
Use of Medical-Grade Honey to Treat Clinically Infected Heel Pressure Ulcers in High-Risk Patients: A Prospective Case Series

Abstract
:1. Introduction
2. Results
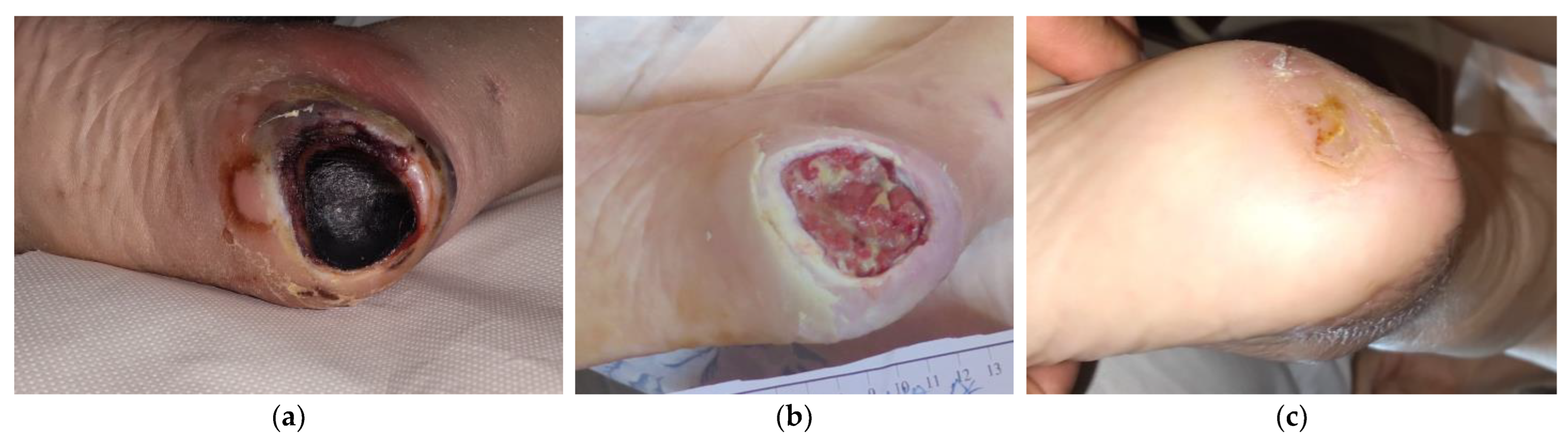
2.1. Case 1
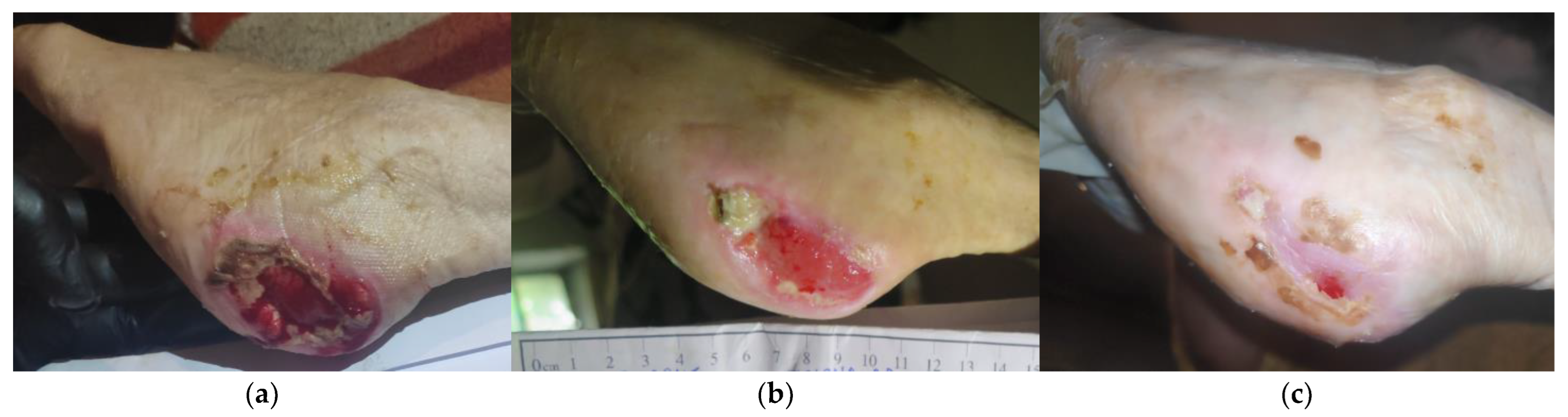
2.2. Case 2
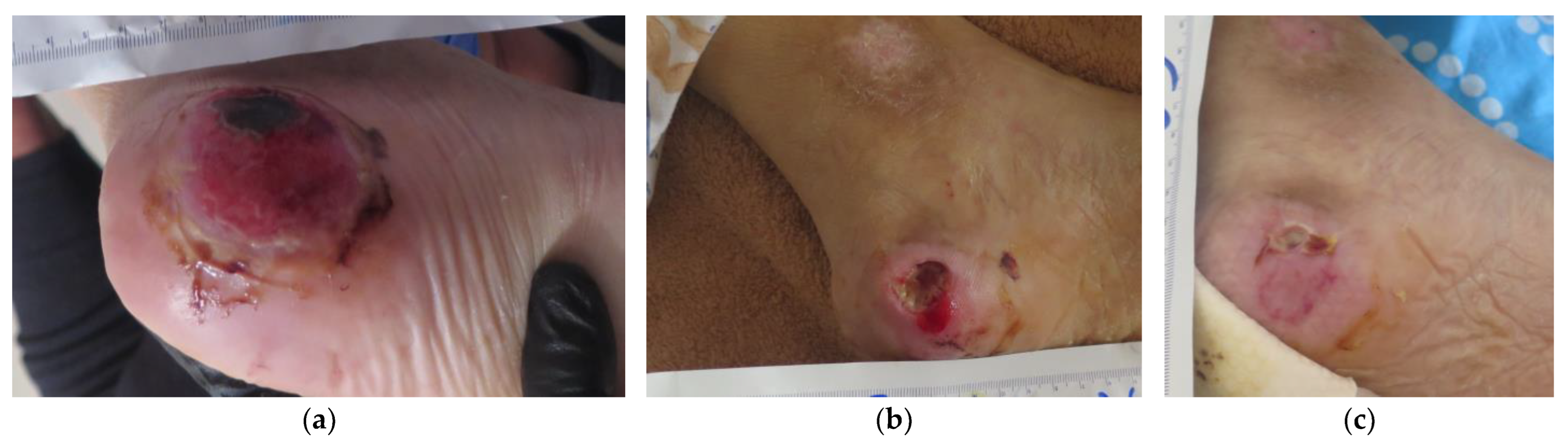
2.3. Case 3
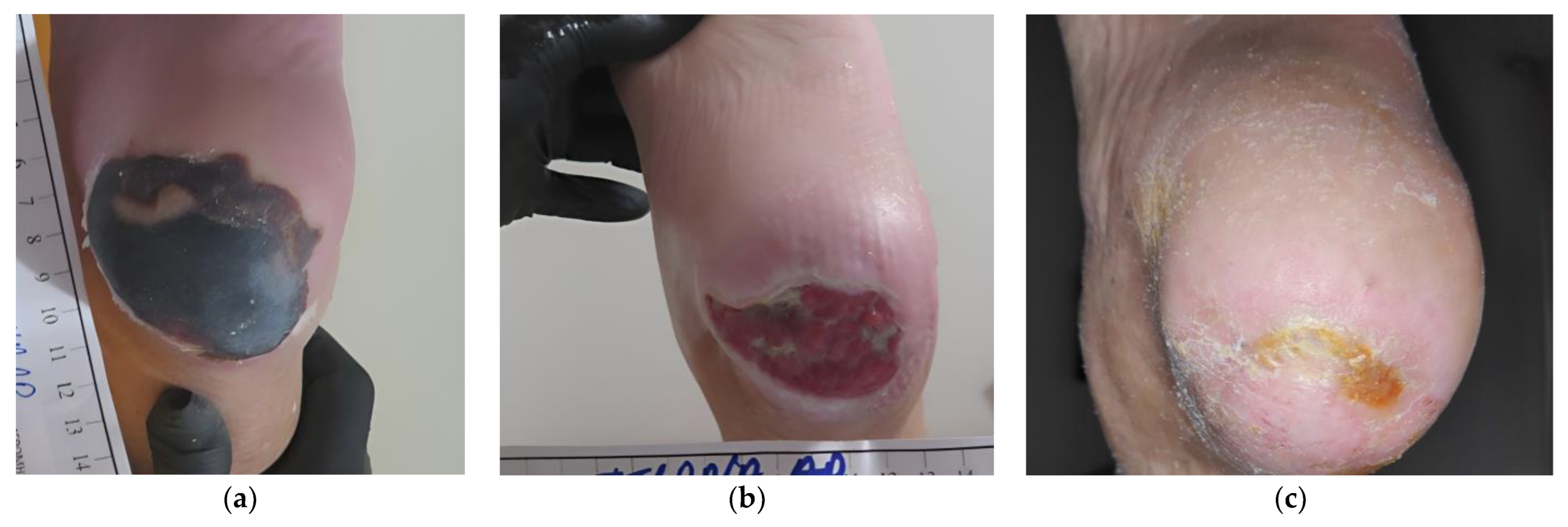
2.4. Case 4
2.5. Case 5
2.6. Case 6
2.7. Case 7
2.8. Case 8
2.9. Case 9
3. Discussion
4. Materials and Methods
4.1. Patients
4.2. L-Mesitran Wound Care Products and Therapeutic Interventions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bhattacharya, S.; Mishra, R.K. Pressure ulcers: Current understanding and newer modalities of treatment. Indian J. Plast. Surg. 2015, 48, 4–16. [Google Scholar] [CrossRef] [PubMed]
- Raetz, J.G.M.; Wick, K.H. Common Questions About Pressure Ulcers. Am. Fam. Physician 2015, 92, 888–894. [Google Scholar] [PubMed]
- European Pressure Ulcer Advisory Panel; National Pressure Injury Advisory Panel; Pan Pacific Pressure Injury Alliance. Chapter 9: Heel pressure injuries. In Prevention and Treatment of Pressure Ulcers/Pressure Injuries: Clinical Practice Guideline; Haesler, E., Ed.; EPUAP/NPIAP/PPPIA: Perth, WA, Australia, 2019. [Google Scholar]
- VanGilder, C.; MacFarlane, G.D.; Harrison, P.; Lachenbruch, C.; Meyer, S. The Demographics of Suspected Deep Tissue Injury in the United States. Adv. Skin Wound Care 2010, 23, 254–261. [Google Scholar] [CrossRef] [PubMed]
- Greenwood, C. Heel pressure ulcers: Understanding why they develop and how to prevent them. Nurs. Stand. 2022, 37, 60–66. [Google Scholar] [CrossRef]
- Dube, A.; Sidambe, V.; Verdon, A.; Phillips, E.; Jones, S.; Lintern, M.; Radford, M. Risk factors associated with heel pressure ulcer development in adult population: A systematic literature review. J. Tissue Viability 2022, 31, 84–103. [Google Scholar] [CrossRef] [PubMed]
- Vanderwee, K.; Clark, M.; Dealey, C.; Gunningberg, L.; Defloor, T. Pressure ulcer prevalence in Europe: A pilot study. J. Eval. Clin. Pract. 2007, 13, 227–235. [Google Scholar] [CrossRef] [PubMed]
- Gunningberg, L.; Stotts, N.A.; Idvall, E. Hospital-acquired pressure ulcers in two Swedish County Councils: Cross-sectional data as the foundation for future quality improvement. Int. Wound J. 2011, 8, 465–473. [Google Scholar] [CrossRef]
- Agale, S.V. Chronic Leg Ulcers: Epidemiology, Aetiopathogenesis, and Management. Ulcers 2013, 2013, 9. [Google Scholar] [CrossRef] [Green Version]
- World Union of Wound Healing Societies (WUWHS). Florence Congress, Position Document. In Advance in Wound Care: The Triangle of Wound Assessment; Wounds International: London, UK, 2016. [Google Scholar]
- Delmore, B.; Ayello, E.A.; Smith, D.; Rolnitzky, L.; Chu, A.S. Refining Heel Pressure Injury Risk Factors in the Hospitalized Patient. Adv. Skin Wound Care 2019, 32, 512–519. [Google Scholar] [CrossRef]
- Athlin, .M.; Engström, M.; Gunningberg, L.; Bååth, C. Heel pressure ulcer, prevention and predictors during the care delivery chain – when and where to take action? A descriptive and explorative study. Scand. J. Trauma Resusc. Emerg. Med. 2016, 24, 134. [Google Scholar] [CrossRef]
- Delmore, B.P.; Ayello, E.A.P. Heel Pressure Injuries. Adv. Skin Wound Care 2021, 34, 236–237. [Google Scholar] [CrossRef] [PubMed]
- Sibbald, R.G.; Woo, K.; Ayello, E.A. Increased Bacterial Burden and Infection: The story of NERDS and STONES. Adv. Skin Wound Care 2006, 19, 447–461; quiz 461–443. [Google Scholar] [CrossRef] [PubMed]
- Langemo, D.K.; Hanson, D.; Anderson, J.; Thompson, P.; Hunter, S. Use of Honey for Wound Healing. Adv. Skin Wound Care 2009, 22, 113–118. [Google Scholar] [CrossRef] [PubMed]
- Hermanns, R.; Mateescu, C.; Thrasyvoulou, A.; Tananaki, C.; Wagener, F.A.; Cremers, N.A. Defining the standards for medical grade honey. J. Apic. Res. 2020, 59, 125–135. [Google Scholar] [CrossRef]
- Cremers, N.; Belas, A.; Costa, S.S.; Couto, I.; de Rooster, H.; Pomba, C. In vitro antimicrobial efficacy of two medical grade honey formulations against common high-risk meticillin-resistant staphylococci and Pseudomonas spp. pathogens. Vet. Dermatol. 2019, 31, 90–96. [Google Scholar] [CrossRef]
- Pleeging, C.C.F.; Coenye, T.; Mossialos, D.; De Rooster, H.; Chrysostomou, D.; Wagener, F.; Cremers, N.A.J. Synergistic Antimicrobial Activity of Supplemented Medical-Grade Honey against Pseudomonas aeruginosa Biofilm Formation and Eradication. Antibiotics 2020, 9, 866. [Google Scholar] [CrossRef]
- Combarros-Fuertes, P.; Fresno, J.M.; Estevinho, M.M.; Sousa-Pimenta, M.; Tornadijo, M.E.; Estevinho, L.M. Honey: Another Alternative in the Fight against Antibiotic-Resistant Bacteria? Antibiotics 2020, 9, 774. [Google Scholar] [CrossRef]
- De Groot, T.; Janssen, T.; Faro, D.; Cremers, N.A.J.; Chowdhary, A.; Meis, J.F. Antifungal Activity of a Medical-Grade Honey Formulation against Candida auris. J. Fungi 2021, 7, 50. [Google Scholar] [CrossRef]
- Pieper, B. Honey-Based Dressings and Wound Care: An option for care in the United States. J. Wound Ostomy Cont. Nurs. 2009, 36, 60–66. [Google Scholar] [CrossRef]
- Biglari, B.; Moghaddam, A.; Santos, K.; Blaser, G.; Büchler, A.; Jansen, G.; Längler, A.; Graf, N.; Weiler, U.; Licht, V.; et al. Multicentre prospective observational study on professional wound care using honey (Medihoney™). Int. Wound J. 2012, 10, 252–259. [Google Scholar] [CrossRef]
- Smaropoulos, E.; Cremers, N.A.J. Treating severe wounds in pediatrics with medical grade honey: A case series. Clin. Case Rep. 2020, 8, 469–476. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smaropoulos, E.; Cremers, N.A.J. The pro-healing effects of medical grade honey supported by a pediatric case series. Complement. Ther. Med. 2019, 45, 14–18. [Google Scholar] [CrossRef]
- Oryan, A.; Alemzadeh, E.; Moshiri, A. Biological properties and therapeutic activities of honey in wound healing: A narrative review and meta-analysis. J. Tissue Viability 2016, 25, 98–118. [Google Scholar] [CrossRef]
- Saikaly, S.K.; Khachemoune, A. Honey and Wound Healing: An Update. Am. J. Clin. Dermatol. 2017, 18, 237–251. [Google Scholar] [CrossRef] [PubMed]
- Yapucu Gunes, U.; Eser, I. Effectiveness of a Honey Dressing for Healing Pressure Ulcers. J. Wound Ostomy Cont. Nurs. 2007, 34, 184–190. [Google Scholar] [CrossRef]
- Yilmaz, A.C.; Aygin, D. Honey dressing in wound treatment: A systematic review. Complement. Ther. Med. 2020, 51, 102388. [Google Scholar] [CrossRef] [PubMed]
- Vestby, L.K.; Grønseth, T.; Simm, R.; Nesse, L.L. Bacterial Biofilm and its Role in the Pathogenesis of Disease. Antibiotics 2020, 9, 59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nair, H.K.R.; Tatavilis, N.; Pospíšilová, I.; Kučerová, J.; Cremers, N.A.J. Medical-Grade Honey Kills Antibiotic-Resistant Bacteria and Prevents Amputation in Diabetics with Infected Ulcers: A Prospective Case Series. Antibiotics 2020, 9, 529. [Google Scholar] [CrossRef]
- Holubová, A.; Chlupáčová, L.; Cetlová, L.; Cremers, N.A.J.; Pokorná, A. Medical-Grade Honey as an Alternative Treatment for Antibiotics in Non-Healing Wounds—A Prospective Case Series. Antibiotics 2021, 10, 918. [Google Scholar] [CrossRef]
- Naik, P.P.; Chrysostomou, D.; Cinteza, M.; Pokorná, A.; Cremers, N.A. When time does not heal all wounds—The use of medical grade honey in wound healing: A case series. J. Wound Care 2022, 31, 548–558. [Google Scholar] [CrossRef]
- McLoone, P.; Tabys, D.; Fyfe, L. Honey Combination Therapies for Skin and Wound Infections: A Systematic Review of the Literature. Clin. Cosmet. Investig. Dermatol. 2020, 13, 875–888. [Google Scholar] [CrossRef] [PubMed]
- Gethin, G.; Cowman, S. Bacteriological changes in sloughy venous leg ulcers treated with manuka honey or hydrogel: An RCT. J. Wound Care 2008, 17, 241–244, 246–247. [Google Scholar] [CrossRef] [Green Version]
- Al-Kafaween, M.A.; Alwahsh, M.; Hilmi, A.B.M.; Abulebdah, D.H. Physicochemical Characteristics and Bioactive Compounds of Different Types of Honey and Their Biological and Therapeutic Properties: A Comprehensive Review. Antibiotics 2023, 12, 337. [Google Scholar] [CrossRef] [PubMed]
- Sherlock, O.; Dolan, A.; Athman, R.; Power, A.; Gethin, G.; Cowman, S.; Humphreys, H. Comparison of the antimicrobial activity of Ulmo honey from Chile and Manuka honey against methicillin-resistant Staphylococcus aureus, Escherichia coli and Pseudomonas aeruginosa. BMC Complement. Altern. Med. 2010, 10, 47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Manderlier, B.; Van Damme, N.; Verhaeghe, S.; Van Hecke, A.; Everink, I.; Halfens, R.; Beeckman, D. Modifiable patient-related factors associated with pressure ulcers on the sacrum and heels: Secondary data analyses. J. Adv. Nurs. 2019, 75, 2773–2785. [Google Scholar] [CrossRef] [PubMed]
- Campbell, K.E.; Woodbury, G.; Labate, T.; LeMesurier, A.; Houghton, P.E. Heel ulcer incidence following orthopedic surgery: A prospective, observational study. J. Wound Ostomy Cont. Nurs. 2010, 56, 32–39. [Google Scholar]
- McGinnis, E.; Greenwood, D.C.; Nelson, E.A.; Nixon, J. A prospective cohort study of prognostic factors for the healing of heel pressure ulcers. Age Ageing 2014, 43, 267–271. [Google Scholar] [CrossRef] [Green Version]
- Delmore, B.; Lebovits, S.; Suggs, B.; Rolnitzky, L.; Ayello, E.A. Risk Factors Associated With Heel Pressure Ulcers in Hospitalized Patients. J. Wound Ostomy Cont. Nurs. 2015, 42, 242–248; quiz E241–242. [Google Scholar] [CrossRef] [Green Version]
- Nishio, Y.; Tsuji, Y.; Kitano, I.; Terashi, H. Influence of Peripheral Arterial Disease on Wound Healing in Heel Pressure Ulcers. Kobe J. Med. Sci. 2022, 67, E146–E154. [Google Scholar]
- Goudie, E.B.; Gendics, C.; Lantis, J.C., 2nd. Multimodal therapy as an algorithm to limb salvage in diabetic patients with large heel ulcers. Int. Wound J. 2012, 9, 132–138. [Google Scholar] [CrossRef]
- Bosanquet, D.C.; Wright, A.M.; White, R.D.; Williams, I.M. A review of the surgical management of heel pressure ulcers in the 21st century. Int. Wound J. 2016, 13, 9–16. [Google Scholar] [CrossRef] [PubMed]
- Bayron, J.; Gallagher, K.; Cardenas, L. Medical-grade Honey as an Alternative to Surgery: A Case Series. Wounds 2019, 31, 36–40. [Google Scholar] [PubMed]
- Smaropoulos, E.; Cremers, N.A.J. Medical-Grade Honey for the Treatment of Extravasation-Induced Injuries in Preterm Neonates: A Case Series. Adv. Neonatal Care 2020, 21, 122–132. [Google Scholar] [CrossRef] [PubMed]
- Pleeging, C.C.F.; Wagener, F.; de Rooster, H.; Cremers, N.A.J. Revolutionizing non-conventional wound healing using honey by simultaneously targeting multiple molecular mechanisms. Drug Resist. Updat. 2022, 62, 100834. [Google Scholar] [CrossRef] [PubMed]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Case # | Gender/Age (Years) | HPU Location/ Dimensions (cm) | HPU Etiology | Relevant Comorbidities | Previous Treatments | Local Signs of Infection | Time for Infection Resolution (Weeks) | Time for Wound Healing (Days) |
|---|---|---|---|---|---|---|---|---|
| 1 | Female 85 | Right 5 × 5 | Hip arthroplasty | Hypertensive heart disease, hyperlipidemia, dementia, deficiency of calcium and vitamin B12 | Neomycin sulfate topical spray | Necrotic eschar, exudate, pain, delayed healing | 4 | 117 |
| 2 | Female 88 | Left 5 × 4 | Permanent immobility | CVD, AHT, dementia, anaemia, iron deficiency, nephritis | Povidone-iodine solution, mupirocin-based topical cream | Hyperthermia, exudate, malodour, pain, slough | 3 | 86 |
| 3 | Female 72 | Left 5 × 5 | Permanent immobility | CVD, AHT, dementia, myocardial infarction, atrial fibrillation, osteoporosis | Normal saline and soap | Debris, erythema, exudate, delayed healing | 3 | 57 |
| 4 | Female 86 | Left 6 × 5 | Hip fracture surgery | CVD, AHT, epilepsy, anxiety, deficiency of vitamin D | Silver and foam dressings | Necrotic eschar, exudate, malodor, pain, delayed healing | 4 | 169 |
| 5 | Female 92 | Right 6 × 4 | Permanent immobility | CVD, rheumatic polymyalgia, glaucoma | Povidone-iodine solution | Central necrotic area, peripheric erythema, pain, delayed healing | 3 | 218 |
| 6 | Male 94 | Right 6 × 5, Left 7 × 7 | Permanent immobility | CVD, diabetes mellitus type 2, benign prostatic hyperplasia, anaemia, deficiency of vitamin B12 | No reported | Necrotic tissue, exudate, malodour, erythema, pain, delayed healing | 8 | 155 |
| 7 | Female 59 | Right 6 × 5, Left 5 × 4 | Permanent immobility | Psychotic disorders, urinary incontinence, lower limb oedema | Povidone–iodine solution | Necrotic tissue, exudate, malodor, delayed healing | 2 | 108 (right) 118 (left) |
| 8 | Female 87 | Right 4 × 4 | Hip fracture surgery | AHT, organic psychotic disorder | Silicone foam dressings, neomycin sulfate topical spray | Necrotic eschar, erythema, malodor, pain, delayed healing | 4 | 89 |
| 9 | Female 78 | Right 6 × 3 | Permanent immobility | AHT, peripheral arterial disease, Parkinson’s disease, osteoporosis | Povidone–iodine solution | Debris, erythema, exudate, edema, delayed healing | 4 | 137 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Papanikolaou, G.E.; Gousios, G.; Cremers, N.A.J. Use of Medical-Grade Honey to Treat Clinically Infected Heel Pressure Ulcers in High-Risk Patients: A Prospective Case Series. Antibiotics 2023, 12, 605. https://doi.org/10.3390/antibiotics12030605
Papanikolaou GE, Gousios G, Cremers NAJ. Use of Medical-Grade Honey to Treat Clinically Infected Heel Pressure Ulcers in High-Risk Patients: A Prospective Case Series. Antibiotics. 2023; 12(3):605. https://doi.org/10.3390/antibiotics12030605
Chicago/Turabian StylePapanikolaou, Georgios E., Georgios Gousios, and Niels A. J. Cremers. 2023. "Use of Medical-Grade Honey to Treat Clinically Infected Heel Pressure Ulcers in High-Risk Patients: A Prospective Case Series" Antibiotics 12, no. 3: 605. https://doi.org/10.3390/antibiotics12030605