
Clinical Equivalence between Generic Versus Branded Antibiotics: Systematic Review and Meta-Analysis

Abstract
:1. Introduction
2. Method
2.1. Study Design
- P (population): Individuals who received antibiotics for prophylaxis and/or therapy for bacterial infections;
- I (intervention): Prescribing antibiotics for prophylaxis and/or treatment of infections based on syndromic or microbiological diagnosis;
- C (comparison): Generic antibiotics, defined as those drugs with proven bioequivalence to the branded drug;
- O (outcomes): The primary outcomes of interest are clinical cure, microbiological cure, and mortality. Secondary outcomes are adverse events switch-back rate, adherence, pharmacotherapy drop-out, hospital admission, and recurrent prescription of antibiotics.
2.2. Selection and Data Extraction
2.3. Risk of Bias
2.4. Synthesis of Results
2.5. Quality of the Evidence
3. Results
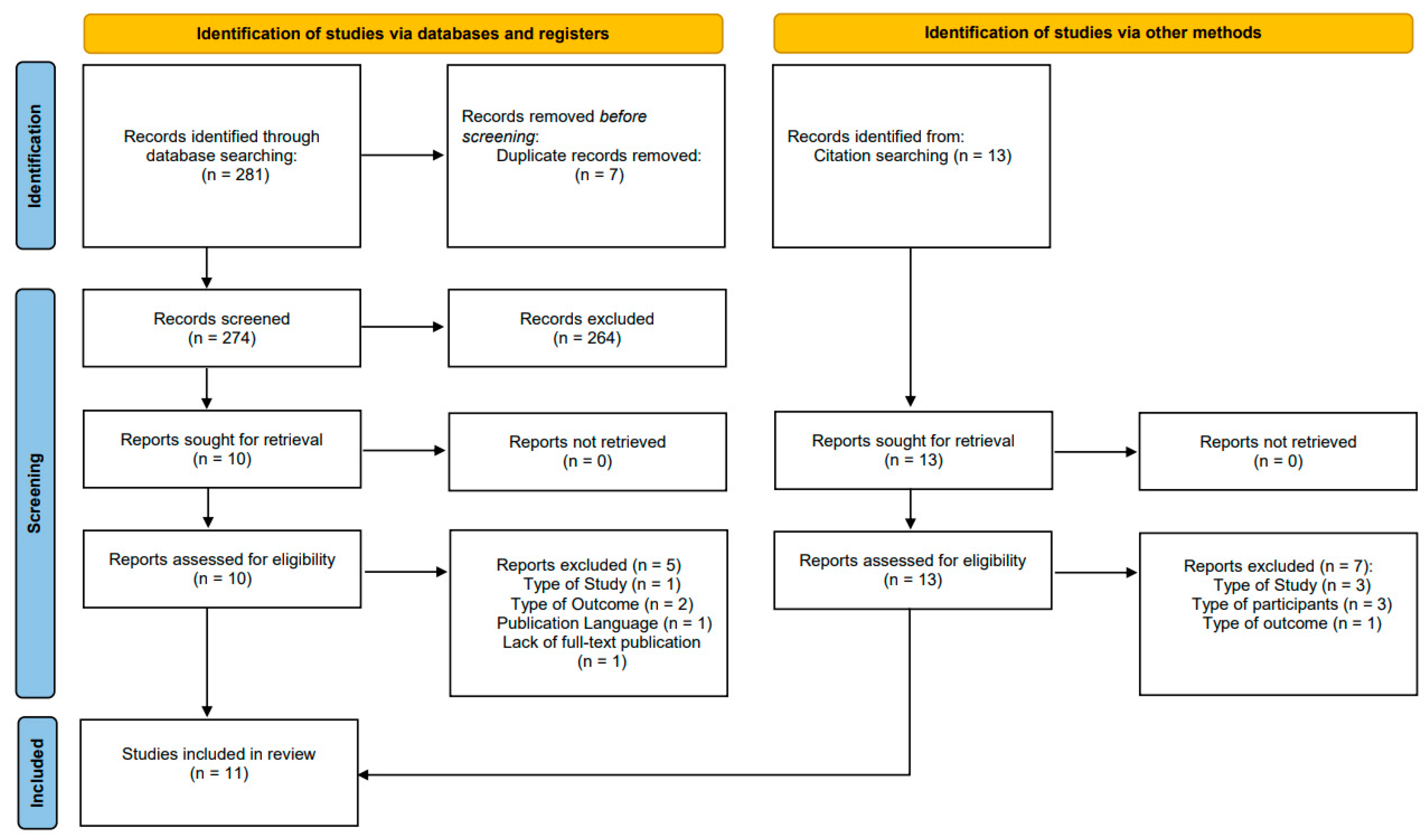
3.1. Study Selection
3.2. Characteristics of the Studies
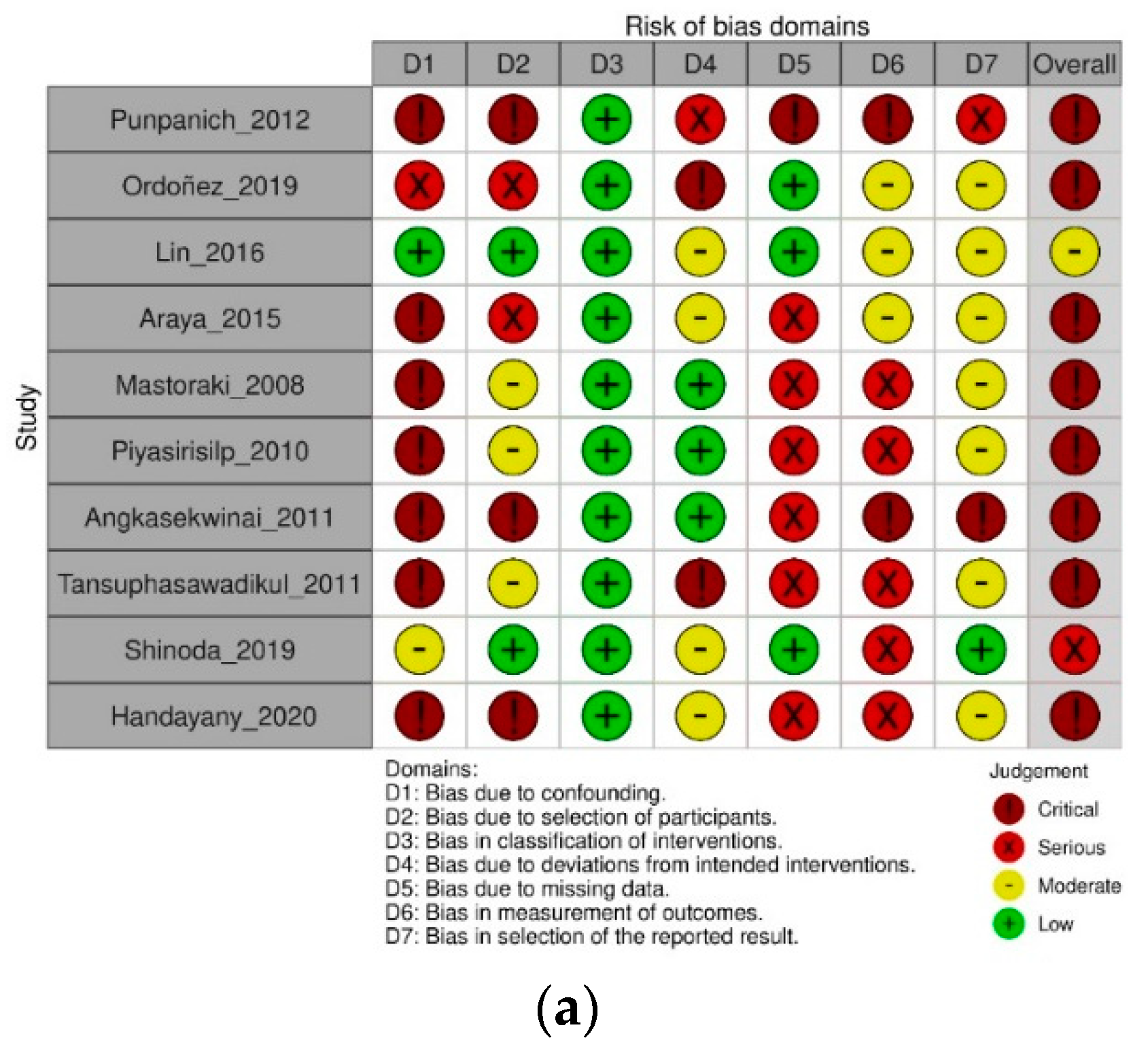
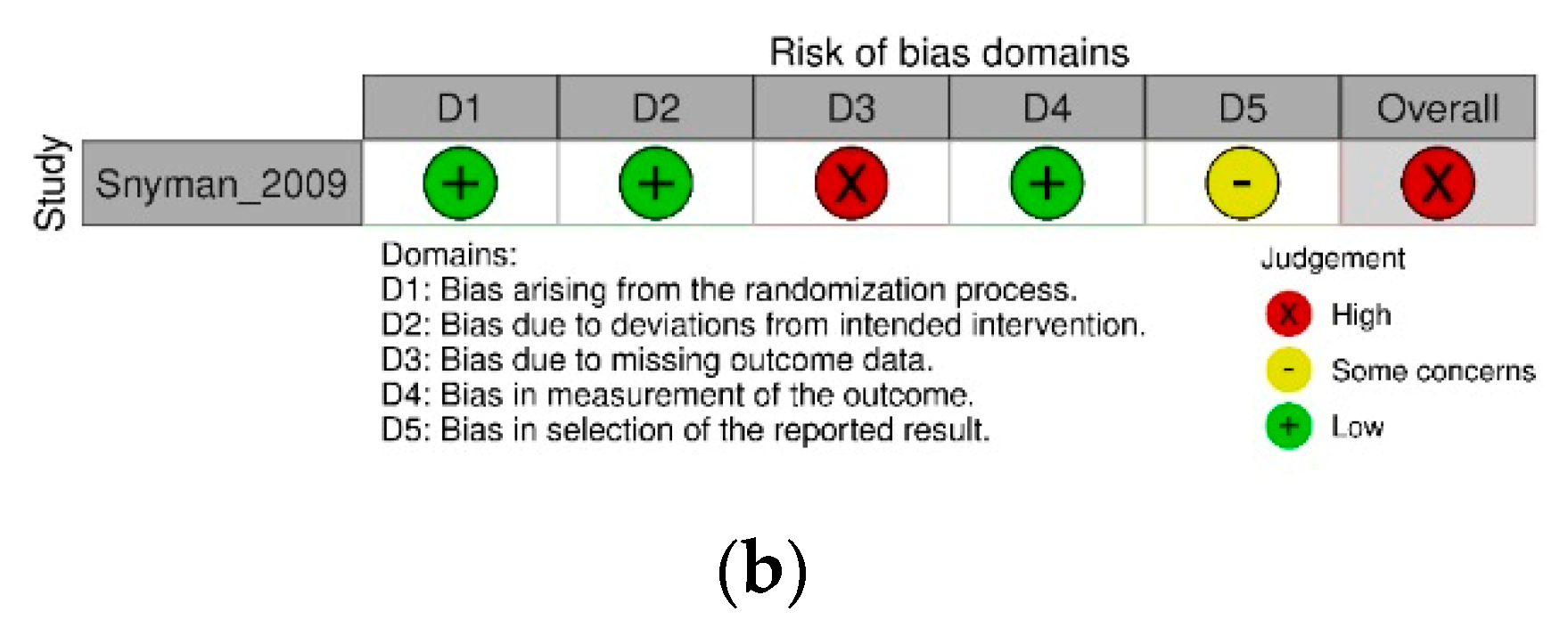
3.3. Risk of Bias
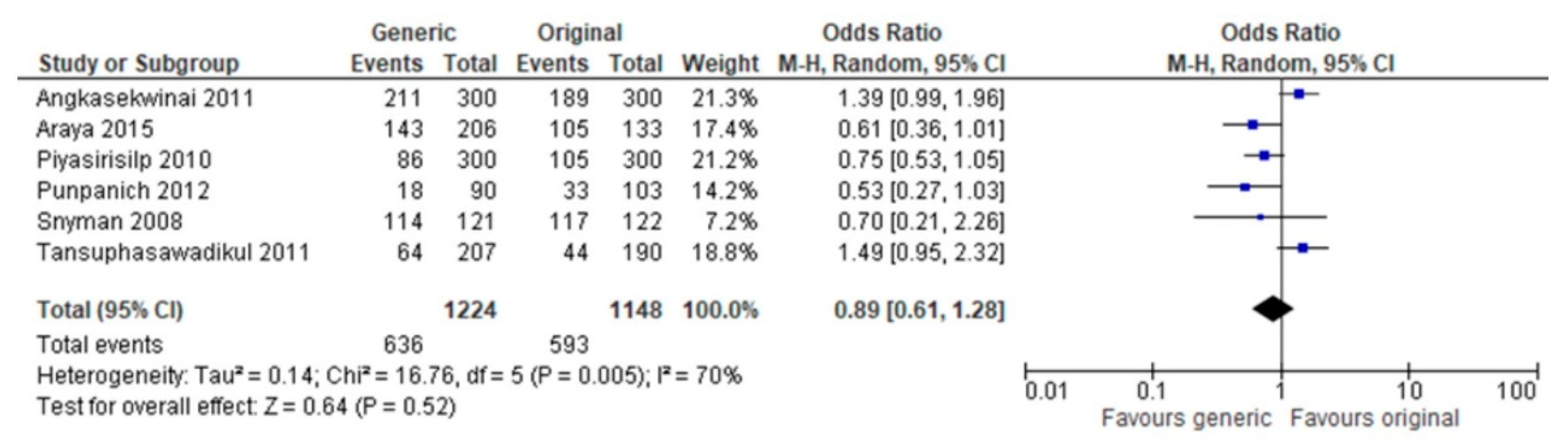
3.4. Summary of Results
3.5. Quality of Evidence

| Study | n | Male (%) | Age, Mean ± SD | Compared Drugs | Type of Infection | Design | Main Findings | Definitions | |
|---|---|---|---|---|---|---|---|---|---|
| Mastoraki et al. (2008) | Generic Branded | 305 313 | 259 (84.9%) 266 (85%) | 63.8 ± 7.7 64.3 ± 7.1 | Intravenous cefuroxime (Normafenac®), Intravenous cefuroxime (Zinacef®) Both received a 3 g single dose as surgical prophylaxis immediately before anesthetic induction. Complicated cases (as stated by authors) received a supplemental doses up to 12 h after the surgery. | Antibiotic prophylaxis before myocardial revascularization. | Quasi-experimental study (before–after). Patients received generic cefuroxime for 4 weeks and then branded cefuroxime for other another 4 weeks. Data were obtained retrospectively. | Surgical site infection rates, generic vs. branded (n = 31, 10.1% vs. n = 6, 1.9%, respectively) p < 0.0001. Total postoperative infections, generic vs. branded (n = 39, 12.8% vs. n = 8, 2.5%, respectively) p < 0.0001. Death associated with infection—not reported. Crude mortality—not reported. | Surgical site infection, local erythema of the skin and soft tissues and/or pus associated with fever or hypothermia, white blood cell count > 10,000/mm3, and positive culture. Infections at other body sites or fluids were defined based on guidelines from the Centers for Disease Control and Prevention. Diagnosis of sepsis was based on the ACCP/SCCM criteria. |
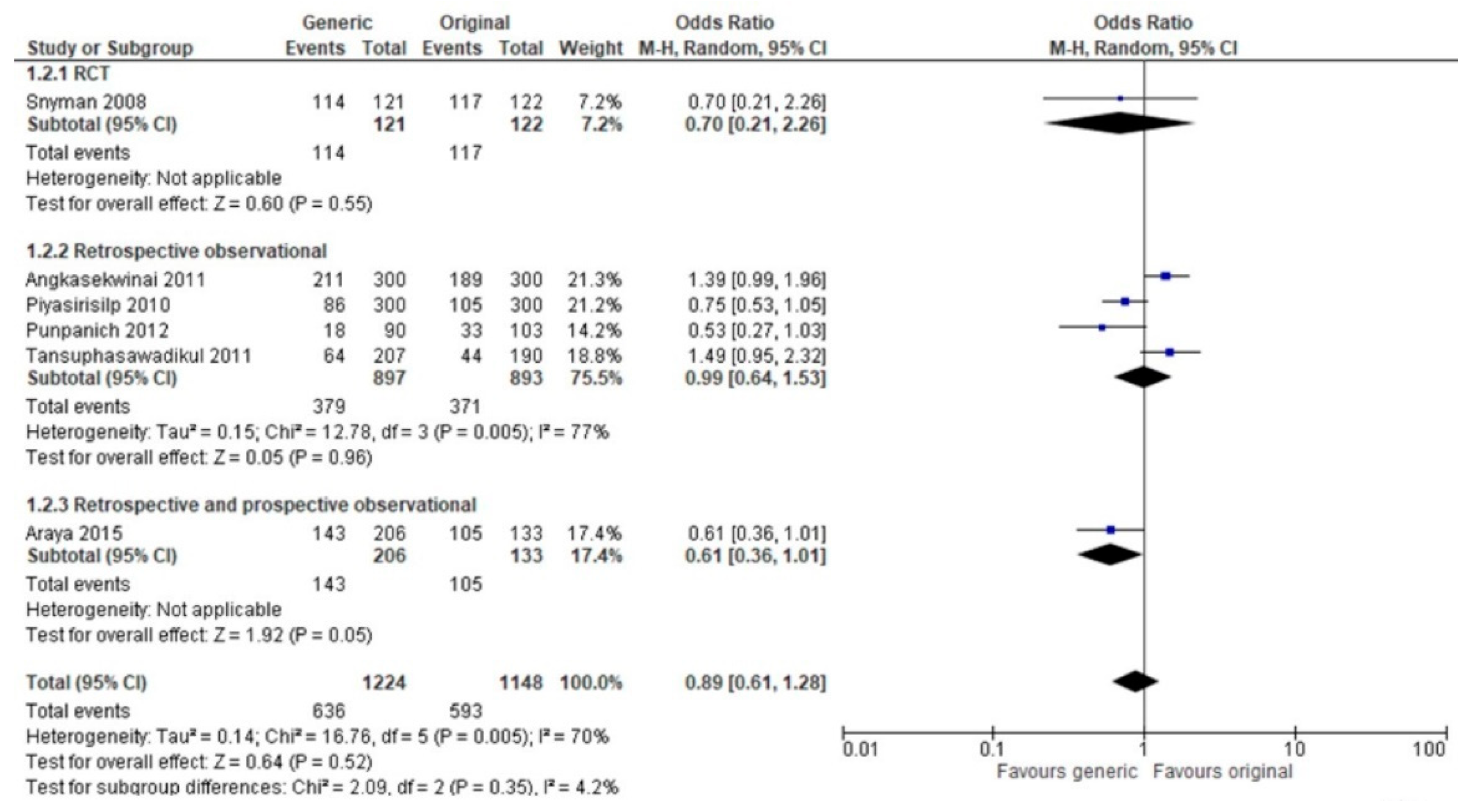
| Snyman et al. (2009) | Generic Branded | 141 136 | 64 (45%) 62 (46%) | 34.68 ± 10.02 35.49 ± 10.56 | Clarithromycin (Klarithran MR®), Ranbaxy Laboratories Ltd, Haryana, India Clarithromycin (Klacid XL®), Abbott Laboratories, Abbott Park, IL, USA 1 vs. 500 mg once a day, five days (tonsillitis); 1 vs. 500 mg once a day, for ten days (sinusitis and pneumonia). | Upper and lower respiratory infections. | Prospective randomize, comparative, investigator-blinded, and multicentric. | Clinical cure rate, (ITT), generic vs. branded (n = 114, 94.2% vs. n = 117, 95.9%, respectively) p = 0.57. Microbiological cure rate, generic vs. branded (n = 31, 79.5% vs. n = 39, 84.8%, respectively) p = 0.577. No deaths occurred during the study. | Clinical cure was defined as resolution of symptoms at the end of therapy. Respiratory specimens were collected at diagnosis and again at the follow-up visit to establish bacteriological cure, which was defined as eradication of the respiratory pathogen after the completion of antibacterial treatment. Sinusitis was diagnosed clinically and not confirmed with microbiological testing. |
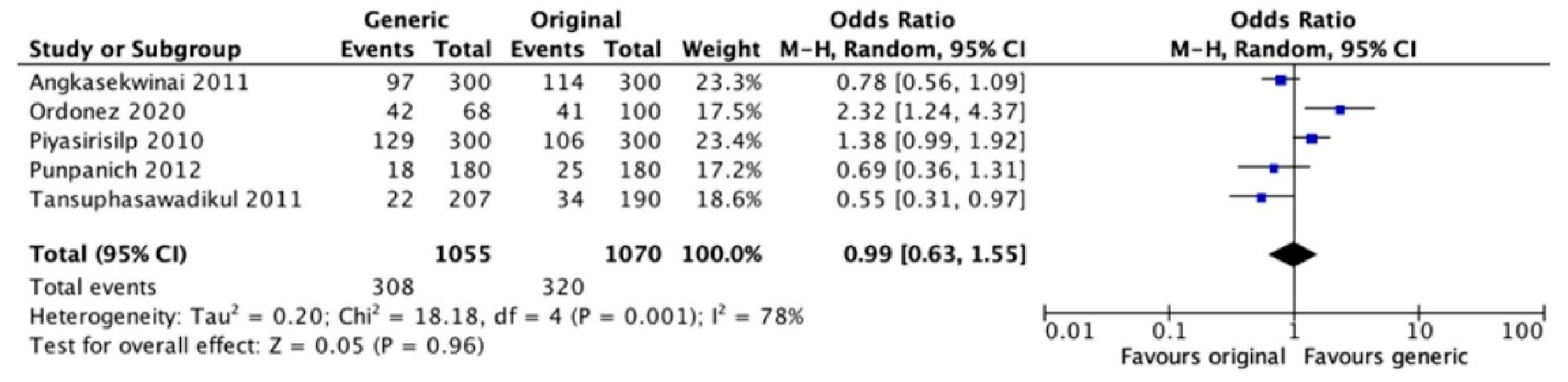
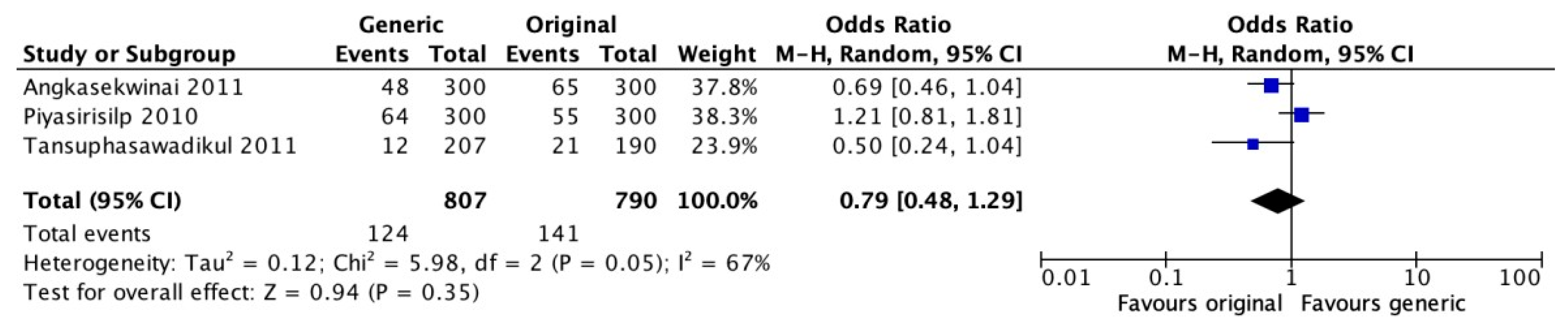
| Piyasirisilp et al. (2010) | Generic Branded | 300 300 | 154 (51.3%) 150 (50%) p = 0.81 | 66.5 ± 18 66.1 ± 17.8 p = 0.93 | Imipenem/cilastatin (Yungin®) Imipenem/cilastatin (Tienam®) | Different sites, including community acquired-infections and healthcare-acquired infections. | Observational, retrospective, descriptive. There were two cohorts with patients who received antimicrobials for treatment > 48 h with generic or branded in each. | Clinical cure rate, generic vs. branded (n = 86, 28.7% vs. n = 105, 35%, respectively) p = 0.09. Microbiological cure rate, generic vs. branded (n = 133, 44.3% vs. n = 147, 49%, respectively) p = 0.29. Death associated with infection, generic vs. branded (n = 64, 21.3% vs. n = 55, 18.3%, respectively) p = 0.41. Crude mortality generic vs. branded (n = 129, 43% vs. n = 106, 35.3%, respectively) p = 0.06. | Clinical cure, microbiological cure, and death associated with infection were not defined. Day at death associated with infections and crude mortality were not defined. |
| Tansuphasawadikul et al. (2011) | Generic Branded | 207 190 | 124 (59.9%) 104 (54.7%) p = 0.30 | 65.7 ± 16.9 67.2 ± 17 p = 0.39 | Mropenem (Mapenem®) Meropenem (Meronem®) | Different infection sites. | Retrospective cohort including inpatients. Multicentric. | Clinical cure rate at day 14, generic vs. branded (n = 64, 30.9% vs. n = 44, 23.2%, respectively) p = 0.08. Microbiological cure rate—not reported. Death associated with infection, generic vs. branded (n = 12, 5.8% vs. n = 21, 11.1%, respectively) p–not reported. Crude mortality, generic vs. branded (n = 22, 10.6% vs. n = 34, 17.9%, respectively) p–not reported. | Clinical cure was complete resolution of infection at day 14. Death associated with infection was not defined. Death was associated with infection and crude mortality at day 14. |
| Angkasekwinai et al. (2011) | Generic Branded | 300 300 | 164 (54.7%) 145 (48.3%) p = 0.12 | 61.7 ± 19.8 64.6 ± 17.8 p = 0.06 | Meropenem (Mapenem®) Meropenem (Meronem®) | Different sites, including community acquired-infections and healthcare-acquired infections. | Observational, retrospective, descriptive. There were two cohorts with patients who received antimicrobials for treatment > 48 h with generic or branded in each | Clinical cure rate, generic vs. branded (n = 211, 70.4% vs. n = 189, 63%, respectively) p = 0.07. Microbiological cure rate, generic vs. branded (n = 89, 29.7% vs. n = 69, 23%, respectively) p = 0.08. Death associated with infection, generic vs. branded (n =48, 16% vs. n = 65, 21,7%, respectively) p = 0.09. Crude mortality, generic vs. branded (n = 97, 32.3% vs. n = 114, 38%, respectively) p = 0.17. | Clinical cure was defined as cure and improvement at the end of treatment. Microbiological cure was not defined but described as eradicated. Death associated with infection was not defined. Day at death associated with infections and crude mortality were not defined. |
| Punpanich et al. (2012) | Generic Branded | 180 180 | 95 (52.8%) 100 (55.6%) p = 0.59 | 6.72 (42) 2.95 (22.3) p = 0.016 Age in months | Meropenem (Mapenem®) Meropenem (Meronem®) | Different infection sites. | Observational, retrospective, and descriptive, including inpatients from 0 to 18 years of age. | Clinical cure rate at day 14, generic vs. branded (n = 18, 20% vs. n = 33, 32%, respectively) p = 0.29. Microbiological cure rate at day 7, generic vs. branded (n = 17, 80.9% vs. n = 13, 81.3%, respectively) p = 0.98. Proportions of those with positive initial culture only. Death associated with infection—not reported. Crude mortality at day 28, generic vs. branded (10% vs. 13.9%, respectively) p = 0.152—no reported absolute numbers. | Clinical cure was complete resolution of infection at day 14. Only pathogens isolated in normally sterile sites or those with higher than 105 colony-forming units isolated in urine were regarded as true pathogens in the present study. Microbiological cure at day 7 of treatment. |
| Araya et al. (2015) | Generic Branded | 135 206 | 51% 47% p = 0.53 | 59 ± 15.6 60 ± 12.6 p = 0.37 | Cefoperazone-sulbactam (Cefactam®), Imipenem-cilastatine (Imipen®), and Piperaciline-tazobactam (Piperazam®), Libra Laboratories Cefoperazone-sulbactam (Sulperazone®), Pfizer Laboratories Imipenem-cilastatine (Tienam®), Merck Sharp & Dohme Corporation and Piperaciline-tazobactam (Tazonam®), Wyeth Laboratories | Different infection sites. | Comparative case series. | Clinical cure rate, all antibiotics, generic vs. branded (n = 105, 79% vs. n = 143, 69.5%, respectively) p = 0.10. Microbiological cure rate–not reported. Death associated with infection–not reported Crude mortality–not reported | Clinical cure not defined. |
| Lin et al. (2017) | Generic Branded | 6900 2294 | 986 (14.3%) 492 (21.5%) p < 0.0001 | Age (year) group: n 20–44: 3155 (45.7%) 45–64: 2549 (36.9%) ≥ 65: 1196 (17.3%) 20–44: 936 (40.8%) 45–6: 867 (37.8%) ≥ 65:91 (21.4%) p < 0.0001 | Trimethoprim-sulfamethoxazole and pipemidic acid | Uncomplicated urinary tract infection. | Population-based retrospective cohort. “Failure” was assumed for those patients who were discharged from the emergency department (ER) with antimicrobials (generic or branded) for the treatment of uncomplicated urinary tract infections and required an additional outpatient visit for continuation of antimicrobials. | Treatment failure: ER or hospitalization due to UTI and required antibiotics generic vs. branded (n = 142, 2.1% vs. n = 78, 3.4%, respectively) p = 0.85. Further outpatient visit due to UTI and required antibiotics generic vs. branded (n = 1096, 16.2% vs. n = 351, 15.8%, respectively) p = 0.5. Microbiological cure rate—not reported. Death associated with infection—not reported. Crude mortality—not reported. | Treatment failure was determined in two ways: (i) an ER visit or hospitalization due to a UTI with antibiotic prescription within 42 days of the index consultation and (ii) an additional outpatient visit for a UTI requiring antibiotic treatment within 42 days of the completion of the original antibiotic therapy. Those who met the criteria of treatment failure (i) would not be enrolled for analysis of treatment failure (ii). |
| Shinoda et al. (2019) | Generic Branded | 44 44 | 24 (55%) 25 (57%) | 70.4 ± 13.2 74.4 ± 9.1 p = 0.19 | Teicoplanin, Nanopia TDM Teicoplanin (Sekisui Medical Co. Ltd.) Teicoplanin, Targocid (Sanofi Co. Ltd.) | Not reported. | Observational, retrospective. | Initial mean serum concentration, generic vs. branded (12.8 mg/L vs. 16.3 mg/L, respectively) p < 0.01. Discontinuation rates due to adverse events, generic vs. branded (n = 1, 2.3% vs. n = 3, 4.8%, respectively) p = 0.64. Microbiological cure rate—not reported Death associated with infection—not reported. Crude mortality—not reported. | Discontinuation rate due to adverse events was determined by chart review. |
| Ordonez et al. (2019) | Generic Branded | 68 100 | 42 (62%) 54 (54%) | 58.6 ± 19.7 56.47 ± 17.45 | Meropenem Meropenem (Meronem®) | Different infection sites. | Observational, retrospective, descriptive. Two cohorts of intensive care unit patients with meropenem susceptible Gram-negative bacilli infections. | Clinical cure rate—not reported. Microbiological cure rate—not reported. Death associated with infection—not reported. Crude mortality, generic vs. branded (n = 42, 62% vs. n = 41, 41%, respectively) p = 0.008. | Crude mortality at day 28. |
| Haydayany et al. (2020) | Generic Branded | 34 33 | Total: 37.3% masculine | Not reported | Ciprofloxacin Ciprofloxacin (Tequinol®) | Typhoid fever, | Observational, retrospective, descriptive. This study included patients from 15 to 60 years of age with a documented diagnosis of typhoid fever who received generic or branded antimicrobials. | The duration of fever reduction for patients using the Tequinol® brand ranged from 1 to 3 days and for patients using ciprofloxacin generic ranged 3–7 days. Microbiological cure rate—not reported, Death associated with infection—not reported. Crude mortality—not reported. | Clinical cure defined as duration of fever reduction. |
4. Discussion
5. Conclusions
6. Registration and Protocol
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
Appendix A
Search Strategy
References
- Hill, A.M.; Barber, M.J.; Gotham, D. Estimated costs of production and potential prices for the WHO Essential Medicines List. BMJ Glob. Health 2018, 3, e000571. [Google Scholar] [CrossRef] [PubMed]
- Tattevin, P.; Crémieux, A.C.; Rabaud, C.; Rémy, G. Efficacy and Quality of Antibacterial Generic Products Approved for Human Use: A Systematic Review. Clin. Infect. Dis. 2014, 58, 458–469. [Google Scholar] [CrossRef] [PubMed]
- Li, D.G.; Najafzadeh, M.; Kesselheim, A.S.; Mostaghimi, A. Spending on World Healtch Organization essential medicines in Medicare Part D, 2011–2015: Retrospective cost analysis. MNJ 2019, 366, 142–157. [Google Scholar]
- Câmara de Regulação do Mercado de Medicamentos Conselho de Ministros Resolução CMED Nº 2, de 5 Março de 2004 (Alterada pela Resolução CMED nº 4, de 15 de Junho de 2005, Publicada no DOU, de 7 October 2005 e pela Resolução CMED nº 4, de 18 de Dezembro de 2006, Publicada no DOU, 12 March 2007). Available online: https://www.gov.br/anvisa/pt-br/assuntos/medicamentos/cmed/air/arquivos/5517json-file-1/view (accessed on 30 June 2022).
- Gauzit, R.; Lakdhari, M. Generic antibiotic drugs: Is effectiveness guaranteed? Med. Mal. Infect. 2012, 42, 141–148. [Google Scholar] [CrossRef]
- Snyman, J.R.; Schoeman, H.S.; Grobusch, M.P.; Henning, M.; Rabie, W.; Hira, M.; Parshotam, K.; Mithal, Y.; Singh, S.; Ramdas, Z. Generic versus Non- Generic Formulation of Extended-Release Clarithromycin in Patients with Community-Acquired Respiratory Tract Infections a Prospective, Randomized, Comparative, Investigator-Blind, Multicentre Study. Clin. Drug. Invest. 2009, 29, 265–274. [Google Scholar] [CrossRef]
- Meredith, P.A. Potential concerns about generic substitution: Bioequivalence versus therapeutic equivalence of different amlodipine salt forms. Curr. Med. Resarch Opin. 2009, 25, 2179–2189. [Google Scholar] [CrossRef]
- Tacca, M.D.; Pasqualetti, G.; Di Paolo, A.; Virdis, A.; Massimetti, G.; Gori, G.; Versari, D.; Taddei, S.; Blandizzi, C. Lack of pharmacokinetic bioequivalence between generic and branded amoxicilina formulations. A pos-marketing clinical study on healthy volunteers. Br. J. Clin. Pharm. 2009, 68, 34–42. [Google Scholar] [CrossRef]
- Lira, C.A.B.; Oliveira, J.N.S.; Andrade, M.S.; Vancini-Campanharo, R.; Vancini, R.L. Knowledge, perceptions and use of generic drugs: A cross sectional study. Einstein 2014, 12, 267–273. [Google Scholar] [CrossRef]
- Associação Brasileira das Indústrias de Medicamentos Genéricos-PróGenéricos. Mercado. Available online: http://www.progenericos.org.br/index.php/mercado (accessed on 30 June 2022).
- Decreto nº 9.787 de 10 de Fevereiro de 1999. Altera a Lei no 6.360, de 23 de Setembro de 1976, que Dispõe sobre a Vigilância Sanitária, Estabelece o Medicamento Genérico, Dispõe sobre a Utilização de nomes Genéricos em Produtos Farmacêuticos e dá outras Providências, Brasília, DF, Fevereiro 1999. Available online: http://www.planalto.gov.br/ccivil_03/LEIS/L9787.htm (accessed on 30 June 2022).
- Scaglione, F.; Paraboni, L. Influence of pharmacokinetics/pharmacodynamics of antibacterials in their dosing regimen selection. Expert. Rev. Anti. Infect. 2006, 4, 479–490. [Google Scholar] [CrossRef]
- Chow, S.C.; Liu, J.P. Meta-analysis for bioequivalence review. J. Biopharm. Stat. 1997, 7, 97–111. [Google Scholar] [CrossRef]
- Raw, A.S.; Furness, M.S.; Gill, D.S.; Adams, R.C.; Holcombre, F.O.; Yu, L.X. Regulatory considerations of pharmaceutical solid polymorphism in Abbreviated New Drug Applications (ANDAs). Adv. Drug Deliv. Rev. 2004, 56, 397–414. [Google Scholar] [CrossRef] [PubMed]
- Reshetko, O.V.; Lutsevich, K.A. Molecular-Biological problems of drug design and mechanism of drug action. Individual bioequivalence: Concept, research, and variability (a review). Pharm. Chem. J. 2009, 43, 431–435. [Google Scholar] [CrossRef]
- Timsit, J.F.; de Kraker, M.E.A.; Sommer, H.; Weiss, E.; Bettiol, E.; Wolkewitz, M.; Nikolakopoulos, S.; Wilson, D.; Harbarth, S.; COMBACTE-NET Consortium. Appropriate endpoints for evaluation of new antibiotic therapies for severe infections: A perspective from COMBACTE’s STAT-Net. Intensive Care Med. 2017, 43, 1002–1012. [Google Scholar] [CrossRef] [PubMed]
- Egger, M.; Davey Smith, G.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [PubMed]
- Harbord, R.M.; Egger, M.; Sterne, J.A. A modified test for small-study effects in meta-analyses of controlled trials with binary endpoints. Stat. Med. 2006, 25, 3443–3457. [Google Scholar] [CrossRef]
- Peters, J.L.; Sutton, A.J.; Jones, D.R.; Abrams, K.R.; Rushton, L. Comparison of two methods to detect publication bias in meta-analysis. JAMA 2006, 295, 676–680. [Google Scholar] [CrossRef]
- Guyatt, G.H.; Oxman, A.D.; Vist, G.E.; Kunz, R.; Falck-Ytter, Y.; Alonso-Coello, P.; Schünemann, H.J.; GRADE Working Group. GRADE: An emerging consensus on rating quality of evidence and strength of recommendations. BMJ 2008, 336, 924–926. [Google Scholar] [CrossRef]
- Angkasekwinai, N.; Werarak, P.; Chaiyasoot, K. Monitoring of Effectiveness and Safety of Generic Formulation of Meropenem for Treatment of Infections at Siriraj Hospital. J. Med. Assoc. Thai 2011, 94, 217–224. [Google Scholar]
- Araya, I.; Fasce, G.; Núñez, E.; Opazo, J.L.; Saez, E.; Hurtado, V.; Contreras, S.; Quiñones, L.A. A Non-inferiority Pilot Study Comparing the Clinical Efficacy and Safety of Generic Wide-spectrum Antibiotic Use in Septic Oncology Patients. Drug Res. 2015, 65, 635–639. [Google Scholar] [CrossRef]
- Punpanich, W.; Srisarang, S.; Prachantasen, U. Therapeutic Effectiveness of the Generic Preparation of Meropenem (Mapenem®) in the Treatment of Moderate to Severe Infection in Children. J. Med. Assoc. Thai 2012, 95, 895–902. [Google Scholar]
- Lin, Y.S.; Jan, I.S.; Cheng, S.H. Comparative analysis of the cost and effectiveness of generic and brand-name antibiotics: The case of uncomplicated urinary tract infection. Pharmacoepidemiol. Drug Saf. 2016, 26, 301–309. [Google Scholar] [CrossRef] [PubMed]
- Mastoraki, E.; Michalopoulos, A.; Kriaras, I. Incidence of postoperative infections in patients undergoing coronary artery bypass grafting surgery receiving antimicrobial prophylaxis with original and generic cefuroxime. J. Infection 2008, 56, 35–39. [Google Scholar] [CrossRef] [PubMed]
- Handayany, G.N.; Mulat, T.C.; Irawaty, I.; Mallongi, A. Comparison of Success Management Effect of Therapy Use of Generic Drugs and Branded Drugs in Typhoid Fever Patients in Installation of Inpatients. Maced. J. Med. Sci. 2020, 8, 67–70. [Google Scholar] [CrossRef]
- Piyasirisilp, S.; Premprawat, W.; Thamlikitkul, V. Therapeutic Equivalence of Generic Imipenem/Cilastatin for Therapy of Infections at Siriraj Hospital. J. Med. Assoc. Thai 2010, 93, 117–125. [Google Scholar]
- Tansuphasawadikul, S.; Simaroj, S.; Chantarothorn, S.; Nuntachit, N.; Jutivorakool, K.; Munsakul, W.; Yomtem, K.; Tangkosakul, T.; Wannasunthornchai, S. Therapeutic Effectiveness of a Generic versus Original Meropenem in Serious Infections. J. Med. Assoc. Thai 2011, 94, 172–178. [Google Scholar]
- Shinoda, R.; Shinoda, Y.; Ohashi, K.; Matsuoka, T.; Hirose, T.; Sugiyama, T.; Yoshimura, T. Single-centre retrospective observational study comparing trough blood concentration and safety of teicoplanin formulations. J. Infect. Chemother. 2019, 25, 563–566. [Google Scholar] [CrossRef]
- Ordónez, K.; Feinstein, M.; Reyes, S.; Hernández-Gómez, C.; Pallares, C.; Villegas, M.V. Clinical and economic impact of generic versus brand name meropenem use in an intensive care unit in Colombia. Braz. J. Infect. Dis. 2019, 23, 237–245. [Google Scholar] [CrossRef]
- Vesga, O.; Agudelo, M.; Salazer, B.E.; Rodrigues, C.A.; Zuluaga, E.F. Generic vancomycin products fail in vivo despite being pharmaceutical equivalents of the innovator. Antimicrob. Ag. Chemother. 2010, 54, 3271–3279. [Google Scholar] [CrossRef]
- Buckley, G.J.; Gostin, L.O. Countering the Problem of Falsified and Substandard Drug; National Academies Press: Washington, DC, USA, 2013; 314p, ISBN 978-0-309-26939-1. ISBN 0-309-26939-3. [Google Scholar]
- Moet, G.J.; Watters, A.A.; Sader, H.S.; Jones, R.N. Expanded studies of piperacillin/tazobactam formulations: Variations among branded product lots and assessment of 46 generic lots. Diagn. Microbiol. Infect. Dis. 2009, 65, 319–322. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cotia, A.; Oliveira Junior, H.A.; Matuoka, J.Y.; Boszczowski, Í. Clinical Equivalence between Generic Versus Branded Antibiotics: Systematic Review and Meta-Analysis. Antibiotics 2023, 12, 935. https://doi.org/10.3390/antibiotics12050935
Cotia A, Oliveira Junior HA, Matuoka JY, Boszczowski Í. Clinical Equivalence between Generic Versus Branded Antibiotics: Systematic Review and Meta-Analysis. Antibiotics. 2023; 12(5):935. https://doi.org/10.3390/antibiotics12050935
Chicago/Turabian StyleCotia, André, Haliton Alves Oliveira Junior, Jessica Y. Matuoka, and Ícaro Boszczowski. 2023. "Clinical Equivalence between Generic Versus Branded Antibiotics: Systematic Review and Meta-Analysis" Antibiotics 12, no. 5: 935. https://doi.org/10.3390/antibiotics12050935