1. Introduction
Bone and joint infections are infectious diseases that can arise due to the haematogenous spread of systemic bacteraemia, contiguous spread from adjoining tissue or direct trauma caused by surgery or injury [
1,
2,
3,
4]. The most common chronic bone and joint infections include osteomyelitis, infectious/septic arthritis and implant/prosthetic-related infections [
5]. These infections pose a serious risk of morbidity, and can result in chronic pain, wounds with discharge, sepsis and even permanent disability [
6]. Currently in Africa, there is limited knowledge regarding the prevalence of bone and joint infections amongst adults. However, a reported incidence of 43–200 cases per 100,000 children from low-income countries appreciably contrasts with 1.94–13 cases per 100,000 from high-income countries, potentially reflecting a higher incidence of chronic infections in Sub-Saharan Africa [
7]. The incidence of bone and joint infections is higher in developing countries due to principally inadequate treatment, health service inaccessibility and poverty, both in seeking care as well as paying for treatment [
8].
The most common causative pathogens of bone and joint infections are
Staphylococcus aureus (
S. aureus) (the most prevalent single pathogen in bone and joint infections),
coagulase –negative staphylococci and
Staphylococcus epidermidis [
2,
4,
5]. Gram-negative bacilli, anaerobes and fungi, have been noted as other causative organisms [
4]. Chronic bone and joint infections can also arise due to surgically implanted devices when bacteria adhere to the implant’s surface or a biofilm is formed at the implantation site [
9]. To treat these infections, long-term antibiotic treatment at high doses combined with surgery and removal of the implant is necessary [
10].
The selection of an antibiotic to effectively eradicate the infection depends on a number of factors. These include antibiotic susceptibility, documented bone and joint tissue penetration, oral bioavailability and cost [
5]. In South Africa, the Standard Treatment Guidelines/Essential Medicine List (STG/EML) currently recommends empiric antibiotic therapy for osteomyelitis and septic arthritis directed against
S. aureus [
11]. As a result, rflucloxacillin and cloxacillin are recommended as the mainstay of antibiotic therapy [
11], with similar recommendations in the recent WHO AWaRE antibiotics guidance [
12]. A summary of treatment for these patients according to the current STG is shown in
Table 1.
However, biofilm formation is also a critical aspect to consider when treating bone and joint infections [
13]. A biofilm is a multi-structural, diverse community of immobile microorganisms enclosed by an extracellular matrix polysaccharide, which usually develops on non-living surfaces, including sequestrum (dead bone) and implants [
13,
14]. Biofilms encapsulate groups of organisms that are resistant to antimicrobial agents; consequently, making infections difficult to treat, potentially requiring antibiotics outside of current STG/EML guidelines.
Considering the long duration of therapy necessary to treat bone and joint infections, patient adherence is another key aspect of successful therapy alongside pertinent antibiotic selection [
15]. Adherence to medication is a well-acknowledged challenge in the pharmacotherapeutic management of patients with chronic conditions [
16]. To successfully eradicate the infection with antibiotics, patients must adhere to all instructions and follow the exact treatment plan given by healthcare professionals [
17]. However, not fully understanding instructions from the prescriber and/or pharmacist could lead to non-adherence, especially since there is a high pill burden in patients with chronic bone and joint infections. Consequently, the necessity of educating the patients on their condition and explaining instructions clearly is crucial [
18]. Limited knowledge in patients about their condition and medication can result in poor clinical outcomes and, in this case, potentially increase antimicrobial resistance (AMR) [
19]. A study by Saqib et al. (2019) reported that insufficient knowledge of prescribed medicines in patients resulted in their incorrect use, which may lead to treatment failure posing a risk to the health of patients [
20]. In addition, insufficient knowledge amongst patients about their condition has been shown to negatively impact on interventions aimed at successfully managing their condition [
21]. Patient education and clinical pharmacist consultation for chronic disease co-management has been shown to successfully improve medication adherence [
22].
The use of STGs in infectious diseases enhances the appropriate use of antibiotics, which is a key concern in Africa [
10,
23,
24]. STGs provide evidence-based treatment recommendations that standardise treatment approaches [
10]. Consequently, they are a key part of antimicrobial stewardship programmes (ASPs) to improve the future use of antibiotics [
25,
26,
27]. Part of ASPs is to ensure compliance with local guidelines, which is the responsibility of all healthcare providers [
28]. In this respect, hospital pharmacists can play a crucial role by providing ASP interventions including antibiotic prescription reviews, dose and duration optimisation, as well as the education of patients and other healthcare providers [
28,
29].
In view of concerns with rising rates of AMR across Africa, as well as concerns with adherence to guidelines amongst hospitals across Africa [
27,
30], including hospitals in South Africa, we wished to provide antimicrobial stewardship (AMS) services to the orthopaedic clinic at a tertiary hospital for outpatients diagnosed with chronic bone and joint infections to improve their care. This included the need to evaluate the use of antibiotics in comparison with the current South African STG, assessing patients’ knowledge of their medication and condition, the importance of adherence as well as potentially educating them on their medical condition and antibiotics where necessary. The findings can subsequently be used to update local guidelines if needed, as well as provide guidance to all key stakeholder groups on the potential role and value of pharmacists conducting AMS activities in an outpatient setting to improve patient outcomes.
3. Discussion
To the best of our knowledge, this is the first study undertaken in a tertiary institution in South Africa that looked at undertaking and evaluating an ASP at an outpatient clinic focusing on bone and joint infections. The most common infection in our study was osteomyelitis. The majority of the patients in our study were males (86%), even when broken down into the diagnosis (chronic osteomyelitis and septic arthritis), the incidence was still higher in males than females; 34:5 and 3:2, respectively. These findings correlate with other studies that observed the incidence of both diagnoses amongst males and females; for chronic osteomyelitis, a ratio of 4:1 was observed and septic arthritis a ratio of 77:47 was observed [
31,
32]. This could be due to the fact that there is an increase of bone and joint infections due to trauma including traffic accidents and sport injuries in our population, which is more predominant in males as they engage in more risky behaviour [
33]. Similarly, a recent study for skin and soft tissue infections in South Africa showed males being more affected [
34].
The majority of patients in our study presented with HIV, hypertension, diabetes and as IV drug users for comorbidities. This mirrors recently published studies in a similar setting in South Africa [
34]. This is also similar to the findings of Romano et al. (2011), who reported an increased prevalence of bone and joint infections in immunocompromised individuals, as well as those with certain lifestyle habits, including intravenous drug use [
35]. South Africa has been reported to have a high prevalence of co-infection of HIV and tuberculosis by the WHO [
36], coupled with an increasing prevalence of diabetes and hypertension [
37,
38]. Consequently, patients with bone and joint infections need to be carefully managed to improve their outcomes.
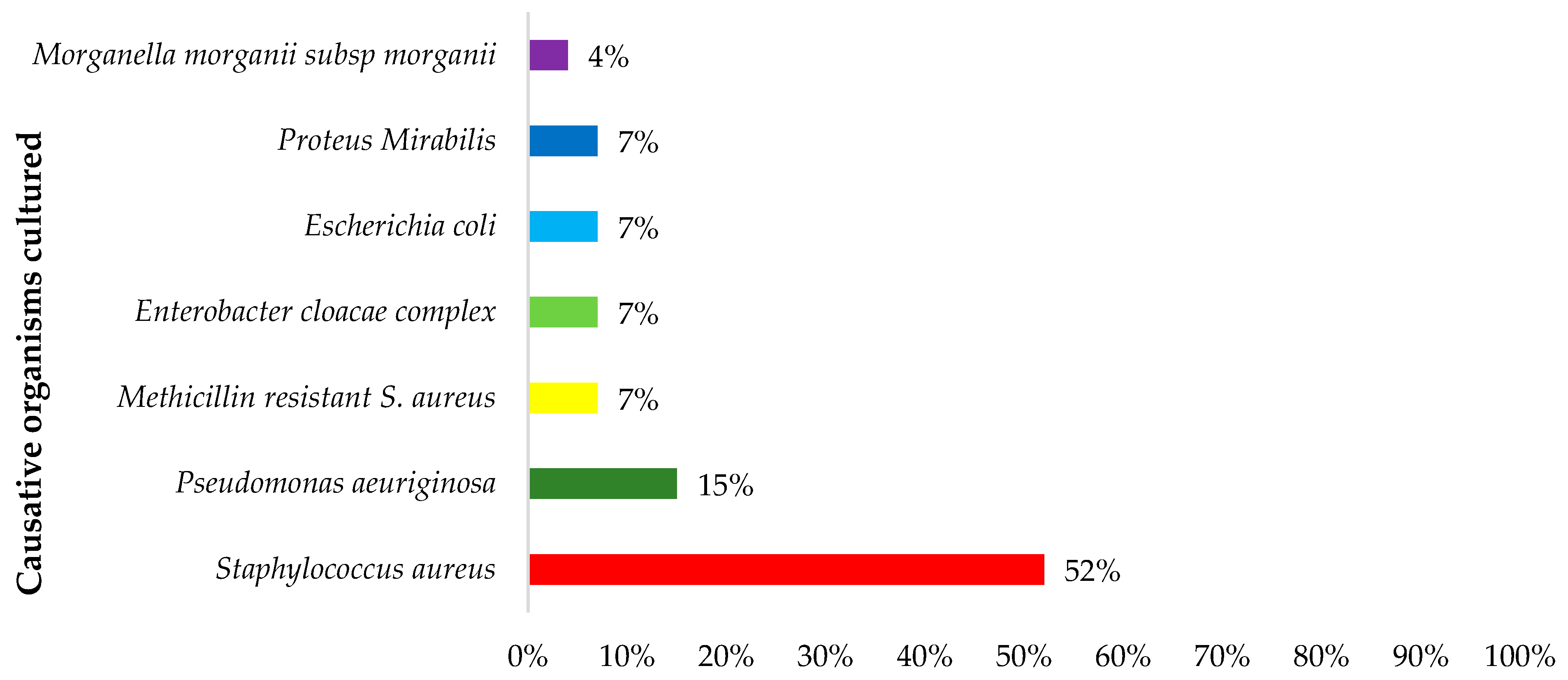
Microbiological cultures play a crucial role in confirming infections and guiding subsequent antimicrobial treatment. The most prevalent bacterial pathogen in our study was
S. aureus (43%) followed by
P. aeruginosa (14%). These findings are similar to those reported in other studies [
1,
5,
39]. However, a recent study by Masters et al. (2022) reported that whilst
S. aureus was the most common organism identified in these patients,
Pseudomonas was one of the least common organisms [
2]. These differences could be due to geographical differences, as well as different prevalence rates in the community and hospital setting. We will be following this up in future studies.
A concern was that rifampicin and ciprofloxacin were amongst the most prescribed antibiotics singly and in combination in our study, with flucloxacillin the third most prescribed with the beta-lactams having proven activity against Gram-positive microorganisms, particularly
S. aureus, which was the most cultured in our study. Whilst this combination is not currently documented in the South African STG (
Table 1), this combination has been shown to be effective in published studies, especially in patients with suspected biofilm formation [
5,
40,
41]. Studies documented a clinical cure rate of up to 100% when this combination was used for 3–6 months [
5,
40,
41]. The current South African STG only gives empiric therapy directed at
S. aureus and not other organisms or biofilm formations (
Table 1) [
11]. This needs to be addressed, especially with rifampicin being the cornerstone of treatment against biofilm
S. aureus musculoskeletal infections [
10]. However, whilst its effectiveness has been proven across studies [
13], care is required in the South African setting as overexposure may lead to resistance [
42]; and in a recent study in South Africa, rifampicin was amongst the top five antibiotics prescribed for skin and soft tissue infections [
34]. This is a concern as rifampicin is currently used as one of the first-line antimicrobials in the treatment of tuberculosis in South Africa, which has a high burden of drug-resistant tuberculosis (DR-TB) [
43]. The efficacy of the floroquinolones has also been proven in bone and joint infections [
5,
34,
35]. However, in South Africa, ciprofloxacin is not used in the treatment of tuberculosis because of its weak efficacy compared to other fluoroquinolones [
44,
45,
46]. This helps explain why adherence to the current South African STG was very low compared to recent point prevalence surveys (PPS) conducted amongst public hospitals in South Africa. In these two PPS studies, compliance with the South African STG was 93.4% and 90.2% of all the prescriptions reviewed [
47,
48]. The compliance rate in our study was also appreciably lower than the rate of 55.2% compliance to the South African STGs to treat patients with skin and soft tissue infections in a recent study [
34] along with other published studies across Africa [
49,
50]. Rifampicin was also given in combination with flucloxacillin in our study. Using this combination in bone and joint infections, Frippiat et al. (2004) found that at the end of the study all (100%) patients achieved complete infectious remission with a minimum follow-up period of 12 months [
40]. This is encouraging.
However, any guidelines produced need to take account of possible shortages of medicines in the public sector necessitating changes to current recommendations. For instance, due to the routine unavailability of oral cloxacillin in the South African public sector, which is dependent on tender supply, flucloxacillin is recommended as the antibiotic of choice where necessary [
51]. There is, though, a higher risk of treatment failure with flucloxacillin as high doses are needed for bone penetration in patients with bone and joint infections. After pharmacist interventions, there was improved prescribing of flucloxacillin instead of cloxacillin in our study, which is also encouraging. Similarly, the dispensing of the correct dosage of flucloxacillin was increasingly observed. This shows the importance of involving hospital pharmacists in ASPs as they can help in identifying dosage errors and instigate necessary changes [
29,
52].
Of equal concern is that both rifampicin and ciprofloxacin are antibiotics in the ‘Watch’ group, and it is essential to ensure their rational use to limit AMR in South Africa, which is a growing problem [
53]. We have seen variable use of ‘Watch’ antibiotics amongst hospitals in South Africa depending on their location, as well as specific wards [
47,
48]. This needs to be monitored as antibiotics in the ‘Watch’ group have a higher toxicity and resistance potential [
54]. Consequently, appropriate doses and combinations of antibiotics in patients with bone and joint infections must be carefully considered before their use taking into consideration comorbidities including HIV in this population, as well as recommendations in the recently published internationally accepted WHO AWaRe Book [
12]. We will be monitoring this in future studies.
Initially in our study, suboptimal dosages of rifampicin were being prescribed including 150 mg po daily. This contradicts published studies which recommend 600 mg once daily in patients with bone and joint infections [
10]. Following successful pharmacist interventions, rifampicin was correctly prescribed at 300 mg twice daily in these patients. This is also in line with other successful ASP interventions undertaken by hospital pharmacists across Africa [
29].
Due to the unavailability of oral cloxacillin in South African public sector facilities dependent on tender supply, flucloxacillin is the recommended drug of choice for therapeutic interchange [
51]. Flucloxacillin has been proven to achieve higher serum concentrations levels, double that of cloxacillin [
55]. As a result of this pharmacokinetic knowledge, for all prescriptions in which cloxacillin was initially prescribed, flucloxacillin was subsequently dispensed with half the dose. This, though, carries a high risk of treatment failure as high doses are needed for bone penetration in bone and joint infections. After pharmacists’ intervention, there was an improved prescribing of flucloxacillin instead of cloxacillin and, similarly, the dispensing of the correct dosage of flucloxacillin was observed. This further shows the importance of the involvement of a pharmacist in AMS initiatives to help in identifying dosage errors and necessary drug changes [
28,
29].
According to the ARMS scale, the majority (n = 39; 89%) of the patients had a score of less than 23 points; and, consequently, are considered as having high-adherence, which is encouraging. These findings were similar to a study by Zidan et al. (2018)
, in which the ARMS overall score was 17.4 amongst 307 patients with diabetes [
56]. However, we are aware of the reduced patient numbers attending follow-up visits in our study, which may impact on our findings. We will be following this up in future studies since it is important that patients regularly return to the orthopaedic clinic to appropriately treat these chronic bone and joint infections.
At baseline, 57% and 55% of patients indicated not knowing the name of their condition or the purpose of their medication, respectively. With chronic osteomyelitis being the most diagnosed condition, only 2% of the patients knew this at baseline. However, encouragingly by Follow up 1 and 2, their knowledge had appreciably improved alongside knowledge of the condition for purposes of their medication. This indicated an improvement in patients’ knowledge on their condition and the purpose for their medication following pharmacists’ interventions. The importance of patient education was further emphasized in this study, which is similar to other studies [
57,
58,
59].
Outpatient settings will continue to be an important target for AMS interventions [
60], and this study has shown possible areas where a pharmacist can play a role. This includes appropriate drug changes and dosing, education of patients and being involved in the overall management of bone and joint infections along with other healthcare professionals (HCPs). It is evident that the initiation of an ASP in this hospital has increased compliance to recommended antibiotics and assisted in reducing inappropriate dosing, similar to other studies [
26,
27]. The clear need for a pharmacist in bone and joint infections is evident not only in the education of the patients but also of other HCPs involved, as pharmacists play an important role in driving forward ASPs in Africa and globally [
28]. Future studies, though, are needed to ensure this service continues and is sustainable to increase better patient outcomes in this important population group, building on the findings of this initial study.
We are aware of a number of limitations in this study. Firstly, this study was only conducted in one tertiary institution focusing on the outpatient population. However, we chose this hospital for this initial study as it is one of the largest tertiary hospitals in South Africa with a designated orthopaedic outpatient clinic. Secondly, the study was performed over only a three-month period using convenience sampling, giving a small sample size. This was a challenge considering that at follow-up visits, not all patients returned, reducing the sample size even further. Thirdly, we are unaware of studies that used the ARMs scale in patients with bone and joint infections. However as stated, this is a validated and reliable tool commonly used in chronic diseases. In addition, the number of patients assessed at follow-up dropped during the study, which may have impacted on our findings. The researchers were only made aware of the different treatment durations during data collection, which made it challenging to investigate this phenomenon as it was not in the original research proposal. This will be looking at this key area in future studies. Lastly, convenience sampling was used, introducing sampling bias as we only included patients who were available and willing to participate in the study. Despite these limitations, we believe our findings are robust providing direction for the future. This includes a key role for hospital pharmacists progressing ASP activities in this key group of patients.


 ,
, 


{kind=link}