
The Impact of the COVID-19 Pandemic in Postoperative Neurosurgical Infections at a Reference Center in México

 , ,
, ,
Abstract
:1. Introduction
2. Results
3. Discussion
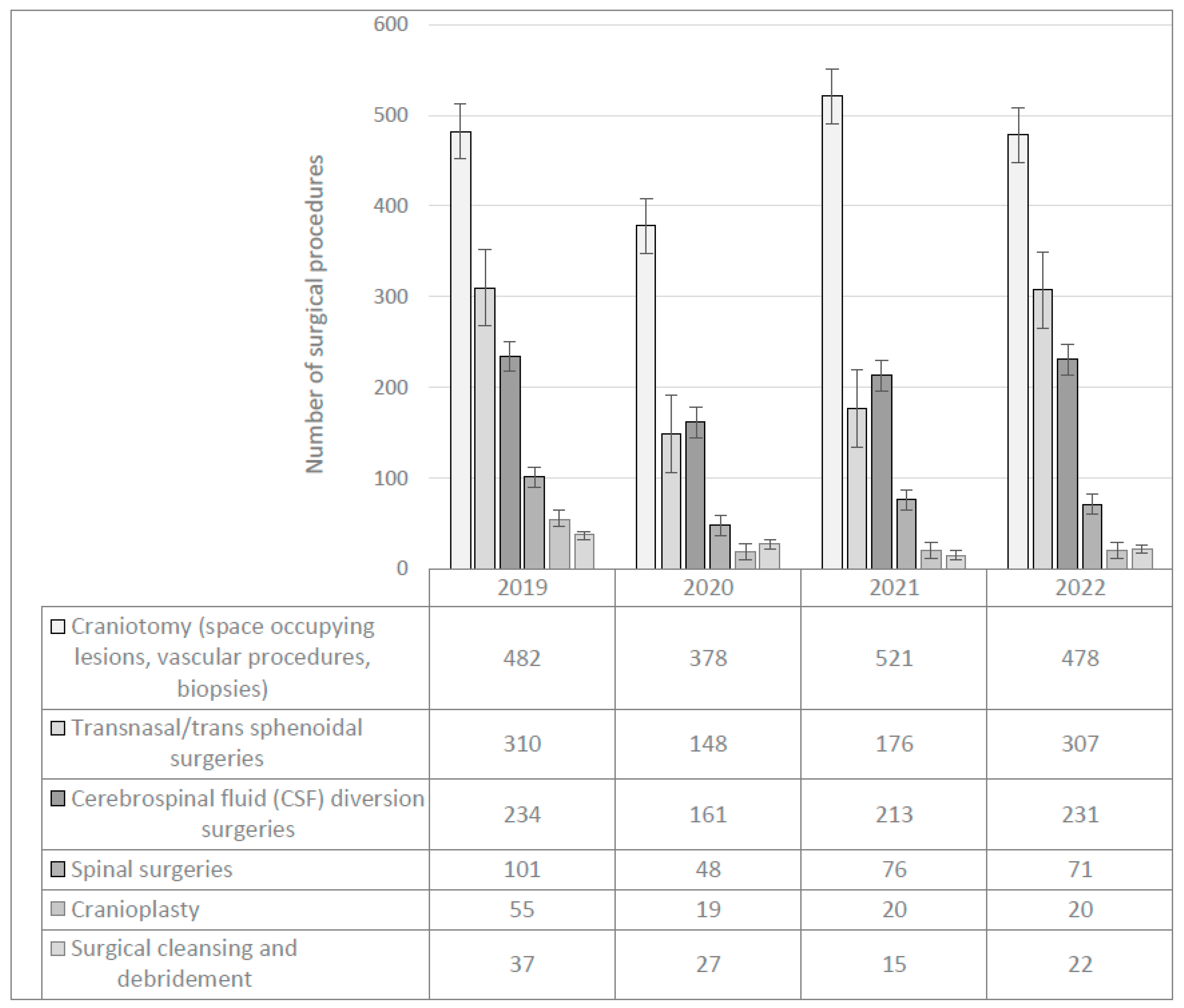
3.1. Reduction of Neurosurgical Procedures
3.2. Changes in Mortality Rates after Neurosurgery during the Pandemic Period
3.3. Impact on Training of Neurosurgical Residents Worldwide, Telehealth Visits and Satisfacton
3.4. Limitations and Strengths of Our Study
4. Materials and Methods
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Khalafallah, A.M.; Jimenez, A.E.; Lee, R.P.; Weingart, J.D.; Theodore, N.; Cohen, A.R.; Tamargo, R.J.; Huang, J.; Brem, H.; Mukherjee, D. Impact of COVID-19 on an Academic Neurosurgery Department: The Johns Hopkins Experience. World Neurosurg. 2020, 139, e877–e884. [Google Scholar] [CrossRef] [PubMed]
- Khalafallah, A.M.; Jimenez, A.E.; Mukherjee, D. In Reply to the Letter to the Editor Regarding “Impact of COVID-19 on an Academic Neurosurgery Department: The Johns Hopkins Experience”. World Neurosurg. 2020, 143, 601–602. [Google Scholar] [CrossRef] [PubMed]
- Goyal, N.; Venkataram, T.; Dash, C.; Chandra, P.P. Letter to the Editor Regarding: ‘Impact of COVID-19 on an Academic Neurosurgery Department: The Johns Hopkins Experience’. World Neurosurg. 2020, 143, 599–600. [Google Scholar] [CrossRef] [PubMed]
- Sander, C.; von Dercks, N.; Fehrenbach, M.K.; Wende, T.; Stehr, S.; Winkler, D.; Meixensberger, J.; Arlt, F. Neurosurgical care during the COVID-19 pandemic in central germany: A retrospective single center study of the second wave. Int. J. Environ. Res. Pub. Health 2022, 18, 12034. [Google Scholar] [CrossRef] [PubMed]
- Hussein, K.; Geoghegan, A.; Hassan, M.; Moore, M. The impact of COVID-19 on neurosurgical theatre activity in the National Neurosurgical Centre of Ireland. Ir. J. Med. Sci. 2022, 192, 823–827. [Google Scholar] [CrossRef] [PubMed]
- Petr, O.; Grassner, L.; Warner, F.M.; Dedeciusová, M.; Voldřich, R.; Geiger, P.; Brawanski, K.; Gsellmann, S.; Meiners, L.C.; Bauer, R.; et al. Current trends and outcomes of non-elective neurosurgical care in Central Europe during the second year of the COVID-19 pandemic. Sci. Rep. 2022, 12, 14631. [Google Scholar] [CrossRef]
- Jankovic, D.; Krenzlin, H.; Keric, N.; Ottenhausen, M. The impact of SARS-CoV-2 measures on patient samples and complication rates in spine surgery—A single center analysis. Front. Surg. 2023, 9, 1086960. [Google Scholar] [CrossRef]
- Nabil, M.; Dorrah, M.; Sharfeldin, A.; Abaza, H. Impact of COVID-19 pandemic on the neurosurgical practice in Egypt. Egypt. J. Neurosurg. 2022, 37, 23. [Google Scholar] [CrossRef]
- Idowu, O.; Oshola, H.; Idowu, J.; Omosuyi, A. A tropical tertiary neurosurgical centre response to COVID-19 pandemic and its effect on neurosurgical practices. Afr. Health Sci. 2022, 22, 512–519. [Google Scholar] [CrossRef]
- De Macêdo Filho, L.J.M.; Aragão, A.C.A.; dos Santos, V.T.D.; Galvão, L.B.A.; Shlobin, N.A.; de Biase, G.; Suarez-Meade, P.; Almeida, J.P.C.; Quinones-Hinojosa, A.; de Albuquerque, L.A.F. Impact of COVID-19 on Neurosurgery in Brazil’s Health System: The Reality of a Developing Country Affected by the Pandemic. World Neurosurg. 2021, 155, e142–e149. [Google Scholar] [CrossRef]
- Díaz-Bello, S.; Hernández-Hernández, A.; Guinto-Nishimura, G.Y.; Mondragón-Soto, M.G.; Lem-Carrillo, M.; González-Aguilar, A.; Calleja-Castillo, J.M.; Leyva-Rendón, A.; León-Ortiz, P.; Chávez-Piña, C.M.; et al. Reconversion of neurosurgical practice in times of the SARS-CoV-2 pandemic: A narrative review of the literature and guideline implementation in a Mexican neurosurgical referral center. Neurosurg. Focus 2020, 49, E4. [Google Scholar] [CrossRef]
- Prokop, M.; Van Everdingen, W.; van Rees Vellinga, T.; Quarles van Ufford, H.; Stöger, L.; Beenen, L.; Geurts, B.; Gietema, H.; Krdzalic, J.; Schaefer-Prokop, C.; et al. CO-RADS: A Categorical CT Assessment Scheme for Patients Suspected of Having COVID-19-Definition and Evaluation. Radiology 2020, 296, E97–E104. [Google Scholar] [CrossRef]
- Horan, T.C.; Andrus, M.; Dudeck, M.A. CDC/NHSN surveillance definition of health care-associated infection and criteria for specific types of infections in the acute care setting. Am. J. Infect. Control 2008, 36, 309–332. [Google Scholar] [CrossRef]
- Toman, E.; Soon, W.C.; Thanabalasundaram, G.; Burns, D.; Petrik, V.; Watts, C.; Wykes, V.; White, A. Comparison of outcomes of neurosurgical operations performed before and during the COVID-19 pandemic: A matched cohort study. BMJ Open 2021, 11, e047063. [Google Scholar] [CrossRef] [PubMed]
- Soriano Sánchez, J.A.; Perilla Cepeda, T.A.; Zenteno, M.; Campero, A.; Yampolsky, C.; Varela, M.L.; Soto García, M.E.; Romero Rangel, J.A.I. Early Report on the Impact of COVID-19 Outbreak in Neurosurgical Practice Among Members of the Latin American Federation of Neurosurgical Societies. World Neurosurg. 2020, 140, e195–e202. [Google Scholar] [CrossRef] [PubMed]
- Kuo, C.C.; Aguirre, A.O.; Kassay, A.; Donnelly, B.M.; Bakr, H.; Aly, M.; Ezzat, A.A.M.; Soliman, M.A.R. A look at the global impact of COVID-19 pandemic on neurosurgical services and residency training. Sci. Afr. 2023, 19, e01504. [Google Scholar] [CrossRef] [PubMed]
- Munda, M.; Bosnjak, R.; Velnar, T. Problematics of neurosurgical service during the COVID-19 pandemic in Slovenia. World J. Clin. Cases 2022, 10, 12462–12803. [Google Scholar] [CrossRef] [PubMed]
- Permana, G.I.; Faris, M.; Subagio, E.A.; Bajamal, A.H. The effects of the coronavirus disease 2019 pandemic on neurospine surgery practice in the referral center hospital developing country. Surg. Neurol. Int. 2021, 12, 620. [Google Scholar] [CrossRef]
- ElGhamry, A.N.; Jayakumar, N.; Youssef, M.; Shumon, S.; Mitchell, P. COVID-19 and Changes in Neurosurgical Workload in the United Kingdom. World Neurosurg. 2021, 148, e689–e694. [Google Scholar] [CrossRef]
- Chau, M.J.; Quintero, J.E.; Guiliani, A.; Hines, T.; Samaan, C.; Seybold, K.; Stowe, M.; Hanlon, D.; Gerhardth, G.A.; van Horne, C.G. Telehealth Sustainability in a Neurosurgery Department During the COVID-19 Pandemic. World Neurosurg. 2021, 152, e617–e624. [Google Scholar] [CrossRef]
- Karimov, Z.; Ozgiray, E. The effect of COVID-19 in a university hospital neurosurgery clinic comparison to pre-pandemic period: A retrospective study with 6 months of data. World Neurosurg. 2023, 173, e616–e621. [Google Scholar] [CrossRef] [PubMed]
- Poon, M.T.C.; Piper, R.J.; Thango, N.; Fountain, D.M.; Marcus, H.J.; Lippa, L.; Servadei, F.; Esene, I.N.; Freyschlag, C.F.; Neville, I.S.; et al. Variation in postoperative outcomes of patients with intracranial tumors: Insights from a prospective international cohort study during the COVID-19 pandemic. Neuro-Oncology 2023, 10, 34. [Google Scholar] [CrossRef]
- Dokponou, Y.C.H.; Nyalundja, A.D.; Madjoue, A.D.O.; Dossou, M.W.; Badirou, O.; Agada, N.; Lasssissi, K.; Adjovi, F.M.; Lawson, L.D.; Bankole, N.D.A. COVID-19 impact on the global neurosurgery resident training course and admission: A scoping review. Surg. Neurol. Int. 2023, 14, 96. [Google Scholar] [CrossRef]
- Tomlinson, S.B.; Hendricks, B.K.; Cohen-Gadol, A.A. Editorial. Innovations in neurosurgical education during the COVID-19 pandemic: Is it time to reexamine our neurosurgical training models? J. Neurosurg. 2020, 17, 1–2. [Google Scholar] [CrossRef] [Green Version]
- Gadjradj, P.S.; Matawlie, R.H.S.; Harhangi, B.S. Telemedicine use by neurosurgeons due to the COVID-19 related lockdown. Brain Spine 2021, 1, 100851. [Google Scholar] [CrossRef] [PubMed]
- Hopkins, B.S.; Cloney, M.B.; Texakalidis, P.; Karras, C.L.; El Tecle, N.; Swong, K.; Ganju, A.; Stricsek, G.; Wolinksy, J.P.; Potts, M.B.; et al. Outpatient telemedicine in neurosurgery: 15,677 consecutive encounters in a comparative analysis of its effectiveness and impact on the surgical conversion rate. J. Neurosurg. 2023, 14, 1–10. [Google Scholar] [CrossRef]
- Porche, K.; Vaziri, S.; Mehkri, Y.; Christie, C.; Laurent, D.; Wang, Y.; Rahman, M. Patient satisfaction scores with telemedicine in the neurosurgical population. Clin. Neurol. Neurosurg. 2021, 205, 106605. [Google Scholar] [CrossRef]
- Deora, H.; Mishra, S.; Tripathi, M.; Garg, K.; Tandon, V.; Borkar, S.; Varshney, N.; Raut, R.; Chaurasia, B.; Chandra, P.S.; et al. Adapting Neurosurgery Practice During the COVID-19 Pandemic in the Indian Subcontinent. World Neurosurg. 2020, 142, e396–e406. [Google Scholar] [CrossRef]
- Menlibayeva, K.; Babi, A.; Makhambetov, Y.; Akshulakov, S. Challenges in Neurosurgery During the COVID-19 Pandemic: The Experience of Kazakhstan. World Neurosurg. 2021, 161, e376–e383. [Google Scholar] [CrossRef]
- Ashry, A.H.; Soffar, H.M.; Alsawy, M.F. Neurosurgical education during COVID-19: Challenges and lessons learned in Egypt. Egypt. J. Neurol. Psychiatry Neurosurg. 2020, 56, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Magiorakos, A.P.; Srinivasan, A.; Carey, R.B.; Carmeli, Y.; Falagas, M.E.; Giske, C.G.; Harbarth, S.; Hindler, J.F.; Kahlmeter, G.; Olsson-Liljequist, B.; et al. Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria: An international expert proposal for interim standard definitions for acquired resistance. Clin. Microbiol. Infect. 2012, 18, 268–281. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Year | 2019 | 2020 | 2021 | 2022 |
|---|---|---|---|---|
| Number Neurosurgeries/year | 1219 | 781 | 1021 | 1129 |
| Infections number (%) | 39 (3.19) | 44 (5.63) | 42 (4.11) | 35 (3.10) |
| Hospital deaths (%) | 7 (0.57) | 6 (0.76) | 11 (1.07) | 11 (0.97) |
| Year | 2019 | 2020 | 2021 | 2022 |
|---|---|---|---|---|
| Ventriculoperitoneal shunt (VPS) initial placement | 124 | 83 | 112 | 142 |
| Ventriculostomy for acute hydrocephalus | 35 | 23 | 43 | 39 |
| Ventriculostomy for intracranial bleeding | 25 | 21 | 22 | 19 |
| Change from ventriculostomy to VPS | 19 | 12 | 11 | 3 |
| Change from VPS to ventriculostomy | 9 | 4 | 16 | 16 |
| Ventriculostomy after VPS removal due to infection or exchange | 22 | 18 | 9 | 12 |
| Total | 234 | 161 | 213 | 231 |
| Year | 2019 | 2020 | 2021 | 2022 | ||
|---|---|---|---|---|---|---|
| Type of Infection | Total | (%) | ||||
| Surgical site infections * | 15 | 25 | 17 | 12 | 69 | 43.1 |
| Postoperative meningitis | 10 | 10 | 6 | 12 | 38 | 23.8 |
| CSF shunt infection (SSI-meningitis) | 7 | 7 | 11 | 8 | 33 | 20.6 |
| Ventriculitis | 5 | 1 | 6 | 3 | 15 | 9.4 |
| Postoperative bone flap osteomyelitis | 1 | 2 | 3 | 1.9 | ||
| Postoperative abscess | 1 | 1 | 2 | 1.3 | ||
| Total | 39 | 44 | 42 | 35 | 160 | 100 |
| Year | 2019 | 2020 | 2021 | 2022 | Total | (%) |
|---|---|---|---|---|---|---|
| Microorganisms | ||||||
| Coagulase negative staphylo-coccus | 11 | 11 | 16 | 8 | 46 | 27.4 |
| Staphylococcus aureus | 4 | 4 | 5 | 5 | 18 | 10.7 |
| Enterococcus species | 3 | 3 | 1 | 2 | 9 | 5.4 |
| Klebsiella pneumoniae | 4 | 10 | 6 | 10 | 30 | 17.9 |
| Pseudomonas aeruginosa | 9 | 5 | 2 | 9 | 25 | 14.9 |
| Other gram negative bacilli | 7 | 6 | 11 | 11 | 35 | 20.9 |
| Candida albicans | 2 | 1 | 1 | 1 | 5 | 2.9 |
| Total | 168 * | |||||
| MDR and XDR ** bacteria | 9 | 9 | 4 | 4 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Soto Hernández, J.L.; González, L.E.R.; Ramírez, G.R.; Hernández, C.H.; Torreblanca, N.R.; Morales, V.Á.; Moreno, K.F.; Peek, M.R.; Jiménez, S.M. The Impact of the COVID-19 Pandemic in Postoperative Neurosurgical Infections at a Reference Center in México. Antibiotics 2023, 12, 1055. https://doi.org/10.3390/antibiotics12061055
Soto Hernández JL, González LER, Ramírez GR, Hernández CH, Torreblanca NR, Morales VÁ, Moreno KF, Peek MR, Jiménez SM. The Impact of the COVID-19 Pandemic in Postoperative Neurosurgical Infections at a Reference Center in México. Antibiotics. 2023; 12(6):1055. https://doi.org/10.3390/antibiotics12061055
Chicago/Turabian StyleSoto Hernández, José Luis, Luis Esteban Ramírez González, Guadalupe Reyes Ramírez, Carolina Hernández Hernández, Natalia Rangel Torreblanca, Verónica Ángeles Morales, Karen Flores Moreno, Miguel Ramos Peek, and Sergio Moreno Jiménez. 2023. "The Impact of the COVID-19 Pandemic in Postoperative Neurosurgical Infections at a Reference Center in México" Antibiotics 12, no. 6: 1055. https://doi.org/10.3390/antibiotics12061055