Day 10 Post-Prescription Audit Optimizes Antibiotic Therapy in Patients with Bloodstream Infections

 , ,
, ,  , and
, and
Abstract
:1. Introduction
2. Results
2.1. Baseline Characteristics
2.2. BSI Etiology
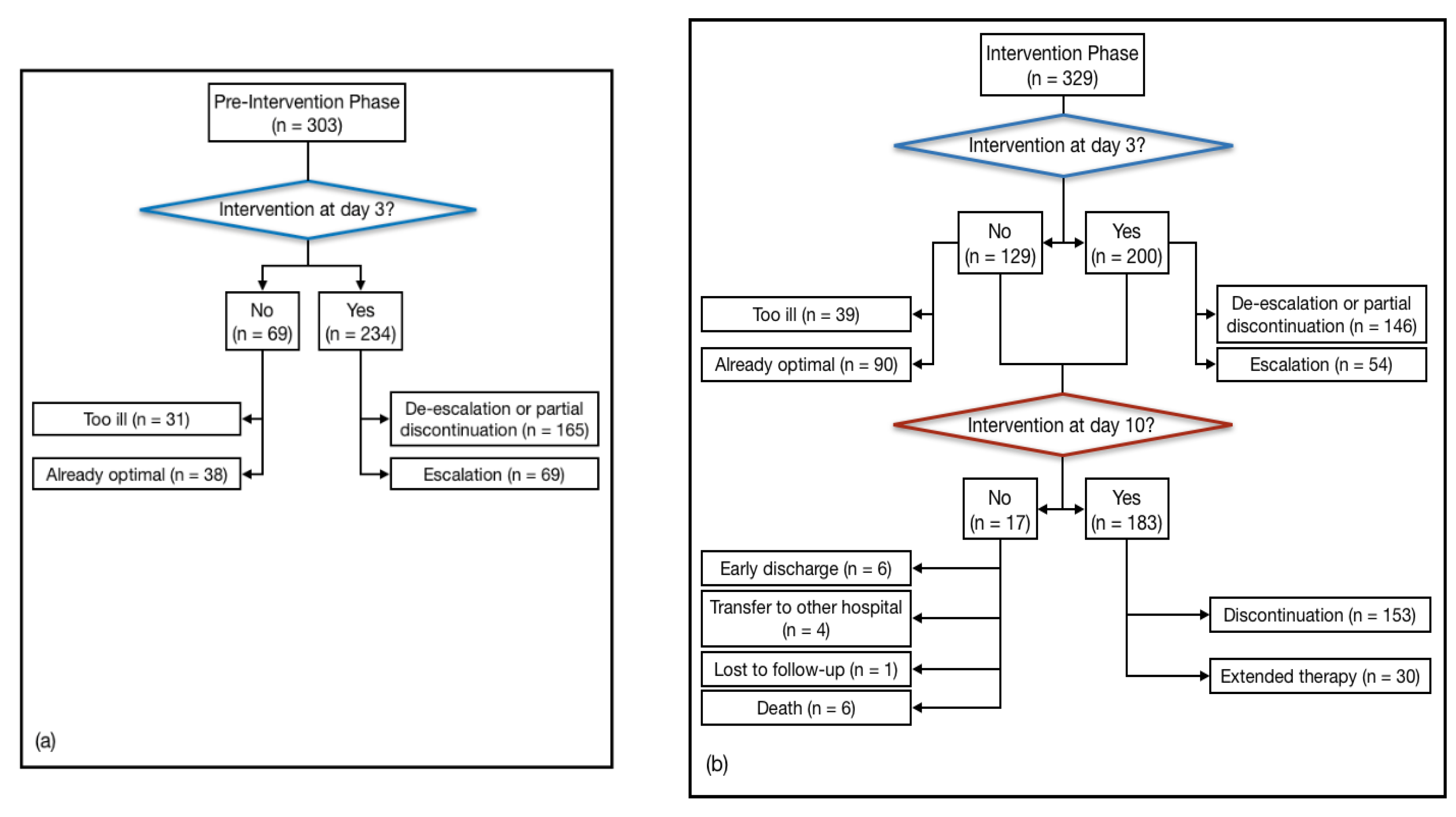
2.3. IDS Actions and Inter-Group Differences in IDS Actions at Day 3
2.4. IDS Interventions at Day 10
2.5. Inter-Group Comparison of Clinical and Organizational Outcomes
3. Discussion
4. Materials and Methods
4.1. Study Design and Setting
4.2. Study Population
4.3. Data Collection and Definitions
4.4. Study Periods and Interventions
4.5. Microbiological Analysis
4.6. Outcome Measures
4.7. Statistical Analysis
4.8. Ethical Approval
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Tackling Drug-Resistant Infections Globally: Final Report and Recommendations the Review on Antimicrobial Resistance Chaired by Jim O’neill. Available online: https://amr-review.org/sites/default/files/160518_Final%20paper_with%20cover.pdf (accessed on 29 May 2020).
- Marston, H.D.; Dixon, D.M.; Knisely, J.M.; Palmore, T.N.; Fauci, A.S. Antimicrobial resistance. JAMA J. Am. Med. Assoc. 2016. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Antibiotic Consumption in Europe. Available online: http://drive-ab.eu/wp-content/uploads/2014/09/WP1A_Final-QMs-QIs_final.pdf (accessed on 29 May 2020).
- Barlam, T.F.; Cosgrove, S.E.; Abbo, L.M.; Macdougall, C.; Schuetz, A.N.; Septimus, E.J.; Srinivasan, A.; Dellit, T.H.; Falck-Ytter, Y.T.; Fishman, N.O.; et al. Executive summary: Implementing an antibiotic stewardship program: Guidelines by the infectious diseases society of America and the society for healthcare epidemiology of America. Clin. Infect. Dis. 2016, 62, e51–e77. [Google Scholar] [CrossRef]
- Honda, H.; Murakami, S.; Tagashira, Y.; Uenoyama, Y.; Goto, K.; Takamatsu, A.; Hasegawa, S.; Tokuda, Y. Efficacy of a Postprescription Review of Broad-Spectrum Antimicrobial Agents With Feedback: A 4-Year Experience of Antimicrobial Stewardship at a Tertiary Care Center. Open Forum Infect. Dis. 2018. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sikkens, J.J.; Van Agtmael, M.A.; Peters, E.J.G.; Lettinga, K.D.; Van Der Kuip, M.; Vandenbroucke-Grauls, C.M.J.E.; Wagner, C.; Kramer, M.H.H. Behavioral approach to appropriate antimicrobial prescribing in hospitals the Dutch unique method for antimicrobial stewardship (DUMAS) participatory intervention study. JAMA Intern. Med. 2017. [Google Scholar] [CrossRef] [PubMed]
- Royer, S.; DeMerle, K.M.; Dickson, R.P.; Prescott, H.C. Shorter versus longer courses of antibiotics for infection in hospitalized patients: A systematic review and meta-analysis. J. Hosp. Med. 2018, 13, 336–342. [Google Scholar] [CrossRef] [Green Version]
- Hanretty, A.M.; Gallagher, J.C. Shortened courses of antibiotics for bacterial infections: A systematic review of randomized controlled trials. Pharmacotherapy 2018, 38, 674–687. [Google Scholar] [CrossRef]
- Sandberg, T.; Skoog, G.; Hermansson, A.B.; Kahlmeter, G.; Kuylenstierna, N.; Lannergård, A.; Otto, G.; Settergren, B.; Ekman, G.S. Ciprofloxacin for 7 days versus 14 days in women with acute pyelonephritis: A randomised, open-label and double-blind, placebo-controlled, non-inferiority trial. Lancet 2012, 380, 484–490. [Google Scholar] [CrossRef]
- Peterson, J.; Kaul, S.; Khashab, M.; Fisher, A.C.; Kahn, J.B. A double-blind, randomized comparison of levofloxacin 750 mg once-daily for five days with ciprofloxacin 400/500 mg twice-daily for 10 days for the treatment of complicated urinary tract infections and acute pyelonephritis. Urology 2008, 71, 17–22. [Google Scholar] [CrossRef]
- Uranga, A.; España, P.P.; Bilbao, A.; Quintana, J.M.; Arriaga, I.; Intxausti, M.; Lobo, J.L.; Tomás, L.; Camino, J.; Nuñez, J.; et al. Duration of antibiotic treatment in community-acquired pneumonia: A multicenter randomized clinical trial. JAMA Intern. Med. 2016, 176, 1257–1265. [Google Scholar] [CrossRef] [Green Version]
- Capellier, G.; Mockly, H.; Charpentier, C.; Annane, D.; Blasco, G.; Desmettre, T.; Roch, A.; Faisy, C.; Cousson, J.; Limat, S.; et al. Early-onset ventilator-associated pneumonia in adults randomized clinical trial: Comparison of 8 versus 15 days of antibiotic treatment. PLoS ONE 2012, 7, e41290. [Google Scholar] [CrossRef] [Green Version]
- Sawyer, R.G.; Claridge, J.A.; Nathens, A.B.; Rotstein, O.D.; Duane, T.M.; Evans, H.L.; Cook, C.H.; O’Neill, P.J.; Mazuski, J.E.; Askari, R.; et al. Trial of short-course antimicrobial therapy for intraabdominal infection. N. Engl. J. Med. 2015, 372, 1996–2005. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mermel, L.A.; Allon, M.; Bouza, E.; Craven, D.E.; Flynn, P.; O’Grady, N.P.; Raad, I.I.; Rijnders, B.J.; Sherertz, R.J.; Warren, D.K. Clinical practice guidelines for the diagnosis and management of intravascular catheter-related infection: 2009 update by the Infectious Disease Society of America. Clin. Infect. Dis. 2009, 49, 1–45. [Google Scholar] [CrossRef] [PubMed]
- Yahav, D.; Franceschini, E.; Koppel, F.; Turjeman, A.; Babich, T.; Bitterman, R.; Neuberger, A.; Ghanem-Zoubi, N.; Santoro, A.; Eliakim-Raz, N.; et al. Bacteremia Duration Study Group. Seven versus fourteen days of antibiotic therapy for uncomplicated gram-negative bacteremia: A non-inferiority randomized controlled trial. Clin. Infect. Dis. 2018. [Google Scholar] [CrossRef]
- Nelson, A.N.; Justo, J.A.; Bookstaver, P.B.; Kohn, J.; Albrecht, H.; Al-Hasan, M.N. Optimal duration of antimicrobial therapy for uncomplicated Gram-negative bloodstream infections. Infection 2017, 45, 613–620. [Google Scholar] [CrossRef]
- Sousa, A.; Pérez-Rodríguez, M.T.; Suárez, M.; Val, N.; Martínez-Lamas, L.; Nodar, A.; Longueira, R.; Crespo, M. Short- versus long-course therapy in gram-negative bacilli bloodstream infections. Eur. J. Clin. Microbiol. Infect. Dis. 2019. [Google Scholar] [CrossRef] [PubMed]
- Chotiprasitsakul, D.; Han, J.H.; Cosgrove, S.E.; Harris, A.D.; Lautenbach, E.; Conley, A.T.; Tolomeo, P.; Wise, J.; Tamma, P.D. Antibacterial Resistance Leadership Group. Comparing the Outcomes of Adults with Enterobacteriaceae Bacteremia Receiving Short-Course Versus Prolonged-Course Antibiotic Therapy in a Multicenter, Propensity Score-Matched Cohort. Clin. Infect. Dis 2018. [Google Scholar] [CrossRef]
- Tansarli, G.S.; Andreatos, N.; Pliakos, E.E.; Mylonakis, E. A Systematic Review and Meta-analysis of Antibiotic Treatment Duration for Bacteremia Due to Enterobacteriaceae. Antimicrob. Agents Chemother. 2019. [Google Scholar] [CrossRef] [Green Version]
- San-Juan, R.; Martínez-Redondo, I.; Fernández-Ruiz, M.; Ruiz-Ruigómez, M.; Corbella, L.; Hernández-Jiménez, P.; Tiago Silva, J.; López-Medrano, F.; Recio, R.; Orellana, M.A.; et al. A short course of antibiotic treatment is safe after catheter withdrawal in catheter-related bloodstream infections due to coagulase-negative staphylococci. Eur. J. Clin. Microbiol. Infect. Dis 2019. [Google Scholar] [CrossRef]
- Corey, G.R.; Stryjewski, M.E.; Everts, R.J. Short-course therapy for bloodstream infections in immunocompetent adults. Int. J. Antimicrob. Agents. 2009. [Google Scholar] [CrossRef]
- Chong, Y.P.; Moon, S.M.; Bang, K.M.; Park, H.J.; Park, S.Y.; Kim, M.N.; Park, K.H.; Kim, S.H.; Lee, S.O.; Choi, S.O.; et al. Treatment duration for uncomplicated Staphylococcus aureus bacteremia to prevent relapse: Analysis of a prospective observational cohort study. Antimicrob. Agents Chemother. 2013. [Google Scholar] [CrossRef] [Green Version]
- Murri, R.; Taccari, F.; Spanu, T.; D’Inzeo, T.; Mastrorosa, I.; Giovannenze, F.; Scoppettuolo, G.; Ventura, G.; Palazzolo, C.; Camici, M.; et al. A 72-h intervention for improvement of the rate of optimal antibiotic therapy in patients with bloodstream infections. Eur. J. Clin. Microbiol. Infect. Dis. 2018, 37. [Google Scholar] [CrossRef] [PubMed]
- Mehta, J.M.; Haynes, K.; Wileyto, E.P.; Gerber, J.S.; Timko, D.R.; Morgan, S.C.; Binkley, S.; Fishman, N.O.; Lautenbach, E.; Zaoutis, T. Comparison of Prior Authorization and Prospective Audit with Feedback for Antimicrobial Stewardship. Infect. Control. Hosp. Epidemiol. 2014. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Okumura, L.M.; Riveros, B.S.; da Silva, M.M.G.; Veroneze, I. Strategies of hospital antimicrobial stewardship associated with different health outcomes. Lancet Infect. Dis. 2016. [Google Scholar] [CrossRef]
- Tamma, P.D.; Avdic, E.; Keenan, J.F.; Zhao, Y.; Anand, G.; Cooper, J.; Dezube, R.; Hsu, S.; Cosgrove, S.E. What is the more effective antibiotic stewardship intervention: Preprescription authorization or postprescription review with feedback? Clin. Infect. Dis. 2017, 64, 537–543. [Google Scholar] [PubMed]
- Hurst, A.L.; Child, J.; Pearce, K.; Palmer, C.; Todd, J.K.; Parker, S.K. Handshake stewardship: A highly effective rounding-based antimicrobial optimization service. Pediatr. Infect. Dis. J. 2016. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Okumura, L.M.; da Silva, M.M.G.; Veroneze, I. Effects of a bundled Antimicrobial Stewardship Program on mortality: A cohort study. Braz. J. Infect. Dis. 2015. [Google Scholar] [CrossRef] [Green Version]
- Okumura, L.M.; Riveros, B.S.; Gomes-da-Silva, M.M.; Veroneze, I. A cost-effectiveness analysis of two different antimicrobial stewardship programs. Braz. J. Infect. Dis. 2016. [Google Scholar] [CrossRef] [Green Version]
- Forsblom, E.; Ruotsalainen, E.; Ollgren, J.; Järvinen, A. Telephone consultation cannot replace bedside infectious disease consultation in the management of staphylococcus aureus bacteremia. Clin. Infect. Dis. 2013. [Google Scholar] [CrossRef] [Green Version]
- Emberger, J.; Tassone, D.; Stevens, M.P.; Markley, J.D. The Current State of Antimicrobial Stewardship: Challenges, Successes, and Future Directions. Curr. Infect. Dis. Rep. 2018, 20, 31. [Google Scholar] [CrossRef]
- Schmitt, S.; Macintyre, A.T.; Bleasdale, S.C.; Ritter, J.T.; Nelson, S.B.; Berbari, E.F.; Burdette, S.D.; Hewlett, A.; Miles, M.; Robinson, P.A.; et al. Early Infectious Diseases Specialty Intervention Is Associated with Shorter Hospital Stays and Lower Readmission Rates: A Retrospective Cohort Study. Clin. Infect. Dis. 2019. [Google Scholar] [CrossRef] [Green Version]
- Schuts, E.C.; Hulscher, M.E.J.L.; Mouton, J.W.; Verduin, C.M.; Stuart, J.W.T.C.; Overdiek, H.W.P.M.; van der Linden, P.D.; Natsch, S.; Hertogh, C.M.P.M.; Wolfs, T.F.W.; et al. Current evidence on hospital antimicrobial stewardship objectives: A systematic review and meta-analysis. Lancet Infect. Dis. 2016. [Google Scholar] [CrossRef]
- Fiori, B.; D’Inzeo, T.; Di Florio, V.; De Maio, F.; De Angelis, G.; Giaquinto, A.; Campana, L.; Tanzarella, E.; Tumbarello, M.; Antonelli, M.; et al. Performance of two resin-containing blood culture media in detection of bloodstream infections and in direct matrix-assisted laser desorption ionization-time of flight mass spectrometry (MALDI-TOF MS) broth assays for isolate identification: Clinical comp. J. Clin. Microbiol. 2014. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barenfanger, J.; Graham, D.R.; Kolluri, L.; Sangwan, G.; Lawhorn, J.; Drake, C.A.; Verhulst, S.J.; Peterson, R.; Moja, L.B.; Ertmoed, M.M.; et al. Decreased mortality associated with prompt gram staining of blood cultures. Am. J. Clin. Pathol. 2008. [Google Scholar] [CrossRef] [PubMed]
- Perez, K.K.; Olsen, R.J.; Musick, W.L.; Cernoch, P.L.; Davis, J.R.; Land, G.A.; Peterson, L.E.; Musser, J.M. Integrating rapid pathogen identification and antimicrobial stewardship significantly decreases hospital costs. Arch. Pathol. Lab. Med. 2013. [Google Scholar] [CrossRef] [Green Version]
- Huang, A.M.; Newton, D.; Kunapuli, A.; Gandhi, T.N.; Washer, L.L.; Isip, J.; Collins, C.D.; Nagel, J.L. Impact of rapid organism identification via matrix-assisted laser desorption/ionization time-of-flight combined with antimicrobial stewardship team intervention in adult patients with bacteremia and candidemia. Clin. Infect. Dis. 2013. [Google Scholar] [CrossRef]
- Ferrer, R.; Martin-Loeches, I.; Phillips, G.; Osborn, T.M.; Townsend, S.; Dellinger, R.P.; Artigas, A.; Schorr, C.; Levy, M.M. Empiric antibiotic treatment reduces mortality in severe sepsis and septic shock from the first hour: Results from a guideline-based performance improvement program. Crit. Care Med. 2014. [Google Scholar] [CrossRef]
- Onakpoya, I.J.; Walker, A.S.; Tan, P.S.; Spencer, E.A.; Gbinigie, O.A.; Cook, J.; Llewelyn, M.J.; Butler, C.C. Overview of systematic reviews assessing the evidence for shorter versus longer duration antibiotic treatment for bacterial infections in secondary care. PLoS ONE 2018, 13, e0194858. [Google Scholar] [CrossRef] [Green Version]
- Timsit, J.F.; Bassetti, M.; Cremer, O.; Daikos, G.; de Waele, J.; Kallil, A.; Kipnis, E.; Kollef, M.; Laupland, K.; Paiva, J.A.; et al. Rationalizing antimicrobial therapy in the ICU: A narrative review. Intensive Care Med. 2019, 45, 172–189. [Google Scholar] [CrossRef]
- Stenehjem, E.; Hersh, A.L.; Buckel, W.R.; Jones, P.; Sheng, X.; Evans, R.S.; Burke, J.P.; Lopansri, B.K.; Srivastava, R.; Greene, T.; et al. Impact of Implementing Antibiotic Stewardship Programs in 15 Small Hospitals: A Cluster-Randomized Intervention. Clin. Infect. Dis 2018. [Google Scholar] [CrossRef]
- Baur, D.; Gladstone, B.P.; Burkert, F.; Carrara, E.; Foschi, F.; Döbele, S.; Tacconelli, E. Effect of antibiotic stewardship on the incidence of infection and colonisation with antibiotic-resistant bacteria and Clostridium difficile infection: A systematic review and meta-analysis. Lancet Infect. Dis. 2017. [Google Scholar] [CrossRef]
- Magiorakos, A.P.; Srinivasan, A.; Carey, R.B.; Carmeli, Y.; Falagas, M.E.; Giske, C.G.; Harbarth, S.; Hindler, J.F.; Kahlmeter, G.; Olsson-Liljequist, B.; et al. Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria: An international expert proposal for interim standard definitions for acquired resistance. Clin. Microbiol. Infect. 2012. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Knaus, W.A.; Draper, E.A.; Wagner, D.P.; Zimmerman, J. APACHE II: A severity of disease classification system. Crit. Care Med. 1985, 13, 818–829. [Google Scholar] [CrossRef] [PubMed]
- Fiori, B.; D’Inzeo, T.; Giaquinto, A.; Menchinelli, G.; Liotti, F.M.; De Maio, F.; De Angelis, G.; Quaranta, G.; Nagel, D.; Tumbarello, M.; et al. Optimized Use of the MALDI BioTyper System and the FilmArray BCID Panel for Direct Identification of Microbial Pathogens from Positive Blood Cultures. J. Clin. Microbiol. 2016. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- The European Committee on Antimicrobial Susceptibility Testing—EUCAST Home Page. Available online: http://www.eucast.org (accessed on 22 July 2020).
- University College London—UCL Home >> UCL Antimicrobial Resistance >> Reporting Guidelines >> ORION statement. Available online: https://www.ucl.ac.uk/amr/Reporting_Guidelines/ORION (accessed on 22 July 2020).


{kind=link}
| Characteristic | Total n = 632 | Pre-IP n = 303 | IP n = 329 | p |
|---|---|---|---|---|
| Age, mean, years (SD) | 71 (15.2) | 67.7 (15.6) | 69.7 (14.8) | 0.15 |
| Males (%) | 385 (60.9) | 123 (40.6) | 124 (37.7) | 0.49 |
| Number of comorbidities (SD) | 1.00 (0.9) | 1.2 (0.9) | 0.7 (0.8) | <0.001 |
| Ward (%) | ||||
| Medical | 424 (67.1) | 204 (67.3) | 220 (66.9) | |
| Surgical | 208 (32.9) | 99 (32.7) | 109 (33.1) | 0.01 |
| Hospitalization in the previous 90 days (%) | 224 (35.4) | 116 (38.3) | 108 (32.8) | 0.08 |
| Antibiotic therapy in the previous 30 days (%) | 150 (23.7) | 89 (29.4) | 61 (18.5) | 0.002 |
| Central venous catheter | 238 (37.6) | 139 (45.9) | 99 (30.1) | 0.001 |
| APACHE II score, mean (SD) | 11.8 (5.9) | 12.5 (6.2) | 10.2 (5.0) | <0.001 |
| Septic shock (%) | 28 (4.4) | 14 (5.1) | 14 (5.6) | 0.95 |
| Polymicrobial (%) | 104 (16.5) | 66 (21.8) | 38 (11.6) | <0.001 |
| Multi-drug resistant BSI (%) | 194 (30.7) | 100 (33.0) | 99 (30.1) | <0.001 |
| Gram-Positive Bacteria | n of Samples |
|---|---|
| Staphylococci | |
| Coagulase-negative | 43 |
| Methicillin-sensitive Staphylococcus aureus | 64 |
| Methicillin-resistant Staphylococcus aureus | 30 |
| Enterococci | |
| Enterococcus faecalis | 29 |
| Enterococcus faecium | 9 |
| Streptococcus pneumoniae | 6 |
| Streptococcus spp. | 18 |
| Gram-negative bacteria | |
| Escherichia coli | 69 |
| ESBL-producing | 48 |
| Klebsiella spp. | 26 |
| K. aerogenes | |
| K. pneumoniae | 26 |
| ESBL-producing | 5 |
| Carbapenemase-producing | 27 |
| Acinetobacter XDR3 | 20 |
| Proteus mirabilis | 8 |
| MDR | 5 |
| Pseudomonas aeruginosa | 19 |
| MDR | 9 |
| Stenotrophomonas maltophilia | 2 |
| Intervention | Total n = 632 | Pre-IP n = 303 | IP n = 329 | p |
|---|---|---|---|---|
| Intervention done (%) | 434 (68.6) | 234 (77.2) | 200 (60.8) | <0.001 |
| De-escalation or partial discontinuation (%) at day 3 | 165 (70.5) | 146 (73) | ||
| Escalation (%) at day 3 | 69 (29.4) | 54 (27) | ||
| Discontinuation of therapy after 10 days re-evaluation | - | 153 (62.7) | ||
| Study intervention not feasible (%) | 198 (31.3) | 69 (22.8) | 129 (39.2) | <0.001 |
| Patient too ill (%) | 31 (44.9) | 39 (30.2) | ||
| Optimal therapy already ongoing (%) | 38 (55) | 90 (69.7) |
| Outcome | Total n = 632 | Pre-IP n = 303 | IP n = 329 | p |
|---|---|---|---|---|
| Time to start of antibiotic therapy, mean, days (SD) | 0.5 (0.9) | 0.5 (1.0) | 0.49 (0.86) | 0.002 |
| Time to start of effective antibiotic therapy, mean, days (SD) | 1.0 (1.5) | 1.51 (1.8) | 0.89 (1.2) | <0.0001 |
| Time to start of optimal antibiotic therapy, mean, days (SD) | 2.0 (2.3) | 3.03 (2.5) | 2.29 (2.1) | <0.0001 |
| Number of effective therapy cases (%) | 96.1 (13.2) | 89.8 (14.6) | 93.3 (11.6) | <0.0001 |
| Number of patients receiving effective therapy (%) | 629 (99.5) | 301 (99.3) | 328 (99.7) | 0.01 |
| Number of optimal therapy cases (%) | 97 (24.5) | 87.2 (28.0) | 92.9 (20.5) | <0.0001 |
| Number of patients receiving optimal therapy (%) | 589 (93.1) | 275 (90.8) | 314 (95.4) | <0.0001 |
| Duration of antibiotic therapy, mean, days (SD) | 17.40 (14.5) | 18.1 (11.4) | 16.8 (12.7) | <0.0001 |
| Length of hospitalization, mean, days (SD) | 16 (19.3) | 24.1 (20.8) | 20.6 (17.7) | 0.001 |
| Number of deaths at 30 days (%) | 105 (16.6) | 64 (21.1) | 64 (19.5) | 0.12 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Murri, R.; Palazzolo, C.; Giovannenze, F.; Taccari, F.; Camici, M.; Spanu, T.; Posteraro, B.; Sanguinetti, M.; Cauda, R.; Fantoni, M. Day 10 Post-Prescription Audit Optimizes Antibiotic Therapy in Patients with Bloodstream Infections. Antibiotics 2020, 9, 437. https://doi.org/10.3390/antibiotics9080437
Murri R, Palazzolo C, Giovannenze F, Taccari F, Camici M, Spanu T, Posteraro B, Sanguinetti M, Cauda R, Fantoni M. Day 10 Post-Prescription Audit Optimizes Antibiotic Therapy in Patients with Bloodstream Infections. Antibiotics. 2020; 9(8):437. https://doi.org/10.3390/antibiotics9080437
Chicago/Turabian StyleMurri, Rita, Claudia Palazzolo, Francesca Giovannenze, Francesco Taccari, Marta Camici, Teresa Spanu, Brunella Posteraro, Maurizio Sanguinetti, Roberto Cauda, and Massimo Fantoni. 2020. "Day 10 Post-Prescription Audit Optimizes Antibiotic Therapy in Patients with Bloodstream Infections" Antibiotics 9, no. 8: 437. https://doi.org/10.3390/antibiotics9080437