 2019, 20, 34. [Google Scholar] [CrossRef]
- Fang, C.; Wu, L.; Zhu, C.; Xie, W.Z.; Hu, H.; Zeng, X.T. A potential therapeutic strategy for prostatic disease by targeting the oral microbiome. Med. Res. Rev. 2021, 41, 1812–1834. [Google Scholar] [CrossRef]
- Estemalik, J.; Demko, C.; Bissada, N.F.; Joshi, N.; Bodner, D.; Shankar, E.; Gupta, S. Simultaneous Detection of Oral Pathogens in Subgingival Plaque and Prostatic Fluid of Men With Periodontal and Prostatic Diseases. J. Periodontol. 2017, 88, 823–829. [Google Scholar] [CrossRef] [PubMed]
- Boyapati, R.; Swarna, C.; Devulapalli, N.; Sanivarapu, S.; Katuri, K.K.; Kolaparthy, L. Unveiling the Link between Prostatitis and Periodontitis. Contemp. Clin. Dent. 2018, 9, 524–529. [Google Scholar] [CrossRef]
- Saito, T.; Shimazaki, Y. Metabolic disorders related to obesity and periodontal disease. Periodontol. 2000 2007, 43, 254–266. [Google Scholar] [CrossRef] [PubMed]
- Wu, L.; Li, B.H.; Wang, Y.Y.; Wang, C.Y.; Zi, H.; Weng, H.; Huang, Q.; Zhu, Y.J.; Zeng, X.T. Periodontal disease and risk of benign prostate hyperplasia: A cross-sectional study. Mil. Med. Res. 2019, 6, 34. [Google Scholar] [CrossRef]
- Kim, Y.; Han, B.G.; Ko, G.E.S.g. Cohort Profile: The Korean Genome and Epidemiology Study (KoGES) Consortium. Int. J. Epidemiol. 2017, 46, 1350. [Google Scholar] [CrossRef]
- Byun, S.H.; Lee, S.; Kang, S.H.; Choi, H.G.; Hong, S.J. Cross-Sectional Analysis of the Association between Periodontitis and Cardiovascular Disease Using the Korean Genome and Epidemiology Study Data. Int. J. Environ. Res. Public Health 2020, 17, 5237. [Google Scholar] [CrossRef] [PubMed]
- Byun, S.H.; Min, C.; Hong, S.J.; Choi, H.G.; Koh, D.H. Analysis of the Relation between Periodontitis and Chronic Gastritis/Peptic Ulcer: A Cross-Sectional Study Using KoGES HEXA Data. Int. J. Environ. Res. Public Health 2020, 17, 4387. [Google Scholar] [CrossRef]
- Boland, M.R.; Hripcsak, G.; Albers, D.J.; Wei, Y.; Wilcox, A.B.; Wei, J.; Li, J.; Lin, S.; Breene, M.; Myers, R.; et al. Discovering medical conditions associated with periodontitis using linked electronic health records. J. Clin. Periodontol. 2013, 40, 474–482. [Google Scholar] [CrossRef]
- Mojon, P. Oral health and respiratory infection. J. Can. Dent. Assoc. 2002, 68, 340–345. [Google Scholar]
- Darveau, R.P. Periodontitis: A polymicrobial disruption of host homeostasis. Nat. Rev. Microbiol. 2010, 8, 481–490. [Google Scholar] [CrossRef] [PubMed]
- Porter, C.M.; Shrestha, E.; Peiffer, L.B.; Sfanos, K.S. The microbiome in prostate inflammation and prostate cancer. Prostate Cancer Prostatic Dis. 2018, 21, 345–354. [Google Scholar] [CrossRef]
- Figuero, E.; Sánchez-Beltrán, M.; Cuesta-Frechoso, S.; Tejerina, J.M.; del Castro, J.A.; Gutiérrez, J.M.; Herrera, D.; Sanz, M. Detection of periodontal bacteria in atheromatous plaque by nested polymerase chain reaction. J. Periodontol. 2011, 82, 1469–1477. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Témoin, S.; Chakaki, A.; Askari, A.; El-Halaby, A.; Fitzgerald, S.; Marcus, R.E.; Han, Y.W.; Bissada, N.F. Identification of oral bacterial DNA in synovial fluid of patients with arthritis with native and failed prosthetic joints. J. Clin. Rheumatol. 2012, 18, 117–121. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gevers, D.; Kugathasan, S.; Denson, L.A.; Vázquez-Baeza, Y.; Van Treuren, W.; Ren, B.; Schwager, E.; Knights, D.; Song, S.J.; Yassour, M.; et al. The treatment-naive microbiome in new-onset Crohn’s disease. Cell Host Microbe 2014, 15, 382–392. [Google Scholar] [CrossRef] [Green Version]
- De Nunzio, C.; Presicce, F.; Tubaro, A. Inflammatory mediators in the development and progression of benign prostatic hyperplasia. Nat. Rev. Urol. 2016, 13, 613–626. [Google Scholar] [CrossRef]
- Alexander, R.B.; Ponniah, S.; Hasday, J.; Hebel, J.R. Elevated levels of proinflammatory cytokines in the semen of patients with chronic prostatitis/chronic pelvic pain syndrome. Urology 1998, 52, 744–749. [Google Scholar] [CrossRef]
- Krušlin, B.; Tomas, D.; Džombeta, T.; Milković-Periša, M.; Ulamec, M. Inflammation in Prostatic Hyperplasia and Carcinoma-Basic Scientific Approach. Front. Oncol. 2017, 7, 77. [Google Scholar] [CrossRef] [Green Version]
- Cardoso, E.M.; Reis, C.; Manzanares-Cespedes, M.C. Chronic periodontitis, inflammatory cytokines, and interrelationship with other chronic diseases. Postgrad. Med. 2018, 130, 98–104. [Google Scholar] [CrossRef] [PubMed]
- Fang, C.; Wu, L.; Zhao, M.J.; Deng, T.; Gu, J.M.; Guo, X.P.; Li, C.; Li, W.; Zeng, X.T. Periodontitis Exacerbates Benign Prostatic Hyperplasia through Regulation of Oxidative Stress and Inflammation. Oxid. Med. Cell. Longev. 2021, 2021, 2094665. [Google Scholar] [CrossRef]
- Cakir, S.S.; Polat, E.C.; Ozcan, L.; Besiroglu, H.; Otunctemur, A.; Ozbek, E. The effect of prostatic inflammation on clinical outcomes in patients with benign prostate hyperplasia. Prostate Int. 2018, 6, 71–74. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.; Dong, G.; Xiao, W.; Xiao, E.; Miao, F.; Syverson, A.; Missaghian, N.; Vafa, R.; Cabrera-Ortega, A.A.; Rossa, C., Jr.; et al. Effect of Aging on Periodontal Inflammation, Microbial Colonization, and Disease Susceptibility. J. Dent. Res. 2016, 95, 460–466. [Google Scholar] [CrossRef] [Green Version]
- Macedo Paizan, M.L.; Vilela-Martin, J.F. Is there an association between periodontitis and hypertension? Curr. Cardiol. Rev. 2014, 10, 355–361. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Characteristics | Total Participants | ||
|---|---|---|---|
| Periodontitis | Control | p-Value | |
| Age (mean, SD, y) † | 55.5 (8.1) | 53.9 (8.6) | <0.001 * |
| BMI (mean, SD, kg/m2) † | 24.5 (2.7) | 24.4 (2.7) | 0.174 |
| Income (n, %) ‡ | <0.001 * | ||
| Missing, no response | 181 (5.5) | 2171 (6.1) | |
| Lowest | 924 (28.0) | 8391 (23.8) | |
| Middle | 1369 (41.5) | 14,791 (41.9) | |
| Highest | 823 (25.0) | 9939 (28.2) | |
| Smoking status (n, %) ‡ | <0.001 * | ||
| Nonsmoker | 722 (21.9) | 9774 (27.7) | |
| Past smoker | 1474 (44.7) | 14,639 (41.5) | |
| Current smoker | 1101 (33.4) | 10,879 (30.8) | |
| Alcohol consumption (n, %) ‡ | 0.001 * | ||
| Non-drinker | 581 (17.6) | 7045 (20.0) | |
| Past drinker | 266 (8.1) | 2503 (7.1) | |
| Current drinker | 2450 (74.3) | 25,744 (72.9) | |
| Hypertension ‡ | 1094 (33.2) | 9803 (27.8) | <0.001 * |
| Diabetes mellitus ‡ | 491 (14.9) | 4019 (11.4) | <0.001 * |
| Hyperlipidemia ‡ | 686 (20.8) | 5136 (14.6) | <0.001 * |
| Ischemic heart disease ‡ | 226 (6.9) | 1668 (4.7) | <0.001 * |
| Stroke ‡ | 94 (2.9) | 672 (1.9) | <0.001 * |
| Anthropometry data (mean, SD) † | |||
| Systolic blood pressure (mmHg) | 125.5 (14.1) | 125.4 (14.2) | 0.649 |
| Diastolic blood pressure (mmHg) | 78.3 (9.4) | 78.4 (9.7) | 0.167 |
| Fasting blood sugar (mg/dL) | 101.0 (24.8) | 98.9 (23.6) | <0.001 * |
| Total cholesterol (mg/dL) | 191.3 (34.4) | 193.0 (34.9) | 0.009 * |
| Triglyceride (mg/dL) | 153.9 (111.2) | 150.3 (107.1) | 0.069 |
| HDL cholesterol (mg/dL) | 48.8 (11.6) | 49.5 (11.9) | 0.002 * |
| Blood urea nitrogen (mg/dL) | 15.4 (3.4) | 15.2 (4.1) | 0.001 * |
| Creatinine (mg/dL) | 0.97 (0.30) | 0.96 (0.24) | 0.264 |
| Uric acid (mg/dL) | 5.6 (1.3) | 5.7 (1.3) | 0.012 * |
| Benign prostatic hyperplasia (n, %) ‡ | 466 (14.1) | 3179 (9.0) | <0.001 * |
| Characteristics | Odds Ratios for Benign Prostatic Hyperplasia | |||
|---|---|---|---|---|
| Crude | p-Value | Adjusted † | p-Value | |
| Total participants (n = 38,589) | ||||
| Periodontitis | 1.66 (1.50–1.85) | <0.001 * | 1.50 (1.35–1.68) | <0.001 * |
| Control | 1.00 | 1.00 | ||
| Age ≤ 53 years (n = 18,646) | ||||
| Periodontitis | 1.79 (1.41–2.28) | <0.001 * | 1.65 (1.30–2.10) | <0.001 * |
| Control | 1.00 | 1.00 | ||
| Age > 53 years (n = 19,943) | ||||
| Periodontitis | 1.45 (1.29–1.64) | <0.001 * | 1.46 (1.29–1.65) | <0.001 * |
| Control | 1.00 | 1.00 | ||
| Characteristics | Odds Ratios for Benign Prostatic Hyperplasia | |||
|---|---|---|---|---|
| Crude | p-Value | Adjusted † | p-Value | |
| Total participants (n = 37,869) | ||||
| Periodontitis | 1.66 (1.50–1.85) | <0.001 * | 1.57 (1.41–1.76) | <0.001 * |
| Control | 1.00 | 1.00 | ||
| Age ≤ 53 years (n = 18,336) | ||||
| Periodontitis | 1.79 (1.41–2.28) | <0.001 * | 1.73 (1.36–2.21) | <0.001 * |
| Control | 1.00 | 1.00 | ||
| Age > 53 years (n = 19,533) | ||||
| Periodontitis | 1.45 (1.29–1.64) | <0.001 * | 1.52 (1.35–1.72) | <0.001 * |
| Control | 1.00 | 1.00 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Byun, S.-H.; Min, C.; Bang, W.; Yang, B.-E.; Hong, S.J.; Park, S.C.; Choi, H.G. A Cross-Sectional Study for Association between Periodontitis and Benign Prostatic Hyperplasia Using the Korean Genome and Epidemiology Study Data. Coatings 2022, 12, 265. https://doi.org/10.3390/coatings12020265
Byun S-H, Min C, Bang W, Yang B-E, Hong SJ, Park SC, Choi HG. A Cross-Sectional Study for Association between Periodontitis and Benign Prostatic Hyperplasia Using the Korean Genome and Epidemiology Study Data. Coatings. 2022; 12(2):265. https://doi.org/10.3390/coatings12020265
Chicago/Turabian StyleByun, Soo-Hwan, Chanyang Min, Woojin Bang, Byoung-Eun Yang, Seok Jin Hong, Sang Chul Park, and Hyo Geun Choi. 2022. "A Cross-Sectional Study for Association between Periodontitis and Benign Prostatic Hyperplasia Using the Korean Genome and Epidemiology Study Data" Coatings 12, no. 2: 265. https://doi.org/10.3390/coatings12020265