
Treatment of Periodontal Infections, the Possible Role of Hydrogels as Antibiotic Drug-Delivery Systems

 ,
,  ,
,
Abstract
:1. Introduction
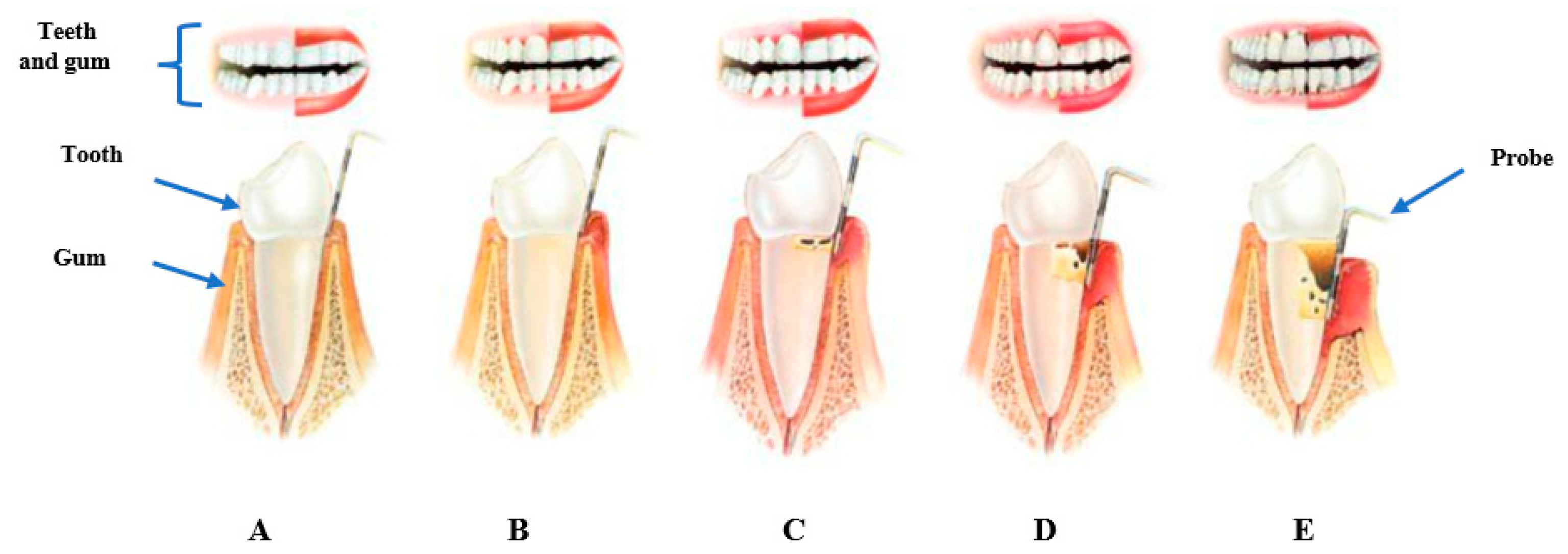
2. Role of Bacteria in the Prognosis of Periodontal Disease
3. Treatment Options Available for Treating Bacterial Infections in Periodontal Disease
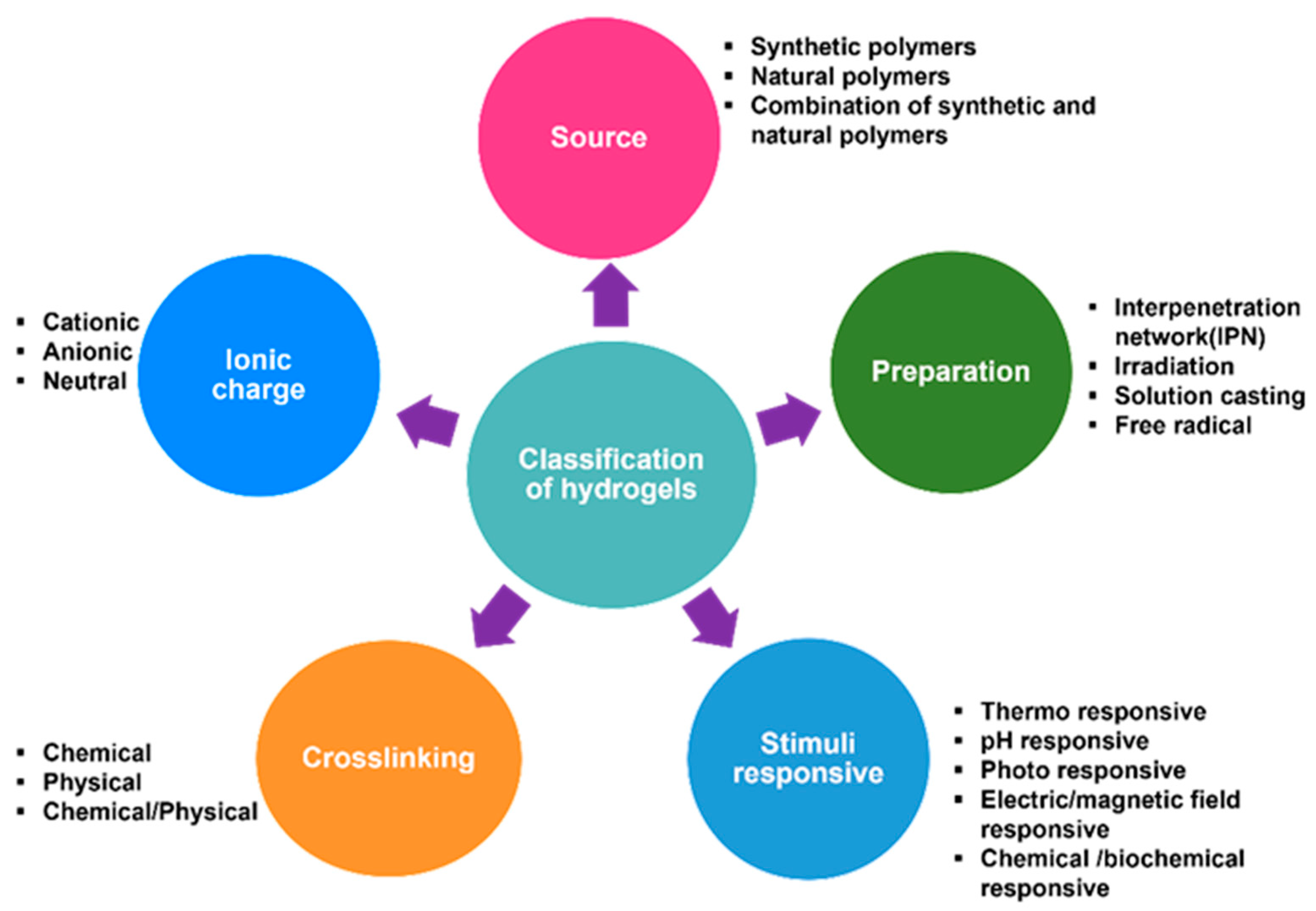
4. Hydrogel Formulations


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Type of Smart Hydrogel | Hydrogel Materials | Antibacterial Agent | Antibacterial Activity | References |
|---|---|---|---|---|
| Thermo-responsive hydrogel | N-isopropylacrylamide (NIPAM), silane-coupled with graphene (GM), vinyl carboxymethyl chitosan (CG); NIPAM-CG/GM loaded with ciprofloxacin | Ciprofloxacin | Antibacterial activity against E. coli (ZOI 18.10 mm–20.16 mm ± SD) and S. aureus (ZOI 18.06 mm–20.62 mm ± SD) | [99] |
| Thermo-responsive hydrogel | β-glycerolphosphate disodium salt pentahydrate (β-Gp), chitosan, and gelatin | Metronidazole | Antibacterial activity of hydrogel–metronidazole formulation with MIC of 40 µg/mL for Clostridium sporogenes. | [112] |
| Reactive oxygen species (ROS) responsive hydrogel | PVA and N1-(4-boronobenzyl)-N3-(4-boronophenyl)-N1, N1,N3,N3-tetramethylpropane-1,3-diaminium | Macrophages (derived from bone marrow) and C5aR antagonist | Blockage of C5aR, a target site controlled by periodontal bacteria Pg (Porphyromonas gingivalis) | [113] |
| Thermo-responsive hydrogel | Chitosan, glycerophosphate salt | Chitosan | Incorporation of atorvastatin and lovastatin reduced Porphyromonas gingivalis-induced inflammation | [114] |
| Hybrid hydrogel | β-cyclodextrin, ciprofloxacin, polydioxanone, | Ciprofloxacin | Increased antimicrobial activity of drug-loaded hydrogel against endodontic pathogen (Enterococcus faecalis) compared to 0.12% chlorhexidine | [115] |
| Thermo-responsive hydrogel | Pluronic F127, silk fibrin, and methyl cellulose, | Metronidazole | A 200-fold of reported MIC (0.063–0.514 µg/mL) of metronidazole for Porphyromonas gingivalis was released from all formulations | [88] |
| pH-sensitive hydrogel | Chitosan, sodium alginate, polyethylene glycol, 1,4 diaminobutane | Sodium ceftriaxone | Antimicrobial activity with ZOI of 10.2 mm and 9.7 mm for test organisms S.aureus and E.coli respectively | [93] |
| Photo-sensitive | Methacrylic gelatin, Methacrylic polyphosphoester | Zeolitic imidazolate framework | Bacteria (Porphyromonas gingivalis and Streptococcus mutans) biofilm destruction by hydrogels. | [116] |
| Near-infrared (NIR) light-sensitive hydrogel | Gold nanobipyramids, gelatin methacrylate, mesoporous silica | Minocycline | A 90% antibacterial efficacy against Porphyromonas gingivalis | [100] |
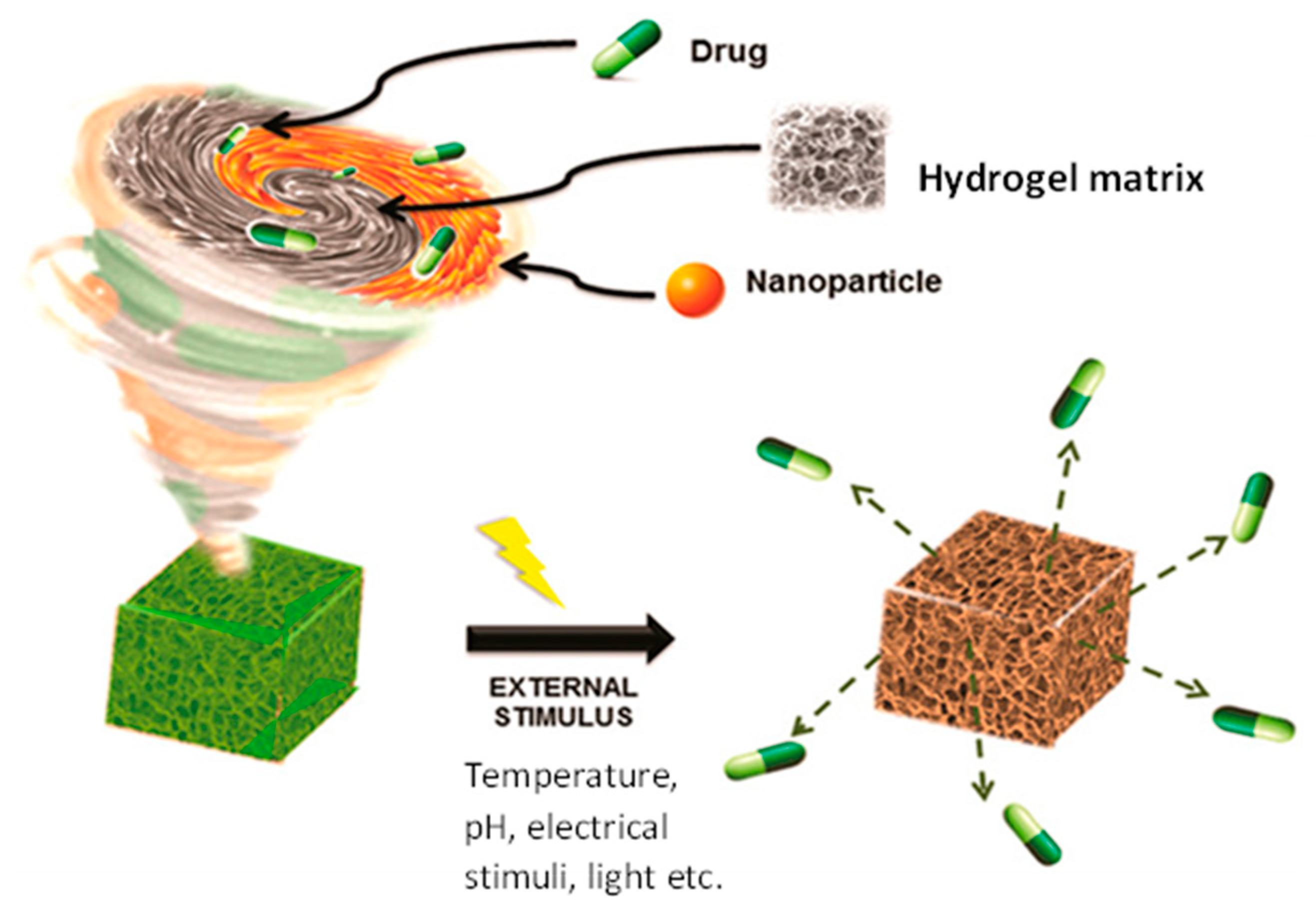
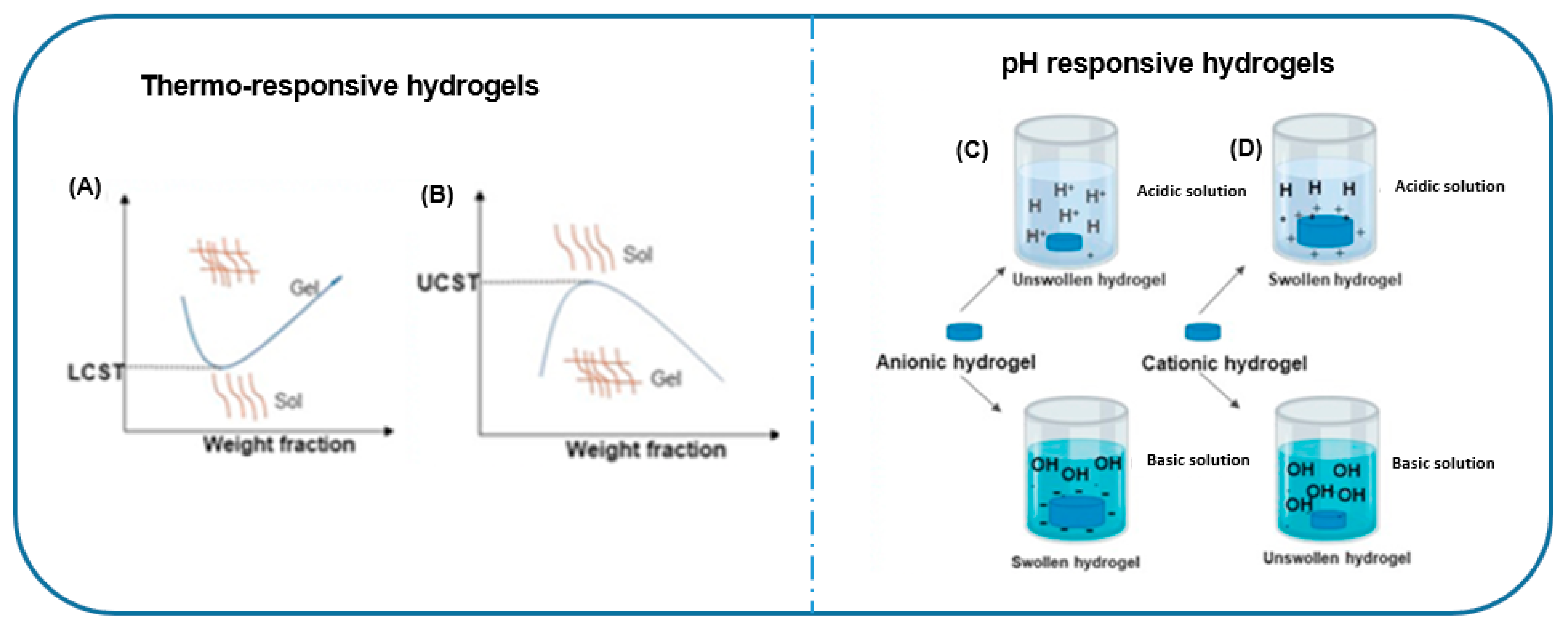
4.1. Release Mechanism of Antibiotics by Hydrogels
4.2. Feasibility of Incorporating Antibiotics into Hydrogels
5. Potential Roadblocks
6. Limitations of this Review
7. Future Directions
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dietrich, T.; Ower, P.; Tank, M.; West, N.X.; Walter, C.; Needleman, I.; Hughes, F.J.; Wadia, R.; Milward, M.R.; Hodge, P.J.; et al. Periodontal diagnosis in the context of the 2017 classification system of periodontal diseases and conditions–implementation in clinical practice. Br. Dent. J. 2019, 226, 16–22. [Google Scholar] [CrossRef] [Green Version]
- Ndjidda Bakari, W.; Thiam, D.; Mbow, N.L.; Samb, A.; Guirassy, M.L.; Diallo, A.M.; Diouf, A.; Diallo, A.S.; Benoist, H.M. New classification of periodontal diseases (NCPD): An application in a sub-Saharan country. BDJ Open 2021, 7, 16. [Google Scholar] [CrossRef]
- Global Burden of Disease Collaborative Network. Global Burden of Disease Study 2019 (GBD 2019). Available online: http://ghdx.healthdata.org/gbd-results-tool (accessed on 7 April 2023).
- Wu, L.; Zhang, S.Q.; Zhao, L.; Ren, Z.H.; Hu, C.Y. Global, regional, and national burden of periodontitis from 1990 to 2019: Results from the Global Burden of Disease study 2019. J. Periodontol. 2022, 93, 1445–1454. [Google Scholar] [CrossRef] [PubMed]
- Sedghi, L.M.; Bacino, M.; Kapila, Y.L. Periodontal disease: The good, the bad, and the unknown. Front. Cell. Infect. Microbiol. 2021, 11, 1210. [Google Scholar] [CrossRef] [PubMed]
- Dental, S. Prevention and Treatment of Periodontal Diseases in Primary Care Dental Clinical Guidance; Scottish Dental Clinical Effectiveness Programme; Dundee Dental Educational Centre, Frankland Building: Dundee, UK, 2014. [Google Scholar]
- Qare, E. Periodontal Gum Disease. Available online: https://www.dreliasqare.com/periodontal-gum-disease (accessed on 7 April 2023).
- Beck, J.D.; Philips, K.; Moss, K.; Sen, S.; Morelli, T.; Preisser, J.; Pankow, J. Periodontal disease classifications and incident coronary heart disease in the Atherosclerosis Risk in Communities study. J. Periodontol. 2020, 91, 1409–1418. [Google Scholar] [CrossRef]
- Larvin, H.; Gao, C.; Kang, J.; Aggarwal, V.R.; Pavitt, S.; Wu, J. The impact of study factors in the association of periodontal disease and cognitive disorders: Systematic review and meta-analysis. Age Ageing 2023, 52, afad015. [Google Scholar] [CrossRef] [PubMed]
- Liccardo, D.; Cannavo, A.; Spagnuolo, G.; Ferrara, N.; Cittadini, A.; Rengo, C.; Rengo, G. Periodontal disease: A risk factor for diabetes and cardiovascular disease. Int. J. Mol. Sci. 2019, 20, 1414. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zardawi, F.; Gul, S.; Abdulkareem, A.; Sha, A.; Yates, J. Association between periodontal disease and atherosclerotic cardiovascular diseases: Revisited. Front. Cardiovasc. Med. 2021, 7, 625579. [Google Scholar] [CrossRef]
- Drug Prescribing for Dentistry, Dental Clinical Guidance. 2016. Available online: https://www.sdcep.org.uk/published-guidance/ (accessed on 7 April 2023).
- Sethulekshmi, A.; Saritha, A.; Joseph, K.; Aprem, A.S.; Sisupal, S.B. MoS2 based nanomaterials: Advanced antibacterial agents for future. J. Control. Release 2022, 348, 158–185. [Google Scholar] [CrossRef] [PubMed]
- Mokhtar, A.; Djelad, A.; Bengueddach, A.; Sassi, M. CuNPs-magadiite/chitosan nanocomposite beads as advanced antibacterial agent: Synthetic path and characterization. Int. J. Biol. Macromol. 2018, 118, 2149–2155. [Google Scholar] [CrossRef]
- Suflet, D.M.; Popescu, I.; Pelin, I.M.; Ichim, D.L.; Daraba, O.M.; Constantin, M.; Fundueanu, G. Dual cross-linked chitosan/pva hydrogels containing silver nanoparticles with antimicrobial properties. Pharmaceutics 2021, 13, 1461. [Google Scholar] [CrossRef]
- Namivandi-Zangeneh, R.; Wong, E.H.; Boyer, C. Synthetic antimicrobial polymers in combination therapy: Tackling antibiotic resistance. ACS Infect. Dis. 2021, 7, 215–253. [Google Scholar] [CrossRef] [PubMed]
- Parkin, H.C.; Garcia-Hernandez, J.D.; Street, S.T.; Hof, R.; Manners, I. Uniform, length-tunable antibacterial 1D diblock copolymer nanofibers. Polym. Chem. 2022, 13, 2941–2949. [Google Scholar] [CrossRef]
- Jung, K.; Corrigan, N.; Wong, E.H.; Boyer, C. Bioactive synthetic polymers. Adv. Mater. 2022, 34, 2105063. [Google Scholar] [CrossRef]
- Liu, Y.; Li, X.; Liang, A. Current research progress of local drug delivery systems based on biodegradable polymers in treating chronic osteomyelitis. Front. Bioeng. Biotechnol. 2022, 10, 2215. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Wang, F.; Liu, Q.; Du, J. Antibacterial polymeric nanostructures for biomedical applications. Chem. Commun. 2014, 50, 14482–14493. [Google Scholar] [CrossRef]
- Yang, K.; Han, Q.; Chen, B.; Zheng, Y.; Zhang, K.; Li, Q.; Wang, J. Antimicrobial hydrogels: Promising materials for medical application. Int. J. Nanomed. 2018, 13, 2217. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, S.; Dong, S.; Xu, W.; Tu, S.; Yan, L.; Zhao, C.; Ding, J.; Chen, X. Antibacterial hydrogels. Adv. Sci. 2018, 5, 1700527. [Google Scholar] [CrossRef] [Green Version]
- Smith, R.; Russo, J.; Fiegel, J.; Brogden, N. Antibiotic delivery strategies to treat skin infections when innate antimicrobial defense fails. Antibiotics 2020, 9, 56. [Google Scholar] [CrossRef] [Green Version]
- Zhou, C.; Sheng, C.; Chen, J.; Liang, Y.; Liu, Q.; Li, P.; Huang, X.; Liu, B. Gradual hydrogel degradation for programable repairing full-thickness skin defect wound. Chem. Eng. J. 2022, 450, 138200. [Google Scholar] [CrossRef]
- Hu, C.; Zhang, F.; Long, L.; Kong, Q.; Luo, R.; Wang, Y. Dual-responsive injectable hydrogels encapsulating drug-loaded micelles for on-demand antimicrobial activity and accelerated wound healing. J. Control. Release 2020, 324, 204–217. [Google Scholar] [CrossRef] [PubMed]
- Dai, T.; Wang, C.; Wang, Y.; Xu, W.; Hu, J.; Cheng, Y. A nanocomposite hydrogel with potent and broad-spectrum antibacterial activity. ACS Appl. Mater. Interfaces 2018, 10, 15163–15173. [Google Scholar] [CrossRef] [PubMed]
- Abdollahi, Z.; Zare, E.N.; Salimi, F.; Goudarzi, I.; Tay, F.R.; Makvandi, P. Bioactive carboxymethyl starch-based hydrogels decorated with CuO nanoparticles: Antioxidant and antimicrobial properties and accelerated wound healing in vivo. Int. J. Mol. Sci. 2021, 22, 2531. [Google Scholar] [CrossRef]
- Berglundh, T.; Giannobile, W.V.; Sanz, M.; Lang, N.P. Lindhe’s Clinical Periodontology and Implant Dentistry; John Wiley & Sons: Hoboken, NJ, USA, 2021. [Google Scholar]
- Mahendra, J.; Palathingal, P.; Mahendra, L.; Alzahrani, K.J.; Banjer, H.J.; Alsharif, K.F.; Halawani, I.F.; Muralidharan, J.; Annamalai, P.T.; Verma, S.S.; et al. Impact of Red Complex Bacteria and TNF-α Levels on the Diabetic and Renal Status of Chronic Kidney Disease Patients in the Presence and Absence of Periodontitis. Biology 2022, 11, 451. [Google Scholar] [CrossRef]
- Suzuki, N.; Yoneda, M.; Hirofuji, T. Mixed red-complex bacterial infection in periodontitis. Int. J. Dent. 2013, 2013, 587279. [Google Scholar] [CrossRef]
- Brissette, C.; Fives-Taylor, P. Actinobacillus actinomycetemcomitans may utilize either actin-dependent or actin-independent mechanisms of invasion. Oral Microbiol. Immunol. 1999, 14, 137–142. [Google Scholar] [CrossRef] [PubMed]
- Ardila, C.-M.; Bedoya-García, J.-A. Antimicrobial resistance of Aggregatibacter actinomycetemcomitans, Porphyromonas gingivalis and Tannerella forsythia in periodontitis patients. J. Glob. Antimicrob. Resist. 2020, 22, 215–218. [Google Scholar] [CrossRef] [PubMed]
- Mohanty, R.; Asopa, S.J.; Joseph, M.D.; Singh, B.; Rajguru, J.P.; Saidath, K.; Sharma, U. Red complex: Polymicrobial conglomerate in oral flora: A review. J. Fam. Med. Prim. Care 2019, 8, 3480. [Google Scholar]
- Meng, Q.; Gao, Q.; Mehrazarin, S.; Tangwanichgapong, K.; Wang, Y.; Huang, Y.; Pan, Y.; Robinson, S.; Liu, Z.; Zangiabadi, A.; et al. Fusobacterium nucleatum secretes amyloid-like FadA to enhance pathogenicity. EMBO Rep. 2021, 22, e52891. [Google Scholar] [CrossRef]
- MContaldo, I.A.; Lajolo, C.; Gioco, G.; Inchingolo, F.; Serpico, R. Overview on osteoporosis, periodontitis and oral dysbiosis: The emerging role of oral microbiota. Appl. Sci. 2020, 10, 6000. [Google Scholar] [CrossRef]
- Negrini, T.D.C.; Carlos, I.Z.; Duque, C.; Caiaffa, K.S.; Arthur, R.A. Interplay among the oral microbiome, oral cavity conditions, the host immune response, diabetes mellitus, and its associated-risk factors—An overview. Front. Oral Health 2021, 2, 697428. [Google Scholar] [CrossRef] [PubMed]
- Dahlen, G.; Basic, A.; Bylund, J. Importance of virulence factors for the persistence of oral bacteria in the inflamed gingival crevice and in the pathogenesis of periodontal disease. J. Clin. Med. 2019, 8, 1339. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nakagawa, M.; Shirasugi, M.; Yamamoto, T.; Nakaya, T.; Kanamura, N. Long-term exposure to butyric acid induces excessive production of matrix metalloproteases in human gingival fibroblasts. Arch. Oral Biol. 2021, 123, 105035. [Google Scholar] [CrossRef] [PubMed]
- Chen, M.; Cai, W.; Zhao, S.; Shi, L.; Chen, Y.; Li, X.; Sun, X.; Mao, Y.; He, B.; Hou, Y.; et al. Oxidative stress-related biomarkers in saliva and gingival crevicular fluid associated with chronic periodontitis: A systematic review and meta-analysis. J. Clin. Periodontol. 2019, 46, 608–622. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.; Gou, Y.; Pan, X.; Gu, Z.; Xie, H. Advances of multifunctional hydrogels for periodontal disease. Smart Mater. Med. 2023, 4, 460–467. [Google Scholar] [CrossRef]
- Curtis, D.A.; Lin, G.H.; Rajendran, Y.; Gessese, T.; Suryadevara, J.; Kapila, Y.L. Treatment planning considerations in the older adult with periodontal disease. Periodontology 2000 2021, 87, 157–165. [Google Scholar] [CrossRef]
- Salhi, L.; De Carvalho, B.; Reners, M. Update on the roles of oral hygiene and plaque control on periodontal disease. In Periodontitis Advances in Experimental Research; Springer: Berlin/Heidelberg, Germany, 2022; pp. 329–339. [Google Scholar]
- Pejčić, A.; Kesić, L.; Obradović, R.; Mirković, D. Antibiotics in the Management of Periodontal Disease. Acta Fac. Med. Naissensis 2010, 27, 85–92. [Google Scholar]
- Abazi, B.; Mihani, J. Prescription of Antibiotics for Periodontal Disease among Dentists in the Region of Tirana. Open Access. Maced. J. Med. Sci. 2018, 6, 1486–1491. [Google Scholar] [CrossRef] [Green Version]
- van der Ouderaa, F.J. Anti-plaque agents. Rationale and prospects for prevention of gingivitis and periodontal disease. J. Clin. Periodontol. 1991, 18, 447–454. [Google Scholar] [CrossRef]
- Bhat, N.; Bapat, S.; Asawa, K.; Tak, M.; Chaturvedi, P.; Gupta, V.V.; George, P.P. The antiplaque efficacy of propolis-based herbal toothpaste: A crossover clinical study. J. Nat. Sci. Biol. Med. 2015, 6, 364. [Google Scholar]
- Magaz, V.R.; Llovera, B.F.; Martí, M.; Garre, A. Clinical Impact and Cosmetic Acceptability of Chlorhexidine-enriched Toothpaste and Mouthwash Application on Periodontal Disease: A Randomized Clinical Study. J. Contemp. Dent. Pract. 2018, 19, 1295–1300. [Google Scholar] [CrossRef] [PubMed]
- Rajendiran, M.; Trivedi, H.M.; Chen, D.; Gajendrareddy, P.; Chen, L. Recent development of active ingredients in mouthwashes and toothpastes for periodontal diseases. Molecules 2021, 26, 2001. [Google Scholar] [CrossRef] [PubMed]
- Maestre, J.R.; Bascones, A.; Sánchez, P.; Matesanz, P.; Aguilar, L.; Giménez, M.J.; Pérez-Balcabao, I.; Granizo, J.J.; Prieto, J. Odontogenic bacteria in periodontal disease and resistance patterns to common antibiotics used as treatment and prophylaxis in odontology in Spain. Rev. Esp. Quimioter. 2007, 20, 61–67. [Google Scholar]
- Castillo, Y.; Delgadillo, N.A.; Neuta, Y.; Hernández, A.; Acevedo, T.; Cárdenas, E.; Montaño, A.; Lafaurie, G.I.; Castillo, D.M. Antibiotic Susceptibility and Resistance Genes in Oral Clinical Isolates of Prevotella intermedia, Prevotella nigrescens, and Prevotella melaninogenica. Antibiotics 2022, 11, 888. [Google Scholar] [CrossRef]
- Jepsen, K.; Falk, W.; Brune, F.; Fimmers, R.; Jepsen, S.; Bekeredjian-Ding, I. Prevalence and antibiotic susceptibility trends of periodontal pathogens in the subgingival microbiota of German periodontitis patients: A retrospective surveillance study. J. Clin. Periodontol. 2021, 48, 1216–1227. [Google Scholar] [CrossRef]
- Saleem, H.G.M.; Seers, C.A.; Sabri, A.N.; Reynolds, E.C. Dental plaque bacteria with reduced susceptibility to chlorhexidine are multidrug resistant. BMC Microbiol. 2016, 16, 214. [Google Scholar] [CrossRef] [Green Version]
- British National Formulary (Online) London. 2022. Available online: https://www.medicinescomplete.com/#/ (accessed on 7 April 2023).
- Ardila, C.M.; López, M.A.; Guzmán, I.C. High resistance against clindamycin, metronidazole and amoxicillin in Porphyromonas gingivalis and Aggregatibacter actinomycetemcomitans isolates of periodontal disease. Med. Oral Patol. Oral Cir. Bucal 2010, 15, e947–e951. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rams, T.E.; Sautter, J.D.; van Winkelhoff, A.J. Comparative in vitro resistance of human periodontal bacterial pathogens to tinidazole and four other antibiotics. Antibiotics 2020, 9, 68. [Google Scholar] [CrossRef] [Green Version]
- Maeda, K.; Hirai, Y.; Nashi, M.; Yamamoto, S.; Taniike, N.; Takenobu, T. Clinical features and antimicrobial susceptibility of oral bacteria isolated from the blood cultures of patients with infective endocarditis. J. Dent. Sci. 2022, 17, 870–875. [Google Scholar] [CrossRef]
- Conrads, G.; Klomp, T.; Deng, D.; Wenzler, J.-S.; Braun, A.; Abdelbary, M.M. The Antimicrobial susceptibility of porphyromonas gingivalis: Genetic repertoire, global phenotype, and review of the literature. Antibiotics 2021, 10, 1438. [Google Scholar] [CrossRef]
- Ni, J.; Yuan, C.; Zhang, S. Study on the drug resistance of pathogens causing an oral and maxillofacial space infection in children. Zhongguo Bingyuan Shengwuxue Zazhi/J. Pathog. Biol. 2019, 14, 592–599. [Google Scholar]
- Eisenblätter, M.; Klaus, C.; Pletz, M.W.R.; Orawa, H.; Hahn, H.; Wagner, J.; Lode, H. Influence of azithromycin and clarithromycin on macrolide susceptibility of viridans streptococci from the oral cavity of healthy volunteers. Eur. J. Clin. Microbiol. Infect. Dis. 2008, 27, 1087–1092. [Google Scholar] [CrossRef]
- Gilmore, W.; Jacobus, N.; Gorbach, S.; Doku, H.; Tally, F. A prospective double-blind evaluation of penicillin versus clindamycin in the treatment of odontogenic infections. J. Oral Maxillofac. Surg. 1988, 46, 1065–1070. [Google Scholar] [CrossRef]
- Loyola-Rodriguez, J.P.; Ponce-Diaz, M.E.; Loyola-Leyva, A.; Garcia-Cortes, J.O.; Medina-Solis, C.E.; Contreras-Ramire, A.A.; Serena-Gomez, E. Determination and identification of antibiotic-resistant oral streptococci isolated from active dental infections in adults. Acta Odontol. Scand. 2018, 76, 229–235. [Google Scholar] [CrossRef]
- Arredondo, A.; Blanc, V.; Mor, C.; Nart, J.; León, R. Azithromycin and erythromycin susceptibility and macrolide resistance genes in Prevotella from patients with periodontal disease. Oral Dis. 2019, 25, 860–867. [Google Scholar] [CrossRef] [PubMed]
- Gaharwar, A.K.; Peppas, N.A.; Khademhosseini, A. Nanocomposite hydrogels for biomedical applications. Biotechnol. Bioeng. 2014, 111, 441–453. [Google Scholar] [CrossRef] [Green Version]
- Fu, G.; Chen, Y.; Cui, Z.; Li, Y.; Zhou, W.; Xin, S.; Tang, Y.; Goodenough, J.B. Novel hydrogel-derived bifunctional oxygen electrocatalyst for rechargeable air cathodes. Nano Lett. 2016, 16, 6516–6522. [Google Scholar] [CrossRef]
- Ahmed, E.M. Hydrogel: Preparation, characterization, and applications: A review. J. Adv. Res. 2015, 6, 105–121. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bustamante-Torres, M.; Romero-Fierro, D.; Arcentales-Vera, B.; Palomino, K.; Magaña, H.; Bucio, E. Hydrogels classification according to the physical or chemical interactions and as stimuli-sensitive materials. Gels 2021, 7, 182. [Google Scholar] [CrossRef] [PubMed]
- Ahovan, Z.A.; Esmaeili, Z.; Eftekhari, B.S.; Khosravimelal, S.; Alehosseini, M.; Orive, G.; Dolatshahi-Pirouz, A.; Chauhan, N.P.S.; Janmey, P.A.; Hashemi, A.; et al. Antibacterial smart hydrogels: New hope for infectious wound management. Materials Today Bio 2022, 17, 100499. [Google Scholar] [CrossRef]
- Khan, Y.A.; Ozaltin, K.; Bernal-Ballen, A.; Di Martino, A. Chitosan-alginate hydrogels for simultaneous and sustained releases of ciprofloxacin, amoxicillin and vancomycin for combination therapy. J. Drug Deliv. Sci. Technol. 2021, 61, 102126. [Google Scholar] [CrossRef]
- Zhao, C.; Zhou, L.; Chiao, M.; Yang, W. Antibacterial hydrogel coating: Strategies in surface chemistry. Adv. Colloid Interface Sci. 2020, 285, 102280. [Google Scholar] [CrossRef]
- Caló, E.; Barros, J.; Ballamy, L.; Khutoryanskiy, V.V. Poly (vinyl alcohol)–Gantrez® AN cryogels for wound care applications. RSC Adv. 2016, 6, 105487–105494. [Google Scholar] [CrossRef] [Green Version]
- Caló, E.; de Barros, J.M.; Fernández-Gutiérrez, M.; Román, J.S.; Ballamy, L.; Khutoryanskiy, V.V. Antimicrobial hydrogels based on autoclaved poly (vinyl alcohol) and poly (methyl vinyl ether-alt-maleic anhydride) mixtures for wound care applications. RSC Adv. 2016, 6, 55211–55219. [Google Scholar] [CrossRef] [Green Version]
- Larrañeta, E.; Henry, M.; Irwin, N.J.; Trotter, J.; Perminova, A.A.; Donnelly, R.F. Synthesis and characterization of hyaluronic acid hydrogels crosslinked using a solvent-free process for potential biomedical applications. Carbohydr. Polym. 2018, 181, 1194–1205. [Google Scholar] [CrossRef] [Green Version]
- Larrañeta, E.; Imízcoz, M.; Toh, J.X.; Irwin, N.J.; Ripolin, A.; Perminova, A.; Domínguez-Robles, J.; Rodríguez, A.; Donnelly, R.F. Synthesis and characterization of lignin hydrogels for potential applications as drug eluting antimicrobial coatings for medical materials. ACS Sustain. Chem. Eng. 2018, 6, 9037–9046. [Google Scholar] [CrossRef]
- González-Vázquez, P.; Larrañeta, E.; McCrudden, M.T.; Jarrahian, C.; Rein-Weston, A.; Quintanar-Solares, M.; Zehrung, D.; McCarthy, H.; Courtenay, A.J.; Donnelly, R.F. Transdermal delivery of gentamicin using dissolving microneedle arrays for potential treatment of neonatal sepsis. J. Control. Release 2017, 265, 30–40. [Google Scholar] [CrossRef] [Green Version]
- Yu, H.; Xu, X.; Chen, X.; Lu, T.; Zhang, P.; Jing, X. Preparation and antibacterial effects of PVA-PVP hydrogels containing silver nanoparticles. J. Appl. Polym. Sci. 2007, 103, 125–133. [Google Scholar] [CrossRef]
- Forero-Doria, O.; Polo, E.; Marican, A.; Guzmán, L.; Venegas, B.; Vijayakumar, S.; Wehinger, S.; Guerrero, M.; Gallego, J.; Durán-Lara, E.F. Supramolecular hydrogels based on cellulose for sustained release of therapeutic substances with antimicrobial and wound healing properties. Carbohydr. Polym. 2020, 242, 116383. [Google Scholar] [CrossRef] [PubMed]
- Tang, X.; Gu, X.; Wang, Y.; Chen, X.; Ling, J.; Yang, Y. Stable antibacterial polysaccharide-based hydrogels as tissue adhesives for wound healing. RSC Adv. 2020, 10, 17280–17287. [Google Scholar] [CrossRef]
- Gharibi, R.; Shaker, A.; Rezapour-Lactoee, A.; Agarwal, S. Antibacterial and biocompatible hydrogel dressing based on gelatin-and castor-oil-derived biocidal agent. ACS Biomater. Sci. Eng. 2021, 7, 3633–3647. [Google Scholar] [CrossRef]
- Zakia, M.; Koo, J.M.; Kim, D.; Ji, K.; Huh, P.; Yoon, J.; Yoo, S.I. Development of silver nanoparticle-based hydrogel composites for antimicrobial activity. Green Chem. Lett. Rev. 2020, 13, 34–40. [Google Scholar] [CrossRef] [Green Version]
- Ter Boo, G.J.; Schmid, T.; Zderic, I.; Nehrbass, D.; Camenisch, K.; Richards, R.G.; Grijpma, D.W.; Moriarty, T.F.; Eglin, D. Local application of a gentamicin-loaded thermo-responsive hydrogel allows for fracture healing upon clearance of a high Staphylococcus aureus load in a rabbit model. Eur. Cells Mater. 2018, 35, 151–164. [Google Scholar] [CrossRef]
- Rodgers, A.M.; McCrudden, M.T.; Courtenay, A.J.; Kearney, M.C.; Edwards, K.L.; Ingram, R.J.; Bengoechea, J.; Donnelly, R.F. Control of Klebsiella pneumoniae infection in mice by using dissolving microarray patches containing gentamicin. Antimicrob. Agents Chemother. 2019, 63, e02612-18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tallet, L.; Gribova, V.; Ploux, L.; Vrana, N.E.; Lavalle, P. New smart antimicrobial hydrogels, nanomaterials, and coatings: Earlier action, more specific, better dosing? Adv. Healthc. Mater. 2021, 10, 2001199. [Google Scholar] [CrossRef]
- Merino, S.; Martín, C.; Kostarelos, K.; Prato, M.; Vázquez, E. Nanocomposite hydrogels: 3D polymer–nanoparticle synergies for on-demand drug delivery. ACS Nano 2015, 9, 4686–4697. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jalababu, R.; Reddy, M.K.; Reddy, K.S.; Rao, K.S.K. Hydrogels as Smart Drug Delivery Systems: Recent Advances. In Smart Nanomaterials in Biomedical Applications; Springer: Berlin/Heidelberg, Germany, 2022; pp. 173–201. [Google Scholar]
- Gheysoori, P.; Paydayesh, A.; Jafari, M.; Peidayesh, H. Thermoresponsive nanocomposite hydrogels based on Gelatin/poly (N–isopropylacrylamide)(PNIPAM) for controlled drug delivery. Eur. Polym. J. 2023, 186, 111846. [Google Scholar] [CrossRef]
- Zarrintaj, P.; Jouyandeh, M.; Ganjali, M.R.; Hadavand, B.S.; Mozafari, M.; Sheiko, S.S.; Vatankhah-Varnoosfaderani, M.; Gutiérrez, T.J.; Saeb, M.R. Thermo-sensitive polymers in medicine: A review. Eur. Polym. J. 2019, 117, 402–423. [Google Scholar] [CrossRef]
- Wang, C.; Feng, N.; Chang, F.; Wang, J.; Yuan, B.; Cheng, Y.; Liu, H.; Yu, J.; Zou, J.; Ding, J.; et al. Injectable Cholesterol-Enhanced Stereocomplex Polylactide Thermogel Loading Chondrocytes for Optimized Cartilage Regeneration. Adv. Healthc. Mater. 2019, 8, 1900312. [Google Scholar] [CrossRef]
- Pham, D.T.; Phewchan, P.; Navesit, K.; Chokamonsirikun, A.; Khemwong, T.; Tiyaboonchai, W. Development of metronidazole-loaded in situ thermosensitive hydrogel for periodontitis treatment. Turk. J. Pharm. Sci. 2021, 18, 510. [Google Scholar] [CrossRef] [PubMed]
- Anirudhan, T.; Mohan, M.; Rajeev, M. Modified chitosan-hyaluronic acid based hydrogel for the pH-responsive Co-delivery of cisplatin and doxorubicin. Int. J. Biol. Macromol. 2022, 201, 378–388. [Google Scholar] [CrossRef] [PubMed]
- Sah, A.K.; Dewangan, M.; Suresh, P.K. Potential of chitosan-based carrier for periodontal drug delivery. Colloids Surf. B Biointerfaces 2019, 178, 185–198. [Google Scholar] [CrossRef] [PubMed]
- Ikinci, G.; Şenel, S.; Akıncıbay, H.; Kaş, S.; Erciş, S.; Wilson, C.G.; Hıncal, A.A. Effect of chitosan on a periodontal pathogen Porphyromonas gingivalis. Int. J. Pharm. 2002, 235, 121–127. [Google Scholar] [CrossRef]
- Liu, J.; Liu, H.; Jia, Y.; Tan, Z.; Hou, R.; Lu, J.; Luo, D.; Fu, X.; Wang, L.; Wang, X. Glucose-sensitive delivery of tannic acid by a photo-crosslinked chitosan hydrogel film for antibacterial and anti-inflammatory therapy. J. Biomater. Sci. Polym. Ed. 2022, 33, 1644–1663. [Google Scholar] [CrossRef] [PubMed]
- Ghauri, Z.H.; Islam, A.; Qadir, M.A.; Ghaffar, A.; Gull, N.; Azam, M.; Mehmood, A.; Ghauri, A.A.; Khan, R.U. Novel pH-responsive chitosan/sodium alginate/PEG based hydrogels for release of sodium ceftriaxone. Mater. Chem. Phys. 2022, 277, 125456. [Google Scholar] [CrossRef]
- Tian, B.; Liu, J. Smart stimuli-responsive chitosan hydrogel for drug delivery: A review. Int. J. Biol. Macromol. 2023, 235, 123902. [Google Scholar] [CrossRef]
- Rizwan, M.; Yahya, R.; Hassan, A.; Yar, M.; Azzahari, A.D.; Selvanathan, V.; Sonsudin, F.; Abouloula, C.N. pH sensitive hydrogels in drug delivery: Brief history, properties, swelling, and release mechanism, material selection and applications. Polymers 2017, 9, 137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aycan, D.; Alemdar, N. Development of pH-responsive chitosan-based hydrogel modified with bone ash for controlled release of amoxicillin. Carbohydr. Polym. 2018, 184, 401–407. [Google Scholar] [CrossRef]
- Kulkarni, R.; Biswanath, S. Electrically responsive smart hydrogels in drug delivery: A review. J. Appl. Biomater. Biomech. 2007, 5, 125–139. [Google Scholar]
- Verma, A.; Sharma, B.; Kalia, S.; Alsanie, W.F.; Thakur, S.; Thakur, V.K. Carboxymethyl cellulose based sustainable hydrogel for colon-specific delivery of gentamicin. Int. J. Biol. Macromol. 2023, 228, 773–782. [Google Scholar] [CrossRef]
- Kang, W.; Liang, J.; Liu, T.; Long, H.; Huang, L.; Shi, Q.; Zhang, J.; Deng, S.; Tan, S. Preparation of silane-dispersed graphene crosslinked vinyl carboxymethyl chitosan temperature-responsive hydrogel with antibacterial properties. Int. J. Biol. Macromol. 2022, 200, 99–109. [Google Scholar] [CrossRef] [PubMed]
- Lin, J.; He, Z.; Liu, F.; Feng, J.; Huang, C.; Sun, X.; Deng, H. Hybrid hydrogels for synergistic periodontal antibacterial treatment with sustained drug release and NIR-responsive photothermal effect. Int. J. Nanomed. 2020, 15, 5377–5387. [Google Scholar] [CrossRef]
- Adams, S.B., Jr.; Shamji, M.F.; Nettles, D.L.; Hwang, P.; Setton, L.A. Sustained release of antibiotics from injectable and thermally responsive polypeptide depots. J. Biomed. Mater. Res. Part B Appl. Biomater. 2009, 90, 67–74. [Google Scholar] [CrossRef] [Green Version]
- Souto, E.; Wissing, S.; Barbosa, C.; Müller, R. Development of a controlled release formulation based on SLN and NLC for topical clotrimazole delivery. Int. J. Pharm. 2004, 278, 71–77. [Google Scholar] [CrossRef] [PubMed]
- Adepu, S.; Ramakrishna, S. Controlled drug delivery systems: Current status and future directions. Molecules 2021, 26, 5905. [Google Scholar] [CrossRef]
- Kumar, N.; Ghosh, B.; Kumar, A.; Koley, R.; Dhara, S.; Chattopadhyay, S. Multilayered SMART hydrogel systems for on-site drug delivery applications. J. Drug Deliv. Sci. Technol. 2022, 80, 104111. [Google Scholar] [CrossRef]
- Ladet, S.; David, L.; Domard, A. Multi-membrane hydrogels. Nature 2008, 452, 76–79. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y. Hydrogels Based on Natural Polymers; Elsevier: Amsterdam, The Netherlands, 2019. [Google Scholar]
- Martínez-Sanz, M.; Mikkelsen, D.; Flanagan, B.; Gidley, M.J.; Gilbert, E.P. Multi-scale model for the hierarchical architecture of native cellulose hydrogels. Carbohydr. Polym. 2016, 147, 542–555. [Google Scholar] [CrossRef]
- Unagolla, J.M.; Jayasuriya, A.C. Hydrogel-based 3D bioprinting: A comprehensive review on cell-laden hydrogels, bioink formulations, and future perspectives. Appl. Mater. Today 2020, 18, 100479. [Google Scholar] [CrossRef]
- Duan, J.; Hou, R.; Xiong, X.; Wang, Y.; Wang, Y.; Fu, J.; Yu, Z. Versatile fabrication of arbitrarily shaped multi-membrane hydrogels suitable for biomedical applications. J. Mater. Chem. B 2013, 1, 485–492. [Google Scholar] [CrossRef]
- Xiong, Y.; Yan, K.; Bentley, W.E.; Deng, H.; Du, Y.; Payne, G.F.; Shi, X.W. Compartmentalized multilayer hydrogel formation using a stimulus-responsive self-assembling polysaccharide. ACS Appl. Mater. Interfaces 2014, 6, 2948–2957. [Google Scholar] [CrossRef] [PubMed]
- Dhanasingh, A.; Groll, J. Polysaccharide based covalently linked multi-membrane hydrogels. Soft Matter 2012, 8, 1643–1647. [Google Scholar] [CrossRef]
- Pakzad, Y.; Ganji, F. Thermosensitive hydrogel for periodontal application: In vitro drug release, antibacterial activity and toxicity evaluation. J. Biomater. Appl. 2016, 30, 919–929. [Google Scholar] [CrossRef]
- Gan, Z.; Xiao, Z.; Zhang, Z.; Li, Y.; Liu, C.; Chen, X.; Liu, Y.; Wu, D.; Liu, C.; Shuai, X.; et al. Stiffness-tuned and ROS-sensitive hydrogel incorporating complement C5a receptor antagonist modulates antibacterial activity of macrophages for periodontitis treatment. Bioact. Mater. 2023, 25, 347–359. [Google Scholar] [CrossRef] [PubMed]
- Petit, C.; Batool, F.; Stutz, C.; Anton, N.; Klymchenko, A.; Vandamme, T.; Benkirane-Jessel, N.; Huck, O. Development of a thermosensitive statin loaded chitosan-based hydrogel promoting bone healing. Int. J. Pharm. 2020, 586, 119534. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro, J.S.; Daghrery, A.; Dubey, N.; Li, C.; Mei, L.; Fenno, J.C.; Schwendeman, A.; Aytac, Z.; Bottino, M.C. Hybrid antimicrobial hydrogel as injectable therapeutics for oral infection ablation. Biomacromolecules 2020, 21, 3945–3956. [Google Scholar] [CrossRef]
- Li, N.; Xie, L.; Wu, Y.; Wu, Y.; Liu, Y.; Gao, Y.; Yang, J.; Zhang, X.; Jiang, L. Dexamethasone-loaded zeolitic imidazolate frameworks nanocomposite hydrogel with antibacterial and anti-inflammatory effects for periodontitis treatment. Mater. Today Bio 2022, 16, 100360. [Google Scholar] [CrossRef]
- Tian, B.; Hua, S.; Tian, Y.; Liu, J. Chemical and physical chitosan hydrogels as prospective carriers for drug delivery: A review. J. Mater. Chem. B 2020, 8, 10050–10064. [Google Scholar] [CrossRef]
- Li, J.; Mooney, D.J. Designing hydrogels for controlled drug delivery. Nat. Rev. Mater. 2016, 1, 16071. [Google Scholar] [CrossRef]
- Liu, J.; Tian, B.; Liu, Y.; Wan, J.-B. Cyclodextrin-containing hydrogels: A review of preparation method, drug delivery, and degradation behavior. Int. J. Mol. Sci. 2021, 22, 13516. [Google Scholar] [CrossRef]
- Larrañeta, E.; Stewart, S.; Ervine, M.; Al-Kasasbeh, R.; Donnelly, R.F. Hydrogels for hydrophobic drug delivery. Classification, synthesis and applications. J. Funct. Biomater. 2018, 9, 13. [Google Scholar] [CrossRef] [Green Version]
- Larrañeta, E.; Barturen, L.; Ervine, M.; Donnelly, R.F. Hydrogels based on poly (methyl vinyl ether-co-maleic acid) and Tween 85 for sustained delivery of hydrophobic drugs. Int. J. Pharm. 2018, 538, 147–158. [Google Scholar] [CrossRef] [Green Version]
- Gu, D.; O’Connor, A.J.; Qiao, G.G.H.; Ladewig, K. Hydrogels with smart systems for delivery of hydrophobic drugs. Expert Opin. Drug Deliv. 2017, 14, 879–895. [Google Scholar] [CrossRef] [PubMed]
- Al-Hasani, K.; Mathiyalagan, P.; El-Osta, A. Epigenetics, cardiovascular disease, and cellular reprogramming. J. Mol. Cell Cardiol. 2019, 128, 129–133. [Google Scholar] [CrossRef]
- Dias, A.M.; da Silva, F.G.; de Figueiredo Monteiro, A.P.; Pinzón-García, A.D.; Sinisterra, R.D.; Cortés, M.E. Polycaprolactone nanofibers loaded oxytetracycline hydrochloride and zinc oxide for treatment of periodontal disease. Mater. Sci. Eng. C 2019, 103, 109798. [Google Scholar] [CrossRef] [PubMed]
- Krishnan, S. Biofilm formation on medical devices and infection: Preventive approaches. In Biofilm and Materials Science; Springer: Berlin/Heidelberg, Germany, 2015; pp. 93–108. [Google Scholar]
- Wroe, J.A.; Johnson, C.T.; García, A.J. Bacteriophage delivering hydrogels reduce biofilm formation in vitro and infection in vivo. J. Biomed. Mater. Res. Part A 2020, 108, 39–49. [Google Scholar] [CrossRef] [PubMed]




| Generic Drug Name | Drug Class | Available Medicinal Form | PD Antimicrobial Resistance Reported | Formulation | Reference |
|---|---|---|---|---|---|
| Amoxicillin | Penicillins | Capsule, oral suspension, oral powder | Yes | Immediate release | [49,53,54,55] |
| Azithromycin | Macrolides | Capsule, eyedrop, tablet, oral suspension, powder for solution for infusion, | Yes | Immediate release | [49,56,57] |
| Cefalexin | Cephalosporins | Tablet, capsule, oral suspension | Yes | Immediate release | [58] |
| Chlorhexidine | Antiseptic and disinfectant | Oral gel, mouthwash, spray | Yes | Immediate release | [52] |
| Clarithromycin | Macrolides | Tablet, granule, oral suspension, powder for infusion | Yes | Immediate and modified release | [53,56,59] |
| Clindamycin | Lincosamide | Capsule, gel, cream, infusion, solution for injection, oral suspension | Yes | Immediate release | [54,55,57,60,61] |
| Co-amoxiclav | Penicillins | Tablet, oral suspension, powder for solution for injection | No | Immediate release | [49,61] |
| Doxycycline | tetracyclines | Capsule, tablet, dispersible tablets | Yes | Immediate and modified release | [51,55] |
| Erythromycin | Macrolides | Tablet, oral suspension, powder for infusion | Yes | Immediate release | [62] |
| Metronidazole | Nitroimidazole derivative | Tablet, oral suspension, infusion, suppository, cream, gel | Yes | Immediate release | [51,58] |
| Oxytetracycline | tetracyclines | Tablet, oral suspension | - | Immediate release | [53] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mensah, A.; Rodgers, A.M.; Larrañeta, E.; McMullan, L.; Tambuwala, M.; Callan, J.F.; Courtenay, A.J. Treatment of Periodontal Infections, the Possible Role of Hydrogels as Antibiotic Drug-Delivery Systems. Antibiotics 2023, 12, 1073. https://doi.org/10.3390/antibiotics12061073
Mensah A, Rodgers AM, Larrañeta E, McMullan L, Tambuwala M, Callan JF, Courtenay AJ. Treatment of Periodontal Infections, the Possible Role of Hydrogels as Antibiotic Drug-Delivery Systems. Antibiotics. 2023; 12(6):1073. https://doi.org/10.3390/antibiotics12061073
Chicago/Turabian StyleMensah, Adelaide, Aoife M. Rodgers, Eneko Larrañeta, Lyndsey McMullan, Murtaza Tambuwala, John F. Callan, and Aaron J. Courtenay. 2023. "Treatment of Periodontal Infections, the Possible Role of Hydrogels as Antibiotic Drug-Delivery Systems" Antibiotics 12, no. 6: 1073. https://doi.org/10.3390/antibiotics12061073