A Case of Hypokalemia Possibly Induced by Nafcillin

Abstract
:1. Introduction
2. Case Presentation
3. Discussion
4. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Zietse, R.; Zoutendijk, R.; Hoorn, E.J. Fluid, electrolytes and acid-base disorders associated with antibiotic therapy. Nat. Rev. Nephrol. 2009, 5, 193–202. [Google Scholar] [CrossRef] [PubMed]
- Hine, J.; Schwell, A.; Kairys, N. An unlikely cause of hypokalemia. J. Emerg. Med. 2017, 52, e187–e191. [Google Scholar] [CrossRef] [PubMed]
- Qua, D.A.; Tan, M.J. Hypokalemia associated with Nafcillin treatment. Infect. Dis. Clin. Pract. 2009, 17, 130–131. [Google Scholar] [CrossRef]
- Andreoli, S.P.; Kleiman, M.B.; Glick, M.R.; Bergstein, J.M. Nafcillin, pseudoproteinuria, and hypokalemic alkalosis. J. Pediatr. 1980, 97, 841–842. [Google Scholar] [CrossRef]
- Mount, D.B. Evaluation of the Adult Patient with Hypokalemia; Topic 2305, Version 22.0. Last Update 12 December 2017; UpToDate: Waltham, MA, USA; Available online: UpToDate.com (accessed on 25 April 2018).
- Mount, D.B. Causes of Hypokalemia in Adults; Topic 2341, Version 26.0. Last Update 18 December 2017; UpToDate: Waltham, MA, USA; Available online: UpToDate.com (accessed on 25 April 2018).
- Viehman, J.A.; Oleksuik, L.M.; Sheridan, K.R.; Byers, K.E.; He, P.; Falcione, B.A.; Shields, R.K. Adverse events lead to drug discontinuation more commonly among patients who receive Nafcillin than among those who receive Oxacillin. Antimicrob. Agents Chemother. 2016, 60, 3090–3095. [Google Scholar] [CrossRef] [PubMed]
- Rukma, P.; Mohsena, A.; Sunil, M. Nafcillin-associated hypokalemia. Am. J. Ther. 2018, 25, e755–e756. [Google Scholar] [CrossRef] [PubMed]
- Naranjo, C.A.; Busto, U.; Sellers, E.M.; Sandor, P.; Ruiz, I.; Roberts, E.A.; Janecek, E.; Domecq, C.; Greenblatt, D.J. A method for estimating the probability of adverse drug reactions. Clin. Pharmacol. Ther. 1981, 30, 239–245. [Google Scholar] [CrossRef] [PubMed]
- Anuhya, T.V.; Acharya, R.; Madhyastha, S.; Bhat, R.; Nayak, V. Meropenem induced hypokalemia. J. Clin. Diagn. Res. 2017, 11, OD05–OD06. [Google Scholar] [CrossRef] [PubMed]
- Mohr, J.A.; Clark, R.M.; Waack, T.C.; Whang, R. Nafcillin-associated hypokalemia. JAMA 1979, 242, 544. [Google Scholar] [CrossRef] [PubMed]
- Johnson, D.W.; Kay, T.D.; Hawley, C.M. Case Report: Severe Hypokalemia secondary to dicloxacillin. Intern. Med. J. 2002, 32, 357–358. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
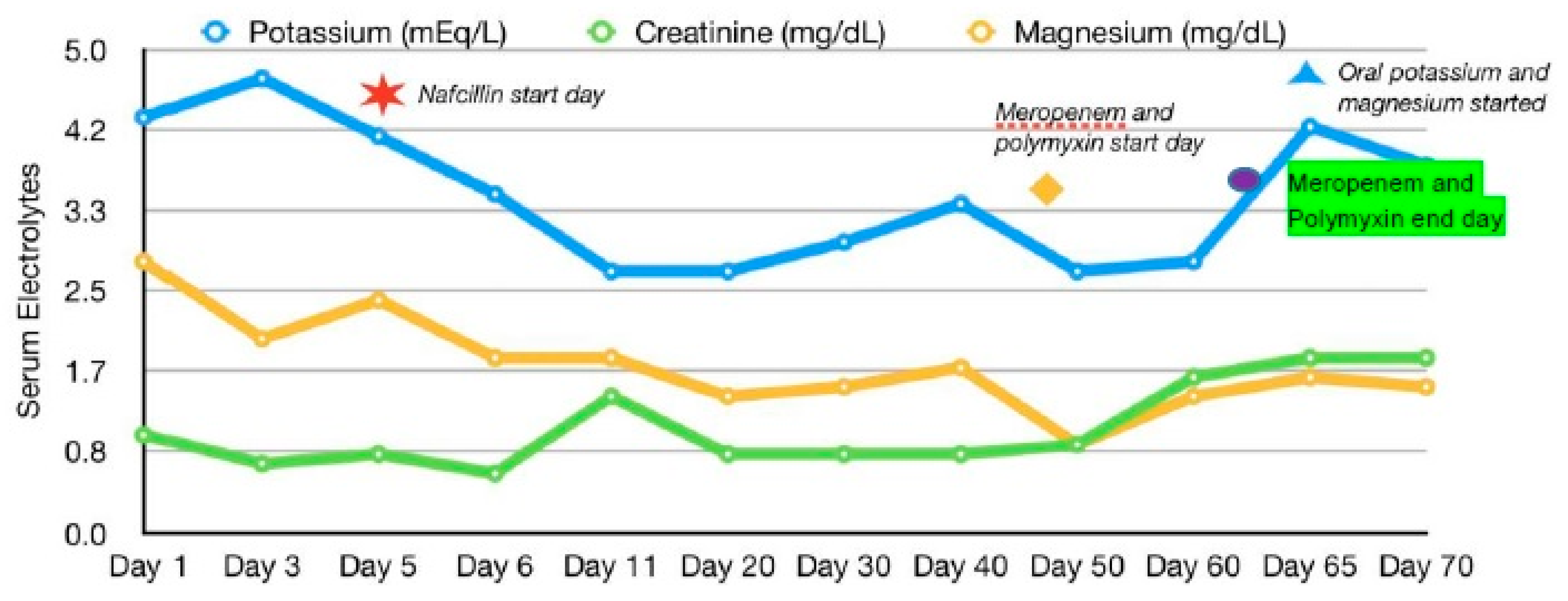
| Serum Electrolyte | Hospital Day | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| #1 | #3 | #5 % | #6 | #11 | #20 | #25 | #30 | #40 | #45 @ | #50 | #55 | #60 ∑ | #65 π | #70 | |
| Sodium (mEq/L) | 138 | 142 | 148 | 142 | 136 | 139 | 137 | 135 | 134 | 133 | 134 | 136 | 132 | 139 | 137 |
| Potassium (mEq/L) | 4.3 | 4.7 | 4.1 | 3.5 | 2.7 | 2.7 | 2.9 | 3.0 | 3.4 | 3.0 | 2.7 | 2.9 | 2.8 | 4.2 | 3.8 |
| Chloride (mEq/L) | 98 | 103 | 106 | 98 | 95 | 99 | 96 | 95 | 90 | 93 | 95 | 96 | 89 | 98 | 98 |
| Bicarbonate (mEq/L) | 22 | 26 | 27 | 29 | 27 | 28 | 29 | 26 | 27 | 24 | 26 | 26 | 28 | 25 | 29 |
| Blood Urea Nitrogen (mg/dL) | 40 | 30 | 32 | 19 | 20 | 6 | 6 | 5 | 5 | 7 | 9 | 5 | 9 | 9 | 11 |
| Creatinine (mg/dL) | 1.0 | 0.7 | 0.8 | 0.6 | 1.4 | 0.8 | 0.7 | 0.8 | 0.8 | 1.4 | 0.9 | 0.8 | 1.6 | 1.8 | 1.8 |
| Magnesium (mg/dL) | 2.8 | - | 2.4 | 1.8 | 1.8 | 1.4 | 1.7 | 1.5 | 1.7 | 1.6 | 0.9 | 1.3 | 1.4 | 1.6 | 1.5 |
| Phosphorous (mg/dL) | 4.2 | - | 3.6 | 2.9 | - | 2.4 | 3.0 | 3.1 | 3.1 | 2.2 | 2.1 | 2.4 | 2.3 | 2.2 | 2.6 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Casado, F.; Mudunuru, S.A.; Nasr, R. A Case of Hypokalemia Possibly Induced by Nafcillin. Antibiotics 2018, 7, 108. https://doi.org/10.3390/antibiotics7040108
Casado F, Mudunuru SA, Nasr R. A Case of Hypokalemia Possibly Induced by Nafcillin. Antibiotics. 2018; 7(4):108. https://doi.org/10.3390/antibiotics7040108
Chicago/Turabian StyleCasado, Fernando, Sitarama Arvind Mudunuru, and Rabih Nasr. 2018. "A Case of Hypokalemia Possibly Induced by Nafcillin" Antibiotics 7, no. 4: 108. https://doi.org/10.3390/antibiotics7040108