
Associations between Polycystic Ovary Syndrome (PCOS) and Antibiotic Use: Results from the UAEHFS

 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Material and Methods
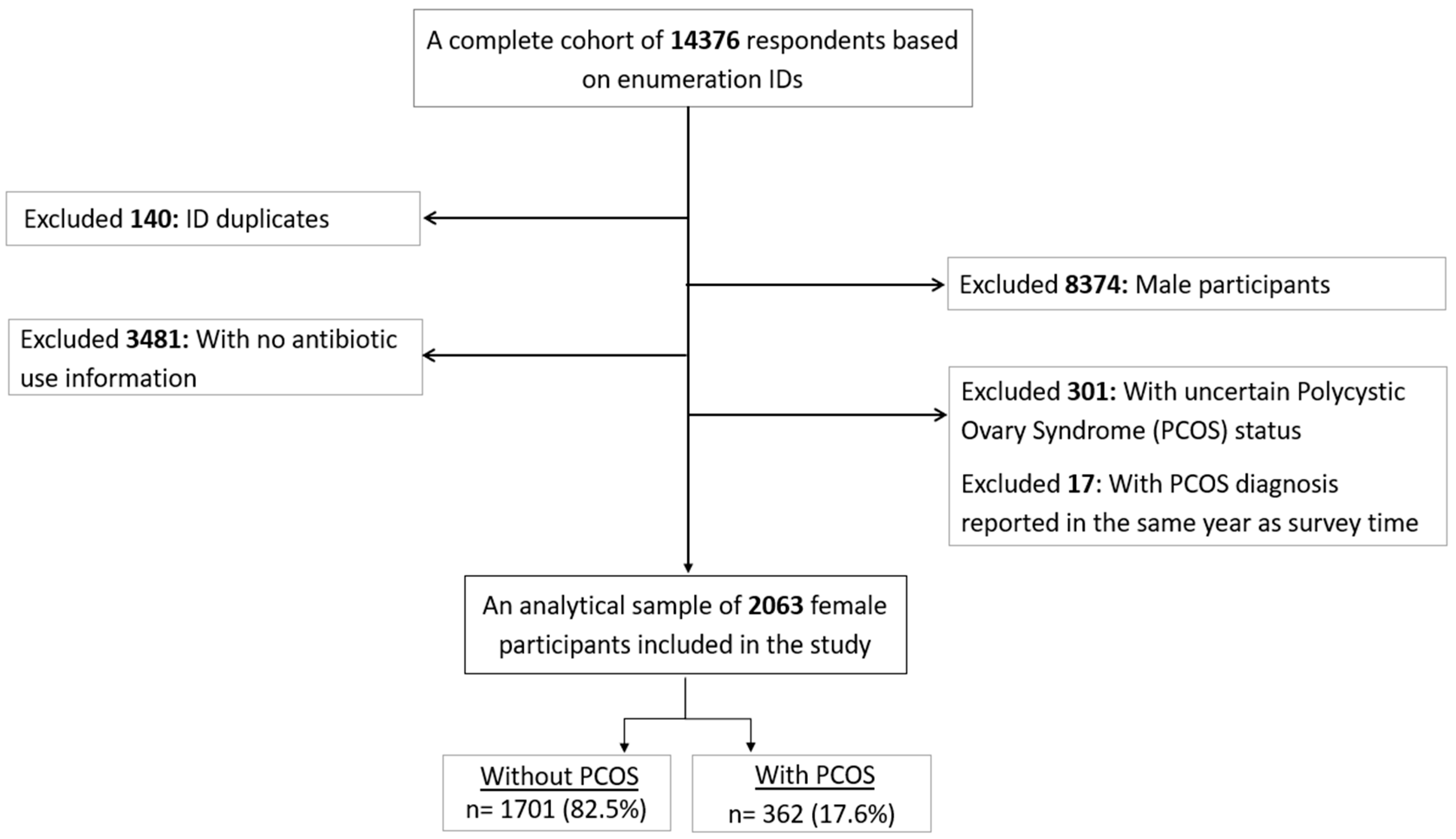
2.1. Study Design, Participants, and Setting
2.2. Measurements
2.2.1. Antibiotic Use as an Outcome Variable
2.2.2. PCOS-Related Status as Exposure Variables
2.2.3. Demographic Characteristics and Health Profiles as Third Variables
2.3. Statistical Analysis
2.4. Ethical Approval
3. Results
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bozdag, G.; Mumusoglu, S.; Zengin, D.; Karabulut, E.; Yildiz, B.O. The prevalence and phenotypic features of polycystic ovary syndrome: A systematic review and meta-analysis. Hum. Reprod. 2016, 31, 2841–2855. [Google Scholar] [CrossRef]
- Deswal, R.; Narwal, V.; Dang, A.; Pundir, C.S. The prevalence of polycystic ovary syndrome: A brief systematic review. J. Hum. Reprod. Sci. 2020, 13, 261–271. [Google Scholar] [CrossRef] [PubMed]
- Ibáñez, L.; Oberfield, S.E.; Witchel, S.; Auchus, R.J.; Chang, R.J.; Codner, E.; Dabadghao, P.; Darendeliler, F.; Elbarbary, N.S.; Gambineri, A.; et al. An international consortium update: Pathophysiology, diagnosis, and treatment of polycystic ovarian syndrome in adolescence. Horm. Res. Paediatr. 2017, 88, 371–395. [Google Scholar] [CrossRef]
- Mohan, A.; Haider, R.; Fakhor, H.; Hina, F.; Kumar, V.; Jawed, A.; Majumder, K.M.; Ayaz, A.M.; Lal, P.M.M.; Tejwaney, U.P.D.; et al. Vitamin D and polycystic ovary syndrome (PCOS): A review. Ann. Med. Surg. 2023, 85, 3506–3511. [Google Scholar] [CrossRef] [PubMed]
- Baptiste, C.G.; Battista, M.-C.; Trottier, A.; Baillargeon, J.-P. Insulin and hyperandrogenism in women with polycystic ovary syndrome. J. Steroid Biochem. Mol. Biol. 2010, 122, 42–52. [Google Scholar] [CrossRef]
- Yang, J.; Chen, C. Hormonal changes in PCOS. J. Endocrinol. 2024, 261, e230342. [Google Scholar] [CrossRef]
- Sahin, S.B.; Nalkiran, I.; Ayaz, T.; Guzel, A.I.; Eldes, T.; Calapoglu, T.; Nalkiran, H.S. Genetic variations in OLR1 gene associated with PCOS and atherosclerotic risk factors. J. Investig. Med. 2023, 71, 113–123. [Google Scholar] [CrossRef] [PubMed]
- Sanchez-Garrido, M.A.; Tena-Sempere, M. Metabolic dysfunction in polycystic ovary syndrome: Pathogenic role of androgen excess and potential therapeutic strategies. Mol. Metab. 2020, 35, 100937. [Google Scholar] [CrossRef]
- Singh, S.; Pal, N.; Shubham, S.; Sarma, D.K.; Verma, V.; Marotta, F.; Kumar, M. Polycystic ovary syndrome: Etiology, current management, and future therapeutics. J. Clin. Med. 2023, 12, 1454. [Google Scholar] [CrossRef]
- El-Hayek, S.; Bitar, L.; Hamdar, L.H.; Mirza, F.G.; Daoud, G. Poly Cystic Ovarian Syndrome: An Updated Overview. Front. Physiol. 2016, 7, 124. [Google Scholar] [CrossRef]
- Kujanpää, L.; Arffman, R.K.; Pesonen, P.; Korhonen, E.; Karjula, S.; Järvelin, M.R.; Franks, S.; Tapanainen, J.S.; Morin-Papunen, L.; Piltonen, T.T. Women with polycystic ovary syndrome are burdened with multimorbidity and medication use independent of body mass index at late fertile age: A population-based cohort study. Acta Obstet. Gynecol. Scand. 2022, 101, 728–736. [Google Scholar] [CrossRef] [PubMed]
- Juber, N.F.; Abdulle, A.; AlJunaibi, A.; AlNaeemi, A.; Ahmad, A.; Leinberger-Jabari, A.; Al Dhaheri, A.S.; AlZaabi, E.; Al-Maskari, F.; AlAnouti, F.; et al. Association between self-reported polycystic ovary syndrome with chronic diseases among emiratis: A cross-sectional analysis from the UAE healthy future study. Int. J. Womens Health 2023, 15, 289–298. [Google Scholar] [CrossRef] [PubMed]
- Qi, X.; Yun, C.; Sun, L.; Xia, J.; Wu, Q.; Wang, Y.; Wang, L.; Zhang, Y.; Liang, X.; Wang, L.; et al. Gut microbiota–bile acid–interleukin-22 axis orchestrates polycystic ovary syndrome. Nat. Med. 2019, 25, 1225–1233. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.-L.; Zhou, W.-W.; Wu, S.; Tang, W.-L.; Wang, Z.-W.; Zhou, Z.-Y.; Li, Z.-W.; Huang, Q.-F.; He, Y.; Zhou, H.-W.; et al. Intestinal flora is a key factor in insulin resistance and contributes to the development of polycystic ovary syndrome. Endocrinology 2021, 162, bqab118. [Google Scholar] [CrossRef] [PubMed]
- Tayler, E.; Gregory, R.; Bloom, G.; Salama, P.; Balkhy, H. Universal health coverage: An opportunity to address antimicrobial resistance? Lancet Glob. Health 2019, 7, e1480–e1481. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Ten Threats to Global Health in 2019; World Health Organization: Geneva, Switzerland, 2019; Available online: https://www.who.int/news-room/spotlight/ten-threats-to-global-health-in-2019 (accessed on 3 March 2024).
- Iskakova, N.; Khismetova, Z.; Suleymenova, D.; Kozhekenova, Z.; Khamidullina, Z.; Samarova, U.; Glushkova, N.; Semenova, Y. Factors Influencing Antibiotic Consumption in Adult Population of Kazakhstan. Antibiotics 2023, 12, 560. [Google Scholar] [CrossRef]
- Hussain, M.A.; Mohamed, A.O.; Abdelkarim, O.A.; Yousef, B.A.; Babikir, A.A.; Mirghani, M.M.; Mohamed, E.A.; Osman, W.; Mothana, R.A.; Elhag, R. Prevalence and Predictors of Antibiotic Self-Medication in Sudan: A Descriptive Cross-Sectional Study. Antibiotics 2023, 12, 612. [Google Scholar] [CrossRef]
- Abduelkarem, A.R.; Othman, A.M.; Abuelkhair, Z.M.; Ghazal, M.M.; Alzouobi, S.B.; El-Zowalaty, M.E. Prevalence of self-medication with antibiotics among residents in United Arab Emirates. Infect. Drug Resist. 2019, 12, 3445–3453. [Google Scholar] [CrossRef] [PubMed]
- Dik, V.K.; van Oijen, M.G.; Smeets, H.M.; Siersema, P.D. Frequent use of antibiotics is associated with colorectal cancer risk: Results of a nested case–control study. Dig. Dis. Sci. 2016, 61, 255–264. [Google Scholar] [CrossRef]
- Wirtz, H.S.; Buist, D.S.; Gralow, J.R.; Barlow, W.E.; Gray, S.; Chubak, J.; Yu, O.; Bowles, E.J.; Fujii, M.; Boudreau, D.M. Frequent Antibiotic Use and Second Breast Cancer EventsAntibiotics and Second Breast Cancer Events. Cancer Epidemiol. Biomarkers Prev. 2013, 22, 1588–1599. [Google Scholar] [CrossRef]
- Radlinski, L.; Conlon, B. Antibiotic efficacy in the complex infection environment. Curr. Opin. Microbiol. 2018, 42, 19–24. [Google Scholar] [CrossRef] [PubMed]
- Liu, M.; Gao, J.; Zhang, Y.; Li, P.; Wang, H.; Ren, X.; Li, C. Serum levels of TSP-1, NF-κB and TGF-β1 in polycystic ovarian syndrome (PCOS) patients in northern China suggest PCOS is associated with chronic inflammation. Clin. Endocrinol. 2015, 83, 913–922. [Google Scholar] [CrossRef] [PubMed]
- Alahmadi, A. The common pathological factors between polycystic ovary syndrome and COVID-19 infection: A review. Biosc Biotech. Res. Comm. 2020, 13, 1708–1716. [Google Scholar] [CrossRef]
- Subramanian, A.; Anand, A.; Adderley, N.J.; Okoth, K.; Toulis, K.A.; Gokhale, K.; Sainsbury, C.; O’reilly, M.W.; Arlt, W.; Nirantharakumar, K. Increased COVID-19 infections in women with polycystic ovary syndrome: A population-based study. Eur. J. Endocrinol. 2021, 184, 637–645. [Google Scholar] [CrossRef] [PubMed]
- Barber, T.M.; Hanson, P.; Weickert, M.O.; Franks, S. Obesity and Polycystic Ovary Syndrome: Implications for Pathogenesis and Novel Management Strategies. Clin. Med. Insights Reprod. Health 2019, 13, 1179558119874042. [Google Scholar] [CrossRef] [PubMed]
- Falagas, M.E.; Kompoti, M. Obesity and infection. Lancet Infect. Dis. 2006, 6, 438–446. [Google Scholar] [CrossRef] [PubMed]
- Marti, A.; Marcos, A.; Martinez, J.A. Obesity and immune function relationships. Obes. Rev. 2001, 2, 131–140. [Google Scholar] [CrossRef]
- Abdulle, A.; Alnaeemi, A.; Aljunaibi, A.; Al Ali, A.; Al-Saedi, K.; Al-Zaabi, E.; Oumeziane, N.; Al Bastaki, M.; Al-Houqani, M.; Al Maskari, F.; et al. The UAE healthy future study: A pilot for a prospective cohort study of 20,000 United Arab Emirates nationals. BMC Public. Health 2018, 18, 101. [Google Scholar] [CrossRef]
- Hoskin-Parr, L.; Teyhan, A.; Blocker, A.; Henderson, A. Antibiotic exposure in the first two years of life and development of asthma and other allergic diseases by 7.5 yr: A dose-dependent relationship. Pediatr. Allergy Immunol. 2013, 24, 762–771. [Google Scholar] [CrossRef]
- Ahmad, A.K.; Quinn, M.; Kao, C.-N.; Greenwood, E.; Cedars, M.I.; Huddleston, H.G. Improved diagnostic performance for the diagnosis of polycystic ovary syndrome using age-stratified criteria. Fertil. Steril. 2019, 111, 787–793. [Google Scholar] [CrossRef]
- Jena, S.K.; Mishra, L.; Naik, S.S.; Khan, S. Awareness and opinion about polycystic ovarian syndrome (PCOS) among young women: A developing country perspective. Int. J. Adolesc. Med. Health 2020, 33, 123–126. [Google Scholar] [CrossRef] [PubMed]
- Higuita-Gutiérrez, L.F.; Roncancio Villamil, G.E.; Jiménez Quiceno, J.N. Knowledge, attitude, and practice regarding antibiotic use and resistance among medical students in Colombia: A cross-sectional descriptive study. BMC Public. Health 2020, 20, 1861. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Obesity: Preventing and Managing the Global Epidemic. Report of a WHO Consultation. World Health Organ. Tech. Rep. Ser. 2000, 1–12, 1–253. Available online: https://pubmed.ncbi.nlm.nih.gov/11234459/ (accessed on 19 February 2024).
- Juber, N.F.; Abdulle, A.; Ahmad, A.; Leinberger-Jabari, A.; Dhaheri, A.S.A.; Al-Maskari, F.; AlAnouti, F.; Al-Houqani, M.; Ali, M.H.; El-Shahawy, O.; et al. Associations between Birth Weight and Adult Sleep Characteristics: A Cross-Sectional Analysis from the UAEHFS. J. Clin. Med. 2023, 12, 5618. [Google Scholar] [CrossRef]
- Glintborg, D.; Hass Rubin, K.; Nybo, M.; Abrahamsen, B.; Andersen, M. Morbidity and medicine prescriptions in a nationwide Danish population of patients diagnosed with polycystic ovary syndrome. Eur. J. Endocrinol. 2015, 172, 627–638. [Google Scholar] [CrossRef] [PubMed]
- Clark, A.W.; Durkin, M.J.; Olsen, M.A.; Keller, M.; Ma, Y.; O’Neil, C.A.; Butler, A.M. Rural–urban differences in antibiotic prescribing for uncomplicated urinary tract infection. Infect. Control. Hosp. Epidemiol. 2021, 42, 1437–1444. [Google Scholar] [CrossRef]
- Radha, P.; Devi, R.S.; Madhavi, J. Comparative Study of Prevalence of Polycystic Ovarian Syndrome in Rural and Urban Population. J. Adv. Med. Dent. Scie. Res. 2016, 4, 90. Available online: https://jamdsr.com/uploadfiles/19.PREVALENCEOFPOLYCYSTICOVARIANSYNDROME.20160310054301.pdf (accessed on 13 March 2024).
- Chow, S.K.Y.; Tao, X.; Zhu, X.; Niyomyart, A.; Choi, E. How socioeconomic, health seeking behaviours, and educational factors are affecting the knowledge and use of antibiotics in four different cities in Asia. Antibiotics 2021, 10, 1522. [Google Scholar] [CrossRef]
- Bell, G.A.; Sundaram, R.; Mumford, S.L.; Park, H.; Mills, J.; Bell, E.M.; Broadney, M.; Yeung, E.H. Maternal polycystic ovarian syndrome and early offspring development. Hum. Reprod. 2018, 33, 1307–1315. [Google Scholar] [CrossRef]
- Leong, K.S.; Derraik, J.G.; Hofman, P.L.; Cutfield, W.S. Antibiotics, gut microbiome and obesity. Clin. Endocrinol. 2018, 88, 185–200. [Google Scholar] [CrossRef]
- Steinberg, M.B.; Akincigil, A.; Kim, E.J.; Shallis, R.; Delnevo, C.D. Tobacco smoking as a risk factor for increased antibiotic prescription. Am. J. Prev. Med. 2016, 50, 692–698. [Google Scholar] [CrossRef]
- Zaitoun, B.; Al Kubaisi, A.; AlQattan, N.; Alassouli, Y.; Mohammad, A.; Alameeri, H.; Mohammed, G. Polycystic ovarian syndrome awareness among females in the UAE: A cross-sectional study. BMC Womens Health 2023, 23, 181. [Google Scholar] [CrossRef]
- Begum, G.S.; Shariff, A.; Ayman, G.; Mohammad, B.; Housam, R.; Khaled, N. Assessment of Risk Factors for Development of Polycystic Ovarian Syndrome. Int. J. Contemp. Med. Res. 2017, 4, 164–167. Available online: https://www.ijcmr.com/uploads/7/7/4/6/77464738/ijcmr_1209_feb_6.pdf (accessed on 21 February 2024).
- Pramodh, S. Exploration of Lifestyle Choices, Reproductive Health Knowledge, and Polycystic Ovary Syndrome (PCOS) Awareness Among Female Emirati University Students. Int. J. Womens Health 2020, 12, 927–938. [Google Scholar] [CrossRef] [PubMed]
- Dalibalta, S.; Abukhaled, Y.; Samara, F. Factors influencing the prevalence of polycystic ovary syndrome (PCOS) in the United Arab Emirates. Rev. Environ. Health 2022, 37, 311–319. [Google Scholar] [CrossRef]
- Ding, T.; Hardiman, P.J.; Petersen, I.; Wang, F.-F.; Qu, F.; Baio, G. The prevalence of polycystic ovary syndrome in reproductive-aged women of different ethnicity: A systematic review and meta-analysis. Oncotarget 2017, 8, 96351. [Google Scholar] [CrossRef] [PubMed]
- Mamdouh, H.; Hussain, H.Y.; Ibrahim, G.M.; Alawadi, F.; Hassanein, M.; Zarooni, A.A.; Al Suwaidi, H.; Hassan, A.; Alsheikh-Ali, A.; Alnakhi, W.K. Prevalence and associated risk factors of overweight and obesity among adult population in Dubai: A population-based cross-sectional survey in Dubai, the United Arab Emirates. BMJ Open 2023, 13, e062053. [Google Scholar] [CrossRef] [PubMed]
- Shallcross, L.; Beckley, N.; Rait, G.; Hayward, A.; Petersen, I. Antibiotic prescribing frequency amongst patients in primary care: A cohort study using electronic health records. J. Antimicrob. Chemother. 2017, 72, 1818–1824. [Google Scholar] [CrossRef] [PubMed]
- Crofts, T.S.; Gasparrini, A.J.; Dantas, G. Next-generation approaches to understand and combat the antibiotic resistome. Nat. Rev. Microbiol. 2017, 15, 422–434. [Google Scholar] [CrossRef]
- Kim, J.J.; Hwang, K.R.; Choi, Y.M.; Moon, S.Y.; Chae, S.J.; Park, C.W.; Kim, H.O.; Choi, D.S.; Kwon, H.C.; Kang, B.M.; et al. Complete phenotypic and metabolic profiles of a large consecutive cohort of untreated Korean women with polycystic ovary syndrome. Fertil. Steril. 2014, 101, 1424–1430. [Google Scholar] [CrossRef]
- Michelmore, K.F. Polycystic ovary syndrome in adolescence and early adulthood. Hum. Fertil. 2000, 3, 96–100. [Google Scholar] [CrossRef] [PubMed]
- Davison, S.L.; Bell, R.; Donath, S.; Montalto, J.; Davis, S.R. Androgen levels in adult females: Changes with age, menopause, and oophorectomy. J. Clin. Endocrinol. Metab. 2005, 90, 3847–3853. [Google Scholar] [CrossRef] [PubMed]
- Hsu, M.-I. Changes in the PCOS phenotype with age. Steroids 2013, 78, 761–766. [Google Scholar] [CrossRef] [PubMed]
- Liang, S.-J.; Hsu, C.-S.; Tzeng, C.-R.; Chen, C.-H.; Hsu, M.-I. Clinical and biochemical presentation of polycystic ovary syndrome in women between the ages of 20 and 40. Hum. Reprod. 2011, 26, 3443–3449. [Google Scholar] [CrossRef] [PubMed]
- Panidis, D.; Tziomalos, K.; Macut, D.; Delkos, D.; Betsas, G.; Misichronis, G.; Katsikis, I. Cross-sectional analysis of the effects of age on the hormonal, metabolic, and ultrasonographic features and the prevalence of the different phenotypes of polycystic ovary syndrome. Fertil. Steril. 2012, 97, 494–500. [Google Scholar] [CrossRef] [PubMed]
- Baldwin, H. Oral antibiotic treatment options for acne vulgaris. J. Clin. Aesthet. Dermatol. 2020, 13, 26. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7577330/ (accessed on 30 March 2024). [PubMed]
- Hardy, O.T.; Czech, M.P.; Corvera, S. What causes the insulin resistance underlying obesity? Curr. Opin. Endocrinol. Diabetes Obes. 2012, 19, 81–87. [Google Scholar] [CrossRef]
- Pai, M.P.; Bearden, D.T. Antimicrobial dosing considerations in obese adult patients: Insights from the Society of Infectious Diseases Pharmacists. Pharmacotherapy 2007, 27, 1081–1091. [Google Scholar] [CrossRef]
- Chang, S.; Dunaif, A. Diagnosis of Polycystic Ovary Syndrome: Which Criteria to Use and When? Endocrinol. Metab. Clin. North. Am. 2021, 50, 11–23. [Google Scholar] [CrossRef]
- Liyanage, G.S.; Inoue, R.; Fujitani, M.; Ishijima, T.; Shibutani, T.; Abe, K.; Kishida, T.; Okada, S. Effects of soy isoflavones, resistant starch and antibiotics on polycystic ovary syndrome (PCOS)-like features in letrozole-treated rats. Nutrients 2021, 13, 3759. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Demographic Characteristics and Health Profiles | Without PCOS (n = 1701, 82.5%) | With PCOS (n = 362, 17.6%) |
|---|---|---|
| Demographic characteristics | ||
| Age, median (IQR range), year | 22.0 (20–31) | 28.5 (23–36) |
| Urbanicity | ||
| Rural or non-urban areas | 240 (14.1) | 36 (9.9) |
| Urban areas | 1461 (85.9) | 326 (90.1) |
| Education | ||
| 12 years of schooling or below | 785 (46.2) | 121 (33.4) |
| Above 12 years of schooling | 916 (53.9) | 241 (66.6) |
| Health profiles | ||
| BMI, median (IQR range), kg/m2 | 23.9 (20.4–28.9) | 26.6 (23.0–30.9) |
| BMI categories, without missing category, reported | ||
| Normal BMI or below (<25 kg/m2) | 835 (49.1) | 125 (34.5) |
| Overweight (25 kg/m2 to <30 kg/m2) | 335 (19.7) | 85 (23.5) |
| Obese (30 kg/m2 or above) | 313 (18.4) | 99 (27.4) |
| Overall health status | ||
| Poor or fair | 426 (25.0) | 101 (27.9) |
| Excellent or good | 1275 (75.0) | 261 (72.1) |
| Smoking, without missing category reported | ||
| Never | 1410 (82.9) | 280 (77.4) |
| Ever | 148 (8.7) | 48 (13.3) |
| Regular medication use * | ||
| No | 702 (41.3) | 115 (31.8) |
| Yes | 999 (58.7) | 247 (68.2) |
| Antibiotic Use in the Past Year | ||||
|---|---|---|---|---|
| Crude Model | p-Value | Adjusted Model * | p-Value | |
| OR (95% CI) | OR (95% CI) | |||
| Main analysis | ||||
| Without PCOS (n = 1701) | (Reference) | (Reference) | ||
| With PCOS (n = 362) | 1.65 [1.34–2.02] | <0.001 | 1.55 [1.26–1.90] | <0.001 |
| PCOS-treatment-stratified models | ||||
| No | ||||
| Without PCOS (n = 1701) | (Reference) | (Reference) | ||
| Without PCOS treatment (n = 242) | 1.57 [1.23–1.99] | <0.001 | 1.46 [1.14–1.87] | 0.003 |
| Yes | ||||
| Without PCOS (n = 1701) | (Reference) | (Reference) | ||
| Being treated for PCOS (n = 120) | 1.81 [1.30–2.52] | <0.001 | 1.70 [1.22–2.38] | 0.002 |
| Age-of-PCOS-diagnosis-stratified models | ||||
| <25 years of age | ||||
| Without PCOS (n = 1701) | (Reference) | (Reference) | ||
| PCOS diagnosed at <25 years (n = 211) | 1.65 [1.28–2.13] | <0.001 | 1.60 [1.24–2.07] | <0.001 |
| >25 years of age | ||||
| Without PCOS (n = 1701) | (Reference) | (Reference) | ||
| PCOS diagnosed at ≥25 years (n = 108) | 1.66 [1.17–2.37] | 0.005 | 1.44 [0.99–2.10] | 0.055 |
| Antibiotic Use in the Past Year | ||||
|---|---|---|---|---|
| Crude Model | p-Value | Adjusted Model * | p-Value | |
| OR (95% CI) | OR (95% CI) | |||
| Main analysis | ||||
| Without PCOS (n = 338) | (Reference) | (Reference) | ||
| With PCOS (n = 132) | 1.78 [1.24–2.55] | 0.002 | 1.69 [1.17–2.46] | 0.006 |
| PCOS-treatment-stratified models | ||||
| No | ||||
| Without PCOS (n = 338) | (Reference) | (Reference) | ||
| Without PCOS treatment (n = 88) | 1.68 [1.10–2.57] | 0.017 | 1.59 [1.03–2.46] | 0.038 |
| Yes | ||||
| Without PCOS (n = 338) | (Reference) | (Reference) | ||
| Being treated for PCOS (n = 44) | 1.95 [1.12–3.39] | 0.018 | 1.87 [1.06–3.30] | 0.031 |
| Age-at-PCOS-diagnosis-stratified models | ||||
| <25 years of age | ||||
| Without PCOS (n = 338) | (Reference) | (Reference) | ||
| PCOS diagnosed at <25 years (n = 68) | 2.08 [1.32–3.28] | 0.002 | 2.09 [1.30–3.36] | 0.002 |
| >25 years of age | ||||
| Without PCOS (n = 338) | (Reference) | (Reference) | ||
| PCOS diagnosed at ≥25 year (n = 47) | 1.51 [0.86–2.64] | 0.154 | 1.31 [0.73–2.36] | 0.363 |
| Antibiotic Use in the Past Year | ||||
|---|---|---|---|---|
| Crude Model | p-Value | Adjusted Model * | p-Value | |
| OR (95% CI) | OR (95% CI) | |||
| Main analysis | ||||
| Without PCOS (n = 313) | (Reference) | (Reference) | ||
| With PCOS (n = 99) | 1.50 [0.99–2.27] | 0.054 | 1.42 [0.93–2.17] | 0.109 |
| PCOS-treatment-stratified models | ||||
| No | ||||
| Without PCOS (n = 313) | (Reference) | (Reference) | ||
| Without PCOS treatment (n = 71) | 1.61 [1.01–2.58] | 0.050 | 1.50 [0.92–2.44] | 0.103 |
| Yes | ||||
| Without PCOS (n = 313) | (Reference) | (Reference) | ||
| Being treated for PCOS (n = 28) | 1.28 [0.63–2.63] | 0.494 | 1.19 [0.57–2.46] | 0.641 |
| Age-at-PCOS-diagnosis-stratified models | ||||
| <25 years of age | ||||
| Without PCOS (n = 313) | (Reference) | (Reference) | ||
| PCOS diagnosed at <25 years (n =48) | 1.28 [0.74–2.21] | 0.375 | 1.24 [0.71–2.17] | 0.446 |
| >25 years of age | ||||
| Without PCOS (n = 313) | (Reference) | (Reference) | ||
| PCOS diagnosed at ≥25 years (n = 39) | 1.76 [0.94–3.29] | 0.076 | 1.70 [0.87–3.32] | 0.119 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Juber, N.F.; Abdulle, A.; Ahmad, A.; AlAnouti, F.; Loney, T.; Idaghdour, Y.; Valles, Y.; Ali, R. Associations between Polycystic Ovary Syndrome (PCOS) and Antibiotic Use: Results from the UAEHFS. Antibiotics 2024, 13, 397. https://doi.org/10.3390/antibiotics13050397
Juber NF, Abdulle A, Ahmad A, AlAnouti F, Loney T, Idaghdour Y, Valles Y, Ali R. Associations between Polycystic Ovary Syndrome (PCOS) and Antibiotic Use: Results from the UAEHFS. Antibiotics. 2024; 13(5):397. https://doi.org/10.3390/antibiotics13050397
Chicago/Turabian StyleJuber, Nirmin F., Abdishakur Abdulle, Amar Ahmad, Fatme AlAnouti, Tom Loney, Youssef Idaghdour, Yvonne Valles, and Raghib Ali. 2024. "Associations between Polycystic Ovary Syndrome (PCOS) and Antibiotic Use: Results from the UAEHFS" Antibiotics 13, no. 5: 397. https://doi.org/10.3390/antibiotics13050397