

Characterization of Listeria monocytogenes Strains Isolated in Palermo (Sicily and Italy) during the Years 2018–2020 from Severe Cases of Listeriosis
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Collection of Patients
2.2. DNA Extraction of Clinical LM Strains
2.3. PCR Serogroup
2.4. Multilocus Sequence Typing (MLST)
2.5. Multi-Virulence-Locus Sequence Typing (MVLST)
2.6. Antibiotic Susceptibility of L. monocytogenes Isolates
3. Results
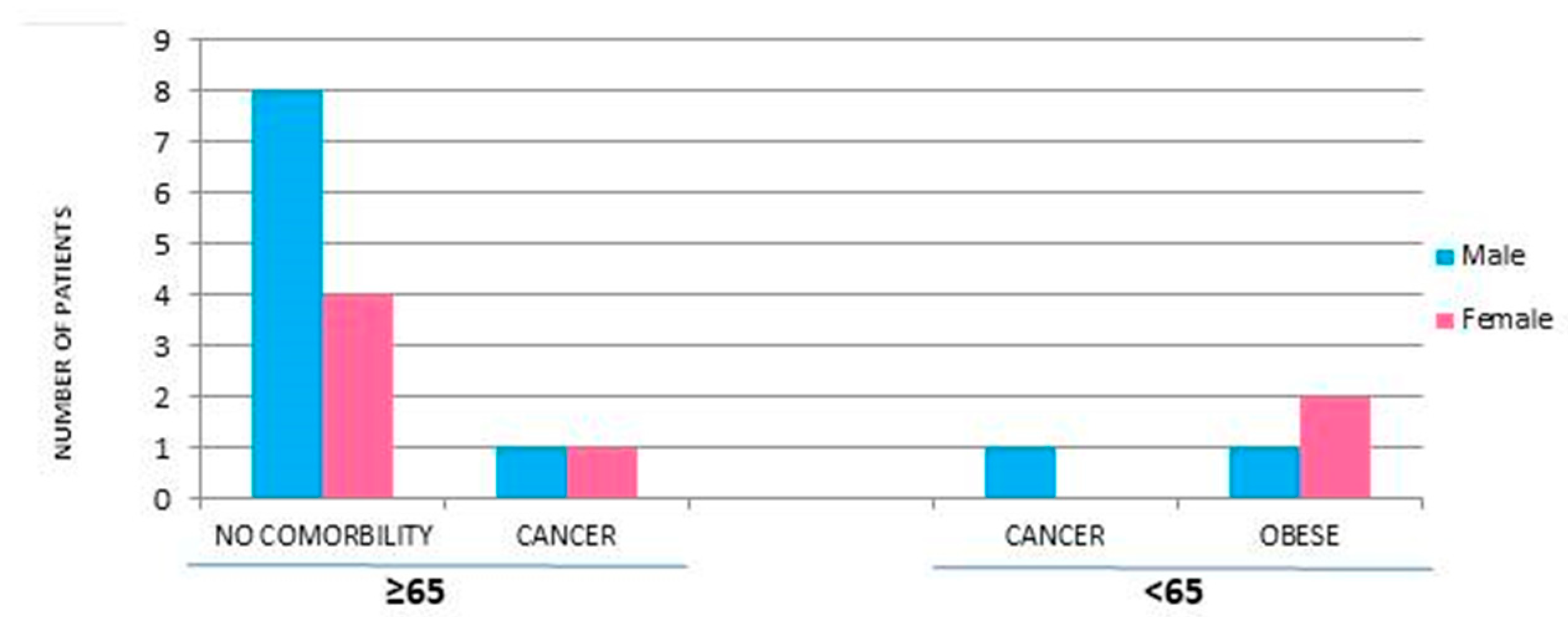
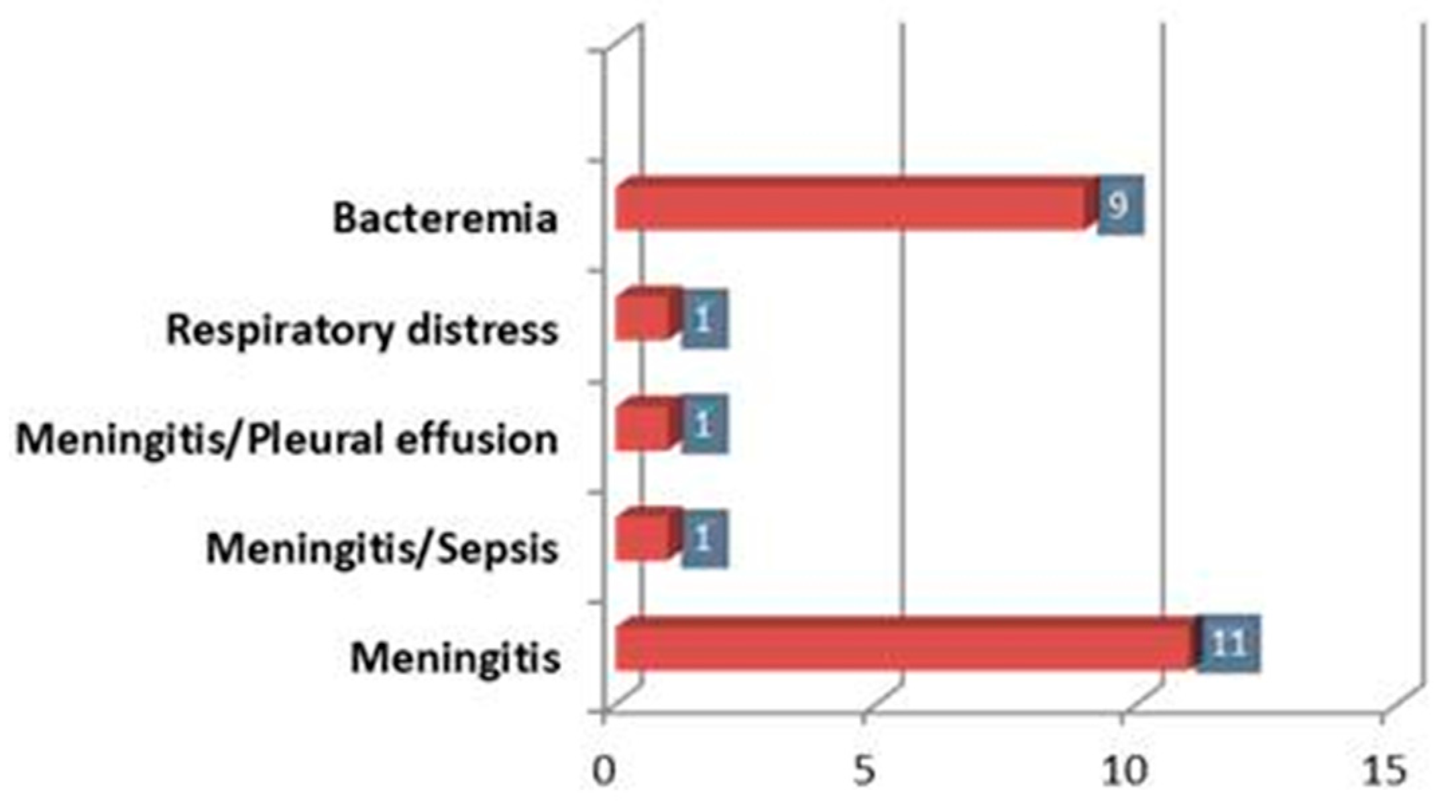
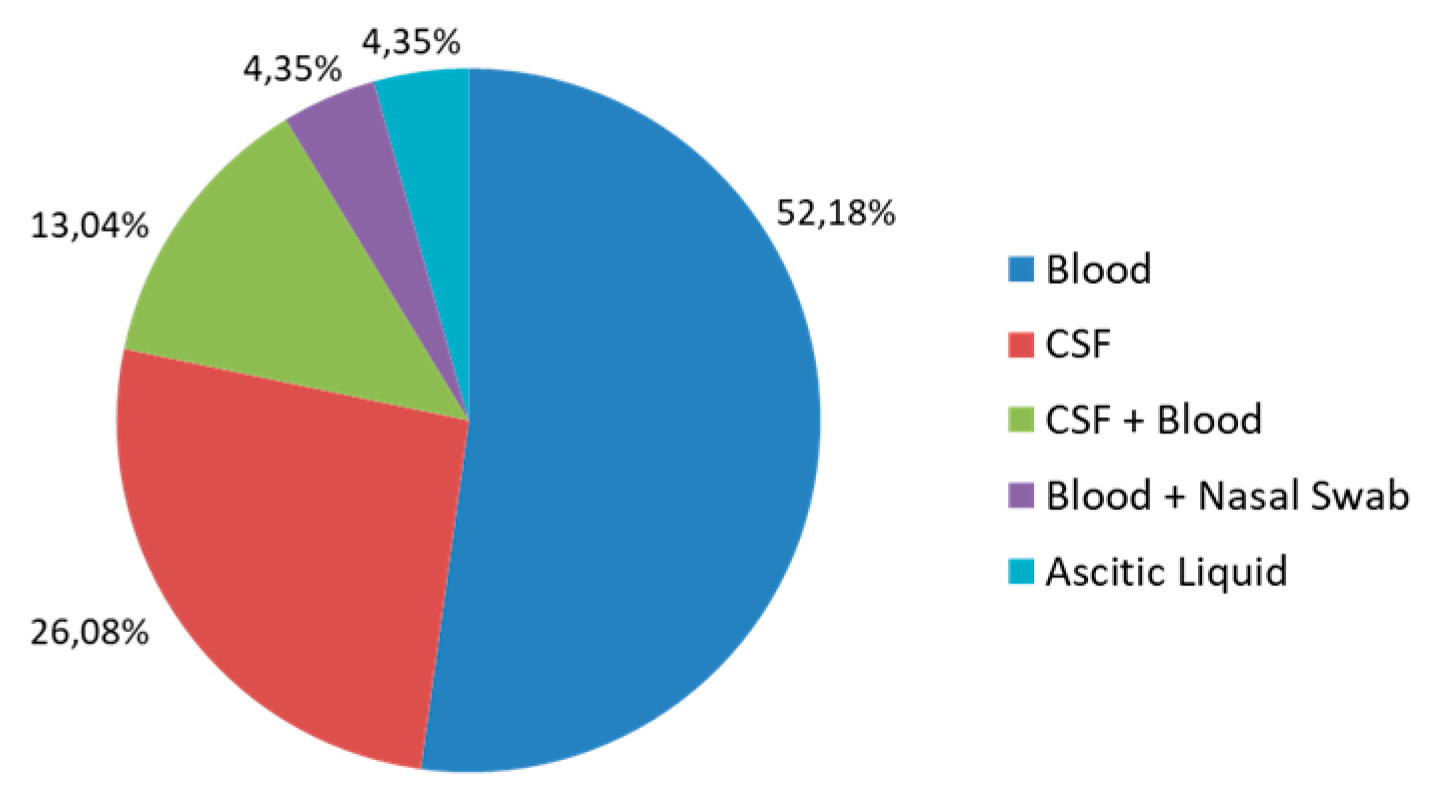
3.1. Demographic and Clinical Characteristics of Listeriosis Patients
3.2. Serogroup
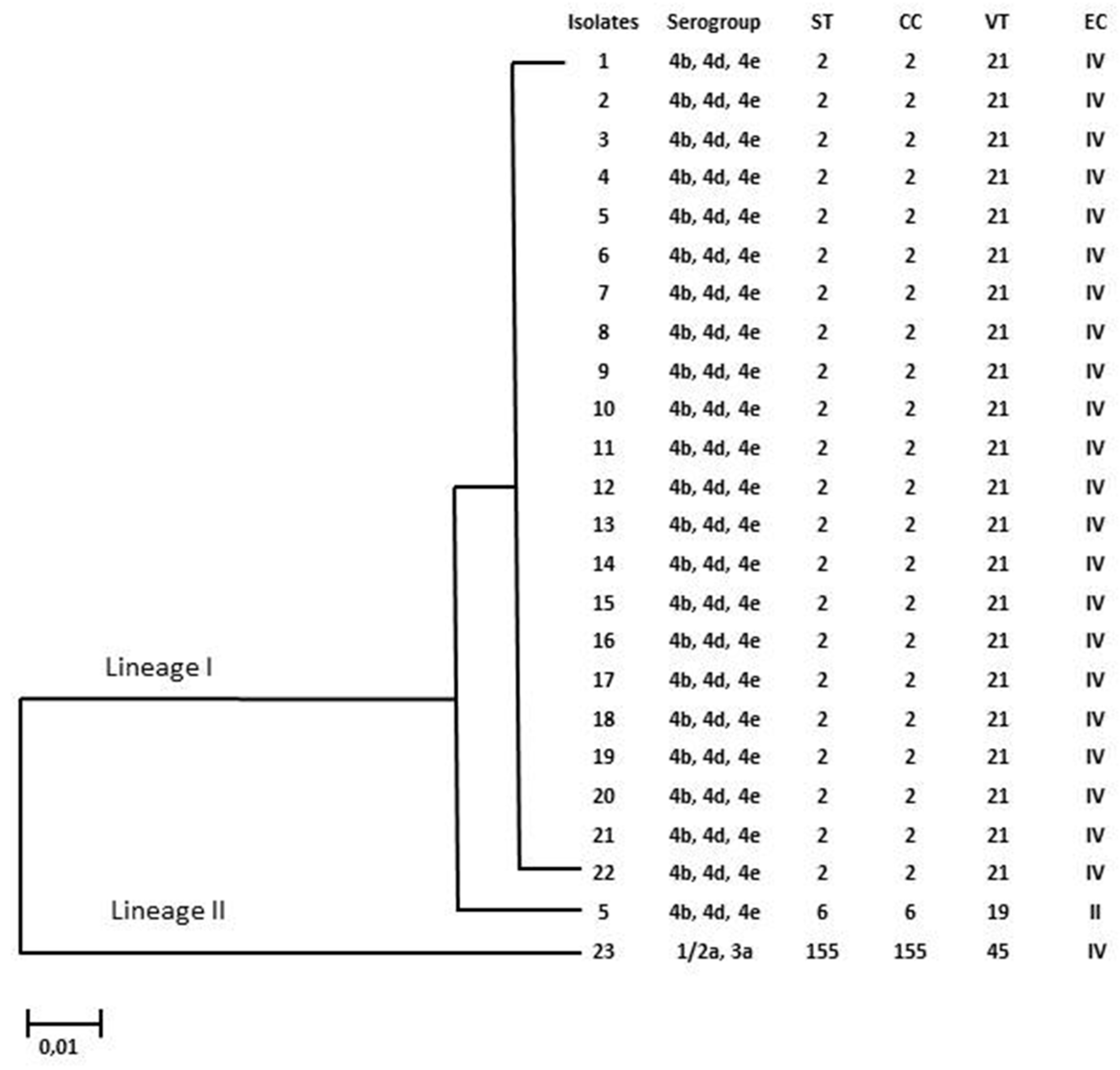
3.3. Multilocus Sequence Typing (MLST)
3.4. Multi-Virulence-Locus Sequence Typing (MvLST)
3.5. MLST and MvLST Analysis
3.6. Antibiotic Susceptibility of L. monocytogenes Isolates
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Swaminathan, B.; Gerner-Smidt, P. The epidemiology of human listeriosis. Microbes Infect. 2007, 9, 1236–1243. [Google Scholar] [CrossRef] [PubMed]
- Lake, F.B.; van Overbeek, L.S.; Baars, J.J.; Koomen, J.; Abee, T.; Besten, H.M.D. Genomic characteristics of Listeria monocytogenes isolated during mushroom (Agaricus bisporus) production and processing. Int. J. Food Microbiol. 2021, 360, 109438. [Google Scholar] [CrossRef] [PubMed]
- Thomas, M.K.; Murray, R.; Flockhart, L.; Pintar, K.; Pollari, F.; Fazil, A.; Nesbitt, A.; Marshall, B.; Racicot, M.; Comeau, G.; et al. Estimates of the Burden of Foodborne Illness in Canada for 30 Specified Pathogens and Unspecified Agents, Circa 2006. Foodborne Pathog. Dis. 2013, 10, 639–648. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Liu, Y.; Zhang, P.; Niu, Y.; Chen, Q.; Ma, X. Genomic Characterization of Clinical Listeria monocytogenes Isolates in Beijing, China. Front. Microbiol. 2021, 12, 751003. [Google Scholar] [CrossRef] [PubMed]
- Cartwright, E.J.; Jackson, K.A.; Johnson, S.D.; Graves, L.M.; Silk, B.J.; Mahon, B.E. Listeriosis Outbreaks and Associated Food Vehicles, United States, 1998–2008. Emerg. Infect. Dis. 2013, 19, 1–9, quiz 184. [Google Scholar] [CrossRef] [PubMed]
- Moravkova, M.; Verbikova, V.; Michna, V.; Babak, V.; Cahlikova, H.; Karpiskova, R.; Kralik, P. Detection and Quantification of Listeria monocytogenes in Ready-to-eat Vegetables, Frozen Vegetables and Sprouts Examined by Culture Methods and Real-time PCR. J. Food Nutr. Res. 2017, 5, 832–837. [Google Scholar] [CrossRef]
- Available online: https://www.epicentro.iss.it/listeria/ (accessed on 2 November 2023).
- Schlech, W.F., 3rd; Acheson, D. Foodborne Listeriosis. Clin. Infect. Dis. 2000, 31, 770–775. [Google Scholar] [CrossRef]
- Available online: https://www.ecdc.europa.eu/en/surveillance-atlas-infectious-diseases (accessed on 2 November 2023).
- Hedberg, C. Listeria in Europe: The need for a European surveillance network is growing. Eurosurveillance 2006, 11, 75–76. [Google Scholar] [CrossRef]
- McLauchlin, J.; Mitchell, R.; Smerdon, W.J.; Jewell, K. Listeria monocytogenes, and listeriosis: A review of hazard characterization for use in microbiological risk assessment of foods. Int. J. Food Microbiol. 2003, 92, 15–33. [Google Scholar] [CrossRef]
- Orsi, R.H.; den Bakker, H.C.; Wiedmann, M. Listeria monocytogenes lineages: Genomics, evolution, ecology and phenotypic characteristics. Int. J. Med. Microbiol. 2011, 301, 79–96. [Google Scholar] [CrossRef]
- Doumith, M.; Buchrieser, C.; Glaser, P.; Jacquet, C.; Martin, P. Differentiation of the Major Listeria monocytogenes Serovars by Multiplex PCR. J. Clin. Microbiol. 2004, 42, 3819–3822. [Google Scholar] [CrossRef] [PubMed]
- Salcedo, C.; Arreaza, L.; Alcalá, B.; de la Fuente, L.; Vázquez, J.A.; Kazor, C.E.; Mitchell, P.M.; Lee, A.M.; Stokes, L.N.; Loesche, W.J.; et al. Development of a Multilocus Sequence Typing Method for Analysis of Listeria monocytogenes Clones. J. Clin. Microbiol. 2003, 41, 558–563. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.; Jayarao, B.M.; Knabel, S.J. Multi-Virulence-Locus Sequence Typing of Listeria monocytogenes. Appl. Environ. Microbiol. 2004, 70, 913–920. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Dong, S.; Chen, H.; Chen, J.; Zhang, J.; Zhang, Z.; Yang, Y.; Xu, Z.; Zhan, L.; Mei, L. Prevalence, Genotypic Characteristics and Antibiotic Resistance of Listeria monocytogenes From Retail Foods in Bulk in Zhejiang Province, China. Front. Microbiol. 2019, 10, 1710. [Google Scholar] [CrossRef] [PubMed]
- Wu, S.; Wu, Q.; Zhang, J.; Chen, M.; Guo, W. Analysis of Multilocus Sequence Typing and Virulence Characterization of Listeria monocytogenes Isolates from Chinese Retail Ready-to-Eat Food. Front. Microbiol. 2016, 7, 168. [Google Scholar] [CrossRef] [PubMed]
- Moura, A.; Criscuolo, A.; Pouseele, H.; Maury, M.M.; Leclercq, A.; Tarr, C. Whole genome-based population biology and epidemiological surveillance of Listeria monocytogenes. Nat. Microbiol. 2016, 2, 16185. [Google Scholar] [CrossRef] [PubMed]
- Available online: https://bigsdb.pasteur.fr/listeria/listeria.html (accessed on 2 November 2023).
- Available online: https://www.megasoftware.net (accessed on 2 November 2023).
- Available online: https://sites.google.com/site/mvlstdatabase/home (accessed on 2 November 2023).
- Marco, F.; Almela, M.; Nolla-Salas, J.; Coll, P.; Gasser, I.; Ferrer, M.D.; de Simon, M. In vitro activities of 22 antimicrobial agents against Listeria monocytogenes strains isolated in Barcelona, Spain. Diagn. Microbiol. Infect. Dis. 2000, 38, 259–261. [Google Scholar] [CrossRef]
- Available online: https://www.cdc.gov/listeria/risk-groups/pregnant-women.html (accessed on 2 November 2023).
- Bauer, A.W.; Kirby, W.M.M.; Sherris, J.C.; Turck, M. Antibiotic Susceptibility Testing by a Standardized Single Disk Method. Am. J. Clin. Pathol. 1966, 45, 493–496. [Google Scholar] [CrossRef]
- Available online: https://www.eucast.org/ (accessed on 2 November 2023).
- Huang, Y.-T.; Kuo, Y.-W.; Lee, M.-R.; Tsai, Y.-H.; Teng, L.-J.; Tsai, M.-S.; Liao, C.-H.; Hsueh, P.-R. Clinical and molecular epidemiology of human listeriosis in Taiwan. Int. J. Infect. Dis. 2021, 104, 718–724. [Google Scholar] [CrossRef]
- Radoshevich, L.; Cossart, P. Listeria monocytogenes: Towards a complete picture of its physiology and pathogenesis. Nat. Rev. Microbiol. 2018, 16, 32–46. [Google Scholar] [CrossRef]
- Available online: https://www.sites.google.com/site/mvlstdatabase/isolates-information-sorted-by-vts/isolates-belonging-to-vt21 (accessed on 2 November 2023).
- Available online: https://www.sites.google.com/site/mvlstdatabase/isolates-information-sorted-by-vts/isolates-belonging-to-vt19 (accessed on 2 November 2023).
- Available online: https://www.sites.google.com/site/mvlstdatabase/isolates-information-sorted-by-vts/isolates-belonging-to-vt45 (accessed on 2 November 2023).
- da Silva, D.A.F.; Vallim, D.C.; Rosas, C.D.O.; de Mello, V.M.; Brandão, M.L.L.; de Filippis, I. Genetic diversity of Listeria monocytogenes serotype 1/2a strains collected in Brazil by Multi-Virulence-Locus Sequence Typing. Lett. Appl. Microbiol. 2020, 72, 316–324. [Google Scholar] [CrossRef] [PubMed]
- Thønnings, S.; Knudsen, J.D.; Schønheyder, H.C.; Søgaard, M.; Arpi, M.; Gradel, K.O.; Østergaard, C.; Jensen, U.; Koch, K.; Pinholt, M.; et al. Antibiotic treatment and mortality in patients with Listeria monocytogenes meningitis or bacteraemia. Clin. Microbiol. Infect. 2016, 22, 725–730. [Google Scholar] [CrossRef] [PubMed]
- Aureli, P.; Fiorucci, G.C.; Caroli, D.; Marchiaro, G.; Novara, O.; Leone, L.; Salmaso, S. An Outbreak of Febrile Gastroenteritis Associated with Corn Contaminated by Listeria monocytogenes. N. Engl. J. Med. 2000, 342, 1236–1241. [Google Scholar] [CrossRef] [PubMed]
- Althaus, D.; Jermini, M.; Giannini, P.; Martinetti, G.; Reinholz, D.; Nüesch-Inderbinen, M.; Lehner, A.; Stephan, R. Local outbreak of Listeria monocytogenes serotype 4b sequence type 6 due to contaminated meat pâté. Foodborne Pathog. Dis. 2017, 14, 219–222. [Google Scholar] [CrossRef] [PubMed]
- Smith, A.M.; Tau, N.P.; Smouse, S.L.; Allam, M.; Ismail, A.; Ramalwa, N.R.; Disenyeng, B.; Ngomane, M.; Thomas, J. Outbreak of Listeria monocytogenes in South Africa, 2017–2018: Laboratory activities and experiences associated with whole-genome sequencing analysis of isolates. Foodborne Pathog. Dis. 2019, 16, 524–530. [Google Scholar] [CrossRef] [PubMed]
- Nüesch-Inderbinen, M.; Bloemberg, G.V.; Müller, A.; Stevens, M.J.; Cernela, N.; Kollöffel, B.; Stephan, R. Listeriosis Caused by Persistence of Listeria monocytogenes Serotype 4b Sequence Type 6 in Cheese Production Environment. Emerg. Infect. Dis. 2021, 27, 284–288. [Google Scholar] [CrossRef] [PubMed]
- Wagner, E.; Zaiser, A.; Leitner, R.; Quijada, N.M.; Pracser, N.; Pietzka, A.; Ruppitsch, W.; Schmitz-Esser, S.; Wagner, M.; Rychli, K. Virulence characterization and comparative genomics of Listeria monocytogenes sequence type 155 strains. BMC Genom. 2020, 21, 847. [Google Scholar] [CrossRef] [PubMed]
- Amato, E. Epidemiologia Della Listeriosi Invasiva in Regione Lombardia: Identificazione dei Genotipi Emergent; Università degli Studi di Milano, Scienze Biomediche, Cliniche e Sperimentali: Milan, Italy, 2016. [Google Scholar] [CrossRef]
- Guidi, F.; Centorotola, G.; Chiaverini, A.; Iannetti, L.; Schirone, M.; Visciano, P.; Cornacchia, A.; Scattolini, S.; Pomilio, F.; D’Alterio, N.; et al. The Slaughterhouse as Hotspot of CC1 and CC6 Listeria monocytogenes Strains with Hypervirulent Profiles in an Integrated Poultry Chain of Italy. Microorganisms 2023, 11, 1543. [Google Scholar] [CrossRef]
- Korsak, D.; Krawczyk-Balska, A.; Hutchinson, H.; Muñoz-Vargas, L.; Feicht, S.; Habing, G.; Colonna, W.; Brehm-Stecher, B.; Shetty, K.; Iii, A.P.; et al. Identification of the Molecular Mechanism of Trimethoprim Resistance in Listeria monocytogenes. Foodborne Pathog. Dis. 2017, 14, 696–700. [Google Scholar] [CrossRef]
- Srinivasan, V.; Nam, H.M.; Nguyen, L.T.; Tamilselvam, B.; Murinda, S.E.; Oliver, S.P. Prevalence of Antimicrobial Resistance Genes in Listeria monocytogenes Isolated from Dairy Farms. Foodborne Pathog. Dis. 2005, 2, 201–211. [Google Scholar] [CrossRef]
- Davis, M.L.; Ricke, S.C.; Donaldson, J.R. Establishment of Listeria monocytogenes in the Gastrointestinal Tract. Microorganisms 2019, 7, 75. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| STs | Clonal Complex (CC) | Lineage | Serovar | VTs | N° Isolates (%) |
|---|---|---|---|---|---|
| 2 | 2 | I | IVb, IVd, IVe | 21 | 21 (92%) |
| 6 | 6 | II | IVb, IVd, IVe | 19 | 1 (4%) |
| 155 | 155 | II | I/IIa, IIIa | 45 | 1 (4%) |
| 2018 | 2019 | 2020 | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| WINTER | SPRING | SUMMER | AUTUMN | WINTER | SPRING | SUMMER | AUTUMN | WINTER | SPRING | SUMMER | AUTUMN | |
| ST2 | 1 | - | - | - | 8 | 3 | 3 | 2 | - | 2 | 2 | - |
| ST6 | - | - | - | - | - | - | 1 | - | - | - | - | - |
| ST155 | - | - | - | - | 1 | - | - | - | - | - | - | - |
| AMPICILLIN | ERYTHROMYCIN | MEROPENEM | PENICILLIN G | TRIMETHOPRIM/ SULFAM | |
|---|---|---|---|---|---|
| LM_01 | S | S | S | S | S |
| LM_02 | S | S | S | S | S |
| LM_03 | S | S | S | S | R |
| LM_04 | S | S | S | S | R |
| LM_05 | S | S | S | R | R |
| LM_06 | S | S | S | S | I |
| LM_07 | S | S | S | S | R |
| LM_08 | S | S | S | S | S |
| LM_09 | S | S | S | S | R |
| LM_10 | S | S | S | S | S |
| LM_11 | S | S | S | S | S |
| LM_12 | S | S | S | S | R |
| LM_13 | S | S | S | S | R |
| LM_14 | S | S | S | S | R |
| LM_15 | S | S | S | S | S |
| LM_16 | S | S | S | S | S |
| LM_17 | S | S | S | S | S |
| LM_18 | S | S | S | S | R |
| LM_19 | S | S | S | S | R |
| LM_20 | S | S | S | I | S |
| LM_21 | S | S | S | S | S |
| LM_22 | S | S | S | S | S |
| LM_23 | S | S | S | S | S |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tricoli, M.R.; Massaro, C.; Arrigo, I.; Diquattro, O.; Di Bernardo, F.; Galia, E.; Palermo, M.; Fasciana, T.; Giammanco, A. Characterization of Listeria monocytogenes Strains Isolated in Palermo (Sicily and Italy) during the Years 2018–2020 from Severe Cases of Listeriosis. Antibiotics 2024, 13, 57. https://doi.org/10.3390/antibiotics13010057
Tricoli MR, Massaro C, Arrigo I, Diquattro O, Di Bernardo F, Galia E, Palermo M, Fasciana T, Giammanco A. Characterization of Listeria monocytogenes Strains Isolated in Palermo (Sicily and Italy) during the Years 2018–2020 from Severe Cases of Listeriosis. Antibiotics. 2024; 13(1):57. https://doi.org/10.3390/antibiotics13010057
Chicago/Turabian StyleTricoli, Maria Rita, Chiara Massaro, Ignazio Arrigo, Orazia Diquattro, Francesca Di Bernardo, Elena Galia, Mario Palermo, Teresa Fasciana, and Anna Giammanco. 2024. "Characterization of Listeria monocytogenes Strains Isolated in Palermo (Sicily and Italy) during the Years 2018–2020 from Severe Cases of Listeriosis" Antibiotics 13, no. 1: 57. https://doi.org/10.3390/antibiotics13010057