
Identifying Predictors Associated with Risk of Death or Admission to Intensive Care Unit in Internal Medicine Patients with Sepsis: A Comparison of Statistical Models and Machine Learning Algorithms

 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Patients and Methods
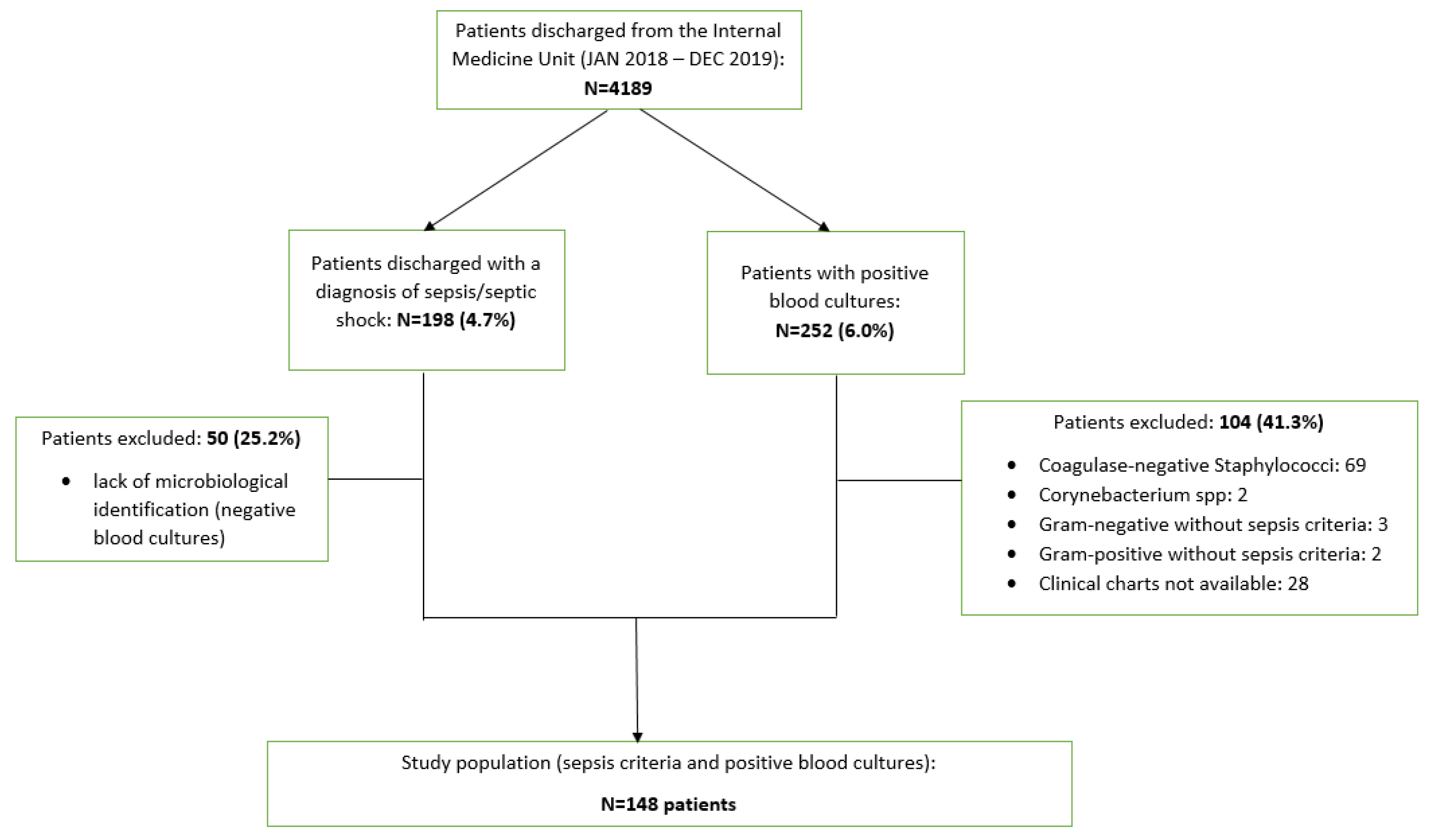
2.1. Patients
2.2. Methods
2.3. Statistical Analysis
3. Results
3.1. Demographic and Anamnestic Characteristics of Patients at Enrollment
3.2. Building Classical Statistical Models and Machine Learning Algorithms for Mortality and/or ICU Transfer Risk Prediction
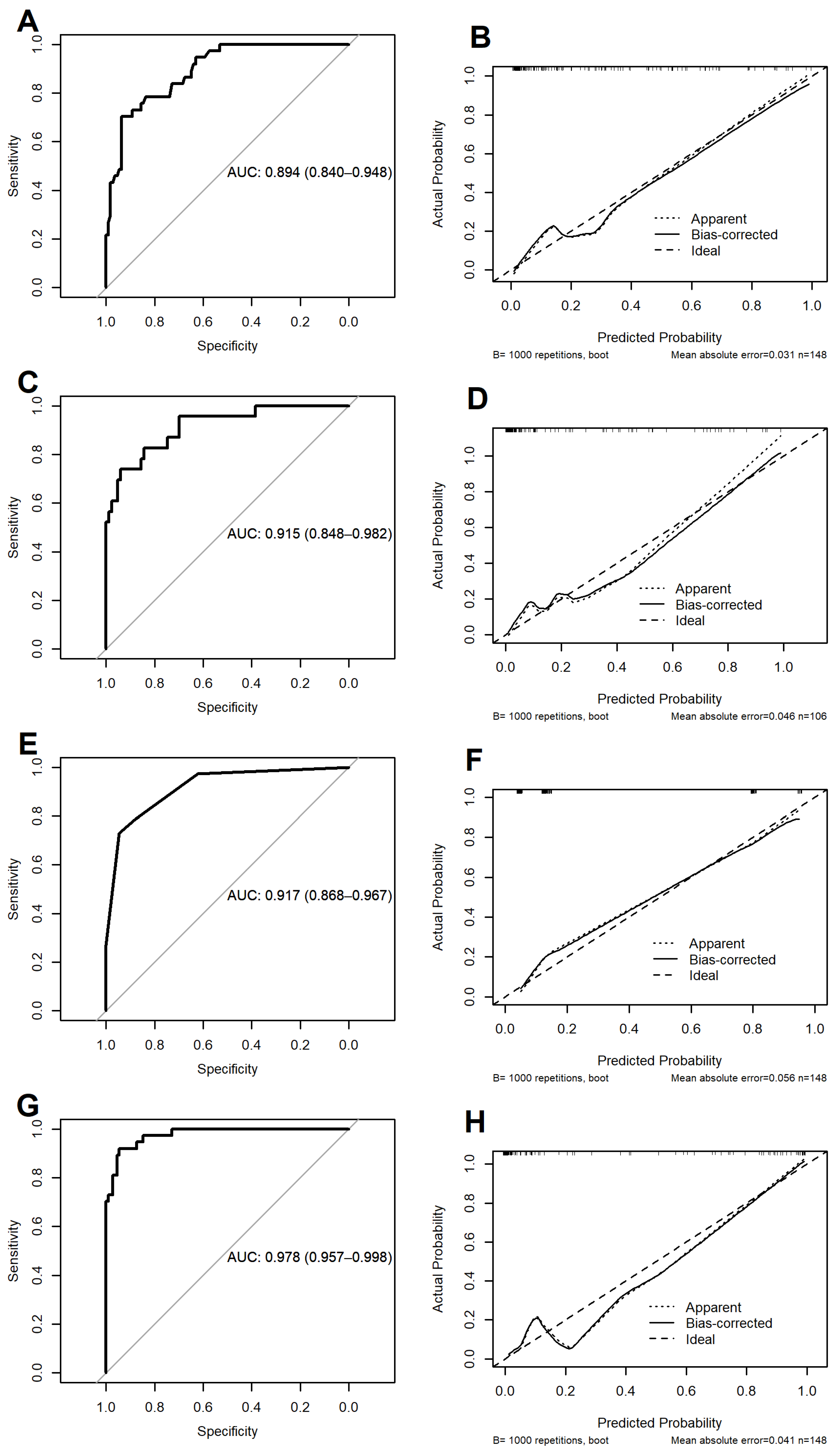
3.2.1. METHOD 1: Multivariable Logistic Model Using the Stepwise Variable Selection Procedure
3.2.2. METHOD 2: Cross-Validated Multivariable Logistic Model with LASSO Penalty
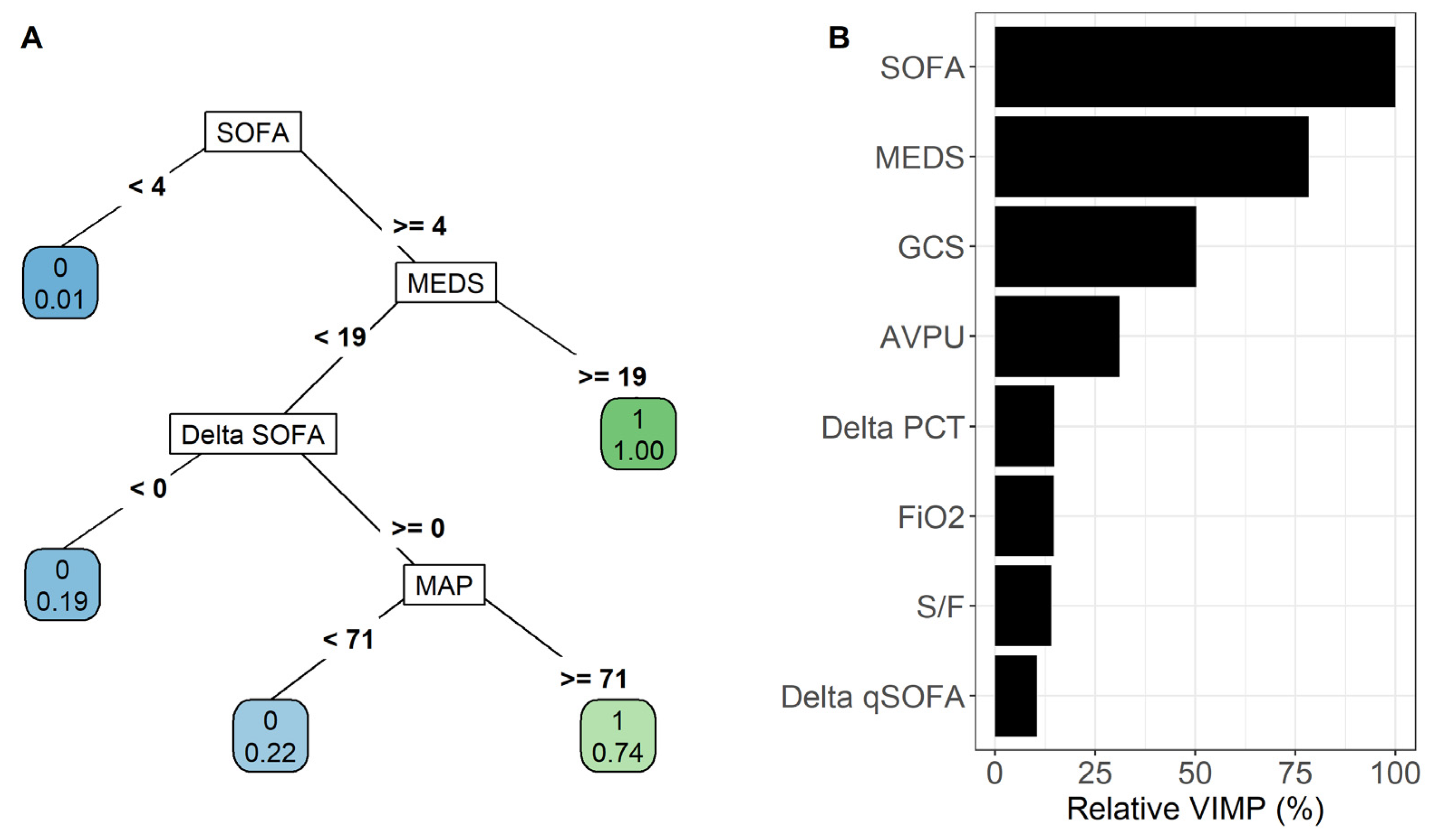
3.2.3. METHOD 3: Recursive Partitioning and Regression Tree
3.2.4. METHOD 4: Random Forest
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.D.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef] [PubMed]
- Rudd, K.E.; Johnson, S.C.; Agesa, K.M.; Shackelford, K.A.; Tsoi, D.; Kievlan, D.R.; Colombara, D.V.; Ikuta, K.S.; Kissoon, N.; Finfer, S.; et al. Global, regional, and national sepsis incidence and mortality, 1990–2017: Analysis for the Global Burden of Disease Study. Lancet 2020, 395, 200–211. [Google Scholar] [CrossRef] [PubMed]
- Rhee, C.; Dantes, R.; Epstein, L.; Murphy, D.J.; Seymour, C.W.; Iwashyna, T.J.; Kadri, S.S.; Angus, D.C.; Danner, R.L.; Fiore, A.E.; et al. CDC Prevention Epicenter Program. Incidence and Trends of Sepsis in US Hospitals Using Clinical vs Claims Data, 2009-2014. JAMA 2017, 318, 1241–1249. [Google Scholar] [CrossRef]
- Zaccone, V.; Tosoni, A.; Passaro, G.; Vallone, C.V.; Impagnatiello, M.; Li Puma, D.D.; De Cosmo, S.; Landolfi, R.; Mirijello, A. Internal Medicine Sepsis Study Group. Sepsis in Internal Medicine wards: Current knowledge, uncertainties and new approaches for management optimization. Ann. Med. 2017, 49, 582–592. [Google Scholar] [CrossRef]
- Reinhart, K.; Daniels, R.; Kissoon, N.; Machado, F.R.; Schachter, R.D.; Finfer, S. Recognizing Sepsis as a Global Health Priority—A WHO Resolution. N. Engl. J. Med. 2017, 377, 414–417. [Google Scholar] [CrossRef] [PubMed]
- Esteban, A.; Frutos-Vivar, F.; Ferguson, N.D.; Peñuelas, O.; Lorente, J.A.; Gordo, F.; Honrubia, T.; Algora, A.; Bustos, A.; García, G.; et al. Sepsis incidence and outcome: Contrasting the intensive care unit with the hospital ward. Crit. Care Med. 2007, 35, 1284–1289. [Google Scholar] [CrossRef] [PubMed]
- Mirijello, A.; Tosoni, A.; On Behalf Of The Internal Medicine Sepsis Study Group. New Strategies for Treatment of Sepsis. Medicina 2020, 56, 527. [Google Scholar] [CrossRef]
- Mirijello, A.; Tosoni, A.; Zaccone, V.; Impagnatiello, M.; Passaro, G.; Vallone, C.V.; Cossari, A.; Ventura, G.; Gambassi, G.; De Cosmo, S.; et al. Internal Medicine Sepsis Study Group. MEDS score and vitamin D status are independent predictors of mortality in a cohort of Internal Medicine patients with microbiological identified sepsis. Eur. Rev. Med. Pharmacol. Sci. 2019, 23, 4033–4043. [Google Scholar]
- Papadimitriou-Olivgeris, M.; Psychogiou, R.; Garessus, J.; Camaret, A.; Fourre, N.; Kanagaratnam, S.; Jecker, V.; Nusbaumer, C.; Monnerat, L.B.; Kocher, A.; et al. Predictors of mortality of bloodstream infections among internal medicine patients in a Swiss Hospital: Role of quick Sequential Organ Failure Assessment. Eur. J. Intern. Med. 2019, 65, 86–92. [Google Scholar] [CrossRef]
- Mazzone, A.; Dentali, F.; La Regina, M.; Foglia, E.; Gambacorta, M.; Garagiola, E.; Bonardi, G.; Clerici, P.; Concia, E.; Colombo, F.; et al. Clinical Features, Short-Term Mortality, and Prognostic Risk Factors of Septic Patients Admitted to Internal Medicine Units: Results of an Italian Multicenter Prospective Study. Medicine 2016, 95, e2124. [Google Scholar] [CrossRef]
- Belfiore, A.; Mastroianni, F.; Ventrella, F.; Errico, M.; Suppressa, P.; Tomai, M.; Sabatino, S.; De Palma, G.; Pappagallo, F.; Erbi, A.; et al. Epidemiology of sepsis in Internal Medicine Units of Apulia: Results of SEMINA (SEpsis Management in INternal medicine Apulia) study. Ann. Ig. 2023, 35, 282–296. [Google Scholar] [PubMed]
- Bautista Hernández, A.; de Vega-Ríos, E.; Serrano Ballesteros, J.; Useros Braña, D.; Cardeñoso Domingo, L.; Figuerola Tejerina, A.; Jiménez Jiménez, D.; de Los Santos Gil, I.; Sáez Béjar, C. Impact of the implementation of a Sepsis Code Program in medical patient management: A cohort study in an Internal Medicine ward. Rev. Esp. Quimioter. 2022, 35, 178–191. [Google Scholar] [CrossRef] [PubMed]
- Mirijello, A.; Tosoni, A. Sepsis: New Challenges and Future Perspectives for an Evolving Disease-Precision Medicine Is the Way! Medicina 2021, 57, 1109. [Google Scholar] [CrossRef] [PubMed]
- Torvik, M.A.; Nymo, S.H.; Nymo, S.H.; Bjørnsen, L.P.; Kvarenes, H.W.; Ofstad, E.H. Patient characteristics in sepsis-related deaths: Prevalence of advanced frailty, comorbidity, and age in a Norwegian hospital trust. Infection 2023. [Google Scholar] [CrossRef]
- Kaukonen, K.M.; Bailey, M.; Suzuki, S.; Pilcher, D.; Bellomo, R. Mortality related to severe sepsis and septic shock among critically ill patients in Australia and New Zealand, 2000-2012. JAMA 2014, 311, 1308–1316. [Google Scholar] [CrossRef]
- GBD 2019 Antimicrobial Resistance Collaborators. Global mortality associated with 33 bacterial pathogens in 2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2022, 400, 2221–2248. [Google Scholar] [CrossRef]
- Seymour, C.W.; Kennedy, J.N.; Wang, S.; Chang, C.H.; Elliott, C.F.; Xu, Z.; Berry, S.; Clermont, G.; Cooper, G.; Gomez, H.; et al. Derivation, Validation, and Potential Treatment Implications of Novel Clinical Phenotypes for Sepsis. JAMA 2019, 321, 2003–2017. [Google Scholar] [CrossRef]
- Tosoni, A.; Cossari, A.; Paratore, M.; Impagnatiello, M.; Passaro, G.; Vallone, C.V.; Zaccone, V.; Gasbarrini, A.; Addolorato, G.; De Cosmo, S.; et al. Delta-Procalcitonin and Vitamin D Can Predict Mortality of Internal Medicine Patients with Microbiological Identified Sepsis. Medicina 2021, 57, 331. [Google Scholar] [CrossRef]
- Tosoni, A.; Paratore, M.; Piscitelli, P.; Addolorato, G.; De Cosmo, S.; Mirijello, A.; Internal Medicine Sepsis Study Group. The use of procalcitonin for the management of sepsis in Internal Medicine wards: Current evidence. Panminerva Med. 2020, 62, 54–62. [Google Scholar] [CrossRef]
- Spoto, S.; Daniel Markley, J.; Valeriani, E.; Abbate, A.; Argemi, J.; Markley, R.; Fogolari, M.; Locorriere, L.; Anguissola, G.B.; Battifoglia, G.; et al. Active Surveillance Cultures and Procalcitonin in Combination with Clinical Data to Guide Empirical Antimicrobial Therapy in Hospitalized Medical Patients With Sepsis. Front. Microbiol. 2022, 13, 797932. [Google Scholar] [CrossRef]
- Spoto, S.; Cella, E.; de Cesaris, M.; Locorriere, L.; Mazzaroppi, S.; Nobile, E.; Lanotte, A.M.; Pedicino, L.; Fogolari, M.; Costantino, S.; et al. Procalcitonin and MR-Proadrenomedullin Combination with SOFA and qSOFA Scores for Sepsis Diagnosis and Prognosis: A Diagnostic Algorithm. Shock 2018, 50, 44–52. [Google Scholar] [CrossRef] [PubMed]
- Angus, D.C.; Linde-Zwirble, W.T.; Lidicker, J.; Clermont, G.; Carcillo, J.; Pinsky, M.R. Epidemiology of severe sepsis in the United States: Analysis of incidence, outcome, and associated costs of care. Crit. Care Med. 2001, 29, 1303–1310. [Google Scholar] [CrossRef] [PubMed]
- Vardi, M.; Ghanem-Zoubi, N.O.; Bitterman, H.; Abo-Helo, N.; Yurin, V.; Weber, G.; Laor, A. Sepsis in nonagenarians admitted to internal medicine departments: A comparative study of outcomes. QJM 2013, 106, 261–266. [Google Scholar] [CrossRef] [PubMed]
- Teasdale, G.; Jennett, B. Assessment of coma and impaired consciousness. A practical scale. Lancet 1974, 2, 81–84. [Google Scholar] [CrossRef] [PubMed]
- Hosmer, D. Applied Logistic Regression, 3rd ed.; Wiley: Hoboken, NJ, USA, 2013. [Google Scholar]
- Friedman, J.; Hastie, T.; Tibshirani, R. Regularization Paths for Generalized Linear Models via Coordinate Descent. J. Stat. Softw. 2010, 33, 1–22. [Google Scholar] [CrossRef]
- Breiman, L.; Friedman, J.H.; Olshen, R.A.; Stone, C.J. Classification and Regression Trees, 1st ed.; Routledge: Wadsworth, NY, USA, 1984. [Google Scholar]
- Breiman, L. Random forests. Mach. Learn. 2001, 45, 5–32. [Google Scholar] [CrossRef]
- Seymour, C.W.; Liu, V.X.; Iwashyna, T.J.; Brunkhorst, F.M.; Rea, T.D.; Scherag, A.; Rubenfeld, G.; Kahn, J.M.; Shankar-Hari, M.; Singer, M.; et al. Assessment of Clinical Criteria for Sepsis: For the Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 762–774. [Google Scholar] [CrossRef]
- Churpek, M.M.; Snyder, A.; Han, X.; Sokol, S.; Pettit, N.; Howell, M.D.; Edelson, D.P. Quick Sepsis-related Organ Failure Assessment, Systemic Inflammatory Response Syndrome, and Early Warning Scores for Detecting Clinical Deterioration in Infected Patients outside the Intensive Care Unit. Am. J. Respir. Crit. Care Med. 2017, 195, 906–911. [Google Scholar] [CrossRef]
- Saeed, K.; Wilson, D.C.; Bloos, F.; Schuetz, P.; van der Does, Y.; Melander, O.; Hausfater, P.; Legramante, J.M.; Claessens, Y.E.; Amin, D.; et al. The early identification of disease progression in patients with suspected infection presenting to the emergency department: A multi-centre derivation and validation study. Crit. Care 2019, 23, 40. [Google Scholar] [CrossRef]
- Spoto, S.; Fogolari, M.; De Florio, L.; Minieri, M.; Vicino, G.; Legramante, J.; Lia, M.S.; Terrinoni, A.; Caputo, D.; Costantino, S.; et al. Procalcitonin and MR-proAdrenomedullin combination in the etiological diagnosis and prognosis of sepsis and septic shock. Microb. Pathog. 2019, 137, 103763. [Google Scholar] [CrossRef]
- Pace, E.; Bracco, C.; Magnino, C.; Badinella Martini, M.; Serraino, C.; Brignone, C.; Testa, E.; Fenoglio, L.M.; Porta, M. Multidrug-Resistant Bloodstream Infections in Internal Medicine: Results from a Single-Center Study. South. Med. J. 2022, 115, 333–339. [Google Scholar] [CrossRef] [PubMed]
- Rayan, Z.; Alfonse, M.; Salem, A.-B.M. Machine learning approaches in smart health. Procedia Comput. Sci. 2019, 154, 361–368. [Google Scholar] [CrossRef]
- Zhang, Z.; Hong, Y. Development of a novel score for the prediction of hospital mortality in patients with severe sepsis: The use of electronic healthcare records with LASSO regression. Oncotarget 2017, 8, 49637–49645. [Google Scholar] [CrossRef] [PubMed]
- Taylor, R.A.; Pare, J.R.; Venkatesh, A.K.; Mowafi, H.; Melnick, E.R.; Fleischman, W.; Hall, M.K. Prediction of In-hospital Mortality in Emergency Department Patients With Sepsis: A Local Big Data-Driven, Machine Learning Approach. Acad. Emerg. Med. 2016, 23, 269–278. [Google Scholar] [CrossRef]
- Cheng, C.Y.; Kung, C.T.; Chen, F.C.; Chiu, I.M.; Lin, C.R.; Chu, C.C.; Kung, C.F.; Su, C.M. Machine learning models for predicting in-hospital mortality in patient with sepsis: Analysis of vital sign dynamics. Front. Med. 2022, 9, 964667. [Google Scholar] [CrossRef]
- Giamarellos-Bourboulis, E.J.; Tsaganos, T.; Tsangaris, I.; Lada, M.; Routsi, C.; Sinapidis, D.; Koupetori, M.; Bristianou, M.; Adamis, G.; Mandragos, K.; et al. Hellenic Sepsis Study Group. Validation of the new Sepsis-3 definitions: Proposal for improvement in early risk identification. Clin. Microbiol. Infect. 2017, 23, 104–109. [Google Scholar] [CrossRef]
- Shapiro, N.I.; Wolfe, R.E.; Moore, R.B.; Smith, E.; Burdick, E.; Bates, D.W. Mortality in Emergency Department Sepsis (MEDS) score: A prospectively derived and validated clinical prediction rule. Crit. Care Med. 2003, 31, 670–675. [Google Scholar] [CrossRef]
- Gamboa-Antiñolo, F.M. Prognostic tools for elderly patients with sepsis: In search of new predictive models. Intern. Emerg. Med. 2021, 16, 1027–1030. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Total (N = 148) | Outcome NO (N = 111) | Outcome YES (N = 37) | p-Value * | |
|---|---|---|---|---|
| Male gender | 77 (52%) | 55 (49%) | 22 (59.5%) | 0.296 |
| Type 2 diabetes mellitus | 40 (27.0%) | 27 (24.3%) | 13 (35.1%) | 0.200 |
| Residing in long term facilities | 26 (17.6%) | 14 (12.6%) | 12 (32.4%) | 0.006 |
| Age ≥ 65 years | 101 (68.2%) | 73 (65.8%) | 28 (75.7%) | 0.262 |
| Active neoplasm | 48 (32.4%) | 34 (30.6%) | 14 (37.8%) | 0.417 |
| End-stage illness | 55 (37.2%) | 32 (28.8%) | 23 (62.1%) | <0.001 |
| Hospitalization (previous 90 days) | 64 (43.2%) | 47 (42.3%) | 17 (45.9%) | 0.702 |
| COPD | 28 (18.9%) | 27 (24.3%) | 1 (2.7%) | 0.003 # |
| Respiratory failure | 42 (28.4%) | 24 (21.8%) | 18 (48.6%) | 0.002 |
| Chronic heart failure | 42 (28.4%) | 30 (27.0%) | 12 (32.4%) | 0.528 |
| Chronic kidney failure | 38 (25.7%) | 25 (22.5%) | 13 (35.1%) | 0.128 |
| Central venous catether | 60 (40.5%) | 42 (37.8%) | 18 (48.6%) | 0.246 |
| Haemodialysis | 3 (2.0%) | 0 (0%) | 3 (8.1%) | 0.015 # |
| Bladder catether | 54 (36.5%) | 34 (30.6%) | 20 (54.1%) | 0.010 |
| Parenteral nutrition | 45 (30.4%) | 30 (27.0%) | 15 (40.5%) | 0.122 |
| Chronic immunosuppression (including corticosteroids) | 45 (30.4%) | 24 (21.6%) | 8 (21.6%) | 1.000 |
| Previous antibiotic treatment (10 days) | 55 (37.2%) | 39 (35.1%) | 16 (43.2%) | 0.377 |
| MDRO/MRSA estimated risk | 122 (82.4%) | 89 (80.2%) | 33 (89.2%) | 0.212 |
| MDRO/MRSA infection | 41 (27.7%) | 26 (23.4%) | 15 (40.5%) | 0.044 |
| AVPU > <A (V/P/U = 1) | 47 (31.8%) | 22 (19.8) | 25 (67.6) | <0.001 |
| Total (N = 148) | Outcome NO (N = 111) | Outcome YES (N = 37) | p-Value * | |
|---|---|---|---|---|
| GCS | 13.6 ± 2.2 | 14.2 ± 1.8 | 12.0 ± 2.4 | <0.001 |
| Heart rate (bpm) | 96.2 ± 17.0 | 95.8 ± 16.0 | 97.4 ± 19.9 | 0.608 |
| Systolic blood pressure (mmHg) | 111.7 ± 22.8 | 112.8 ± 22.3 | 108.5 ± 24.5 | 0.323 |
| Diastolic blood pressure (mmHg) | 66.2 ± 12.9 | 66.8 ± 12.4 | 64.3 ± 14.5 | 0.322 |
| Mean blood pressure (mmHg) | 81.3 ± 15.3 | 82.0 ± 14.6 | 79.0 ± 17.1 | 0.304 |
| Body temperature (°C) | 38.2 ± 1.0 | 38.3 ± 1.0 | 38.1 ± 1.1 | 0.333 |
| FiO2 | 0.2 ± 0.1 | 0.2 ± 0.1 | 0.3 ± 0.1 | 0.001 |
| S/F | 408.9 ± 82.8 | 421.9 ± 74.0 | 369.8 ± 95.6 | 0.001 |
| P/F | 301.4 ± 85.0 | 314.1 ± 78.8 | 263.7 ± 92.4 | 0.002 |
| PaCO2 (mmHg) § | 36.5 ± 7.2 | 37.5 ± 7.4 | 34.3 ± 6.1 | 0.098 |
| SpO2 | 93.8 ± 3.6 | 94.0 ± 3.7 | 93.2 ± 3.2 | 0.261 |
| PaO2 (mmHg) | 70.1 ± 10.7 | 70.7 ± 10.8 | 68.4 ± 10.3 | 0.280 |
| Respiratory rate | 19.9 ± 4.7 | 19.7 ± 4.8 | 20.7 ± 4.4 | 0.339 |
| Bilirubin (mg/dL) | 0.8 [0.6, 1.5] | 0.8 [0.6, 1.4] | 0.9 [0.5, 1.8] | 0.288 * |
| Creatinine (mg/dL) | 0.9 [0.6, 1.4] | 0.8 [0.6, 1.3] | 1.2 [0.7, 2.0] | 0.044 * |
| PCT (ng/mL) | 4.1 [0.7, 30.6] | 4.3 [0.7, 30.6] | 3.8 [1.0, 24.9] | 0.597 * |
| PLT (103/µL) | 189,500 [120,500, 270,250] | 215,000 [137,500, 279,000] | 140,000 [98,000, 225,000] | 0.002 * |
| SOFA | 4.0 [2.0, 5.0] | 3.0 [2.0, 5.0] | 6.0 [5.0, 7.0] | <0.001 # |
| qSOFA | 1.0 [0.0, 2.0] | 1.0 [0.0, 1.0] | 1.0 [1.0, 2.0] | <0.001 # |
| qSOFA ≥ 2 | 39 (26.4%) | 22 (19.8%) | 17 (45.9%) | 0.002 ° |
| NEWS2 | 6.0 [4.0, 9.0] | 6.0 [4.0, 8.0] | 9.0 [6.0, 10.0] | 0.002 # |
| MEDS | 9.0 [6.0, 14.0] | 8.0 [5.0, 12.0] | 14.0 [10.0, 19.0] | <0.001 # |
| Delta SOFA | 0.0 [−1.0, 1.0] | 0.0 [−1.5, 0.0] | 0.0 [−1.0, 2.0] | 0.013 # |
| Delta qSOFA | 0.0 [−1.0, 0.0] | 0.0 [−1.0, 0.0] | 0.0 [0.0, 0.0] | 0.001 # |
| Delta MEDS | 0.0 [−3.0, 0.0] | 0.0 [−3.0, 0.0] | 0.0 [−3.0, 1.0] | 0.214 # |
| Delta-PCT % | −1.0 [−1.7, −0.2] | −1.1 [−1.8, −0.4] | −0.3 [−1.3, 0.7] | 0.002 * |
| Delta PLT % | 0.0 [−0.2, 0.3] | 0.0 [−0.2, 0.3] | −0.1 [−0.5, 0.2] | 0.249 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mirijello, A.; Fontana, A.; Greco, A.P.; Tosoni, A.; D’Agruma, A.; Labonia, M.; Copetti, M.; Piscitelli, P.; De Cosmo, S.; on behalf of the Internal Medicine Sepsis Study Group. Identifying Predictors Associated with Risk of Death or Admission to Intensive Care Unit in Internal Medicine Patients with Sepsis: A Comparison of Statistical Models and Machine Learning Algorithms. Antibiotics 2023, 12, 925. https://doi.org/10.3390/antibiotics12050925
Mirijello A, Fontana A, Greco AP, Tosoni A, D’Agruma A, Labonia M, Copetti M, Piscitelli P, De Cosmo S, on behalf of the Internal Medicine Sepsis Study Group. Identifying Predictors Associated with Risk of Death or Admission to Intensive Care Unit in Internal Medicine Patients with Sepsis: A Comparison of Statistical Models and Machine Learning Algorithms. Antibiotics. 2023; 12(5):925. https://doi.org/10.3390/antibiotics12050925
Chicago/Turabian StyleMirijello, Antonio, Andrea Fontana, Antonio Pio Greco, Alberto Tosoni, Angelo D’Agruma, Maria Labonia, Massimiliano Copetti, Pamela Piscitelli, Salvatore De Cosmo, and on behalf of the Internal Medicine Sepsis Study Group. 2023. "Identifying Predictors Associated with Risk of Death or Admission to Intensive Care Unit in Internal Medicine Patients with Sepsis: A Comparison of Statistical Models and Machine Learning Algorithms" Antibiotics 12, no. 5: 925. https://doi.org/10.3390/antibiotics12050925