
Severity and Bothersomeness of Urinary Tract Infection Symptoms in Women before and after Menopause

Abstract
:1. Introduction
2. Results
3. Discussion
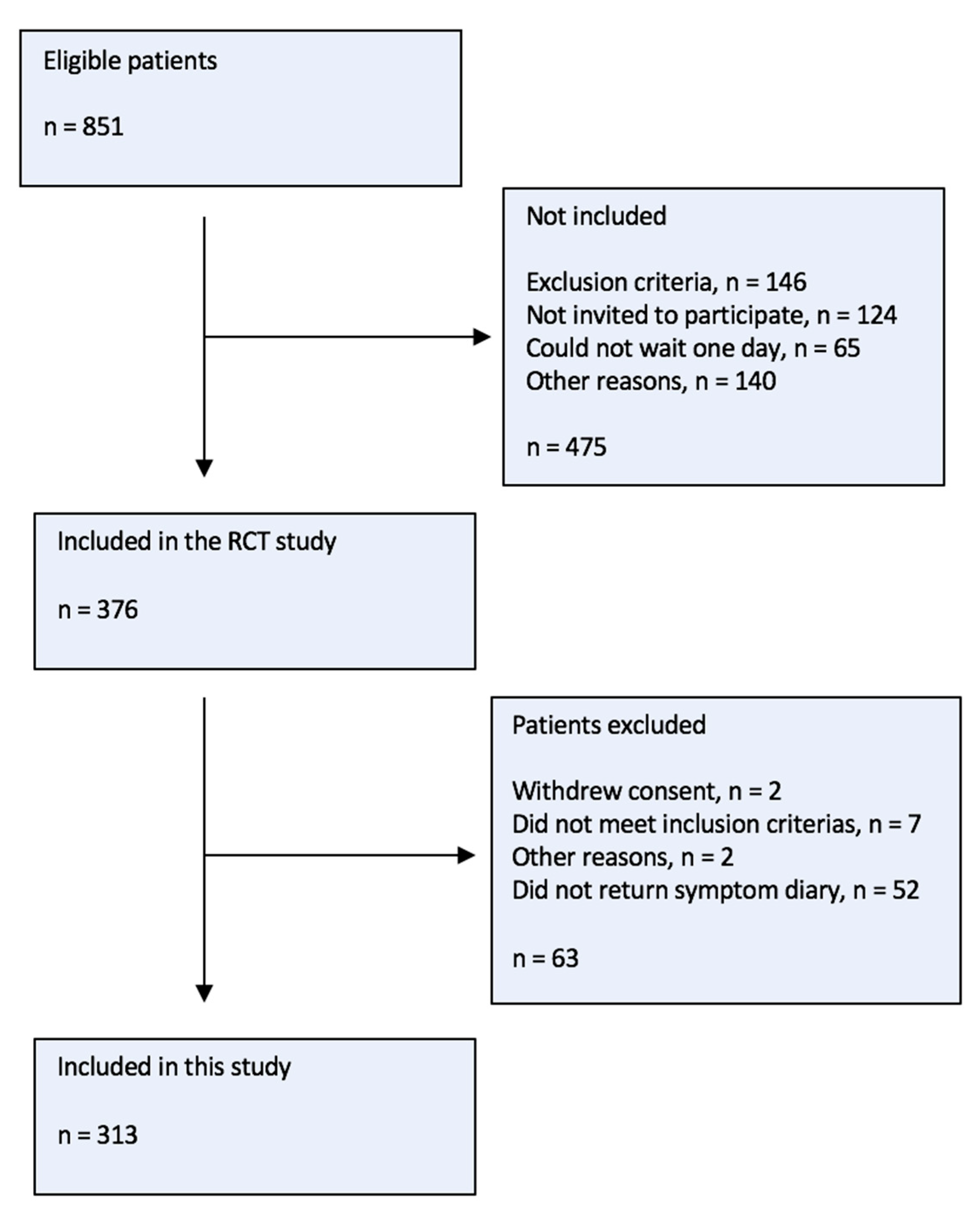
4. Materials and Methods
4.1. Inclusion Criteria
4.2. Data Collection
4.3. Variables
4.4. Statistical Methods
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Pace, W.D.; Dickinson, L.M.; Staton, E.W. Seasonal Variation in Diagnoses and Visits to Family Physicians. Ann. Fam. Med. 2004, 2, 411–417. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aabenhus, R.; Hansen, M.P.; Siersma, V.; Bjerrum, L. Clinical Indications for Antibiotic Use in Danish General Practice: Results from a Nationwide Electronic Prescription Database. Scand. J. Prim. Health Care 2017, 35, 162–169. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Costelloe, C.; Metcalfe, C.; Lovering, A.; Mant, D.; Hay, A.D. Effect of Antibiotic Prescribing in Primary Care on Antimicrobial Resistance in Individual Patients: Systematic Review and Meta-Analysis. BMJ 2010, 340, c2096. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bryce, A.; Hay, A.; Lane, I.; Thornton, H.; Wootton, M.; Costelloe, C. Global Prevalence of Antibiotic Resistance in Paediatric Urinary Tract Infections Caused by Escherichia Coli and Association with Routine Use of Antibiotics in Primary Care: Systematic Review and Meta-Analysis. Br. Med. J. 2016, 352, i939. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaußner, Y.; Röver, C.; Heinz, J.; Hummers, E.; Debray, T.P.A.; Hay, A.D.; Heytens, S.; Vik, I.; Little, P.; Moore, M.; et al. Reducing Antibiotic Use in Uncomplicated Urinary Tract Infections in Adult Women: A Systematic Review and Individual Participant Data Meta-Analysis. Clin. Microbiol. Infect. 2022, 28, 1558–1566. [Google Scholar] [CrossRef] [PubMed]
- Hummers-Pradier, E.; Kochen, M. Urinary Tract Infections in Adult General Practice Patients. Br. J. Gen. Pract. 2002, 52, 752–761. [Google Scholar]
- Hoffmann, T.; Peiris, R.; Del Mar, C.; Cleo, G.; Glasziou, P. Natural History of Uncomplicated Urinary Tract Infection without Antibiotics: A Systematic Review. Br. J. Gen. Pract. 2020, 70, E714–E722. [Google Scholar] [CrossRef]
- Ellis, A.K.; Verma, S. Quality of Life in Women with Urinary Tract Infections: Is Benign Disease a Misnomer? J. Am. Board Fam. Pract. 2000, 13, 392–397. [Google Scholar] [CrossRef]
- Little, P.; Turner, S.; Rumsby, K.; Warner, G.; Moore, M.; Lowes, J.A.; Smith, H.; Hawke, C.; Mullee, M. Developing Clinical Rules to Predict Urinary Tract Infection in Primary Care Settings: Sensitivity and Specificity of near Patient Tests (Dipsticks) and Clinical Scores. Br. J. Gen. Pract. 2006, 56, 606–612. [Google Scholar]
- Giesen, L.G.M.; Cousins, G.; Dimitrov, B.D.; van de Laar, F.A.; Fahey, T. Predicting Acute Uncomplicated Urinary Tract Infection in Women: A Systematic Review of the Diagnostic Accuracy of Symptoms and Signs. BMC Fam. Pract. 2010, 11, 78. [Google Scholar] [CrossRef] [Green Version]
- Malterud, K.; Baerheim, A. Peeing Barbed Wire. Symptom Experiences in Women with Lower Urinary Tract Infection. Scand. J. Prim. Health Care 1999, 17, 49–53. [Google Scholar]
- Gágyor, I.; Rentzsch, K.; Strube-Plaschke, S.; Himmel, W. Psychometric Properties of a Self-Assessment Questionnaire Concerning Symptoms and Impairment in Urinary Tract Infections: The UTI-SIQ-8. BMJ Open 2021, 11, e043328. [Google Scholar] [CrossRef]
- Medina-Bombardó, D.; Jover-Palmer, A. Does Clinical Examination Aid in the Diagnosis of Urinary Tract Infections in Women? A Systematic Review and Meta-Analysis. BMC Fam. Pract. 2011, 12, 111. [Google Scholar] [CrossRef] [Green Version]
- Bent, S.; Nallamothu, B.; Simel, D. Does This Woman Have an Acute Uncomplicated Urinary Tract Infection? JAMA 2002, 287, 2701–2710. [Google Scholar] [CrossRef]
- Baerheim, A.; Digranes, A.; Malterud, K. Generalized Symptoms in Adult Women with Acute Uncomplicated Lower Urinary Tract Infection: An Observational Study. MedGenMed Medscape Gen. Med. 2003, 5, 1. [Google Scholar]
- Arinzon, Z.; Shabat, S.; Peisakh, A.; Berner, Y. Clinical Presentation of Urinary Tract Infection (UTI) Differs with Aging in Women. Arch. Gerontol. Geriatr. 2012, 55, 145–147. [Google Scholar] [CrossRef]
- Holm, A.; Siersma, V.; Cordoba, G.C. Diagnosis of Urinary Tract Infection Based on Symptoms: How Are Likelihood Ratios Affected by Age? A Diagnostic Accuracy Study. BMJ Open 2021, 11, e039871. [Google Scholar] [CrossRef]
- Bjerrum, L.; Lindbæk, M. Which Treatment Strategy for Women with Symptoms of Urinary Tract Infection? BMJ 2015, 351, h6888. [Google Scholar] [CrossRef] [Green Version]
- Sedgwick, P. Pitfalls of Statistical Hypothesis Testing: Type I and Type II Errors. BMJ 2014, 349, g4287. [Google Scholar] [CrossRef] [Green Version]
- Gameiro, C.M.; Romão, F.; Castelo-Branco, C. Menopause and Aging: Changes in the Immune System—A Review. Maturitas 2010, 67, 316–320. [Google Scholar] [CrossRef]
- Abraham, S.N.; Miao, Y. The Nature of Immune Responses to Urinary Tract Infections. Nat. Rev. Immunol. 2015, 15, 655–663. [Google Scholar] [CrossRef] [Green Version]
- Holm, A.; Cordoba, G.; Sørensen, T.M.; Jessen, L.R.; Siersma, V.; Bjerrum, L. Effect of Point-of-Care Susceptibility Testing in General Practice on Appropriate Prescription of Antibiotics for Patients with Uncomplicated Urinary Tract Infection: A Diagnostic Randomised Controlled Trial. BMJ Open 2017, 7, e018028. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Holm, A.; Cordoba, G.; Sørensen, T.M.; Jessen, L.R.; Siersma, V.; Bjerrum, L. Point of Care Susceptibility Testing in Primary Care—Does It Lead to a More Appropriate Prescription of Antibiotics in Patients with Uncomplicated Urinary Tract Infections? Protocol for a Randomized Controlled Trial. BMC Fam. Pract. 2015, 16, 106. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aspevall, O.; Hallander, H.; Gant, V.; Kouri, T. European Guidelines for Urinalysis: A Collaborative Document Produced by European Clinical Microbiologists and Clinical Chemists under ECLM in Collaboration with ESCMID. Clin. Microbiol. Infect. 2001, 7, 173–178. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Holm, A.; Cordoba, G.; Siersma, V.; Brodersen, J. Development and Validation of a Condition-Specific Diary to Measure Severity, Bothersomeness and Impact on Daily Activities for Patients with Acute Urinary Tract Infection in Primary Care. Health Qual. Life Outcomes 2017, 15, 57. [Google Scholar] [CrossRef] [Green Version]
- Sterne, J.A.C.; White, I.R.; Carlin, J.B.; Spratt, M.; Royston, P.; Kenward, M.G.; Wood, A.M.; Carpenter, J.R. Multiple Imputation for Missing Data in Epidemiological and Clinical Research: Potential and Pitfalls. BMJ 2009, 339, 157–160. [Google Scholar] [CrossRef]
- Benjamini, Y.; Hochberg, Y. Controlling the False Discovery Rate: A Practical and Powerful Approach to Multiple Testing. J. R. Stat. Soc. Ser. B 1995, 57, 289–300. [Google Scholar] [CrossRef]
- Beecher, C.; Duane, S.; Vellinga, A.; Murphy, A.W.; Cormican, M.; Smyth, A.; Healy, P.; Moore, M.; Little, P.; Geoghegan, C.; et al. COSUTI: A Core Outcome Set (COS) for Interventions for the Treatment of Uncomplicated Urinary Tract Infection (UTI) in Adults. Antibiotics 2022, 11, 1846. [Google Scholar] [CrossRef]


{kind=link}
| Premenopausal (n = 125) | Perimenopausal (n = 76) | Postmenopausal (n = 110) | p | |
|---|---|---|---|---|
| Pathogen (n missing = 18), n (%) | 0.0023 | |||
| No pathogen | 52 (44%) | 15 (20%) | 38 (37%) | |
| Primary pathogen | 60 (51%) | 52 (68%) | 52 (50%) | |
| Other uropathogen(s) | 5 (4%) | 7 (9%) | 14 (13%) | |
| Use of painkillers (n missing = 16) n (%) | 28 (24%) | 23 (31%) | 44 (41%) | 0.0245 |
| Days of symptoms before consultation (n missing = 11), median [QR1;QR3] | 3 [2;5] | 3 [1;4] | 3 [2;6] | 0.1043 |
| Number of previous UTI within past year (n missing = 13), median [QR1;QR3] | 0 [0;1] | 1 [0;2] | 1 [0;2] | 0.0422 |
| Social class (n missing = 122), n (%) | 0.0002 | |||
| 1 (highest) | 5 (7%) | 7 (14%) | 3 (4%) | |
| 2 | 24 (33%) | 15 (29%) | 24 (36%) | |
| 3 | 3 (4%) | 3 (6%) | 8 (12%) | |
| 4 | 14 (19%) | 15 (29%) | 29 (43%) | |
| 5 (lowest) | 27 (37%) | 11 (22%) | 3 (4%) | |
| Employment (n missing = 13), n (%) | <0.001 | |||
| Working | 68 (59%) | 64 (85%) | 21 (19%) | |
| During education | 37 (32%) | 1 (1%) | 0 | |
| Job seeking | 6 (5%) | 3 (4%) | 0 | |
| Early retirement pay, stay-at-home, etc. | 5 (4%) | 7 (9%) | 88 (81%) |
| Symptom | Premenopausal | Perimenopausal | Postmenopausal | Adjusted Difference between Postmenopausal and Premenopasal Women |
|---|---|---|---|---|
| DYSURIA Symptom dimension | 1.54 (1.48 to 1.61) | 1.47 (1.39 to 1.55) | 1.31 (1.24 to 1.38) | −0.30 (−0.51 to −0.08) * |
| Pain on urination | 1.76 (1.68 to 1.85) | 1.89 (1.79 to 1.99) | 1.40 (1.31 to 1.50) | −0.41 (−0.68 to −0.13) * |
| Difficulty to empty bladder | 1.32 (1.24 to 1.41) | 1.29 (1.18 to 1.41) | 1.27 (1.18 to 1.37) | −0.14 (−0.45 to 0.16) |
| Uncomfortable pressure around the bladder | 1.55 (1.46 to 1.64) | 1.24 (1.13 to 1.35) | 1.26 (1.17 to 1.35) | −0.34 (−0.63 to −0.04) * |
| FREQUENCY Symptom dimension | 1.69 (1.62 to 1.77) | 1.77 (1.69 to 1.86) | 1.85 (1.78 to 1.92) | 0.12 (−0.11 to 0.35) |
| Frequent urination–daytime | 2.09 (2.00 to 2.17) | 2.22 (2.12 to 2.32) | 2.06 (1.99 to 2.14) | −0.08 (−0.34 to 0.19) |
| Increased urge for urination | 2.15 (2.07 to 2.23) | 2.29 (2.20 to 2.39) | 2.12 (2.04 to 2.20) | −0.07 (−0.31 to 0.18) |
| Has to hurry to the toilet | 1.57 (1.48 to 1.67) | 1.59 (1.47 to 1.71) | 1.80 (1.70 to 1.90) | 0.21 (−0.10 to 0.51) |
| Incontinence | 0.97 (0.88 to 1.06) | 1 (0.89 to 1.11) | 1.42 (1.32 to 1.51) | 0.41 (0.11 to 0.71) * |
| LOWER BACK Symptom dimension | 0.54 (0.47 to 0.61) | 0.60 (0.51 to 0.68) | 0.54 (0.46 to 0.61) | −0.06 (−0.29 to 0.17) |
| Pain in lower back | 0.61 (0.54 to 0.68) | 0.64 (0.55 to 0.74) | 0.62 (0.54 to 0.70) | −0.05 (−0.3 to 0.20) |
| Uncomfortable pressure in lower back | 0.47 (0.40 to 0.54) | 0.55 (0.46 to 0.64) | 0.46 (0.38 to 0.53) | −0.08 (−0.31 to 0.16) |
| GENERAL Symptom dimension | 0.85 (0.80 to 0.90) | 0.88 (0.79 to 0.97) | 0.66 (0.60 to 0.72) | −0.26 (−0.45 to −0.06) * |
| Feeling unwell | 1.58 (1.49 to 1.66) | 1.35 (1.25 to 1.46) | 1.10 (1.00 to 1.19) | −0.59 (−0.88 to −0.31) *, ** |
| Fever | 0.48 (0.42 to 0.54) | 0.66 (0.56 to 0.76) | 0.46 (0.39 to 0.52) | −0.06 (−0.28 to 0.16) |
| Shivering | 0.50 (0.43 to 0.56) | 0.63 (0.53 to 0.72) | 0.41 (0.34 to 0.48) | −0.12 (−0.35 to 0.11) |
| Single symptoms | ||||
| Burning | 1.67 (1.58 to 1.76) | 1.67 (1.56 to 1.78) | 1.56 (1.47 to 1.66) | −0.20 (−0.50 to 0.11) |
| Smell | 1.24 (1.15 to 1.33) | 1.22 (1.10 to 1.34) | 1.09 (0.99 to 1.19) | −0.22 (−0.56 to 0.11) |
| Appearance | 1.01 (0.93 to 1.08) | 1.19 (1.08 to 1.31) | 1.09 (1.01 to 1.18) | 0.04 (−0.26 to 0.34) |
| Blood | 0.45 (0.38 to 0.51) | 0.53 (0.44 to 0.62) | 0.18 (0.13 to 0.23) | −0.28 (−0.53 to −0.03) * |
| Frequent urination–nighttime | 1.22 (1.13 to 1.31) | 1.25 (1.14 to 1.37) | 1.55 (1.45 to 1.64) | 0.27 (−0.04 to 0.58) |
| Pain around bladder | 1.53 (1.44 to 1.61) | 1.22 (1.12 to 1.33) | 1.2 (1.11 to 1.28) | −0.40 (−0.68 to −0.12) * |
| Symptom | Premenopausal | Perimenopausal | Postmenopausal | Adjusted Difference between Postmenopausal and Premenopasal Women |
|---|---|---|---|---|
| DYSURIA Symptom dimension | 1.64 (1.57 to 1.71) | 1.46 (1.38 to 1.55) | 1.32 (1.25 to 1.39) | −0.38 (−0.61 to −0.15) *, ** |
| Pain on urination | 1.91 (1.81 to 2.00) | 1.94 (1.84 to 2.05) | 1.41 (1.31 to 1.51) | −0.54 (−0.83 to −0.25) *, ** |
| Difficult to empty bladder | 1.48 (1.38 to 1.58) | 1.23 (1.11 to 1.35) | 1.29 (1.19 to 1.39) | −0.28 (−0.61 to 0.04) |
| Uncomfortable pressure around the bladder | 1.53 (1.43 to 1.62) | 1.22 (1.11 to 1.34) | 1.26 (1.17 to 1.35) | −0.32 (−0.62 to −0.01) * |
| FREQUENCY Symptom dimension | 1.68 (1.60 to 1.75) | 1.64 (1.54 to 1.74) | 1.81 (1.73 to 1.89) | 0.09 (−0.16 to 0.34) |
| Frequent urination–daytime | 1.95 (1.87 to 2.04) | 1.84 (1.72 to 1.96) | 1.94 (1.85 to 2.04) | −0.07 (−0.36 to 0.23) |
| Increased urge for urination | 2.05 (1.97 to 2.14) | 2.06 (1.95 to 2.17) | 2.06 (1.98 to 2.15) | −0.03 (−0.31 to 0.25) |
| Has to hurry to the toilet | 1.59 (1.49 to 1.69) | 1.54 (1.42 to 1.66) | 1.79 (1.69 to 1.89) | 0.17 (−0.14 to 0.49) |
| Incontinence | 1.12 (1.02 to 1.22) | 1.13 (1.00 to 1.25) | 1.46 (1.35 to 1.56) | 0.29 (−0.04 to 0.62) |
| LOWER BACK Symptom dimension | 0.54 (0.47 to 0.61) | 0.59 (0.50 to 0.67) | 0.51 (0.43 to 0.58) | −0.10 (−0.33 to 0.14) |
| Pain in lower back | 0.60 (0.53 to 0.67) | 0.63 (0.54 to 0.72) | 0.58 (0.50 to 0.67) | −0.07 (−0.32 to 0.17) |
| Uncomfortable pressure in lower back | 0.48 (0.41 to 0.55) | 0.54 (0.45 to 0.63) | 0.43 (0.36 to 0.50) | −0.12 (−0.36 to 0.12) |
| GENERAL Symptom dimension | 0.84 (0.78 to 0.89) | 0.90 (0.81 to 0.99) | 0.65 (0.59 to 0.71) | −0.26 (−0.46 to −0.06) * |
| Feeling unwell | 1.59 (1.50 to 1.69) | 1.46 (1.34 to 1.58) | 1.11 (1.01 to 1.21) | −0.62 (−0.92 to −0.32) *, ** |
| Fever | 0.45 (0.38 to 0.51) | 0.65 (0.55 to 0.75) | 0.44 (0.37 to 0.51) | −0.05 (−0.28 to 0.17) |
| Shivering | 0.47 (0.40 to 0.54) | 0.60 (0.50 to 0.70) | 0.4 (0.33 to 0.47) | −0.11 (−0.35 to 0.13) |
| Single symptoms | ||||
| Burning | 1.74 (1.64 to 1.83) | 1.72 (1.61 to 1.84) | 1.56 (1.47 to 1.66) | −0.26 (−0.57 to 0.04) |
| Smell | 0.97 (0.88 to 1.07) | 1.02 (0.90 to 1.14) | 0.93 (0.83 to 1.03) | −0.08 (−0.41 to 0.25) |
| Appearance | 0.66 (0.59 to 0.73) | 0.88 (0.77 to 0.98) | 0.88 (0.79 to 0.97) | 0.18 (−0.14 to 0.51) |
| Blood | 0.38 (0.31 to 0.45) | 0.50 (0.40 to 0.59) | 0.19 (0.13 to 0.24) | −0.19 (−0.47 to 0.09) |
| Frequent urination–nighttime | 1.31 (1.21 to 1.40) | 1.30 (1.18 to 1.43) | 1.57 (1.47 to 1.68) | 0.18 (−0.16 to 0.51) |
| Pain around bladder | 1.55 (1.46 to 1.64) | 1.22 (1.11 to 1.33) | 1.20 (1.11 to 1.29) | −0.41 (−0.71 to −0.11) * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Teglbrænder-Bjergkvist, S.; Siersma, V.; Holm, A. Severity and Bothersomeness of Urinary Tract Infection Symptoms in Women before and after Menopause. Antibiotics 2023, 12, 1148. https://doi.org/10.3390/antibiotics12071148
Teglbrænder-Bjergkvist S, Siersma V, Holm A. Severity and Bothersomeness of Urinary Tract Infection Symptoms in Women before and after Menopause. Antibiotics. 2023; 12(7):1148. https://doi.org/10.3390/antibiotics12071148
Chicago/Turabian StyleTeglbrænder-Bjergkvist, Signe, Volkert Siersma, and Anne Holm. 2023. "Severity and Bothersomeness of Urinary Tract Infection Symptoms in Women before and after Menopause" Antibiotics 12, no. 7: 1148. https://doi.org/10.3390/antibiotics12071148