
Daptomycin Use for Persistent Coagulase-Negative Staphylococcal Bacteremia in a Neonatal Intensive Care Unit
 , and
, and
Abstract
:1. Introduction
2. Results
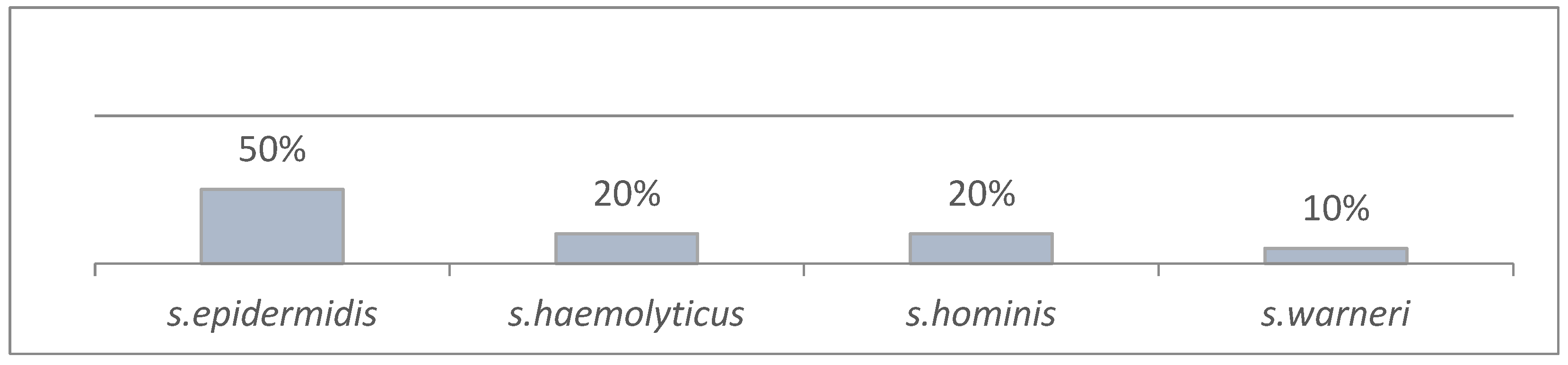
2.1. General
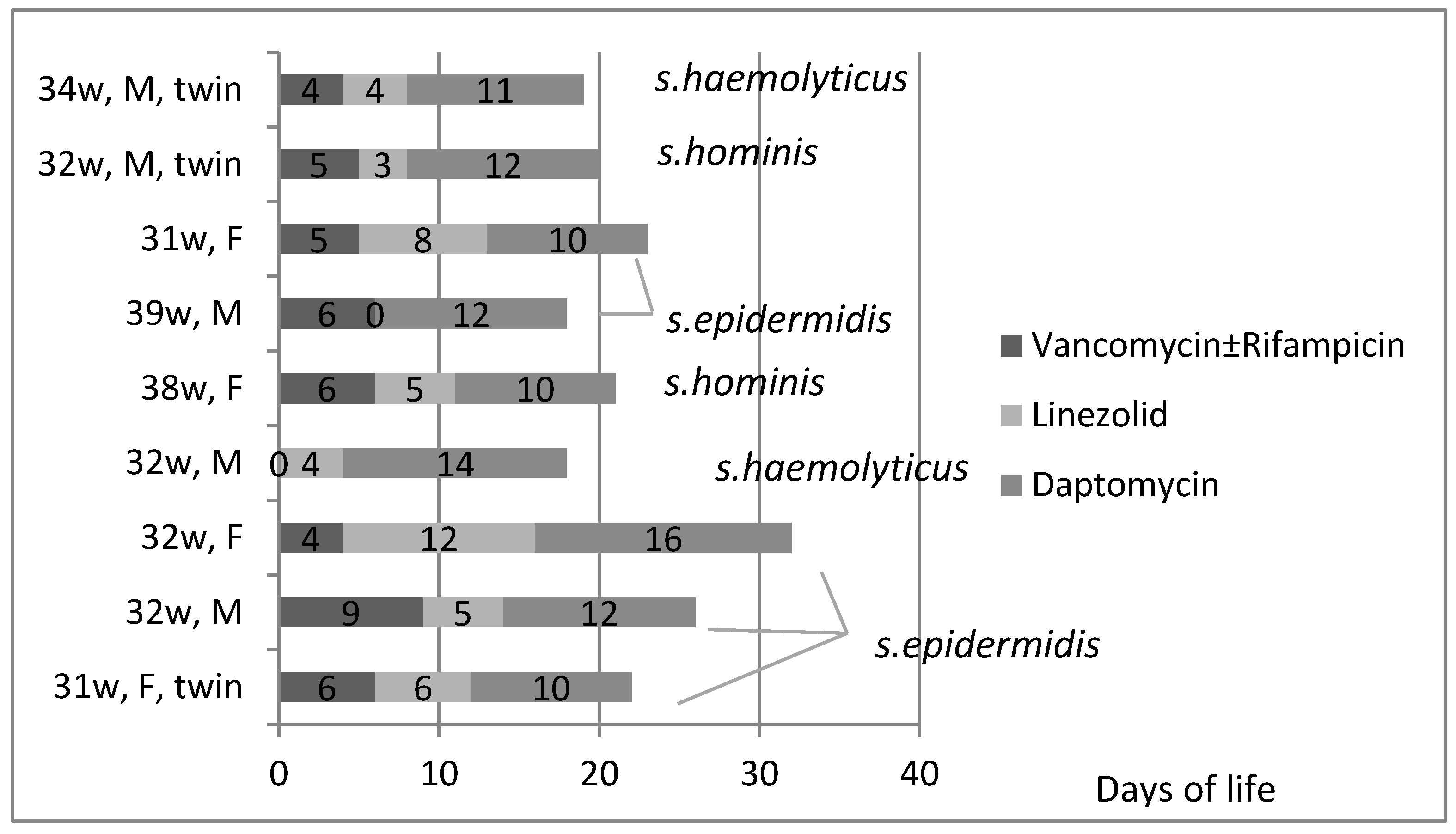
2.2. Daptomycin-Treated Neonates
3. Discussion
4. Materials and Methods
4.1. Patients
4.2. Active Epidemiological Surveillance (Years 2020–2022)
4.3. Microbiological Evaluation
4.4. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Korang, S.K.; Safi, S.; Nava, C.; Greisen, G.; Gupta, M.; Lausten-Thomsen, U.; Jakobsen, J.C. Antibiotic regimens for late-onset neonatal sepsis. Cochrane Database Syst. Rev. 2021, 5, CD013836. [Google Scholar] [CrossRef] [PubMed]
- Stoll, B.J.; Hansen, N.; Fanaroff, A.A.; Wright, L.L.; Carlo, W.A.; Ehrenkranz, R.A.; Lemons, J.A.; Donovan, E.F.; Stark, A.R.; Tyson, J.E.; et al. Late-onset sepsis in very low birth weight neonates: The experience of the NICHD Neonatal Research Network. Pediatrics 2002, 110 Pt 1, 285–291. [Google Scholar] [CrossRef] [PubMed]
- Tsai, M.H.; Hsu, J.F.; Chu, S.M.; Lien, R.; Huang, H.R.; Chiang, M.C.; Fu, R.H.; Lee, C.W.; Huang, Y.C. Incidence, clinical characteristics and risk factors for adverse outcome in neonates with late-onset sepsis. Pediatr. Infect. Dis. J. 2014, 33, e7–e13. [Google Scholar] [CrossRef] [PubMed]
- Greenberg, R.G.; Kandefer, S.; Do, B.T.; Smith, P.B.; Stoll, B.J.; Bell, E.F.; Carlo, W.A.; Laptook, A.R.; Sanchez, P.J.; Shankaran, S.; et al. Late-onset Sepsis in Extremely Premature Infants: 2000–2011. Pediatr. Infect. Dis. J. 2017, 36, 774–779. [Google Scholar] [CrossRef] [PubMed]
- Lutsar, I.; Chazallon, C.; Carducci, F.I.; Trafojer, U.; Abdelkader, B.; de Cabre, V.M.; Esposito, S.; Giaquinto, C.; Heath, P.T.; Ilmoja, M.L.; et al. Current management of late onset neonatal bacterial sepsis in five European countries. Eur. J. Pediatr. 2014, 173, 997–1004. [Google Scholar] [CrossRef] [PubMed]
- Schlapbach, L.J.; Aebischer, M.; Adams, M.; Natalucci, G.; Bonhoeffer, J.; Latzin, P.; Nelle, M.; Bucher, H.U.; Latal, B.; Swiss Neonatal, N.; et al. Impact of sepsis on neurodevelopmental outcome in a Swiss National Cohort of extremely premature infants. Pediatrics 2011, 128, e348–e357. [Google Scholar] [CrossRef] [PubMed]
- Institute of Medicine (US). Committee on Understanding Premature Birth and Assuring Healthy Outcomes. In Preterm Birth: Causes, Consequences, and Prevention; Behrman, R.E., Butler, A.S., Eds.; National Academies Press: Washington, DC, USA, 2007. [Google Scholar]
- Chowers, M.Y.; Gottesman, B.; Paul, M.; Weinberger, M.; Pitlik, S.; Leibovici, L. Persistent bacteremia in the absence of defined intravascular foci: Clinical significance and risk factors. Eur. J. Clin. Microbiol. Infect. Dis. 2003, 22, 592–596. [Google Scholar] [CrossRef] [PubMed]
- Vogel, L.; Sloos, J.H.; Spaargaren, J.; Suiker, I.; Dijkshoorn, L. Biofilm production by Staphylococcus epidermidis isolates associated with catheter related bacteremia. Diagn. Microbiol. Infect. Dis. 2000, 36, 139–141. [Google Scholar] [CrossRef]
- Rohde, H.; Frankenberger, S.; Zahringer, U.; Mack, D. Structure, function and contribution of polysaccharide intercellular adhesin (PIA) to Staphylococcus epidermidis biofilm formation and pathogenesis of biomaterial-associated infections. Eur. J. Cell Biol. 2010, 89, 103–111. [Google Scholar] [CrossRef]
- Furuichi, M.; Miyairi, I. Risk factors for persistent bacteremia in infants with catheter-related bloodstream infection due to coagulase-negative Staphylococcus in the neonatal intensive care unit. J. Infect. Chemother. 2016, 22, 785–789. [Google Scholar] [CrossRef]
- Strunk, T.; Richmond, P.; Simmer, K.; Currie, A.; Levy, O.; Burgner, D. Neonatal immune responses to coagulase-negative staphylococci. Curr. Opin. Infect. Dis. 2007, 20, 370–375. [Google Scholar] [CrossRef]
- Rose, W.E.; Poppens, P.T. Impact of biofilm on the in vitro activity of vancomycin alone and in combination with tigecycline and rifampicin against Staphylococcus aureus. J. Antimicrob. Chemother. 2009, 63, 485–488. [Google Scholar] [CrossRef]
- Gkentzi, D.; Kolyva, S.; Spiliopoulou, I.; Marangos, M.; Dimitriou, G. Treatment Options for Persistent Coagulase Negative Staphylococcal Bacteremia in Neonates. Curr. Pediatr. Rev. 2016, 12, 199–208. [Google Scholar] [CrossRef]
- Pham, J.T. Challenges of Vancomycin Dosing and Therapeutic Monitoring in Neonates. J. Pediatr. Pharmacol. Ther. 2020, 25, 476–484. [Google Scholar] [CrossRef]
- Chan, J.I.; Noor, A.; Clauss, C.; Aggarwal, R.; Nayak, A. Methicillin-Resistant Staphylococcus aureus Endovascular Infection in a Neonate: Prolonged, Safe, and Effective Use of Daptomycin and Enoxaparin. J. Pediatr. Pharmacol. Ther. 2020, 25, 68–74. [Google Scholar] [CrossRef]
- Shibata, Y.; Yamagishi, Y.; Mikamo, H.; Kato, H.; Nishiyama, N.; Asai, N.; Koizumi, Y.; Matsuura, K.; Suematsu, H.; Hagihara, M. Comparative study on safety of linezolid and vancomycin in the treatment of infants and neonates for Gram-positive bacterial infections. J. Infect. Chemother. 2018, 24, 695–701. [Google Scholar] [CrossRef]
- Uptodate, Wolters Kluwer, Daptomycin-Drug Information. Available online: www.uptodate.com (accessed on 12 December 2023).
- Bellou, V.; Gkentzi, D.; Giormezis, N.; Vervenioti, A.; Spiliopoulou, I.; Dimitriou, G. Persistent Coagulase-Negative Staphylococcal Bacteremia in Neonates: Clinical, Microbiological Characteristics and Changes within a Decade. Antibiotics 2022, 11, 765. [Google Scholar] [CrossRef] [PubMed]
- Hsu, J.F.; Chu, S.M.; Lee, C.W.; Yang, P.H.; Lien, R.; Chiang, M.C.; Fu, R.H.; Huang, H.R.; Tsai, M.H. Incidence, clinical characteristics and attributable mortality of persistent bloodstream infection in the neonatal intensive care unit. PLoS ONE 2015, 10, e0124567. [Google Scholar] [CrossRef] [PubMed]
- Saiman, L. Strategies for prevention of nosocomial sepsis in the neonatal intensive care unit. Curr. Opin. Pediatr. 2006, 18, 101–106. [Google Scholar] [CrossRef] [PubMed]
- Antachopoulos, C.; Iosifidis, E.; Sarafidis, K.; Bazoti, F.; Gikas, E.; Katragkou, A.; Drossou-Agakidou, V.; Roilides, E. Serum levels of daptomycin in pediatric patients. Infection 2012, 40, 367–371. [Google Scholar] [CrossRef] [PubMed]
- Hartman, S.J.F.; Bruggemann, R.J.; Orriens, L.; Dia, N.; Schreuder, M.F.; de Wildt, S.N. Pharmacokinetics and Target Attainment of Antibiotics in Critically Ill Children: A Systematic Review of Current Literature. Clin. Pharmacokinet. 2020, 59, 173–205. [Google Scholar] [CrossRef]
- Gawronski, K.M. Successful Use of Daptomycin in a Preterm Neonate with Persistent Methicillin-Resistant Staphylococcus epidermidis Bacteremia. J. Pediatr. Pharmacol. Ther. 2015, 20, 61–65. [Google Scholar] [CrossRef]
- Hussain, A.; Kairamkonda, V.; Jenkins, D.R. Successful treatment of meticillin-resistant Staphylococcus aureus bacteraemia in a neonate using daptomycin. J. Med. Microbiol. 2011, 60 Pt 3, 381–383. [Google Scholar] [CrossRef]
- Sarafidis, K.; Iosifidis, E.; Gikas, E.; Tsivitanidou, M.; Drossou-Agakidou, V.; Roilides, E. Daptomycin use in a neonate: Serum level monitoring and outcome. Am. J. Perinatol. 2010, 27, 421–424. [Google Scholar] [CrossRef]
- Minotti, C.; Zuccon, I.; Priante, E.; Bonadies, L.; Di Chiara, C.; Dona, D.; Baraldi, E.; Costenaro, P. Daptomycin for Treatment of S. Epidermidis Endocarditis in an Extremely Preterm Neonate-Outcome and Perspectives. Children 2022, 9, 457. [Google Scholar] [CrossRef]
- Mohzari, Y.; Aljobair, F.; Alrashed, A.; Asdaq, S.M.B.; Alshuraim, R.A.; Asfour, S.S.; Al-Mouqdad, M.M.; Bamogaddam, R.F.; Al-Anazi, D.; Zeilinger, C.E.; et al. Safety and Efficacy of Daptomycin in Neonates with Coagulase-Negative Staphylococci: Case Series Analysis. Antibiotics 2021, 10, 168. [Google Scholar] [CrossRef]
- Asfour, S.S.; Aljobair, F.; Abdelrahim, A.; Al-Mouqdad, M.M. High alanine aminotransaminase associated with daptomycin use in a premature infant. J. Mother Child. 2021, 25, 65–68. [Google Scholar] [CrossRef]
- Dong, Y.; Speer, C.P.; Glaser, K. Beyond sepsis: Staphylococcus epidermidis is an underestimated but significant contributor to neonatal morbidity. Virulence 2018, 9, 621–633. [Google Scholar] [CrossRef] [PubMed]
- Marchant, E.A.; Boyce, G.K.; Sadarangani, M.; Lavoie, P.M. Neonatal sepsis due to coagulase-negative staphylococci. Clin. Dev. Immunol. 2013, 2013, 586076. [Google Scholar] [CrossRef] [PubMed]
- Klingenberg, C.; Aarag, E.; Ronnestad, A.; Sollid, J.E.; Abrahamsen, T.G.; Kjeldsen, G.; Flaegstad, T. Coagulase-negative staphylococcal sepsis in neonates. Association between antibiotic resistance, biofilm formation and the host inflammatory response. Pediatr. Infect. Dis. J. 2005, 24, 817–822. [Google Scholar] [CrossRef] [PubMed]
- Arrieta, A.C.; Bradley, J.S.; Popejoy, M.W.; Bensaci, M.; Grandhi, A.; Bokesch, P.; Glasser, C.; Du, L.; Patino, H.; Kartsonis, N.A. Randomized Multicenter Study Comparing Safety and Efficacy of Daptomycin Versus Standard-of-care in Pediatric Patients with Staphylococcal Bacteremia. Pediatr. Infect. Dis. J. 2018, 37, 893–900. [Google Scholar] [CrossRef]
- Tedeschi, S.; Tumietto, F.; Conti, M.; Giannella, M.; Viale, P.; Team, S.O.A.S. Use of Daptomycin in Critically Ill Children with Bloodstream Infections and Complicated Skin and Soft-tissue Infections. Pediatr. Infect. Dis. J. 2016, 35, 180–182. [Google Scholar] [CrossRef]
- Syriopoulou, V.; Dailiana, Z.; Dmitriy, N.; Utili, R.; Pathan, R.; Hamed, K. Clinical Experience with Daptomycin for the Treatment of Gram-positive Infections in Children and Adolescents. Pediatr. Infect. Dis. J. 2016, 35, 511–516. [Google Scholar] [CrossRef] [PubMed]
- Syrogiannopoulos, G.A.; Michoula, A.N.; Petinaki, E.; Grivea, I.N. Daptomycin Use in Children: Experience with Various Types of Infection and Age Groups. Pediatr. Infect. Dis. J. 2017, 36, 962–966. [Google Scholar] [CrossRef] [PubMed]
- Garazzino, S.; Castagnola, E.; Di Gangi, M.; Ortolano, R.; Krzysztofiak, A.; Nocerino, A.; Esposito, S.; D’Argenio, P.; Galli, L.; Losurdo, G.; et al. Daptomycin for Children in Clinical Practice Experience. Pediatr. Infect. Dis. J. 2016, 35, 639–641. [Google Scholar] [CrossRef] [PubMed]
- Sakoulas, G.; Alder, J.; Thauvin-Eliopoulos, C.; Moellering, R.C., Jr.; Eliopoulos, G.M. Induction of daptomycin het-erogeneous susceptibility in Staphylococcus aureus by exposure to vancomycin. Antimicrob. Agents Chemother. 2006, 50, 1581–1585. [Google Scholar] [CrossRef]
- Rose, W.E.; Leonard, S.N.; Sakoulas, G.; Kaatz, G.W.; Zervos, M.J.; Sheth, A.; Carpenter, C.F.; Rybak, M.J. Daptomycin activity against Staph-ylococcus aureus following vancomycin exposure in an in vitro pharmacodynamic model with simulated endocardial vegetations. Antimicrob. Agents Chemother. 2008, 52, 831–836. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Demographics (1) | |
|---|---|
| Median gestational age | 32 weeks (IQR 31.25–33.5) |
| Mean birth weight | 1840 ± 867.4 g |
| Apgar 1 min (median IQR) | 9 (8–9) |
| Apgar 5 min (median IQR) | 9 (9–10) |
| Mean day of life of LOS (±sd) | 7 ± 3.9 |
| Admission temperature (°C) | 36.5 ± 0.65 |
| Demographics (2) | Number/Total (%) |
| Sex (male) | 8/12 (66.7%) |
| Prematurity (<37 weeks) | 8/10 (80%) |
| Vaginal delivery | 3/10 (30%) |
| Emergency caesarean section | 7/10 (70%) |
| PROM > 18 h | 2/10 (20%) |
| Meconium-stained liquor | 1/10 (10%) |
| Intubation at birth | 6/10 (60%) |
| Singleton pregnancy | 8/12 (66.7%) |
| Congenital anomalies | 1/12 (8.3%) |
| Ex utero transfers | 2/12 (16.7%) |
| Demographics (3) | s. epidermidis | s. haemolyticus | s. hominis |
|---|---|---|---|
| Median gestational age (IQR) weeks | 33 (31–39) | 33 (32–34) | 34 (31–38) |
| Mean birth weight (±SD) grams | 1930 ± 1127 | 1990 ± 325 | 1990 ± 551 |
| Number of positive blood cultures | 61 | 15 | 15 |
| Positive blood cultures while taking daptomycin (>24 h) | 3 * | 0 | 0 |
| Mean NICU admission (days) | 46 | 30 | 27 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Papachatzi, E.; Gkentzi, D.; Tzifas, S.; Dassios, T.; Dimitriou, G. Daptomycin Use for Persistent Coagulase-Negative Staphylococcal Bacteremia in a Neonatal Intensive Care Unit. Antibiotics 2024, 13, 254. https://doi.org/10.3390/antibiotics13030254
Papachatzi E, Gkentzi D, Tzifas S, Dassios T, Dimitriou G. Daptomycin Use for Persistent Coagulase-Negative Staphylococcal Bacteremia in a Neonatal Intensive Care Unit. Antibiotics. 2024; 13(3):254. https://doi.org/10.3390/antibiotics13030254
Chicago/Turabian StylePapachatzi, Eleni, Despoina Gkentzi, Sotiris Tzifas, Theodore Dassios, and Gabriel Dimitriou. 2024. "Daptomycin Use for Persistent Coagulase-Negative Staphylococcal Bacteremia in a Neonatal Intensive Care Unit" Antibiotics 13, no. 3: 254. https://doi.org/10.3390/antibiotics13030254