
Central Venous Catheters versus Peripherally Inserted Central Catheters: A Comparison of Indwelling Time Resulting in Colonization by Multidrug-Resistant Pathogens

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Collection
2.2. Catheter Care
2.3. Indications for Catheter Removal
2.4. Culture Techniques
2.5. Definitions
2.6. Statistical Analysis
3. Results
3.1. Participants Characteristics
3.2. Colonization Incidence Rates and MDROs/Non-MDROs Proportion in the CVC and PICC Cohorts
3.3. Colonization Incidence Rates among the Three Groups in the CVC Cohort
3.4. Colonization Incidence Rates among the Three Groups in the PICC Cohort
3.5. Comparison of Colonization Events, MDROs, and Non-MDROs between the Three Groups in the CVC and PICC Cohorts
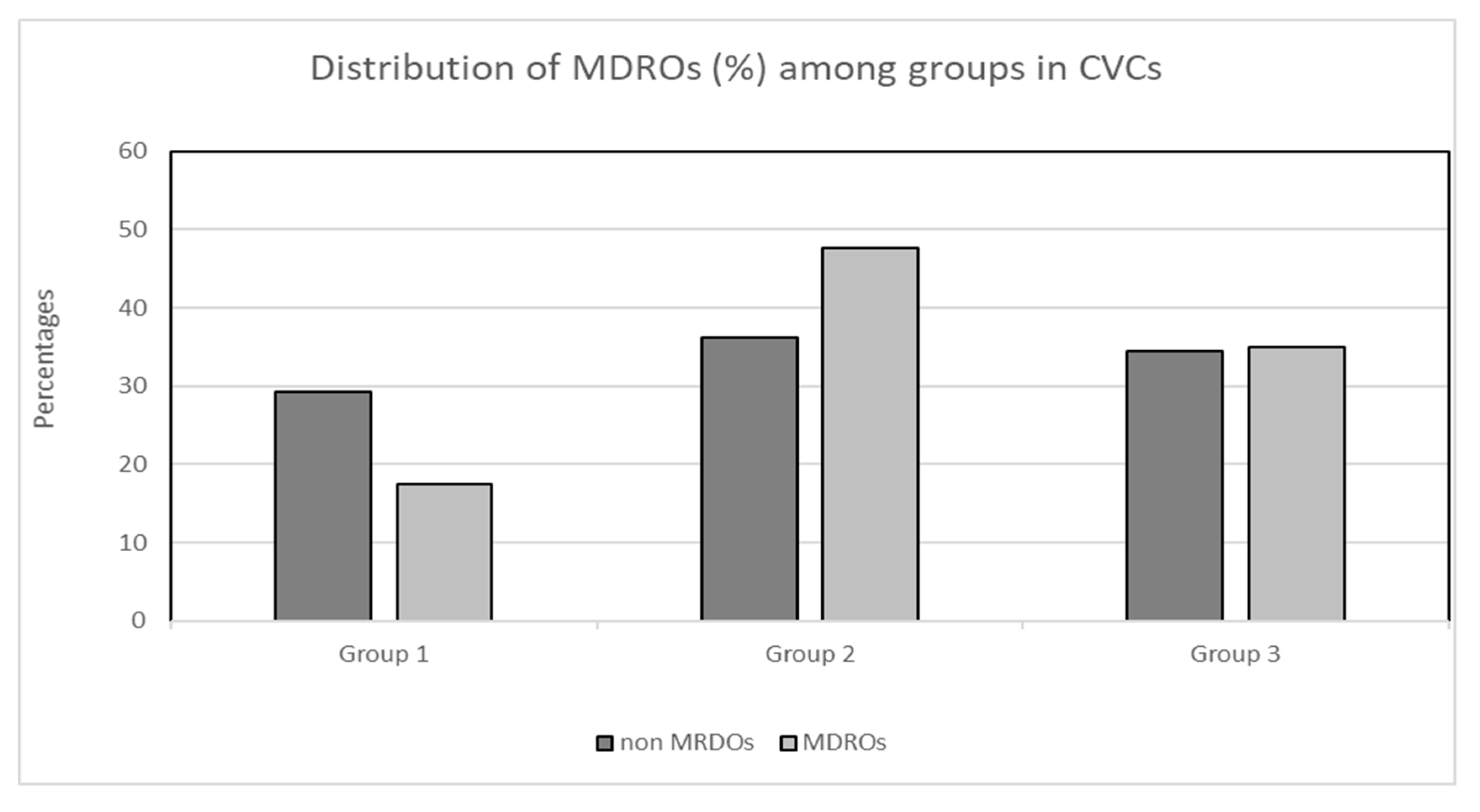
3.6. Comparison of MDRO/Non-MDRO Proportions between the Three Groups in the CVC and PICC Cohorts
3.7. MDRO Identification and Distribution among the Three Groups in the CVC and PICC Cohorts
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mermel, L.A.; Allon, M.; Bouza, E.; Craven, D.E.; Flynn, P.; O’Grady, N.P.; Raad, I.I.; Rijnders, B.J.; Sherertz, R.J.; Warren, D.K. Clinical practice guidelines for the diagnosis and management of intravascular catheter-related infection: 2009 Update by the Infectious Diseases Society of America. Clin. Infect. Dis. 2009, 49, 1–45, Erratum in Clin. Infect. Dis. 2010, 50, 1079; Dosage error in article text. Erratum in Clin. Infect. Dis. 2010, 50, 457. [Google Scholar] [CrossRef]
- Al Raiy, B.; Fakih, M.G.; Bryan-Nomides, N.; Hopfner, D.; Riegel, E.; Nenninger, T.; Rey, J.; Szpunar, S.; Kale, P.; Khatib, R. Peripherally inserted central venous catheters in the acute care setting: A safe alternative to high-risk short-term central venous catheters. Am. J. Infect. Control 2010, 38, 149–153. [Google Scholar] [CrossRef]
- Fearonce, G.; Faraklas, I.; Saffle, J.R.; Cochran, A. Peripherally inserted central venous catheters and central venous catheters in burn patients: A comparative review. J. Burn. Care Res. 2010, 31, 31–35. [Google Scholar] [CrossRef]
- Adrian, M.; Borgquist, O.; Kröger, T.; Linné, E.; Bentzer, P.; Spångfors, M.; Åkeson, J.; Holmström, A.; Linnér, R.; Kander, T. Mechanical complications after central venous catheterisation in the ultrasound-guided era: A prospective multicentre cohort study. Br. J. Anaesth. 2022, 129, 843–850. [Google Scholar] [CrossRef]
- Puri, A.; Dai, H.; Giri, M.; Wu, C.; Huang, H.; Zhao, Q. The incidence and risk of venous thromboembolism associated with peripherally inserted central venous catheters in hospitalized patients: A systematic review and meta-analysis. Front. Cardiovasc. Med. 2022, 9, 917572. [Google Scholar] [CrossRef]
- Santos, F.K.Y.; Flumignan, R.L.G.; Areias, L.L.; Sarpe, A.K.P.; Amaral, F.C.F.; Ávila, R.B.; Vasconcelos, V.T.; Guedes Neto, H.J.; Amorim, J.E.; Nakano, L.C.U. Peripherally inserted central catheter versus central venous catheter for intravenous access: A protocol for systematic review and meta-analysis. Medicine 2020, 99, e20352. [Google Scholar] [CrossRef]
- Bonizzoli, M.; Batacchi, S.; Cianchi, G.; Zagli, G.; Lapi, F.; Tucci, V.; Martini, G.; Di Valvasone, S.; Peris, A. Peripherally inserted central venous catheters and central venous catheters related thrombosis in post-critical patients. Intensive Care Med. 2011, 37, 284–289. [Google Scholar] [CrossRef]
- Revel-Vilk, S.; Yacobovich, J.; Tamary, H.; Goldstein, G.; Nemet, S.; Weintraub, M.; Paltiel, O.; Kenet, G. Risk factors for central venous catheter thrombotic complications in children and adolescents with cancer. Cancer 2010, 116, 4197–4205. [Google Scholar] [CrossRef]
- Lv, Y.; Huang, X.; Lan, Y.; Xia, Q.; Chen, F.; Wu, J.; Li, W.; Cao, H.; Xie, C.; Li, L.; et al. Peripherally inserted central catheters have a protective role and the effect of fluctuation curve feature in the risk of bloodstream infection compared with central venous catheters: A propensity-adjusted analysis. BMC Infect. Dis. 2022, 22, 289. [Google Scholar] [CrossRef]
- Chopra, V.; O’Horo, J.; Rogers, M.; Maki, D.; Safdar, N. The Risk of Bloodstream Infection Associated with Peripherally Inserted Central Catheters Compared with Central Venous Catheters in Adults: A Systematic Review and Meta-Analysis. Infect. Control Hosp. Epidemiol. 2013, 34, 908–918. [Google Scholar] [CrossRef]
- Maki, D.G.; Kluger, D.M.; Crnich, C.J. The risk of bloodstream infection in adults with different intravascular devices: A systematic review of 200 published prospective studies. Mayo Clin. Proc. 2006, 81, 1159–1171. [Google Scholar] [CrossRef]
- Patel, A.R.; Patel, A.R.; Singh, S.; Singh, S.; Khawaja, I. Central Line Catheters and Associated Complications: A Review. Cureus 2019, 11, e4717. [Google Scholar] [CrossRef]
- Pitiriga, V.; Kanellopoulos, P.; Bakalis, I.; Kampos, E.; Sagris, I.; Saroglou, G.; Tsakris, A. Central venous catheter-related bloodstream infection and colonization: The impact of insertion site and distribution of multidrug-resistant pathogens. Antimicrob. Resist. Infect. Control 2020, 9, 189. [Google Scholar] [CrossRef]
- Pitiriga, V.; Bakalis, J.; Kampos, E.; Kanellopoulos, P.; Saroglou, G.; Tsakris, A. Duration of central venous catheter placement and central line-associated bloodstream infections after the adoption of prevention bundles: A two-year retrospective study. Antimicrob. Resist. Infect. Control 2022, 11, 96. [Google Scholar] [CrossRef]
- Lafuente Cabrero, E.; Terradas Robledo, R.; Civit Cuñado, A.; García Sardelli, D.; Hidalgo López, C.; Giro Formatger, D.; Lacueva Perez, L.; Esquinas López, C.; Tortosa Moreno, A. Risk factors of catheter- associated bloodstream infection: Systematic review and meta-analysis. PLoS ONE 2023, 18, e0282290. [Google Scholar] [CrossRef]
- Pitiriga, V.; Bakalis, J.; Theodoridou, K.; Dimitroulia, E.; Saroglou, G.; Tsakris, A. Comparison of microbial colonization rates between central venous catheters and peripherally inserted central catheters. Antimicrob. Resist. Infect. Control 2023, 12, 74. [Google Scholar] [CrossRef]
- Maki, D.G.; Weise, C.E.; Sarafin, H.W. A semiquantitative culture method for identifying intravenous-catheter-related infection. N. Engl. J. Med. 1977, 296, 1305–1309. [Google Scholar] [CrossRef]
- Magiorakos, A.-P.; Srinivasan, A.; Carey, R.B.; Carmeli, Y.; Falagas, M.E.; Giske, C.G.; Harbarth, S.; Hindler, J.F.; Kahlmeter, G.; Olsson-Liljequist, B.; et al. Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria: An international expert proposal for interim standard definitions for acquired resistance. Clin. Microbiol. Infect. 2012, 18, 268–281. [Google Scholar] [CrossRef]
- Stevens, V.; Geiger, K.; Concannon, C.; Nelson, R.E.; Brown, J.; Dumyati, G. Inpatient costs, mortality and 30-day re-admission in patients with central-line-associated bloodstream infections. Clin. Microbiol. Infect. 2014, 20, O318–O324. [Google Scholar] [CrossRef]
- Rijnders, B.J.A.; Van Wijngaerden, E.; Peetermans, W.E. Catheter-Tip Colonization as a Surrogate End Point in Clinical Studies on Catheter-Related Bloodstream Infection: How Strong Is the Evidence? Clin. Infect. Dis. 2002, 35, 1053–1058. [Google Scholar] [CrossRef]
- Mermel, L.A. Short-term Peripheral Venous Catheter-Related Bloodstream Infections: A Systematic Review. Clin. Infect. Dis. 2017, 65, 1757–1762. [Google Scholar] [CrossRef] [PubMed]
- Mermel, L.A. What is the predominant source of intravascular catheter infections? Clin. Infect. Dis. 2011, 52, 211–212. [Google Scholar] [CrossRef] [PubMed]
- Raad, I. Intravascular-catheter-related infections. Lancet 1998, 351, 893–898. [Google Scholar] [CrossRef] [PubMed]
- McLaws, M.; Berry, G. Nonuniform Risk of Bloodstream Infection with Increasing Central Venous Catheter-Days. Infect. Control Hosp. Epidemiol. 2005, 26, 715–719. [Google Scholar] [CrossRef] [PubMed]
- Park, S.; Moon, S.; Pai, H.; Kim, B. Appropriate duration of peripherally inserted central catheter maintenance to prevent central line-associated bloodstream infection. PLoS ONE 2020, 15, e0234966. [Google Scholar] [CrossRef]
- Caris, M.G.; de Jonge, N.A.; Punt, H.J.; Salet, D.M.; de Jong, V.M.T.; Lissenberg-Witte, B.I.; Zweegman, S.; Vandenbroucke-Grauls, C.M.J.E.; van Agtmael, M.A.; Janssen, J.J.W.M. Indwelling time of peripherally inserted central catheters and incidence of bloodstream infections in haematology patients: A cohort study. Antimicrob. Resist. Infect. Control 2022, 11, 37. [Google Scholar] [CrossRef]
- Wang, L.; Ren, Y.; Gao, X. Relationship between central line-associated bloodstream infection and catheter dwell time in neonates. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue 2022, 34, 320–324. (In Chinese) [Google Scholar] [CrossRef]
- Pérez-Granda, M.J.; Guembe, M.; Cruces, R.; Barrio, J.M.; Bouza, E. Assessment of central venous catheter colonization using surveillance culture of withdrawn connectors and insertion site skin. Crit. Care 2016, 20, 32. [Google Scholar] [CrossRef]
- He, Y.; Zhao, H.; Wei, Y.; Gan, X.; Ling, Y.; Ying, Y. Retrospective Analysis of Microbial Colonization Patterns in Central Venous Catheters, 2013–2017. J. Health Eng. 2019, 2019, 8632701. [Google Scholar] [CrossRef]
- Böll, B.; Schalk, E.; Buchheidt, D.; Hasenkamp, J.; Kiehl, M.; Kiderlen, T.R.; Kochanek, M.; Koldehoff, M.; Kostrewa, P.; Claßen, A.Y.; et al. Central venous catheter–related infections in hematology and oncology: 2020 updated guidelines on diagnosis, management, and prevention by the Infectious Diseases Working Party (AGIHO) of the German Society of Hematology and Medical Oncology (DGHO). Ann. Hematol. 2021, 100, 239–259. [Google Scholar] [CrossRef]
- Sohail, M.; Latif, Z. Molecular analysis, biofilm formation, and susceptibility of methicillin-resistant Staphylococcus aureus strains causing community-and health care-associated infections in central venous catheters. Rev. Soc. Bras. Med. Tropical. 2018, 51, 603–609. [Google Scholar] [CrossRef] [PubMed]
- Alonso, B.; Latorre, M.C.; Cruces, R.; Ampuero, D.; Haces, L.; Martín-Rabadán, P.; Sánchez-Carrillo, C.; Rodríguez, B.; Bouza, E.; Muñoz, P.; et al. Evaluation of the Alfred™ turbidity monitoring system (Alifax®) following sonication in the diagnosis of central venous catheter colonization. Eur. J. Clin. Microbiol. Infect. Dis. 2019, 38, 1737–1742. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, F.S.; Clemente de Luca, F.A.; Ribeiro da Cunha, A.; Fortaleza, C.M.C.B. Season, weather and predictors of healthcare-associated gram-negative bloodstream infections: A case-only study. J. Hosp. Infect. 2019, 101, 134–141. [Google Scholar] [CrossRef] [PubMed]
- Bassetti, M.; Merelli, M.; Ansaldi, F.; de Florentiis, D.; Sartor, A.; Scarparo, C.; Callegari, A.; Righi, E. Clinical and therapeutic aspects of candidemia: A five-year single centre study. PLoS ONE 2015, 10, e0127534. [Google Scholar] [CrossRef]
- Chen, C.-Y.; Sheng, W.-H.; Huang, S.-Y.; Chou, W.-C.; Yao, M.; Tang, J.-L.; Tsay, W.; Tien, H.-F.; Hsueh, P.-R. Clinical characteristics and treatment outcomes of patients with candidaemia due to Candida parapsilosis sensulato species at a medical centre in Taiwan, 2000–2012. J. Antimicrob. Chemother. 2015, 70, 1531–1538. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | N of Patients (%) | ||
|---|---|---|---|
| PICCs (n = 63) | CVCs (n = 144) | p-Value * | |
| Age, mean ± SD, (years) | 53.90 ± 17.98 | 55.62 ± 18.36 | NS |
| Gender (M/F) | 41/18 | 80/64 | NS |
| Obesity | 25 (39.6) | 59 (41) | NS |
| Diabetes mellitus | 15 (23.8) | 31 (21.5) | NS |
| Pulmonary disease | 8 (12.7) | 18 (12.5) | NS |
| Hypertension | 35 (55.5) | 70 (48.6) | NS |
| Renal disease | 10 (15.8) | 27 (18.7) | NS |
| Oncologic disease | 12 (19) | 25 (17.3) | NS |
| Immune deficiency/suppression | 18 (28.5) | 39 (27) | NS |
| Admission category | |||
| Medical | 40 (63.5) | 85 (59) | NS |
| Surgery | 23 (36.5) | 59 (41) | NS |
| Mechanical ventilation | 7 (11.1) | 15 (10.4) | NS |
| Cardiovascular disease | 23 (36.5) | 40 (27.7) | NS |
| Neurological disease | 23 (36.5) | 45 (31.2) | NS |
| Gastroenterological disease | 15 (23.8) | 38 (26.3) | NS |
| Hospital death | 2 (3.1) | 4 (2.7) | NS |
| APACHE score | 13.22 ± 3.48 | 13.18 ± 3.1 | NS |
| Variables | ≤7 Days | 8–14 Days | >14 Days | Total | p-Value * |
|---|---|---|---|---|---|
| No. of catheters | 904 | 202 | 81 | 1187 | |
| Catheter days | 4585 | 2874 | 2315 | 9774 | |
| Colonization (No) | 32 | 62 | 50 | 144 | |
| Colonization (%) | 3.5 | 30.7 | 61.7 | 12.1 | |
| Colonization incidence rate (per 1.000 catheter/days) | 6.98 | 21.57 | 21.60 | 14.73 | 0.019 |
| MDROs (No.) | 15 | 41 | 30 | 86 | |
| MDROs (%) | 1.7 | 20.3 | 37.0 | 7.2 | |
| MDROs incidence rate (per 1.000 catheter/days) | 3.27 | 14.27 | 12.96 | 8.79 | 0.025 |
| non-MDROs (No.) | 17 | 21 | 20 | 58 | |
| non-MDROs (%) | 1.9 | 10.4 | 24.7 | 4.8 | |
| non-MDRO incidence rate (per 1.000 catheter/days) | 3.71 | 7.31 | 8.64 | 5.93 | 0.5 |
| Variables | ≤7 Days | 8–14 Days | >14 Days | Total | p-Value * |
|---|---|---|---|---|---|
| No. of catheters | 86 | 378 | 175 | 639 | |
| Catheter days | 2014 | 3756 | 5340 | 11,110 | |
| Colonization (No.) | 3 | 12 | 48 | 63 | |
| Colonization (%) | 3.49 | 3.17 | 27.43 | 9.8 | |
| Colonization incidence rate (per 1.000 catheter/days) | 1.49 | 3.19 | 8.99 | 5.67 | 0.047 |
| MDRO (No) | 0 | 3 | 9 | 12 | |
| MDRO (%) | 0.0 | 0.8 | 5.1 | 1.8 | |
| MDRO incidence rate (per 1.000 catheter/days) | 0.0 | 0.8 | 1.69 | 1.08 | 0.78 |
| non-MDRO (No.) | 3 | 9 | 39 | 51 | |
| non-MDRO (%) | 3.5 | 2.4 | 22.3 | 7.9 | |
| non-MDRO incidence rate (per 1.000 catheter/days) | 1.49 | 2.40 | 7.30 | 4.59 | 0.054 |
| Microorganisms | CVCs (Νo. = 144) | PICCs (Νo. = 63) | Total |
|---|---|---|---|
| Gram-negative bacilli | |||
| Esherichia coli | 10 (6.9%) | 0 (0.0%) | 10 (4.8%) |
| Enterobacter cloacae | 2 (1.4%) | 3 (4.8%) | 5 (2.4%) |
| Klebsiella pneumoniae | 3 (2.1%) | 3 (4.8%) | 6 (2.9%) |
| Morganella morganii | 1 (0.7%) | 0 (0.0%) | 1 (0.5%) |
| Pseudomonas aeruginosa | 7 (4.9%) | 3 (4.8%) | 10 (4.8%) |
| Proteus. mirabilis | 3 (2.1%) | 0 (0.0%) | 3 (1.4%) |
| Serratia marcescens | 3 (2.1%) | 3 (4.8%) | 6 (2.9%) |
| MDR Acinetobacter baumannii | 44 (30.6%) | 3 (4.8%) | 47 (22.7%) |
| MDR Klebsiella pneumoniae | 27 (18.7%) | 6 (9.5%) | 33 (15.9%) |
| MDR Pseudomonas aeruginosa | 12 (8.3%) | 3 (4.8%) | 15 (7.2%) |
| Gram-positive cocci | |||
| CNS | 3 (2.1%) | 6 (9.5%) | 9 (4.3%) |
| MRSA | 3 (2.1%) | 0 (0.0%) | 3 (1.4%) |
| Enterococcus faecalis | 2 (1.4%) | 3 (4.8%) | 5 (2.4%) |
| Staphylococcus aureus | 1 (0.7%) | 3 (4.8%) | 4 (1.9%) |
| Staphylococcus haemolyticus | 4 (2.8%) | 3 (4.8%) | 7 (3.4%) |
| Streptococcus mitis | 1 (0.7%) | 0 (0.0%) | 1 (0.5%) |
| Fungi | |||
| Candida albicans | 7 (4.9%) | 6 (9.5%) | 13 (6.3%) |
| Candida non-albicans | 10 (6.9%) | 15 (23.8%) | 25 (12.1%) |
| Other fungi | 0 (0.0%) | 3 (4.8%) | 3 (1.4%) |
| Other | |||
| Bacillus spp. | 1 (0.7%) | 0 (0.0%) | 1 (0.5%) |
| Total | 144 | 63 | 207 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pitiriga, V.C.; Bakalis, J.; Campos, E.; Kanellopoulos, P.; Sagris, K.; Saroglou, G.; Tsakris, A. Central Venous Catheters versus Peripherally Inserted Central Catheters: A Comparison of Indwelling Time Resulting in Colonization by Multidrug-Resistant Pathogens. Antibiotics 2024, 13, 89. https://doi.org/10.3390/antibiotics13010089
Pitiriga VC, Bakalis J, Campos E, Kanellopoulos P, Sagris K, Saroglou G, Tsakris A. Central Venous Catheters versus Peripherally Inserted Central Catheters: A Comparison of Indwelling Time Resulting in Colonization by Multidrug-Resistant Pathogens. Antibiotics. 2024; 13(1):89. https://doi.org/10.3390/antibiotics13010089
Chicago/Turabian StylePitiriga, Vassiliki C., John Bakalis, Elsa Campos, Petros Kanellopoulos, Konstantinos Sagris, George Saroglou, and Athanasios Tsakris. 2024. "Central Venous Catheters versus Peripherally Inserted Central Catheters: A Comparison of Indwelling Time Resulting in Colonization by Multidrug-Resistant Pathogens" Antibiotics 13, no. 1: 89. https://doi.org/10.3390/antibiotics13010089