Prevention of Pseudomonas aeruginosa Biofilm Formation on Soft Contact Lenses by Allium sativum Fermented Extract (BGE) and Cannabinol Oil Extract (CBD)

 , ,
, , 
 , and
, and
Abstract
:1. Introduction
2. Results
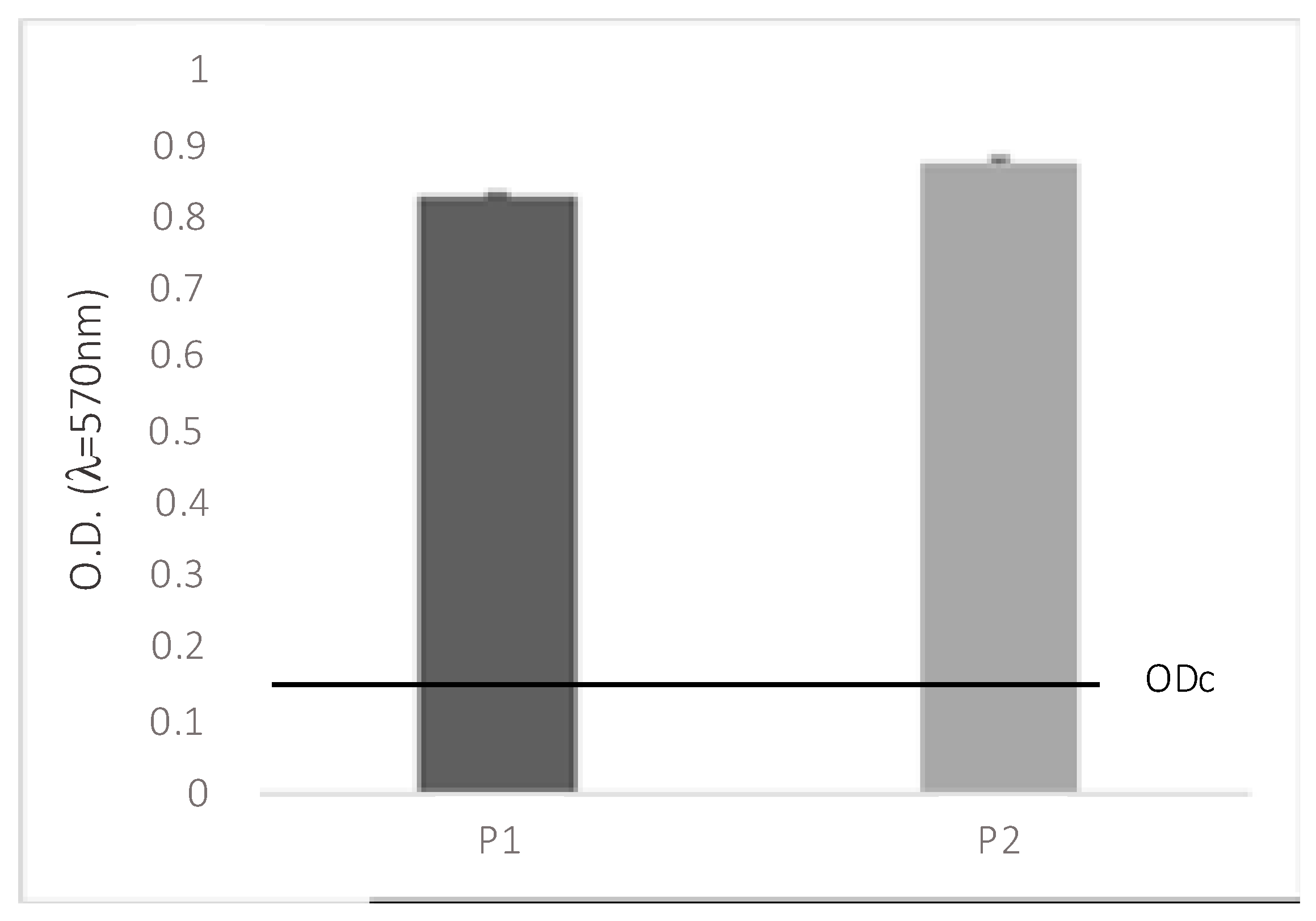
2.1. Assessment of Biofilm Formation
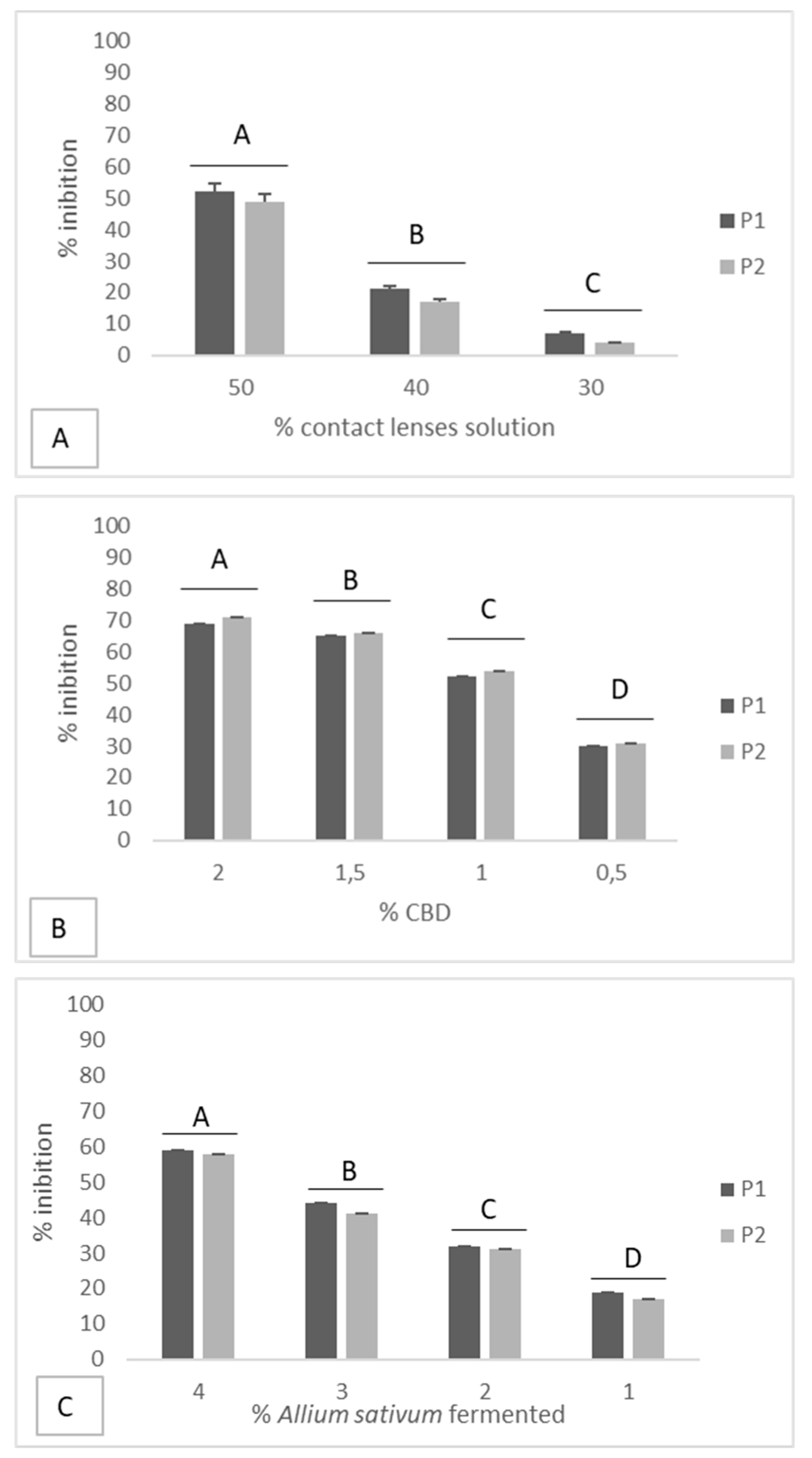
2.2. Effectiveness of Disinfectant Solution and Natural Compounds on the Inhibition of Biofilms
2.3. Prevention of Biofilm Formation
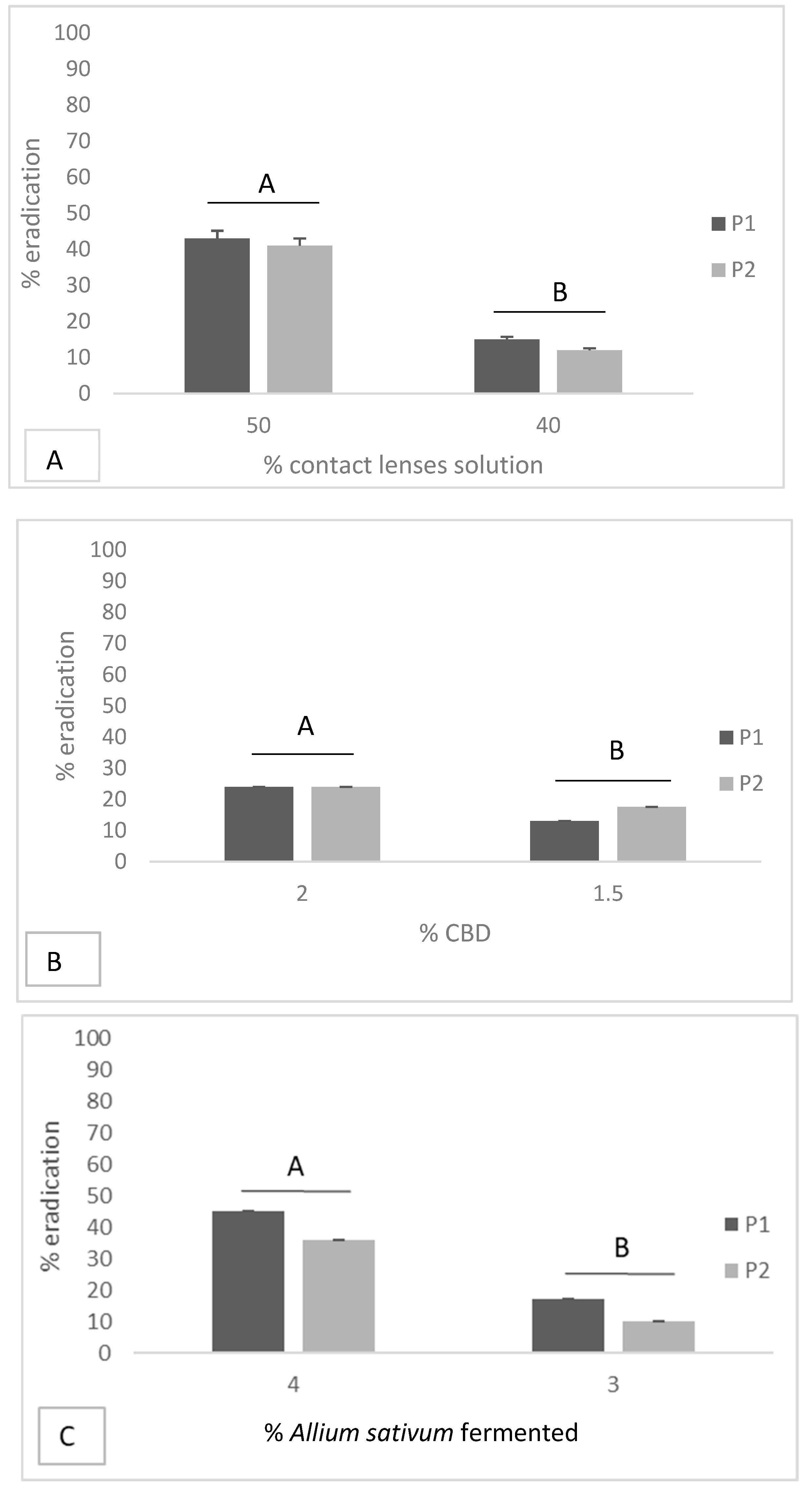
2.4. Eradication of Biofilm Formation
2.5. Determination of Fractional Inhibitory Concentration Index
3. Discussion
4. Materials and Methods
4.1. Bacterial Culture
4.2. Screened Compounds
4.3. Biofilm Production
4.4. Determination of Minimum Inhibitory Concentration of Screened Compounds
4.5. Effectiveness of Screened Compounds on Inhibition and Eradication of Biofilm Formation
4.6. Determination of Fractional Inhibitory Concentration Index
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Steele, K.R.; Szczotka-Flynn, L. Epidemiology of contact lens-induced infiltrates: An updated review. Clin. Exp. Optom. 2017, 100, 473–481. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cope, J.R.; Collier, S.A.; Nethercut, H.; Jones, J.M.; Yates, K.; Yoder, J.S. Risk Behaviors for Contact Lens-Related Eye Infections Among Adults and Adolescents—United States, 2016. MMWR Morb. Mortal. Wkly. Rep. 2017, 66, 841–845. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chalmers, R.L.; Wagner, H.; Mitchell, G.L.; Lam, D.Y.; Kinoshita, B.T.; Jansen, M.E.; Richdale, K.; Sorbara, L.; McMahon, T.T. Age and other risk factors for corneal infiltrative and inflammatory events in young soft contact lens wearers from the Contact Lens Assessment in Youth (CLAY) study. Investig. Ophthalmol. Vis. Sci. 2011, 52, 6690–6696. [Google Scholar] [CrossRef] [PubMed]
- Wagner, H.; Richdale, K.; Mitchell, G.L.; Lam, D.Y.; Jansen, M.E.; Kinoshita, B.T.; Sorbara, L.; Chalmers, R.L. Age, behavior, environment, and health factors in the soft contact lens risk survey. Optom. Vis. Sci. 2014, 91, 252–261. [Google Scholar] [CrossRef] [PubMed]
- Cope, J.R.; Collier, S.A.; Rao, M.M.; Chalmers, R.; Mitchell, G.L.; Richdale, K.; Wagner, H.; Kinoshita, B.T.; Lam, D.Y.; Sorbara, L.; et al. Contact Lens Wearer Demographics and Risk Behaviors for Contact Lens-Related Eye Infections–United States, 2014. MMWR Morb. Mortal. Wkly. Rep. 2015, 64, 865–870. [Google Scholar] [CrossRef] [Green Version]
- Correa, P.C.; Lui, A.C.F.; Silva, C.B.; Gracitelli, C.P.B.; Mimica, L.M.; Sasagawa, S.M.; Netto, A.L. Study of the Effectiveness of Multipurpose Solutions on the Bacterial Disinfection of Silicone Hydrogel Contact Lenses In Vitro. Eye Contact Lens 2018, 44, S24–S28. [Google Scholar] [CrossRef]
- Pachigolla, G.; Blomquist, P.; Cavanagh, H.D. Microbial keratitis pathogens and antibiotic susceptibilities: A 5-year review of cases at an urban county hospital in north Texas. Eye Contact Lens 2007, 33, 45–49. [Google Scholar] [CrossRef]
- Laxmi Narayana, B.; Rao, P.; Bhat, S.; Vidyalakshmi, K. Comparison of the Antimicrobial Efficacy of Various Contact Lens Solutions to Inhibit the Growth of Pseudomonas aeruginosa and Staphylococcus aureus. Int. J. Microbial. 2018, 2018, 5916712. [Google Scholar] [CrossRef]
- Gabriel, M.M.; McAnally, C.; Bartell, J. Antimicrobial Efficacy of Multipurpose Disinfecting Solutions in the Presence of Contact Lenses and Lens Cases. Eye Contact Lens 2018, 44, 125–131. [Google Scholar] [CrossRef] [Green Version]
- El-Ganiny, A.M.; Shaker, G.H.; Aboelazm, A.A.; El-Dash, H.A. Prevention of Bacterial Biofilm Formation on Soft Contact Lenses Using Natural Compounds. J. Ophthalmic Inflamm. Infect. 2017, 7, 11. [Google Scholar] [CrossRef]
- Artini, M.; Cellini, A.; Papa, R.; Tilotta, M.; Scoarughi, G.L.; Gazzola, S.; Fontana, C.; Tempera, G.; Cocconcelli, P.S.; Selan, L. Adhesive behaviour and virulence of coagulase negative staphylococci isolated from Italian cheeses. Int. J. Immunopathol. Pharmacol. 2015, 28, 341–350. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koo, H.; Allan, R.N.; Howlin, R.P.; Stoodley, P.; Hall-Stoodley, L. Targeting microbial biofilms: Current and prospective therapeutic strategies. Nat. Rev. Microbiol. 2017, 15, 740–755. [Google Scholar] [CrossRef] [PubMed]
- Bispo, P.J.; Haas, W.; Gilmore, M.S. Biofilms in infections of the eye. Pathogens 2015, 4, 111–136. [Google Scholar] [CrossRef] [PubMed]
- Biswas, N.R.; Gupta, S.K.; Das, G.K.; Kumar, N.; Mongre, P.K.; Haldar, D.; Beri, S. Evaluation of Ophthacare eye drops—A herbal formulation in the management of various ophthalmic disorders. Phytother. Res. PTR 2001, 15, 618–620. [Google Scholar] [CrossRef] [PubMed]
- Sharifi-Rad, J.; Mnayer, D.; Tabanelli, G.; Stojanovic-Radic, Z.Z.; Sharifi-Rad, M.; Yousaf, Z.; Vallone, L.; Setzer, W.N.; Iriti, M. Plants of the genus Allium as antibacterial agents: From tradition to pharmacy. Cell. Mol. Biol. 2016, 62, 57–68. [Google Scholar]
- Mohsenipour, Z.; Hassanshahian, M. The Effects of Allium sativum Extracts on Biofilm Formation and Activities of Six Pathogenic Bacteria. Jundishapur J. Microbial. 2015, 8, e18971. [Google Scholar] [CrossRef] [Green Version]
- Marini, E.; Magi, G.; Ferretti, G.; Bacchetti, T.; Giuliani, A.; Pugnaloni, A.; Rippo, M.R.; Facinelli, B. Attenuation of Listeria monocytogenes Virulence by Cannabis sativa L. Essential Oil. Front. Cell. Infect. Microbiol. 2018, 8, 293. [Google Scholar] [CrossRef] [Green Version]
- Hildebrandt, C.; Wagner, D.; Kohlmann, T.; Kramer, A. In-vitro analysis of the microbicidal activity of 6 contact lens care solutions. BMC Infect. Dis. 2012, 12, 241. [Google Scholar] [CrossRef] [Green Version]
- Szczotka-Flynn, L.B.; Imamura, Y.; Chandra, J.; Yu, C.; Mukherjee, P.K.; Pearlman, E.; Ghannoum, M.A. Increased resistance of contact lens-related bacterial biofilms to antimicrobial activity of soft contact lens care solutions. Cornea 2009, 28, 918–926. [Google Scholar] [CrossRef] [Green Version]
- Wilson, L.A.; Sawant, A.D.; Simmons, R.B.; Ahearn, D.G. Microbial contamination of contact lens storage cases and solutions. Am. J. Ophthalmol. 1990, 110, 193–198. [Google Scholar] [CrossRef]
- Kilvington, S.; Huang, L.; Kao, E.; Powell, C.H. Development of a new contact lens multipurpose solution: Comparative analysis of microbiological, biological and clinical performance. J. Optom. 2010, 13, 134–142. [Google Scholar] [CrossRef] [Green Version]
- McKenney, C.D.; Ajello, M. Comparative case contamination: Three disinfection systems. Int. Contact Lens Clin. 1991, 18, 14–20. [Google Scholar] [CrossRef]
- Fleiszig, S.M.; Efron, N. Microbial flora in eyes of current and former contact lens wearers. J. Clin. Microbial. 1992, 30, 1156–1161. [Google Scholar]
- Gray, T.B.; Cursons, R.T.; Sherwan, J.F.; Rose, P.R. Acanthamoeba, bacterial, and fungal contamination of contact lens storage cases. Br. J. Ophthalmol. 1995, 79, 601–605. [Google Scholar] [CrossRef] [Green Version]
- Awan, U.A.; Ali, S.; Shahnawaz, A.M.; Shafique, I.; Zafar, A.; Khan, M.A.R.; Ghous, T.; Saleem, A.; Andleeb, S. Biological activities of Allium sativum and Zingiber officinale extracts on clinically important bacterial pathogens, their phytochemical and FT-IR spectroscopic analysis. Pak. J. Pharm. Sci. 2017, 30, 729–745. [Google Scholar]
- Chakraborty, S.; Afaq, N.; Singh, N.; Majumdar, S. Antimicrobial activity of Cannabis sativa, Thuja orientalis and Psidium guajava leaf extracts against methicillin-resistant Staphylococcus aureus. J. Integr. Med. 2018, 16, 350–357. [Google Scholar] [CrossRef]
- Calvo, M.I.; Cavero, R.Y. Medicinal plants used for ophthalmological problems in Navarra (Spain). J. Ethnopharmacol. 2016, 190, 212–218. [Google Scholar] [CrossRef]
- Zaami, S.; Di Luca, A.; Di Luca, N.M.; Montanari Vergallo, G. Medical use of cannabis: Italian and European legislation. Eur. Rev. Med. Pharmacol. Sci. 2018, 22, 1161–1167. [Google Scholar]
- Novack, G.D. Cannabinoids for treatment of glaucoma. Curr. Opin. Ophthalmol. 2016, 27, 146–150. [Google Scholar] [CrossRef]
- Dosler, S.; Karaaslan, E.; Alev Gerceker, A. Antibacterial and anti-biofilm activities of melittin and colistin, alone and in combination with antibiotics against Gram-negative bacteria. J. Chemother. 2016, 28, 95–103. [Google Scholar] [CrossRef]
- Miquel, S.; Lagrafeuille, R.; Souweine, B.; Forestier, C. Anti-biofilm Activity as a Health Issue. Front. Microbial. 2016, 7, 592. [Google Scholar] [CrossRef] [PubMed]
- Garella, I. Dispositivo di Estrazione Solido-Liquido ad Alta Efficienza. Patent n0001396896, 20 December 2012. [Google Scholar]
- Stepanovic, S.; Vukovic, D.; Hola, V.; Di Bonaventura, G.; Djukic, S.; Cirkovic, I.; Ruzicka, F. Quantification of biofilm in microtiter plates: Overview of testing conditions and practical recommendations for assessment of biofilm production by staphylococci. APMIS Acta Pathol. Microbiol. Immunol. Scand. 2007, 115, 891–899. [Google Scholar] [CrossRef] [PubMed]
- Reiter, K.C.; Da Silva Paim, T.G.; De Oliveira, C.F.; D’Azevedo, P.A. High biofilm production by invasive multiresistant staphylococci. APMIS Acta Pathol. Microbial. Immunol. Scand. 2011, 119, 776–781. [Google Scholar] [CrossRef]
- Christensen, G.D.; Simpson, W.A.; Younger, J.J.; Baddour, L.M.; Barrett, F.F.; Melton, D.M.; Beachey, E.H. Adherence of coagulase-negative staphylococci to plastic tissue culture plates: A quantitative model for the adherence of staphylococci to medical devices. J. Clin. Microbial. 1985, 22, 996–1006. [Google Scholar]
- CLSI: Methods for diluition antimicrobial susceptibility tests for bacteria that grow aerobically. Document M7-A6 Performance Standards for Antimicrobial Susceptibility. Testing 2006, 26, 14–16.
- Galdiero, E.; Siciliano, A.; Gesuele, R.; Di Onofrio, V.; Falanga, A.; Maione, A.; Liguori, R.; Libralato, G.; Guida, M. Melittin Inhibition and Eradication Activity for Resistant Polymicrobial Biofilm Isolated from a Dairy Industry after Disinfection. Int. J. Microbial. 2019, 2019, 4012394. [Google Scholar] [CrossRef] [PubMed]
- Zago, C.E.; Silva, S.; Sanita, P.V.; Barbugli, P.A.; Dias, C.M.; Lordello, V.B.; Vergani, C.E. Dynamics of biofilm formation and the interaction between Candida albicans and methicillin-susceptible (MSSA) and -resistant Staphylococcus aureus (MRSA). PLoS ONE 2015, 10, e0123206. [Google Scholar] [CrossRef] [Green Version]
- Ramage, G.; Vande Walle, K.; Wickes, B.L.; Lopez-Ribot, J.L. Standardized method for in vitro antifungal susceptibility testing of Candida albicans biofilms. Antimicrob. Agents Chemother. 2001, 45, 2475–2479. [Google Scholar] [CrossRef] [Green Version]
- Bag, A.; Chattopadhyay, R.R. Synergistic antibiofilm efficacy of a gallotannin 1,2,6-tri-O-galloyl-beta-D-glucopyranose from Terminalia chebula fruit in combination with gentamicin and trimethoprim against multidrug resistant uropathogenic Escherichia coli biofilms. PLoS ONE 2017, 12, e0178712. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Tested Substances | P. aeruginosa ATCC 9027 | S.D. | P. aeruginosa Clinical Strain | S.D. |
|---|---|---|---|---|
| BGE | 4% | 0.13 | 4% | 0.38 |
| CBD | 2% | 0.31 | >2% | - |
| CL-care solutions | 50% | 0.16 | 50% | 0.23 |
| Microorganism. | Combinations | |||||
|---|---|---|---|---|---|---|
| Soft Contact Lenses Solution + BGE (CLS+B) | Soft Contact Lenses Solution + CBD (CLCS+C) | |||||
| FIC | FICI | FIC | FICI | |||
| P. aeruginosa ATCC 9027 | 0.250 (CLS) | 0.450 | Synergistic | 0.150 (CLCS) | 0.153 | Synergistic |
| 0.200 (B) | 0.030 (C) | |||||
| P. aeruginosa clinical strain | 0.250 (CLS) | 0.450 | Synergistic | 0.150 (CLCS) | 0.153 | Synergistic |
| 0.200 (B) | 0.030 (C) | |||||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Di Onofrio, V.; Gesuele, R.; Maione, A.; Liguori, G.; Liguori, R.; Guida, M.; Nigro, R.; Galdiero, E. Prevention of Pseudomonas aeruginosa Biofilm Formation on Soft Contact Lenses by Allium sativum Fermented Extract (BGE) and Cannabinol Oil Extract (CBD). Antibiotics 2019, 8, 258. https://doi.org/10.3390/antibiotics8040258
Di Onofrio V, Gesuele R, Maione A, Liguori G, Liguori R, Guida M, Nigro R, Galdiero E. Prevention of Pseudomonas aeruginosa Biofilm Formation on Soft Contact Lenses by Allium sativum Fermented Extract (BGE) and Cannabinol Oil Extract (CBD). Antibiotics. 2019; 8(4):258. https://doi.org/10.3390/antibiotics8040258
Chicago/Turabian StyleDi Onofrio, Valeria, Renato Gesuele, Angela Maione, Giorgio Liguori, Renato Liguori, Marco Guida, Roberto Nigro, and Emilia Galdiero. 2019. "Prevention of Pseudomonas aeruginosa Biofilm Formation on Soft Contact Lenses by Allium sativum Fermented Extract (BGE) and Cannabinol Oil Extract (CBD)" Antibiotics 8, no. 4: 258. https://doi.org/10.3390/antibiotics8040258