


A Single Dose of Piperacillin Plus Tazobactam Gel as an Adjunct to Professional Mechanical Plaque Removal (PMPR) in Patients with Peri-Implant Mucositis: A 6-Month Double-Blind Randomized Clinical Trial
 , , , and
, , , and
Abstract
:1. Introduction
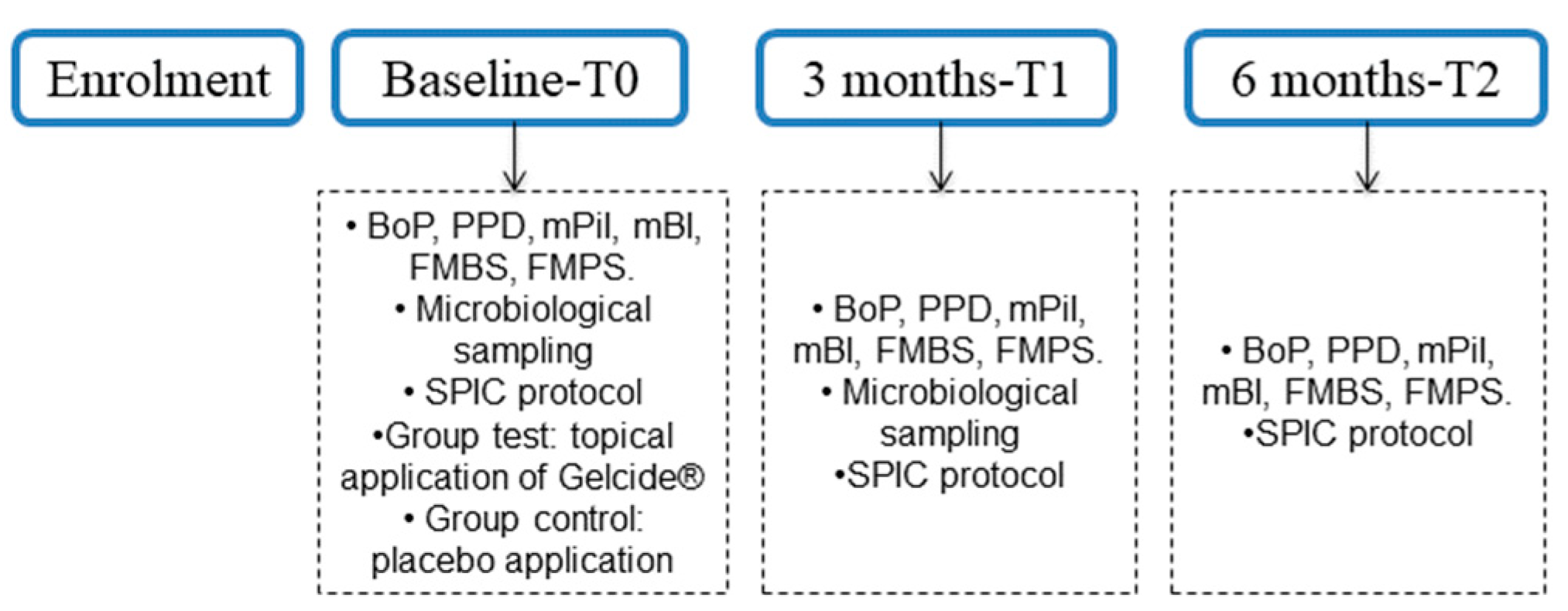
2. Materials and Methods
2.1. Study Design and Study Group Allocation
2.2. Study Sample
2.3. Inclusion Criteria
- (1)
- Age ≥ 18 years;
- (2)
- Absence of relevant systemic disease;
- (3)
- Partially edentulous patients with healthy or treated periodontal conditions enrolled in a regular supportive care program;
- (4)
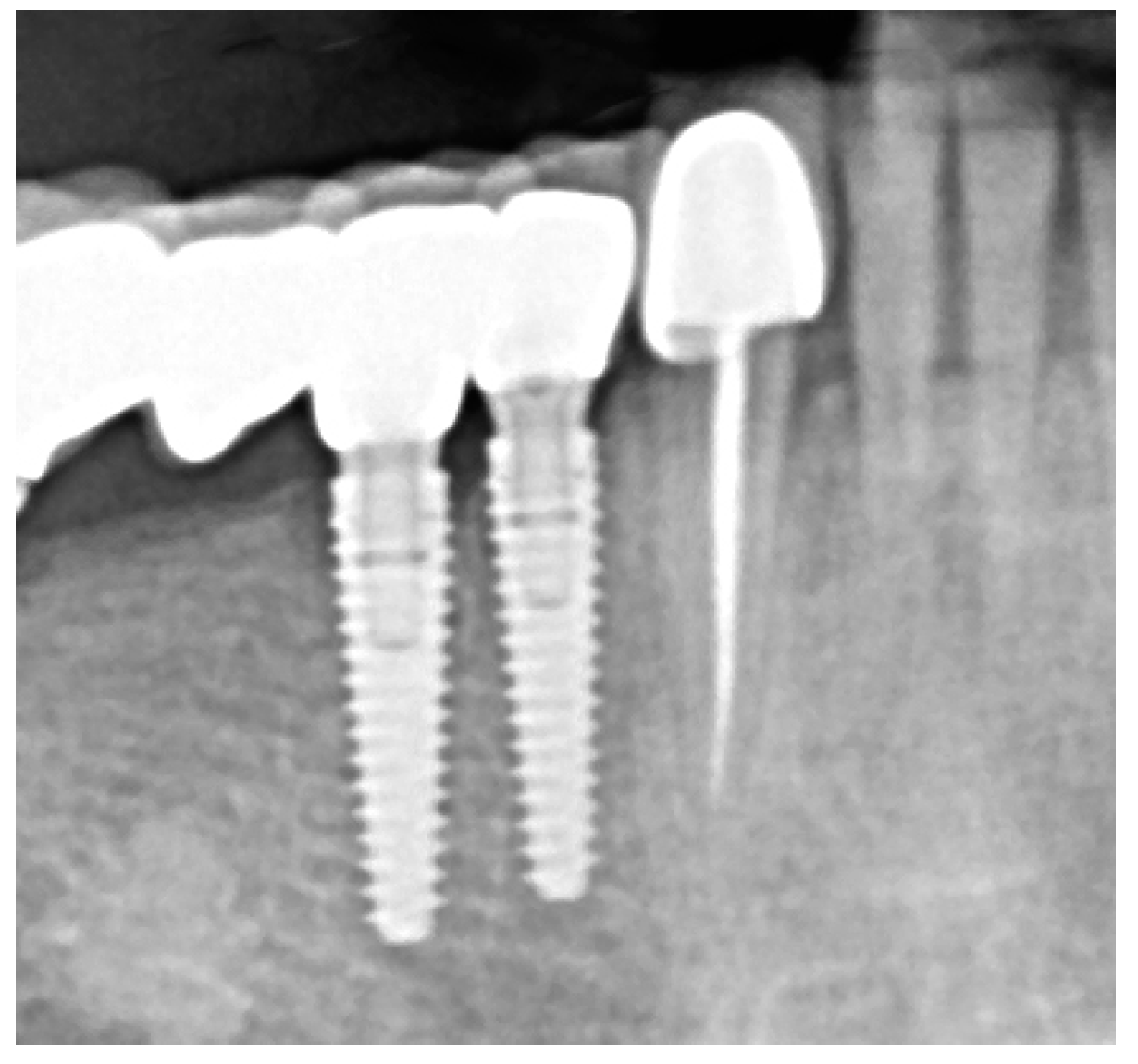
- Peri-implant mucositis defined as >1 implant site with presence of BoP and absence of radiographic bone loss compared with a previous radiograph [2];
- (5)
- Implant in function for ≥1 year;
- (6)
- Full-Mouth Plaque Score (FMPS) ≤ 25;
- (7)
- Full-Mouth Bleeding Score (FMBS) ≤ 25.
2.4. Exclusion Criteria
- (1)
- Uncontrolled medical conditions;
- (2)
- Pregnant or lactating females;
- (3)
- Tobacco smoking ≥ 10 cigarettes/day;
- (4)
- Untreated periodontal conditions;
- (5)
- Removable implant—retained prosthesis;
- (6)
- Use of antibiotics in the past 3 months;
- (7)
- Subjects who received treatment for at least 2 weeks with any medication recognized to impact soft tissue conditions within 1 month of the baseline test;
- (8)
- Other chronic systemic medications that could interfere with the study’s outcomes;
- (9)
- Refusal to sign written informed consent.
2.5. Hypothesis
2.6. Clinical Examination
- (1)
- Implant probing pocket depth (PPD) was measured from the mucosal margin to the bottom of the probable pocket and evaluated at six sites per implant (i.e., disto-buccal, mid-buccal, mesio-buccal, mesio-lingual/palatal, mid-lingual/palatal, disto-lingual/palatal);
- (2)
- (3)
- Suppuration on probing (SoP) was assessed according to either presence or absence of suppuration after probing;
- (4)
- Modified Plaque Index (mPlI) was recorded as 0, 1, 2, 3 (Mombelli et al., 1987) [46];
- (5)
- Modified Bleeding Index (mBI) was recorded as 0, 1, 2, 3 (Mombelli et al., 1987) [46].
2.7. Microbiological Examination
2.8. Treatment Procedures
- Medical history update, risk assessment (interview);
- OH behavior improvements;
- Reinforcing of risk factor control (e.g., smoking, glycemic control);
- PMPR, individualized OH recommendations, for entire dentition/implants;
- Recall interval of 3 months [6].
2.9. Evaluation of Treatment Effect
2.10. Rescue Protocol
2.11. Statistical Analysis
3. Results
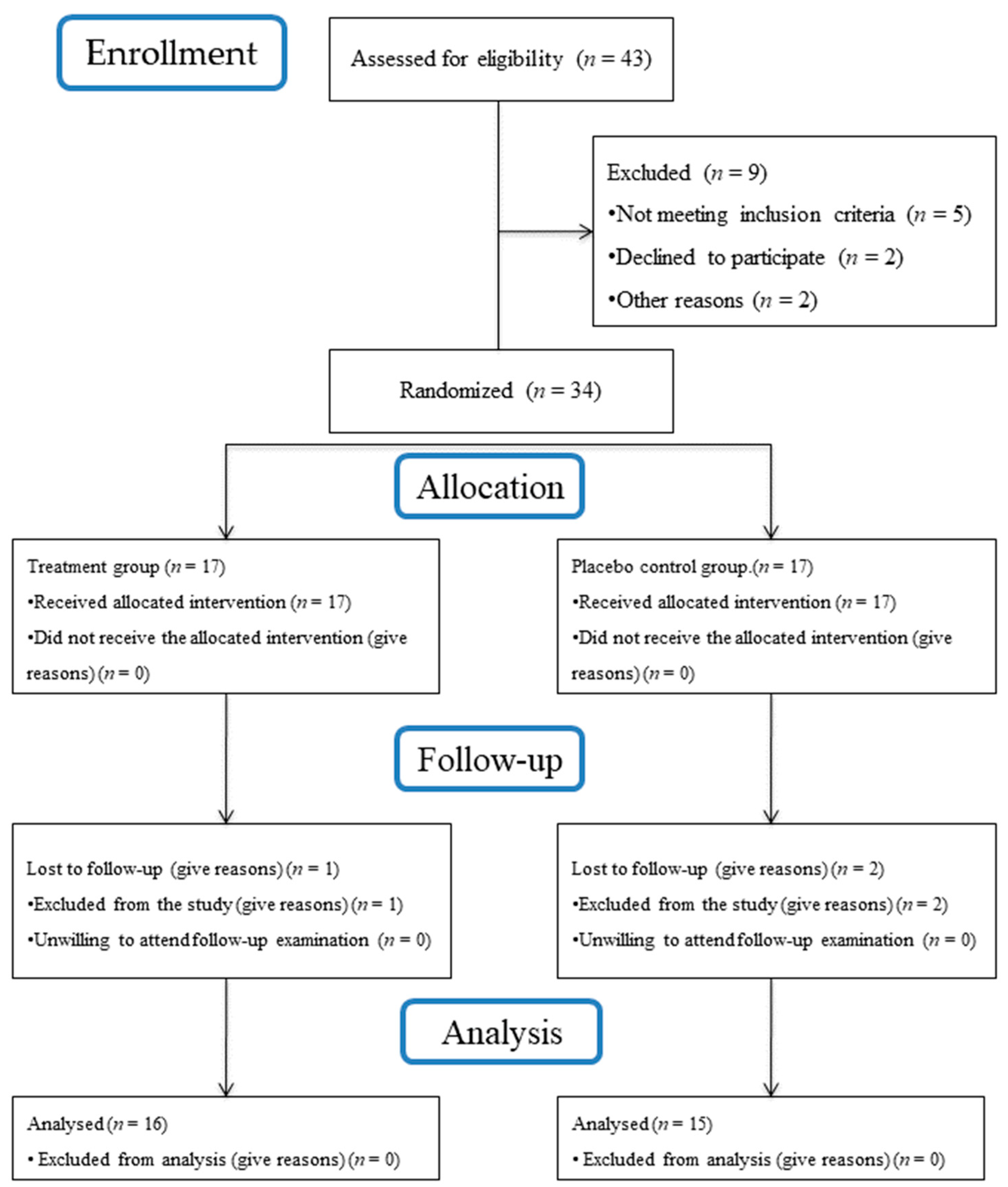
3.1. Subject Accountability
3.2. Study Participants Characteristics
3.3. Clinical Outcomes
3.3.1. Bleeding on Probing
3.3.2. Pocket Probing Depth
3.3.3. Plaque Index
3.3.4. Full-Mouth Plaque Score and Full-Mouth Bleeding Score
3.3.5. Treatment Success (BoP ≤ 1 Site) at 6 Months following Therapy
3.4. Microbiological Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Heitz-Mayfield, L.J.A.; Salvi, G.E. Peri-implant mucositis. J. Clin. Periodontol. 2018, 45 (Suppl. S20), S237–S245. [Google Scholar] [CrossRef] [PubMed]
- Renvert, S.; Persson, G.R.; Pirih, F.Q.; Camargo, P.M. Peri-implant health, peri-implant mucositis, and peri-implantitis: Case definitions and diagnostic considerations. J. Clin. Periodontol. 2018, 45 (Suppl. S20), S278–S285. [Google Scholar] [CrossRef]
- Renvert, S.; Lindahl, C.; Persson, G.R. Occurrence of cases with peri-implant mucositis or peri-implantitis in a 21–26 years follow-up study. J. Clin. Periodontol. 2018, 45, 233–240. [Google Scholar] [CrossRef]
- Sanz, M.; Chapple, I.L.; Working Group 4 of the VIII European Workshop on Periodontology. Clinical research on peri-implant diseases: Consensus report of Working Group 4. J. Clin. Periodontol. 2012, 39, 202–206. [Google Scholar] [CrossRef] [PubMed]
- Máximo, M.B.; de Mendonça, A.C.; Renata Santos, V.; Figueiredo, L.C.; Feres, M.; Duarte, P.M. Short-term clinical and microbiological evaluations of peri-implant diseases before and after mechanical anti-infective therapies. Clin. Oral Implants. Res. 2009, 20, 99–108. [Google Scholar] [CrossRef] [PubMed]
- Herrera, D.; Berglundh, T.; Schwarz, F.; Chapple, I.; Jepsen, S.; Sculean, A.; Kebschull, M.; Papapanou, P.N.; Tonetti, M.S.; Sanz, M.; et al. Prevention and treatment of peri-implant diseases-The EFP S3 level clinical practice guideline. J. Clin. Periodontol. 2023, 50, 4–76. [Google Scholar] [CrossRef] [PubMed]
- Salvi, G.E.; Aglietta, M.; Eick, S.; Sculean, A.; Lang, N.P.; Ramseier, C.A. Reversibility of experimental peri-implant mucositis compared with experimental gingivitis in humans. Clin. Oral Implants Res. 2012, 23, 182–190. [Google Scholar] [CrossRef] [PubMed]
- Meyer, S.; Giannopoulou, C.; Courvoisier, D.; Schimmel, M.; Müller, F.; Mombelli, A. Experimental mucositis and experimental gingivitis in persons aged 70 or over. Clinical and biological responses. Clin. Oral Implants Res. 2017, 28, 1005–1012. [Google Scholar] [CrossRef]
- Tonetti, M.S.; Sanz, M.; Avila-Ortiz, G.; Berglundh, T.; Cairo, F.; Derks, J.; Figuero, E.; Graziani, F.; Guerra, F.; Heitz-Mayfield, L.; et al. Relevant domains, core outcome sets and measurements for implant dentistry clinical trials: The Implant Dentistry Core Outcome Set and Measurement (ID-COSM) international consensus report. J. Clin. Periodontol. 2023, 50 (Suppl. S25), 5–21. [Google Scholar] [CrossRef]
- Renvert, S.; Polyzois, I. Risk indicators for peri-implant mucositis: A systematic literature review. J. Clin. Periodontol. 2015, 42 (Suppl. S16), S172–S186. [Google Scholar] [CrossRef]
- Schwarz, F.; Mihatovic, I.; Golubovic, V.; Eick, S.; Iglhaut, T.; Becker, J. Experimental peri-implant mucositis at different implant surfaces. J. Clin. Periodontol. 2014, 41, 513–520. [Google Scholar] [CrossRef] [PubMed]
- Costa, F.O.; Takenaka-Martinez, S.; Cota, L.O.; Ferreira, S.D.; Silva, G.L.; Costa, J.E. Peri-implant disease in subjects with and without preventive maintenance: A 5-year follow-up. J. Clin. Periodontol. 2012, 39, 173–181. [Google Scholar] [CrossRef] [PubMed]
- Derks, J.; Tomasi, C. Peri-implant health and disease. A systematic review of current epidemiology. J. Clin. Periodontol. 2015, 42 (Suppl. S16), S158–S171. [Google Scholar] [CrossRef]
- Lang, N.P.; Mult, H.C.; Tonetti, M.S. Peri-implantitis: Etiology pathogenesis prevention therapy. In Dental Implant Complications; Froum, S.J., Ed.; John Wiley & Sons: Hoboken, NJ, USA, 2015. [Google Scholar] [CrossRef]
- Jepsen, S.; Berglundh, T.; Genco, R.; Aass, A.M.; Demirel, K.; Derks, J.; Figuero, E.; Giovannoli, J.L.; Goldstein, M.; Lambert, F.; et al. Primary prevention of peri-implantitis: Managing peri-implant mucositis. J. Clin. Periodontol. 2015, 42 (Suppl. S16), S152–S157. [Google Scholar] [CrossRef] [PubMed]
- Mombelli, A.; Lang, N.P. The diagnosis and treatment of peri-implantitis. Periodontol. 2000 1998, 17, 63–76. [Google Scholar] [CrossRef]
- Heitz-Mayfield, L.J.; Salvi, G.E.; Botticelli, D.; Mombelli, A.; Faddy, M.; Lang, N.P.; Implant Complication Research Group. Anti-infective treatment of peri-implant mucositis: A randomised controlled clinical trial. Clin. Oral Implants Res. 2011, 22, 237–241. [Google Scholar] [CrossRef]
- Schwarz, F.; Becker, K.; Sager, M. Efficacy of professionally administered plaque removal with or without adjunctive measures for the treatment of peri-implant mucositis. A systematic review and meta-analysis. J. Clin. Periodontol. 2015, 42 (Suppl. S16), S202–S213. [Google Scholar] [CrossRef]
- Lindhe, J.; Meyle, J.; Group D of European Workshop on Periodontology. Peri-implant diseases: Consensus Report of the Sixth European Workshop on Periodontology. J. Clin. Periodontol. 2008, 35 (Suppl. S8), 282–285. [Google Scholar] [CrossRef]
- Klinge, B.; Meyle, J.; Working Group 2. Peri-implant tissue destruction. The Third EAO Consensus Conference 2012. Clin. Oral Implants Res. 2012, 23 (Suppl. S6), 108–110. [Google Scholar] [CrossRef]
- Heitz-Mayfield, L.J.; Mombelli, A. The therapy of peri-implantitis: A systematic review. Int. J. Oral Maxillofac. Implants 2014, 29, 325–345. [Google Scholar] [CrossRef]
- Renvert, S.; Roos-Jansåker, A.M.; Claffey, N. Non-surgical treatment of peri-implant mucositis and peri-implantitis: A literature review. J. Clin. Periodontol. 2008, 35 (Suppl. S8), 305–315. [Google Scholar] [CrossRef] [PubMed]
- Ciancio, S.G.; Lauciello, F.; Shibly, O.; Vitello, M.; Mather, M. The effect of an antiseptic mouthrinse on implant maintenance: Plaque and peri-implant gingival tissues. J. Periodontol. 1995, 66, 962–965. [Google Scholar] [CrossRef] [PubMed]
- Ramberg, P.; Lindhe, J.; Botticelli, D.; Botticelli, A. The effect of a triclosan dentifrice on mucositis in subjects with dental implants: A six-month clinical study. J. Clin. Dent. 2009, 20, 103–107. [Google Scholar] [PubMed]
- Thöne-Mühling, M.; Swierkot, K.; Nonnenmacher, C.; Mutters, R.; Flores-de-Jacoby, L.; Mengel, R. Comparison of two full-mouth approaches in the treatment of peri-implant mucositis: A pilot study. Clin. Oral Implants Res. 2010, 21, 504–512. [Google Scholar] [CrossRef] [PubMed]
- Schenk, G.; Flemmig, T.F.; Betz, T.; Reuther, J.; Klaiber, B. Controlled local delivery of tetracycline HCl in the treatment of periimplant mucosal hyperplasia and mucositis. A controlled case series. Clin. Oral Implants Res. 1997, 8, 427–433. [Google Scholar] [CrossRef] [PubMed]
- Hallström, H.; Persson, G.R.; Lindgren, S.; Olofsson, M.; Renvert, S. Systemic antibiotics and debridement of peri-implant mucositis. A randomized clinical trial. J. Clin. Periodontol. 2012, 39, 574–581. [Google Scholar] [CrossRef]
- Iorio-Siciliano, V.; Blasi, A.; Stratul, S.I.; Ramaglia, L.; Sculean, A.; Salvi, G.E.; Rusu, D. Anti-infective therapy of peri-implant mucositis with adjunctive delivery of a sodium hypochlorite gel: A 6-month randomized triple-blind controlled clinical trial. Clin. Oral Investig. 2020, 24, 1971–1979. [Google Scholar] [CrossRef]
- Renvert, S.; Lessem, J.; Dahlén, G.; Lindahl, C.; Svensson, M. Topical minocycline microspheres versus topical chlorhexidine gel as an adjunct to mechanical debridement of incipient peri-implant infections: A randomized clinical trial. J. Clin. Periodontol. 2006, 33, 362–369. [Google Scholar] [CrossRef]
- Takasaki, A.A.; Aoki, A.; Mizutani, K.; Schwarz, F.; Sculean, A.; Wang, C.Y.; Koshy, G.; Romanos, G.; Ishikawa, I.; Izumi, Y. Application of antimicrobial photodynamic therapy in periodontal and peri-implant diseases. Periodontol. 2000 2009, 51, 109–140. [Google Scholar] [CrossRef]
- Porras, R.; Anderson, G.B.; Caffesse, R.; Narendran, S.; Trejo, P.M. Clinical response to 2 different therapeutic regimens to treat peri-implant mucositis. J. Periodontol. 2002, 73, 1118–1125. [Google Scholar] [CrossRef]
- Pulcini, A.; Bollaín, J.; Sanz-Sánchez, I.; Figuero, E.; Alonso, B.; Sanz, M.; Herrera, D. Clinical effects of the adjunctive use of a 0.03% chlorhexidine and 0.05% cetylpyridinium chloride mouth rinse in the management of peri-implant diseases: A randomized clinical trial. J. Clin. Periodontol. 2019, 46, 342–353. [Google Scholar] [CrossRef] [PubMed]
- Mombelli, A.; Feloutzis, A.; Brägger, U.; Lang, N.P. Treatment of peri-implantitis by local delivery of tetracycline. Clinical, microbiological and radiological results. Clin. Oral Implants Res. 2001, 12, 287–294. [Google Scholar] [CrossRef] [PubMed]
- Büchter, A.; Meyer, U.; Kruse-Lösler, B.; Joos, U.; Kleinheinz, J. Sustained release of doxycycline for the treatment of peri-implantitis: Randomised controlled trial. Br. J. Oral Maxillofac. Surg. 2004, 42, 439–444. [Google Scholar] [CrossRef] [PubMed]
- Renvert, S.; Lessem, J.; Lindahl, C.; Svensson, M. Treatment of incipient peri-implant infections using topical minocycline microspheres versus topical chlorhexidine gel as an adjunct to mechanical debridement. J. Int. Acad. Periodontol. 2004, 6 (Suppl. S4), 154–159. [Google Scholar] [PubMed]
- Munch, M.W.; Granholm, A.; Jonsson, A.B.; Sjövall, F.; Helleberg, M.; Hertz, F.B.; Andersen, J.S.; Steensen, M.; Achiam, M.P.; Perner, A.; et al. Piperacillin/tazobactam versus carbapenems in patients with severe bacterial infections: A systematic review with meta-analysis. Acta Anaesthesiol. Scand. 2023, 67, 853–868. [Google Scholar] [CrossRef]
- Zhang, W.; Yan, C.Y.; Li, S.R.; Fan, T.T.; Cao, S.S.; Cui, B.; Li, M.Y.; Fan, B.Y.; Ji, B.; Wang, L.; et al. Efficacy and safety of piperacillin-tazobactam compared with meropenem in treating complicated urinary tract infections including acute pyelonephritis due to extended-spectrum β-lactamase-producing Enterobacteriaceae. Front. Cell. Infect. Microbiol. 2023, 13, 1093842. [Google Scholar] [CrossRef]
- Pacifici, G.M. Clinical Pharmacology of Piperacillin/Tazobactam. J. Clin. Biomed. Investig. 2023, 3, 11–19. [Google Scholar] [CrossRef]
- Bush, K.; Bradford, P.A. β-Lactams and β-Lactamase Inhibitors: An Overview. Cold Spring Harb. Perspect. Med. 2016, 6, a025247. [Google Scholar] [CrossRef]
- Weise, H.; Naros, A.; Weise, C.; Reinert, S.; Hoefert, S. Severe odontogenic infections with septic progress—A constant and increasing challenge: A retrospective analysis. BMC Oral Health 2019, 19, 173. [Google Scholar] [CrossRef]
- Ilyes, I.; Rusu, D.; Rădulescu, V.; Vela, O.; Boariu, M.I.; Roman, A.; Surlin, P.; Kardaras, G.; Boia, S.; Chinnici, S.; et al. A Placebo-Controlled Trial to Evaluate Two Locally Delivered Antibiotic Gels (Piperacillin Plus Tazobactam vs. Doxycycline) in Stage III-IV Periodontitis Patients. Medicina 2023, 59, 303. [Google Scholar] [CrossRef]
- Hurtado-Celotti, D.; Martínez-Rodríguez, N.; Ruiz-Sáenz, P.L.; Barona-Dorado, C.; Santos-Marino, J.; Martínez-González, J.M. Piperacillin-Tazobactam as an Adjuvant in the Mechanical Treatment of Patients with Periodontitis: A Randomized Clinical Study. Antibiotics 2022, 11, 1689. [Google Scholar] [CrossRef] [PubMed]
- Sender-Janeczek, A.; Zborowski, J.; Szulc, M.; Konopka, T. New Local Drug Delivery with Antibiotic in the Nonsurgical Treatment of Periodontitis—Pilot Study. Appl. Sci. 2019, 9, 5077. [Google Scholar] [CrossRef]
- Lauenstein, M.; Kaufmann, M.; Persson, G.R. Clinical and microbiological results following nonsurgical periodontal therapy with or without local administration of piperacillin/tazobactam. Clin. Oral Investig. 2013, 17, 1645–1660. [Google Scholar] [CrossRef]
- González Regueiro, I.; Martínez Rodriguez, N.; Barona Dorado, C.; Sanz-Sánchez, I.; Montero, E.; Ata-Ali, J.; Duarte, F.; Martínez-González, J.M. Surgical approach combining implantoplasty and reconstructive therapy with locally delivered antibiotic in the treatment of peri-implantitis: A prospective clinical case series. Clin. Implant Dent. Relat. Res. 2021, 23, 864–873. [Google Scholar] [CrossRef]
- Mombelli, A.; van Oosten, M.A.; Schurch, E., Jr.; Land, N.P. The microbiota associated with successful or failing osseointegrated titanium implants. Oral. Microbiol. Immunol. 1987, 2, 145–151. [Google Scholar] [CrossRef] [PubMed]
- O’Leary, T.J.; Drake, R.B.; Naylor, J.E. The plaque control record. J. Periodontol. 1972, 43, 38. [Google Scholar] [CrossRef]
- Claffey, N.; Nylund, K.; Kiger, R.; Garrett, S.; Egelberg, J. Diagnostic predictability of scores of plaque, bleeding, suppuration and probing depth for probing attachment loss. 3 1/2 years of observation following initial periodontal therapy. J. Clin. Periodontol. 1990, 17, 108–114. [Google Scholar] [CrossRef]
- Jenzsch, A.; Eick, S.; Rassoul, F.; Purschwitz, R.; Jentsch, H. Nutritional intervention in patients with periodontal disease: Clinical, immunological and microbiological variables during 12 months. Br. J. Nutr. 2009, 101, 879–885. [Google Scholar] [CrossRef] [PubMed]
- Rusu, D.; Stratul, S.I.; Sarbu, C.; Roman, A.; Anghel, A.; Didilescu, A.; Jentsch, H. Evaluation of a hydrophobic gel adhering to the gingiva in comparison with a standard water-soluble 1% chlorhexidine gel after scaling and root planing in patients with moderate chronic periodontitis. A randomized clinical trial. Int. J. Dent. Hyg. 2017, 15, 53–64. [Google Scholar] [CrossRef]
- Stoller, N.H.; Johnson, L.R.; Trapnell, S.; Harrold, C.Q.; Garrett, S. The pharmacokinetic profile of a biodegradable controlled-release delivery system containing doxycycline compared to systemically delivered doxycycline in gingival crevicular fluid, saliva, and serum. J. Periodontol. 1998, 69, 1085–1091. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2021; Available online: https://www.r-project.org (accessed on 28 November 2023).
- Renvert, S.; Samuelsson, E.; Lindahl, C.; Persson, G.R. Mechanical non-surgical treatment of peri-implantitis: A double-blind randomized longitudinal clinical study. I: Clinical results. J. Clin. Periodontol. 2009, 36, 604–609. [Google Scholar] [CrossRef] [PubMed]
- Renvert, S.; Lessem, J.; Dahlén, G.; Renvert, H.; Lindahl, C. Mechanical and repeated antimicrobial therapy using a local drug delivery system in the treatment of peri-implantitis: A randomized clinical trial. J. Periodontol. 2008, 79, 836–844. [Google Scholar] [CrossRef] [PubMed]
- Schär, D.; Ramseier, C.A.; Eick, S.; Arweiler, N.B.; Sculean, A.; Salvi, G.E. Anti-infective therapy of peri-implantitis with adjunctive local drug delivery or photodynamic therapy: Six-month outcomes of a prospective randomized clinical trial. Clin. Oral Implants Res. 2013, 24, 104–110. [Google Scholar] [CrossRef] [PubMed]
- van Winkelhoff, A.J. Antibiotics in the treatment of peri-implantitis. Eur. J. Oral Implantol. 2012, 5, S43–S50. [Google Scholar] [PubMed]
- Kotsakis, G.A.; Konstantinidis, I.; Karoussis, I.K.; Ma, X.; Chu, H. Systematic review and meta-analysis of the effect of various laser wavelengths in the treatment of peri-implantitis. J. Periodontol. 2014, 85, 1203–1213. [Google Scholar] [CrossRef] [PubMed]
- Salvi, G.E.; Persson, G.R.; Heitz-Mayfield, L.J.; Frei, M.; Lang, N.P. Adjunctive local antibiotic therapy in the treatment of peri-implantitis II: Clinical and radiographic outcomes. Clin. Oral Implants Res. 2007, 18, 281–285. [Google Scholar] [CrossRef]
- Monje, A.; Aranda, L.; Diaz, K.T.; Alarcón, M.A.; Bagramian, R.A.; Wang, H.L.; Catena, A. Impact of Maintenance Therapy for the Prevention of Peri-implant Diseases: A Systematic Review and Meta-analysis. J. Dent. Res. 2016, 95, 372–379. [Google Scholar] [CrossRef]
- Lang, N.P.; Wetzel, A.C.; Stich, H.; Caffesse, R.G. Histologic probe penetration in healthy and inflamed peri-implant tissues. Clin. Oral Implants Res. 1994, 5, 191–201. [Google Scholar] [CrossRef]
- Ji, Y.J.; Tang, Z.H.; Wang, R.; Cao, J.; Cao, C.F.; Jin, L.J. Effect of glycine powder air-polishing as an adjunct in the treatment of peri-implant mucositis: A pilot clinical trial. Clin. Oral Implants Res. 2014, 25, 683–689. [Google Scholar] [CrossRef]
- Riben-Grundstrom, C.; Norderyd, O.; André, U.; Renvert, S. Treatment of peri-implant mucositis using a glycine powder air-polishing or ultrasonic device: A randomized clinical trial. J. Clin. Periodontol. 2015, 42, 462–469. [Google Scholar] [CrossRef] [PubMed]
- Iorio-Siciliano, V.; Blasi, A.; Isola, G.; Sculean, A.; Salvi, G.E.; Ramaglia, L. Resolution of peri-implant mucositis at tissue- and bone-level implants: A 6-month prospective controlled clinical trial. Clin. Oral Implants Res. 2023, 34, 450–462. [Google Scholar] [CrossRef] [PubMed]
- Menezes, K.M.; Fernandes-Costa, A.N.; Silva-Neto, R.D.; Calderon, P.S.; Gurgel, B.C. Efficacy of 0.12% Chlorhexidine Gluconate for Non-Surgical Treatment of Peri-Implant Mucositis. J. Periodontol. 2016, 87, 1305–1313. [Google Scholar] [CrossRef]
- Coli, P.; Christiaens, V.; Sennerby, L.; Bruyn, H. Reliability of periodontal diagnostic tools for monitoring peri-implant health and disease. Periodontol. 2000 2017, 73, 203–217. [Google Scholar] [CrossRef] [PubMed]
- Farina, R.; Filippi, M.; Brazzioli, J.; Tomasi, C.; Trombelli, L. Bleeding on probing around dental implants: A retrospective study of associated factors. J. Clin. Periodontol. 2017, 44, 115–122. [Google Scholar] [CrossRef] [PubMed]
- Gerber, J.A.; Tan, W.C.; Balmer, T.E.; Salvi, G.E.; Lang, N.P. Bleeding on probing and pocket probing depth in relation to probing pressure and mucosal health around oral implants. Clin. Oral Implants Res. 2009, 20, 75–78. [Google Scholar] [CrossRef] [PubMed]
- Serino, G.; Turri, A.; Lang, N.P. Probing at implants with peri-implantitis and its relation to clinical peri-implant bone loss. Clin. Oral Implants Res. 2013, 24, 91–95. [Google Scholar] [CrossRef] [PubMed]
- Sanz-Martín, I.; Sanz-Sánchez, I.; Carrillo de Albornoz, A.; Figuero, E.; Sanz, M. Effects of modified abutment characteristics on peri-implant soft tissue health: A systematic review and meta-analysis. Clin. Oral Implants Res. 2018, 29, 118–129. [Google Scholar] [CrossRef] [PubMed]
- Rams, T.E.; Degener, J.E.; van Winkelhoff, A.J. Prevalence of β-lactamase-producing bacteria in human periodontitis. J. Periodontal. Res. 2013, 48, 493–499. [Google Scholar] [CrossRef]
- de Tapia, B.; Bonnin, M.; Valles, C.; Mozas, C.; Herrera, D.; Sanz, M.; Nart, J. Clinical outcomes and associated factors in the treatment of peri-implant mucositis, combining mechanical debridement and prosthesis modification: A 30-month follow-up prospective case series. J. Clin. Periodontol. 2022, 49, 1357–1365. [Google Scholar] [CrossRef]
- Romanos, G.E.; Schesni, A.; Nentwig, G.-H.; Winter, A.; Sader, R.; Brandt, S. Impact of Implant Diameter on Success and Survival of Dental Implants: An Observational Cohort Study. Prosthesis 2023, 5, 888–897. [Google Scholar] [CrossRef]
- Ericsson, I.; Berglundh, T.; Marinello, C.; Liljenberg, B.; Lindhe, J. Long-standing plaque and gingivitis at implants and teeth in the dog. Clin. Oral Implants Res. 1992, 3, 99–103. [Google Scholar] [CrossRef] [PubMed]
- Salvi, G.E.; Stähli, A.; Imber, J.C.; Sculean, A.; Roccuzzo, A. Physiopathology of peri-implant diseases. Clin. Implant Dent. Relat. Res. 2023, 25, 629–639. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total | Test Group | Control Group | p-Value | |
|---|---|---|---|---|
| Number of patients | 31 | 16 | 15 | |
| Number of implants | 31 | 16 | 15 | |
| SD) | 0.538 | |||
| Gender | 0.365 | |||
| Female (n, %) | 16 | 7 (43.8%) | 9 (60%) | |
| Male (n, %) | 15 | 9 (56.2%) | 6 (40%) | |
| Smoker | 0.998 | |||
| Smoker ≤ 10 cig/day, n (%) | 3 | 2 (12.5%) | 1 (6.67%) | |
| Never smokers, number (%) | 28 | 14 (87.5%) | 14 (93.33%) | |
| Implant position | 0.238 | |||
| Anterior maxilla | 2 | 2 | 0 | |
| Posterior maxilla | 15 | 8 | 7 | |
| Anterior ma ndible | 2 | 1 | 1 | |
| Posterior ma ndible | 12 | 5 | 7 | |
| PPD (n, %) | 96 | 90 | ||
| 2 mm | 11 (11.45%) | 13 (14.44%) | ||
| 3 mm | 46 (47.91%) | 48 (53.33%) | ||
| 4 mm | 38 (39.58%) | |||
| 5 mm | 1 (1.04%) | 3 (3.33%) |
| Parameter | Group | N | Baseline (T0) | 3-Month (T1) | Baseline–3 Months | p-Value Intra-Group | 6-Month (T2) | Baseline–6 Months | p-Value Intra-Group | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | |||||
| BoP | Test | 16 | <0.001 | <0.001 | ||||||||||
| Control | 15 | <0.001 | <0.001 | |||||||||||
| p-value | 0.094 | 0.471 | 0.199 | 0.813 | 0.039 | |||||||||
| PPD | Test | 16 | 0.006 | 0.009 | ||||||||||
| Control | 15 | 3.00 | 0.116 | 0.125 | ||||||||||
| p-value | 0.460 | 0.444 | 0.082 | 0.560 | 0.060 | |||||||||
| mPiI | Test | 16 | 0.018 | 0.300 | ||||||||||
| Control | 15 | 0.106 | 0.294 | |||||||||||
| p-value | 0.873 | 0.311 | 0.745 | 0.851 | 0.967 | |||||||||
| mBI | Test | 16 | <0.001 | <0.001 | ||||||||||
| Control | 15 | <0.001 | <0.001 | |||||||||||
| p-value | 0.068 | 0.981 | 0.038 | 0.813 | 0.036 | |||||||||
| FMPS | Test | 16 | <0.001 | <0.001 | ||||||||||
| Control | 15 | <0.001 | <0.001 | |||||||||||
| p-value | 0.719 | 0.083 | 0.232 | 0.036 | 0.232 | |||||||||
| FMBS | Test | 16 | <0.001 | <0.001 | ||||||||||
| Control | 15 | <0.001 | <0.001 | |||||||||||
| p-value | 0.809 | 0.135 | 0.201 | 0.082 | 0.105 | |||||||||
| Test Group (n = 16) n (%) | Control Group (n= 15) n (%) | p-Value | |
|---|---|---|---|
| BoP sites ≤ 1 | 9 (56.25%) | 6 (40%) | 0.366 * |
| BoP sites > 1 | 7 (43.75%) | 9 (60%) |
| Species | Time Point | Detection Score | Test Group (n = 16) | Control Group (n = 15) | p-Value |
|---|---|---|---|---|---|
| A. actinomycetemcomitans | baseline | 0 | 14 (87.50%) | 15 (100%) | 0.163 |
| 1 | - | - | |||
| 2 | 1 (6.25%) | - | |||
| 3 | - | - | |||
| 4 | 1 (6.25%) | - | |||
| 3 months | 0 | 14 (87.50%) | 15 (100%) | 0.163 | |
| 1 | - | - | |||
| 2 | 1 (6.25%) | - | |||
| 3 | - | - | |||
| 4 | 1 (6.25%) | - | |||
| p-value | 1 | - | |||
| P. gingivalis | baseline | 0 | 3 (18.8%) | 2 (25%) | 0.779 |
| 1 | 1 (6.25%) | 1 (13.3%) | |||
| 2 | 8 (50%) | 8 (53.3%) | |||
| 3 | 4 (25%) | 4 (26.7%) | |||
| 4 | - | - | |||
| 3 months | 0 | 4 (25%) | 2 (13.3%) | 0.715 | |
| 1 | 2 (1.25%) | 4 (26.7%) | |||
| 2 | 9 (56.2%) | 7 (46.7%) | |||
| 3 | 1 (6.25%) | 2 (13.3%) | |||
| 4 | - | - | |||
| p-value | 0.240 | 0.263 | |||
| P. intermedia | baseline | 0 | 10 (62.5%) | 9 (60%) | 0.783 |
| 1 | 2 (12.5%) | - | |||
| 2 | 3 (18.8%) | 6 (40%) | |||
| 3 | 1 (6.25%) | - | |||
| 4 | - | - | |||
| 3 months | 0 | 13 (81.2%) | 12 (80%) | 0.931 | |
| 1 | 1 (6.25%) | 1 (6.67%) | |||
| 2 | 2 (12.5%) | 2 (13.3%) | |||
| 3 | - | - | |||
| 4 | - | - | |||
| p-value | 0.242 | 0.194 | |||
| T. forsythia | baseline | 0 | 2 (12.5%) | 1 (6.67%) | 0.796 |
| 1 | 1 (6.25%) | 1 (6.67%) | |||
| 2 | 6 (37.5%) | 8 (53.3%) | |||
| 3 | 7 (43.8%) | 5 (33.3%) | |||
| 4 | - | - | |||
| 3 months | 0 | 5 (31.2%) | 1 (6.67%) | 0.535 | |
| 1 | 2 (12.5%) | 4 (26.7%) | |||
| 2 | 5 (31.2%) | 7 (46.7%) | |||
| 3 | 4 (25%) | 3 (20%) | |||
| 4 | - | - | |||
| p-value | 0.138 | 0.242 | |||
| T. denticola | baseline | 0 | 4 (25%) | 3 (20%) | 0.074 |
| 1 | 8 (50%) | 2 (13.3%) | |||
| 2 | 4 (25%) | 10 (66.7%) | |||
| 3 | - | - | |||
| 4 | - | - | |||
| 3 months | 0 | 8 (50%) | 10 (66.7%) | 0.446 | |
| 1 | 6 (37.5%) | 3 (20%) | |||
| 2 | 2 (12.5%) | 2 (13.3%) | |||
| 3 | - | - | |||
| 4 | - | - | |||
| p-value | 0.148 | 0.003 | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ilyes, I.; Boariu, M.; Rusu, D.; Iorio-Siciliano, V.; Vela, O.; Boia, S.; Kardaras, G.; Șurlin, P.; Calniceanu, H.; Jentsch, H.; et al. A Single Dose of Piperacillin Plus Tazobactam Gel as an Adjunct to Professional Mechanical Plaque Removal (PMPR) in Patients with Peri-Implant Mucositis: A 6-Month Double-Blind Randomized Clinical Trial. Antibiotics 2024, 13, 269. https://doi.org/10.3390/antibiotics13030269
Ilyes I, Boariu M, Rusu D, Iorio-Siciliano V, Vela O, Boia S, Kardaras G, Șurlin P, Calniceanu H, Jentsch H, et al. A Single Dose of Piperacillin Plus Tazobactam Gel as an Adjunct to Professional Mechanical Plaque Removal (PMPR) in Patients with Peri-Implant Mucositis: A 6-Month Double-Blind Randomized Clinical Trial. Antibiotics. 2024; 13(3):269. https://doi.org/10.3390/antibiotics13030269
Chicago/Turabian StyleIlyes, Ioana, Marius Boariu, Darian Rusu, Vincenzo Iorio-Siciliano, Octavia Vela, Simina Boia, Georgios Kardaras, Petra Șurlin, Horia Calniceanu, Holger Jentsch, and et al. 2024. "A Single Dose of Piperacillin Plus Tazobactam Gel as an Adjunct to Professional Mechanical Plaque Removal (PMPR) in Patients with Peri-Implant Mucositis: A 6-Month Double-Blind Randomized Clinical Trial" Antibiotics 13, no. 3: 269. https://doi.org/10.3390/antibiotics13030269