

Resistance to Ceftazidime/Avibactam in Klebsiella pneumoniae KPC-Producing Isolates: A Real-Life Observational Study
 , , ,
, , ,  ,
,
Abstract
:1. Introduction
2. Results
3. Discussion
4. Conclusions
5. Materials and Methods
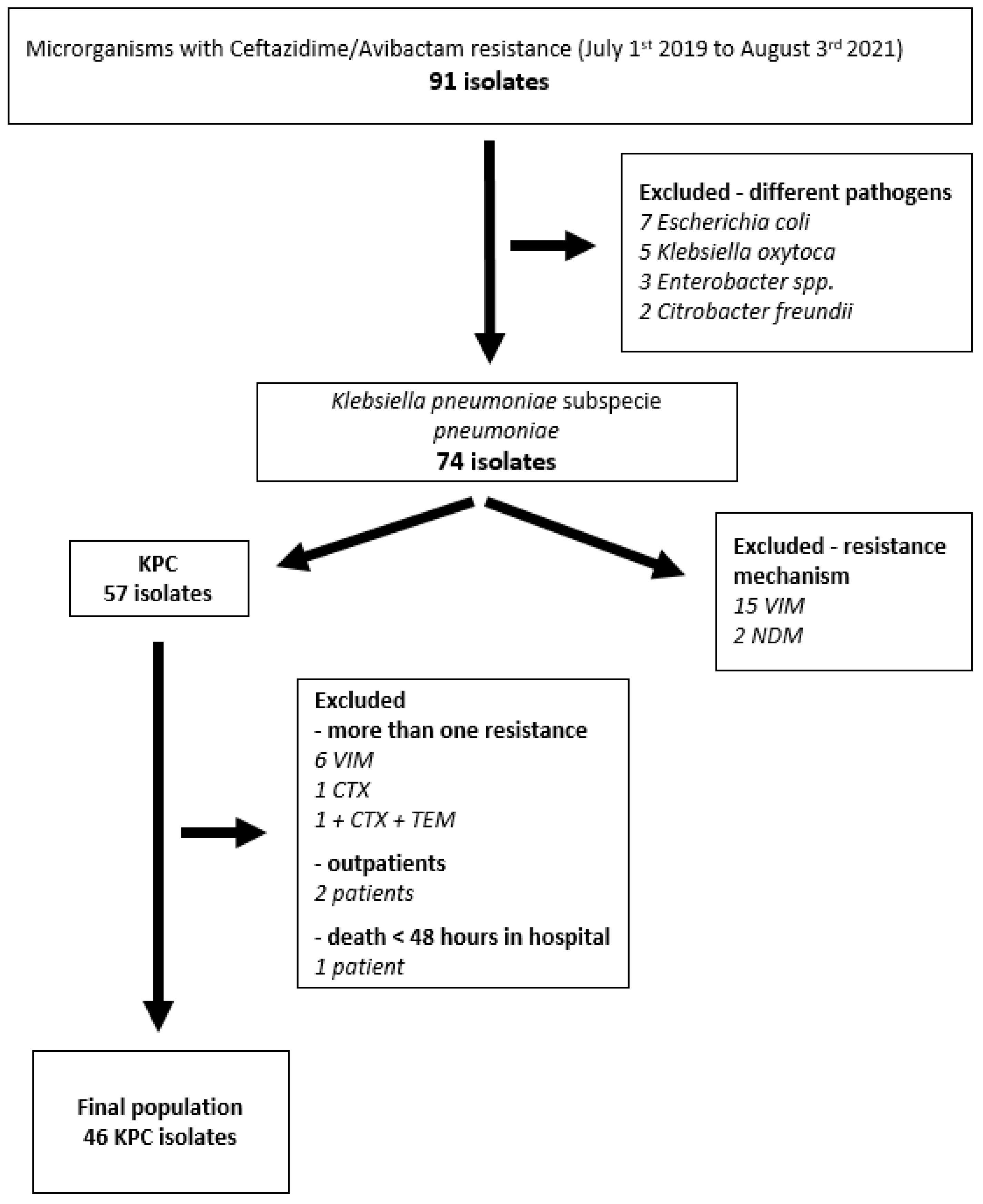
5.1. Study Design and Population Selection
5.2. Microbiology Analysis
5.3. Data Collection
5.4. Statistical Analysis
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- European Centre for Disease Prevention and Control. Antimicrobial Resistance Surveillance in Europe 2022–2020 Data. 2022. Available online: https://www.ecdc.europa.eu/en/publications-data/antimicrobial-resistance-surveillance-europe-2022-2020-data (accessed on 28 September 2022).
- Paul, M.; Carrara, E.; Retamar, P.; Tängdén, T.; Bitterman, R.; Bonomo, R.A.; de Waele, J.; Daikos, G.L.; Akova, M.; Harbarth, S.; et al. European Society of Clinical Microbiology and Infectious Diseases (ESCMID) guidelines for the treatment of infections caused by multidrug-resistant Gram-negative bacilli (endorsed by European society of intensive care medicine). Clin. Microbiol. Infect. 2022, 28, 521–547. [Google Scholar] [PubMed]
- Tamma, P.D.; Aitken, S.L.; Bonomo, R.A.; Mathers, A.J.; van Duin, D.; Clancy, C.J. Infectious Diseases Society of America Guidance on the Treatment of Extended-Spectrum β-lactamase Producing Enterobacterales (ESBL-E), Carbapenem-Resistant Enterobacterales (CRE), and Pseudomonas aeruginosa with Difficult-to-Treat Resistance (DTR-P. aeruginosa). Clin. Infect. Dis. 2021, 72, e169–e183. [Google Scholar] [PubMed]
- Tiseo, G.; Brigante, G.; Giacobbe, D.R.; Maraolo, A.E.; Gona, F.; Falcone, M.; Giannella, M.; Grossi, P.; Pea, F.; Rossolini, G.M.; et al. Diagnosis and management of infections caused by multidrug-resistant bacteria: Guideline endorsed by the Italian Society of Infection and Tropical Diseases (SIMIT), the Italian Society of Anti-Infective Therapy (SITA), the Italian Group for Antimicrobial Stewardship (GISA), the Italian Association of Clinical Microbiologists (AMCLI) and the Italian Society of Microbiology (SIM). Int. J. Antimicrob. Agents 2022, 60, 106611. [Google Scholar] [PubMed]
- Tumbarello, M.; Trecarichi, E.M.; Corona, A.; DE Rosa, F.G.; Bassetti, M.; Mussini, C.; Menichetti, F.; Viscoli, C.; Campoli, C.; Venditti, M.; et al. Efficacy of Ceftazidime-Avibactam Salvage Therapy in Patients with Infections Caused by Klebsiella pneumoniae Carbapenemase-producing K. pneumoniae. Clin. Infect. Dis. 2019, 68, 355–364. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tumbarello, M.; Raffaelli, F.; Giannella, M.; Mantengoli, E.; Mularoni, A.; Venditti, M.; De Rosa, F.G.; Sarmati, L.; Bassetti, M.; Brindicci, G.; et al. Ceftazidime-Avibactam Use for Klebsiella pneumoniae Carbapenemase-Producing K. pneumoniae Infections: A Retrospective Observational Multicenter Study. Clin. Infect. Dis. 2021, 73, 1664–1676. [Google Scholar] [CrossRef]
- Humphries, R.M.; Yang, S.; Hemarajata, P.; Ward, K.W.; Hindler, J.A.; Miller, S.A.; Gregson, A. First Report of Ceftazidime-Avibactam Resistance in a KPC-3-Expressing Klebsiella pneumoniae Isolate. Antimicrob. Agents Chemother. 2015, 59, 6605–6607. [Google Scholar] [CrossRef] [Green Version]
- European Centre for Disease Prevention and Control. Rapid Risk Assessment: Emergence of Resistance to Ceftazidime-Avibactam in Carbapenem-Resistant Enterobacteriaceae. 2018. Available online: https://www.ecdc.europa.eu/en/publications-data/rapid-risk-assessment-emergence-resistance-ceftazidime-avibactam-carbapenem (accessed on 28 September 2022).
- Shields, R.K.; Nguyen, M.H.; Chen, L.; Press, E.G.; Kreiswirth, B.N.; Clancy, C.J. Pneumonia and Renal Replacement Therapy Are Risk Factors for Ceftazidime-Avibactam Treatment Failures and Resistance among Patients with Carbapenem-Resistant Enterobacteriaceae Infections. Antimicrob. Agents Chemother. 2018, 62, e02497-17. [Google Scholar] [CrossRef] [Green Version]
- Hobson, C.A.; Pierrat, G.; Tenaillon, O.; Bonacorsi, S.; Bercot, B.; Jaouen, E.; Jacquier, H.; Birgy, A. Klebsiella pneumoniae Carbapenemase Variants Resistant to Ceftazidime-Avibactam: An Evolutionary Overview. Antimicrob. Agents Chemother. 2022, 66, e0044722. [Google Scholar] [CrossRef]
- Gaibani, P.; Gatti, M.; Rinaldi, M.; Pesce, C.C.; Lazzarotto, T.; Giannella, M.; Lombardo, D.; Amadesi, S.; Viale, P.; Pea, F.; et al. Suboptimal drug exposure leads to selection of different subpopulations of ceftazidime-avibactam-resistant Klebsiella pneumoniae carbapenemase-producing Klebsiella pneumoniae in a critically ill patient. Int. J. Infect. Dis. 2021, 113, 213–217. [Google Scholar] [CrossRef]
- Shields, R.K.; Potoski, B.A.; Haidar, G.; Hao, B.; Doi, Y.; Chen, L.; Press, E.G.; Kreiswirth, B.N.; Clancy, C.J.; Nguyen, M.H. Clinical Outcomes, Drug Toxicity, and Emergence of Ceftazidime-Avibactam Resistance Among Patients Treated for Carbapenem-Resistant Enterobacteriaceae Infections. Clin. Infect. Dis. 2016, 63, 1615–1618. [Google Scholar] [CrossRef] [Green Version]
- Di Bella, S.; Giacobbe, D.R.; Maraolo, A.E.; Viaggi, V.; Luzzati, R.; Bassetti, M.; Luzzaro, F.; Principe, L. Resistance to ceftazidime/avibactam in infections and colonisations by KPC-producing Enterobacterales: A systematic review of observational clinical studies. J. Glob. Antimicrob. Resist. 2021, 25, 268–281. [Google Scholar] [CrossRef] [PubMed]
- Cano, Á.; Guzmán-Puche, J.; García-Gutiérrez, M.; Castón, J.J.; Gracia-Ahufinger, I.; Pérez-Nadales, E.; Recio, M.; Natera, A.M.; Marfil-Pérez, E.; Luís, M.M.; et al. Use of carbapenems in the combined treatment of emerging ceftazidime/avibactam-resistant and carbapenem-susceptible KPC-producing Klebsiella pneumoniae infections: Report of a case and review of the literature. J. Glob. Antimicrob. Resist. 2020, 22, 9–12. [Google Scholar] [CrossRef] [PubMed]
- Shields, R.K.; Nguyen, M.H.; Hao, B.; Kline, E.G.; Clancy, C.J. Colistin Does Not Potentiate Ceftazidime-Avibactam Killing of Carbapenem-Resistant Enterobacteriaceae In Vitro or Suppress Emergence of Ceftazidime-Avibactam Resistance. Antimicrob. Agents Chemother. 2018, 62, e01018-18. [Google Scholar] [CrossRef] [Green Version]
- Venditti, C.; Butera, O.; Meledandri, M.; Balice, M.P.; Cocciolillo, G.C.; Fontana, C.; D’Arezzo, S.; De Giuli, C.; Antonini, M.; Capone, A.; et al. Molecular analysis of clinical isolates of ceftazidime-avibactam-resistant Klebsiella pneumoniae. Clin. Microbiol. Infect. 2021, 27, 1040.e1–1040.e6. [Google Scholar] [CrossRef] [PubMed]
- Carattoli, A.; Arcari, G.; Bibbolino, G.; Sacco, F.; Tomolillo, D.; Di Lella, F.M.; Trancassini, M.; Faino, L.; Venditti, M.; Antonelli, G.; et al. Evolutionary Trajectories toward Ceftazidime-Avibactam Resistance in Klebsiella pneumoniae Clinical Isolates. Antimicrob. Agents Chemother. 2021, 65, e0057421. [Google Scholar] [CrossRef] [PubMed]
- Shields, R.K.; Nguyen, M.H.; Press, E.G.; Chen, L.; Kreiswirth, B.N.; Clancy, C.J. In Vitro Selection of Meropenem Resistance among Ceftazidime-Avibactam-Resistant, Meropenem-Susceptible Klebsiella pneumoniae Isolates with Variant KPC-3 Carbapenemases. Antimicrob. Agents Chemother. 2017, 61, e00079-17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shields, R.K.; Nguyen, M.H.; Press, E.G.; Chen, L.; Kreiswirth, B.N.; Clancy, C.J. Emergence of Ceftazidime-Avibactam Resistance and Restoration of Carbapenem Susceptibility in Klebsiella pneumoniae Carbapenemase-Producing K pneumoniae: A Case Report and Review of Literature. Open Forum Infect. Dis. 2017, 4, ofx101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, P.; Shi, Q.; Hu, H.; Hong, B.; Wu, X.; Du, X.; Akova, M.; Yu, Y. Emergence of ceftazidime/avibactam resistance in carbapenem-resistant Klebsiella pneumoniae in China. Clin. Microbiol. Infect. 2020, 26, e1–e124. [Google Scholar] [CrossRef] [Green Version]
- Tiseo, G.; Falcone, M.; Leonildi, A.; Giordano, C.; Barnini, S.; Arcari, G.; Carattoli, A.; Menichetti, F. Meropenem-Vaborbactam as Salvage Therapy for Ceftazidime-Avibactam-, Cefiderocol-Resistant ST-512 Klebsiella pneumoniae-Producing KPC-31, a D179Y Variant of KPC-3. Open Forum Infect. Dis. 2021, 8, ofab141. [Google Scholar] [CrossRef]
- Oliva, A.; Curtolo, A.; Volpicelli, L.; Cogliati Dezza, F.; De Angelis, M.; Cairoli, S.; Dell’Utri, D.; Goffredo, B.M.; Raponi, G.; Venditti, M. Synergistic Meropenem/Vaborbactam Plus Fosfomycin Treatment of KPC Producing K. pneumoniae Septic Thrombosis Unresponsive to Ceftazidime/Avibactam: From the Bench to the Bedside. Antibiotics 2021, 10, 781. [Google Scholar] [CrossRef]
- Volpicelli, L.; Venditti, M.; Ceccarelli, G.; Oliva, A. Place in Therapy of the Newly Available Armamentarium for Multi-Drug-Resistant Gram-Negative Pathogens: Proposal of a Prescription Algorithm. Antibiotics 2021, 10, 1475. [Google Scholar] [CrossRef] [PubMed]
- Bianco, G.; Boattini, M.; Comini, S.; Iannaccone, M.; Bondi, A.; Cavallo, R.; Costa, C. In Vitro activity of cefiderocol against ceftazidime-avibactam susceptible and resistant KPC-producing Enterobacterales: Cross-resistance and synergistic effects. Eur. J. Clin. Microbiol. Infect. Dis. 2022, 41, 63–70. [Google Scholar] [CrossRef] [PubMed]
- Hobson, C.A.; Cointe, A.; Jacquier, H.; Choudhury, A.; Magnan, M.; Courroux, C.; Tenaillon, O.; Bonacorsi, S.; Birgy, A. Cross-resistance to cefiderocol and ceftazidime-avibactam in KPC β-lactamase mutants and the inoculum effect. Clin. Microbiol. Infect. 2021, 27, 1172.e7–1172.e10. [Google Scholar] [CrossRef] [PubMed]
- Gaibani, P.; Lombardo, D.; Bussini, L.; Bovo, F.; Munari, B.; Giannella, M.; Bartoletti, M.; Viale, P.; Lazzarotto, T.; Ambretti, S. Epidemiology of Meropenem/Vaborbactam Resistance in KPC-Producing Klebsiella pneumoniae Causing Bloodstream Infections in Northern Italy, 2018. Antibiotics 2021, 10, 536. [Google Scholar] [CrossRef] [PubMed]
- Antonelli, A.; Giani, T.; Di Pilato, V.; Riccobono, E.; Perriello, G.; Mencacci, A.; Rossolini, G.M. KPC-31 expressed in a ceftazidime/avibactam-resistant Klebsiella pneumoniae is associated with relevant detection issues. J. Antimicrob. Chemother. 2019, 74, 2464–2466. [Google Scholar] [CrossRef]
- Hernández-García, M.; Castillo-Polo, J.A.; Cordero, D.G.; Pérez-Viso, B.; García-Castillo, M.; de la Fuente, J.S.; Morosini, M.I.; Cantón, R.; Ruiz-Garbajosa, P. Impact of Ceftazidime-Avibactam Treatment in the Emergence of Novel KPC Variants in the ST307-Klebsiella pneumoniae High-Risk Clone and Consequences for Their Routine Detection. J. Clin. Microbiol. 2022, 60, e0224521. [Google Scholar] [CrossRef]
- Fontana, C.; Favaro, M.; Campogiani, L.; Malagnino, V.; Minelli, S.; Bossa, M.C.; Altieri, A.; Andreoni, M.; Sarmati, L. Ceftazidime/Avibactam-Resistant Klebsiella pneumoniae subsp. pneumoniae Isolates in a Tertiary Italian Hospital: Identification of a New Mutation of the Carbapenemase Type 3 (KPC-3) Gene Conferring Ceftazidime/Avibactam Resistance. Microorganisms 2021, 9, 2356. [Google Scholar] [CrossRef]
- EUCAST. Clinical Breakpoints and Dosing of Antibiotics. Available online: https://www.eucast.org/clinical_breakpoints/ (accessed on 28 November 2021).
- Favaro, M.; Sarti, M.; Fontana, C. Multiplex real-time PCR probe-based for identification of strains producing: OXA48, VIM, KPC and NDM. World J. Microbiol. Biotechnol. 2014, 30, 2995–3001. [Google Scholar] [CrossRef]
- National Healthcare Safety Network. 2021 NHSN Patient Safety Component Manual; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2021; p. 428.


{kind=link}
| Overall Population K. pneumoniae KPC 46 Patients | Group R 20 Patients (43.5%) | Group S 26 Patients (56.5%) | p | ||||
|---|---|---|---|---|---|---|---|
| Absolute n° | % | Absolute n° | % | Absolute n° | % | ||
| Year of isolate | |||||||
| 2019 | 3 | 6.5 | 0 | 3 | 11.5 | 0.269 | |
| 2020 | 12 | 26.1 | 5 | 25 | 7 | 26.9 | |
| 2021 | 31 | 67.4 | 15 | 75 | 16 | 61.6 | |
| Age (median, IQR) | 65.5 | 54.5–76 | 69.5 | 55–77.2 | 64 | 54.7–76 | 0.816 |
| Sex (M/F) | 25/21 | 54.3/45.7 | 12/8 | 60/40 | 13/13 | 50/50 | 0.500 |
| Comorbidities | |||||||
| Cardiovascular | 30 | 65.2 | 12 | 60 | 18 | 69.2 | 0.515 |
| Cerebrovascular | 16 | 34.8 | 9 | 45 | 7 | 26.9 | 0.202 |
| Obesity | 11 | 23.9 | 4 | 20 | 7 | 26.9 | 0.585 |
| Psychiatric/dementia | 11 | 23.9 | 5 | 25 | 6 | 23.1 | 0.880 |
| Renal | 11 | 23.9 | 5 | 25 | 6 | 23.1 | 0.880 |
| Respiratory | 10 | 21.7 | 4 | 20 | 6 | 23.1 | 0.802 |
| Diabetes | 8 | 17.4 | 2 | 10 | 6 | 23.1 | 0.246 |
| Solid tumour | 6 | 13 | 4 | 20 | 2 | 7.7 | 0.219 |
| Solid organ transplant | 3 | 6.5 | 0 | 3 | 11.5 | 0.116 | |
| Haematologic | 4 | 8.7 | 2 | 10 | 2 | 7.7 | 0.783 |
| Days from hospital admission to CAZ-AVI-R isolate (median, IQR) | 26 | 13–49.5 | 14 | 9–29.5 | 41 | 23.5–60.5 | 0.003 |
| Ward of CAZ-AVI-R | |||||||
| Intensive care unit | 28 | 60.9 | 13 | 65 | 15 | 57.7 | 0.861 |
| Internal medicine | 15 | 32.6 | 6 | 30 | 9 | 34.6 | |
| Surgical wards | 3 | 6.5 | 1 | 5 | 2 | 7.7 | |
| Previous CAZ-AVI treatment (yes/tot) | 23/46 | 50 | 5/20 | 25 | 18/26 | 69.2 | 0.003 |
| Of which | |||||||
| CAZ-AVI full dose (yes/tot) | 16/23 | 69.5 | 4/5 | 80 | 12/18 | 66.6 | 0.567 |
| CRRT/dialysis | 4/23 | 17.4 | 0/5 | 4/18 | 22.2 | 0.246 | |
| Overall Population K. pneumoniae KPC 46 Patients | Group R 20 Patients (43.5%) | Group S 26 Patients (56.5%) | p | ||||
|---|---|---|---|---|---|---|---|
| Absolute n° | % | Absolute n° | % | Absolute n° | % | ||
| K. pneumoniae isolate | |||||||
| Infection | 22 | 47.8 | 5 | 25 | 17 | 65.4 | 0.007 |
| Colonization | 24 | 52.2 | 15 | 75 | 9 | 34.6 | |
| K. pneumoniae isolation site | |||||||
| Rectal swab colonization | 15 | 32.6 | 13 | 65 | 2 | 7.7 | |
| Colonization—other sites * | 9 | 19.6 | 2 ** | 10 | 7 | 26.9 | |
| Pneumonia | 5 | 10.9 | 0 | 5 | 19.2 | ||
| Urinary tract infection | 5 | 10.9 | 2 | 10 | 3 | 11.5 | |
| Catheter-related BSI | 3 | 6.5 | 1 | 5 | 2 | 7.7 | |
| BSI (primary) | 1 | 2.2 | 1 | 5 | 0 | ||
| BSI (secondary) | 3 | 6.5 | 0 | 3 | 11.5 | ||
| Soft tissue and skin | 2 | 4.3 | 1 | 5 | 1 | 3.9 | |
| Intrabdominal infection | 2 | 4.3 | 0 | 2 | 7.7 | ||
| Surgical site infection | 1 | 2.2 | 0 | 1 | 3.9 | ||
| Positive KPC immunocromatographic test (yes/tot) | 27/32 # | 84.4 | 16/18 | 88.8 | 11/14 | 78.6 | 0.425 |
| Meropenem S | 11 | 23.9 | 5 | 25 | 6 | 23.1 | 0.737 |
| Meropenem I | 4 | 8.7 | 1 | 5 | 3 | 11.5 | |
| Meropenem R | 31 | 67.4 | 14 | 70 | 17 | 65.4 | |
| Overall Population Clinically Relevant Infections 22 Patients | ||
|---|---|---|
| Absolute n° | % | |
| Age (median, IQR) | 54.5 | 57.2–74.7 |
| Sex (M/F) | 14/8 | 63.6/36.4 |
| Comorbidities | ||
| Cardiovascular | 17 | 77.3 |
| Cerebrovascular | 5 | 22.7 |
| Obesity | 4 | 18.2 |
| Psychiatric/dementia | 4 | 18.2 |
| Renal | 6 | 27.3 |
| Respiratory | 5 | 22.7 |
| Diabetes | 2 | 9.1 |
| Solid tumour | 2 | 9.1 |
| Solid organ transplant | 2 | 9.1 |
| Haematologic | 1 | 4.5 |
| Days from hospital admission to CAZ-AVI-R isolate (median, IQR) | 28 | 17–49.5 |
| Ward of CAZ-AVI-R | ||
| Intensive care unit | 14 | 63.6 |
| Internal medicine | 6 | 27.3 |
| Surgical wards | 2 | 9.1 |
| Antibiotic treatment | 20/22 * | 90.9 |
| Combination therapy | 20 | 100 |
| Number of antibiotic (median) | 2 | min 0–max 3 |
| Colistin | 13 | 65 |
| CAZ-AVI | 11 | 55 |
| Carbapenem | 8 | 40 |
| Days of antibiotic (median, IQR) | 10.5 | 4.5–14 |
| Clinical resolution yes/no ** | 8/13 | 38.1/61.9 |
| Death ** | 13 | 61.9 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Campogiani, L.; Vitale, P.; Lodi, A.; Imeneo, A.; Fontana, C.; D’Agostini, C.; Compagno, M.; Coppola, L.; Spalliera, I.; Malagnino, V.; et al. Resistance to Ceftazidime/Avibactam in Klebsiella pneumoniae KPC-Producing Isolates: A Real-Life Observational Study. Antibiotics 2023, 12, 820. https://doi.org/10.3390/antibiotics12050820
Campogiani L, Vitale P, Lodi A, Imeneo A, Fontana C, D’Agostini C, Compagno M, Coppola L, Spalliera I, Malagnino V, et al. Resistance to Ceftazidime/Avibactam in Klebsiella pneumoniae KPC-Producing Isolates: A Real-Life Observational Study. Antibiotics. 2023; 12(5):820. https://doi.org/10.3390/antibiotics12050820
Chicago/Turabian StyleCampogiani, Laura, Pietro Vitale, Alessandra Lodi, Alessandra Imeneo, Carla Fontana, Cartesio D’Agostini, Mirko Compagno, Luigi Coppola, Ilaria Spalliera, Vincenzo Malagnino, and et al. 2023. "Resistance to Ceftazidime/Avibactam in Klebsiella pneumoniae KPC-Producing Isolates: A Real-Life Observational Study" Antibiotics 12, no. 5: 820. https://doi.org/10.3390/antibiotics12050820