
Estimation, Evaluation and Characterization of Carbapenem Resistance Burden from a Tertiary Care Hospital, Pakistan
 , , and
, , and
Abstract
:1. Introduction
2. Results
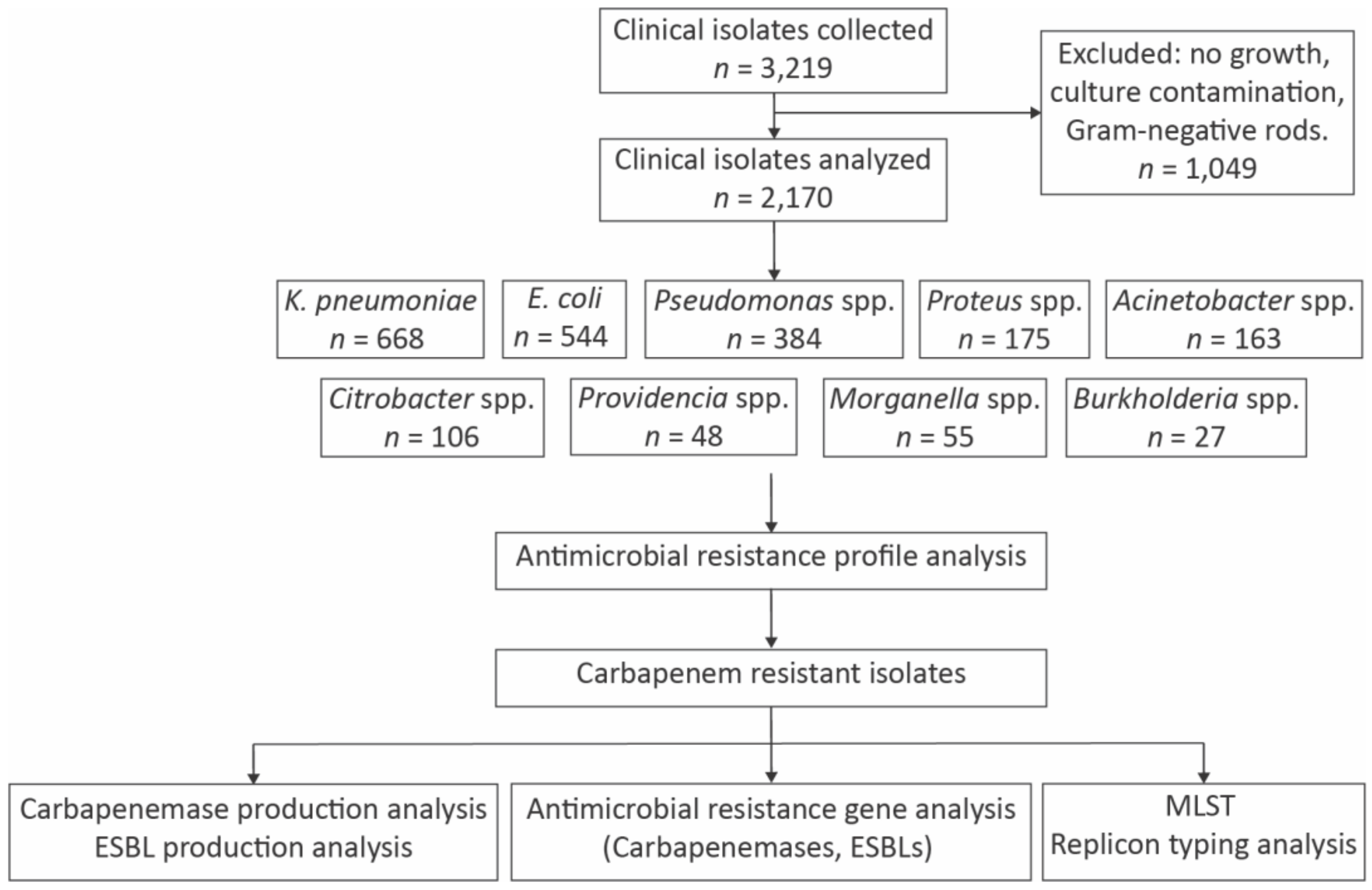
2.1. Phenotypic Identification and Distribution of Bacterial Strains
2.2. Antimicrobial Susceptibility Trend
2.3. Prevalence of Antimicrobial Resistance Genes
2.4. Genetic Diversity Analysis
3. Discussion
4. Conclusions
5. Methodology
5.1. Antimicrobial Susceptibility Testing
5.2. Antimicrobial Resistance Gene Analysis
5.3. Allele Identification by Sequencing
5.4. Determination of Genetic Diversity by Multilocus Sequence Typing and Plasmid Replicon Typing
5.5. Statistical Analysis
Supplementary Materials
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Martens, E.; Demain, A.L. The antibiotic resistance crisis, with a focus on the United States. J. Antibiot. 2017, 70, 520–526. [Google Scholar] [CrossRef] [Green Version]
- Hernando-Amado, S.; Coque, M.T.; Baquero, F.; Martinez, J.L. Defining and combating antibiotic resistance from One Health and Global Health perspectives. Nat. Microbiol. 2019, 4, 1432–1442. [Google Scholar] [CrossRef]
- Ain, N.U.; Abrar, S.; Sherwani, R.A.K.; Hanan, A.; Imran, N.; Riaz, S. Systematic surveillance and meta-analysis on the prevalence of metallo-β-lactamase producers among carbapenem resistant clinical isolates in Pakistan. J. Glob. Antimicrob. Resist. 2020, 23, 55–63. [Google Scholar] [CrossRef]
- Avershina, E.; Shapovalova, V.; Shipulin, G. Fighting antibiotic resistance in hospital-acquired infections: Current state and emerging technologies in disease prevention, diagnostics and therapy. Front. Microbiol. 2021, 12, 707330. [Google Scholar] [CrossRef] [PubMed]
- Farha, M.A.; Brown, E.D. Drug repurposing for antimicrobial discovery. Nat. Microbiol. 2019, 4, 565–577. [Google Scholar] [CrossRef] [PubMed]
- O’neill, J. Antimicrobial Resistance. Tackling a Crisis for the Health and Wealth of Nations; Review on Antimicrobial Resistance: London, UK, 2014. [Google Scholar]
- Khan, E.; Hafeez, A.; Ikram, A. Situation Analysis Report on Antimicrobial Resistance in Pakistan-Findings and Recommendations for Antibiotic Use and Resistance. The Global Antibiotic Resistance Partnership (GARP), Pakistan, 2018. Available online: https://www.cddep.org/publications/garp-pakistan-situation-analysis (accessed on 19 January 2023).
- Hayat, K.; Rosenthal, M.; Gillani, H.A.; Chang, J.; Ji, W.; Yang, C.; Jiang, M.; Zhao, M.; Fang, Y. Perspective of key healthcare professionals on antimicrobial resistance and stewardship programs: A multicenter cross-sectional study from Pakistan. Front. Pharmacol. 2020, 10, 1520. [Google Scholar] [CrossRef] [PubMed]
- Crofts, T.S.; Gasparrini, A.J.; Dantas, G. Next-generation approaches to understand and combat the antibiotic resistome. Nat. Rev. Microbiol. 2017, 15, 422. [Google Scholar] [CrossRef] [Green Version]
- Bush, K.; Bradford, P.A. Interplay between β-lactamases and new β-lactamase inhibitors. Nat. Rev. Microbiol. 2019, 17, 295–306. [Google Scholar]
- Munita, J.M.; Arias, C.A. Mechanisms of antibiotic resistance. Microbiol. Spectr. 2016, 4, 481–511. [Google Scholar] [CrossRef] [Green Version]
- Christaki, E.; Marcou, M.; Tofarides, A. Antimicrobial resistance in bacteria: Mechanisms, evolution, and persistence. J. Mol. Evol. 2019, 88, 26–40. [Google Scholar] [CrossRef]
- Bonnin, R.A.; Jousset, A.B.; Emeraud, C.; Oueslati, S.; Doret, L.; Nass, T. Genetic diversity, biochemical properties, and detection methods of minor carbapenemases in Enterobacterales. Front. Med. 2021, 7, 616490. [Google Scholar] [CrossRef] [PubMed]
- Sattar, H.; Toleman, M.; Nahid, F.; Zahra, R. Co-existence of blaNDM-1 and blaKPC-2 in clinical isolates of Klebsiella pneumoniae from Pakistan. J. Chemother. 2016, 28, 346–349. [Google Scholar] [CrossRef]
- Gondal, A.J.; Saleem, S.; Jahan, S.; Choudhry, N.; Yasmin, N. Novel carbapenem-resistant klebsiella pneumoniae ST147 coharboring blaNDM-1, blaOXA-48 and extended-spectrum β-lactamases from Pakistan. Infect. Drug Resist. 2020, 13, 2105. [Google Scholar] [CrossRef] [PubMed]
- Aslam, B.; Chaudhry, T.H.; Arshad, M.I.; Alvi, R.F.; Shahzad, N.; Yasmeen, N.; Idris, A.; Rasool, M.H.; Khurshid, M.; Ma, Z.; et al. The first blaKPC harboring Klebsiella pneumoniae ST258 strain isolated in Pakistan. Microb. Drug Resist. 2020, 26, 783–786. [Google Scholar] [CrossRef]
- Gondal, A.J.; Choudhry, N.; Bukhari, H.; Rizvi, Z.; Yasmin, N. Characterization of genomic diversity among carbapenem-resistant Escherichia coli clinical isolates and antibacterial efficacy of silver nanoparticles from Pakistan. Microorganisms 2022, 10, 2283. [Google Scholar] [CrossRef] [PubMed]
- Qureshi, R.; Qamar, M.U.; Shafique, M.; Muzammil, S.; Rasool, M.H.; Ahmad, I.; Ejaz, H. Antibacterial efficacy of silver nanoparticles against metallo-β-lactamase (blaNDM, blaVIM, blaOXA) producing clinically isolated Pseudomonas aeruginosa. Pak. J. Pharm. Sci. 2021, 34, 237–243. [Google Scholar]
- Tischendorf, J.; de Avila, R.A.; Safdar, N. Risk of infection following colonization with carbapenem-resistant Enterobactericeae: A systematic review. Am. J. Infect. Control. 2016, 44, 539–543. [Google Scholar] [CrossRef] [Green Version]
- El-Defrawy, I.; Gamal, D.; El-Gharbawy, R.; El-Seidi, E.; El-Dabaa, E.; Eissa, S. Detection of intestinal colonization by carbapenem-resistant Enterobacteriaceae (CRE) among patients admitted to a tertiary care hospital in Egypt. Egypt. J. Med. Hum. Genet. 2022, 23, 83. [Google Scholar] [CrossRef]
- Apanga, P.A.; Ahmed, J.; Tanner, W.; Starcevich, K.; VanDerslice, J.A.; Rehman, U.; Channa, N.; Benson, S.; Garn, J.V. Carbapenem-resistant Enterobacteriaceae in sink drains of 40 healthcare facilities in Sindh, Pakistan: A cross-sectional study. PLoS ONE 2022, 17, e0263297. [Google Scholar] [CrossRef]
- Prescott, K.; Billam, H.; Yates, C.; Clarke, M.; Montgomery, R.; Staniforth, K.; Vaughan, N.; Boswell, T.; Mahida, N. Outbreak of New Delhi Metallo-Beta-lactamase Carbapenemase producing Enterobacterales on a bone marrow transplant unit: Role of the environment. Infect. Prev. Pract. 2021, 3, 100125. [Google Scholar] [CrossRef]
- Mullié, C.; Lemonnier, D.; Adijide, C.C.; Maizel, J.; Mismacque, G.; Cappe, A.; Carles, T.; Pierson-Marchandise, M.; Zerbib, Y. Nosocomial outbreak of monoclonal VIM carbapenemase-producing Enterobacter cloacae complex in an intensive care unit during the COVID-19 pandemic: An integrated approach. J. Hosp. Infect. 2022, 120, 48–56. [Google Scholar] [CrossRef] [PubMed]
- Yamagishi, T.; Matsui, M.; Sekizuka, T.; Ito, H.; Fukusmi, M.; Uehira, T.; Tsubokura, M.; Ogawa, Y.; Miyamoto, A.; Nakamori, S.; et al. A prolonged multispecies outbreak of IMP-6 carbapenemase-producing Enterobacterales due to horizontal transmission of the IncN plasmid. Sci. Rep. 2020, 10, 4139. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bacarakos, P.; Michalis, E.; Galanopoulos, A.; Orfanidou, M.; Ganteris, G.; Vagiakou, E.; Giakkoupi, P. An outbreak of Î2-Lactamase Klebsiella pneumoniae carbapenemase 2–producing Klebsiella pneumoniae bacteremia in hematology patients. Biomed. J. Sci. Tech. Res. 2021, 35, 27700–27707. [Google Scholar]
- Zeng, L.; Yang, C.; Zhanf, J.; Hu, K.; Zou, J.; Li, J.; Wang, J.; Huang, W.; Yin, L.; Zhang, X. An outbreak of carbapenem-resistant Klebsiella pneumoniae in an intensive care unit of a major teaching hospital in Chongqing, China. Front. Cell. Infect. Microbiol. 2021, 11, 656070. [Google Scholar] [CrossRef]
- Zhao, Y.; Hu, K.; Zhang, J.; Guo, Y.; Fan, X.; Wang, Y.; Mensah, S.D.; Zhang, X. Outbreak of carbapenem-resistant Acinetobacter baumannii carrying the carbapenemase OXA-23 in ICU of the eastern Heilongjiang Province, China. BMC Infect. Dis. 2019, 19, 452. [Google Scholar]
- Amarsy, R.; Jacquier, H.; Munier, A.L.; Merimeche, M.; Bercot, B.; Megarbane, B. Outbreak of NDM-1-producing Klebsiella pneumoniae in the intensive care unit during the COVID-19 pandemic: Another nightmare. Am. J. Infect. Control. 2021, 49, 1324–1326. [Google Scholar] [CrossRef]
- Mendes, G.; Ramalho, J.F.; Duarte, A.; Pedrosa, A.; Silva, A.C.; Mendez, L.; Caneiras, C. First outbreak of NDM-1-Producing Klebsiella pneumoniae ST11 in a Portuguese Hospital Centre during the COVID-19 pandemic. Microorganisms 2022, 10, 251. [Google Scholar] [CrossRef] [PubMed]
- Bilal, H.; Khan, M.N.; Rehman, T.; Hameed, M.F.; Yang, X. Antibiotic resistance in Pakistan: A systematic review of past decade. BMC Infect. Dis. 2021, 21, 244. [Google Scholar] [CrossRef]
- Bonomo, R.A.; Burd, E.M.; Conly, J.; Limbago, B.M.; Poirel, L.; Segre, J.A.; Westblade, L.F. Carbapenemase-producing organisms: A global scourge. Clin. Infect. Dis. 2018, 66, 1290–1297. [Google Scholar] [CrossRef] [Green Version]
- Curiao, T.; Morosini, M.I.; Ruiz-Garbajosa, P.; Robustillo, A.; Baquero, F.; Coque, T.M.; Canton, R. Emergence of bla KPC-3-Tn 4401 a associated with a pKPN3/4-like plasmid within ST384 and ST388 Klebsiella pneumoniae clones in Spain. J. Antimicrob. Chemother. 2010, 65, 1608–1614. [Google Scholar] [CrossRef] [PubMed]
- Oteo, J.; Perez-Vazques, M.; Bautista, V.; Ortega, A.; Zamarron, P.; Saez, D.; Ferandez-Romero, S.; Lara, N.; Ramiro, R.; Aracil, B.; et al. The spread of KPC-producing Enterobacteriaceae in Spain: WGS analysis of the emerging high-risk clones of Klebsiella pneumoniae ST11/KPC-2, ST101/KPC-2 and ST512/KPC-3. J. Antimicrob. Chemother. 2016, 71, 3392–3399. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marí-Almirall, M.; Ferrando, N.; Fernandez, M.J.; Cosgaya, C.; Vines, J.; Rubio, E.; Cusco, A.; Munoz, L.; Pellice, M.; Vergara, A.; et al. Clonal spread and intra-and inter-species plasmid dissemination associated with Klebsiella pneumoniae carbapenemase-producing Enterobacterales during a hospital outbreak in Barcelona, Spain. Front. Microbiol. 2021, 12, 781127. [Google Scholar] [CrossRef]
- Yin, C.; Yang, W.; Lv, Y.; Zhao, P.; Wang, J. Clonal spread of carbapenemase-producing Enterobacteriaceae in a region, China. BMC Microbiol. 2022, 22, 81. [Google Scholar] [CrossRef]
- Lo, S.; Lolom, I.; Goldstein, V.; Petitjean, M.; Rondinaud, E.; Bunel-Gourdy, V.; Dinh, A.T.; Wicky, P.H.; Ruppe, E.; d’Humieres, C.; et al. Simultaneous hospital outbreaks of New Delhi Metallo-β-lactamase-producing Enterobacterales unraveled using whole-genome sequencing. Microbiol. Spectr. 2022, 10, e02287-21. [Google Scholar] [CrossRef]
- Ledda, A.; Cummins, M.; Shaw, L.P.; Janueikaite, E.; Cole, K.; Lasalle, F.; Barry, D.; Turton, J.; Rosmarin, C.; Anaraki, S.; et al. Hospital outbreak of carbapenem-resistant Enterobacterales associated with a blaOXA-48 plasmid carried mostly by Escherichia coli ST399. Microb. Genom. 2022, 4, 000675. [Google Scholar]
- Pilato, V.D.; Angelis, L.H.D.; Aiezza, N.; Baccani, I.; Niccolai, C.; Parisio, E.M.; Giordano, C.; Camarlinghi, G.; Barnini, S.; Forni, S.; et al. Resistome and virulome accretion in an NDM-1-producing ST147 sublineage of Klebsiella pneumoniae associated with an outbreak in Tuscany, Italy: A genotypic and phenotypic characterisation. Lancet Microbe 2022, 3, e224–e234. [Google Scholar] [CrossRef]
- Pirzadian, J.; Persoon, M.C.; Severin, J.A.; Klaassen, C.H.W.; Greef, S.C.D.; Mennen, M.G.; Schoffelen, A.F.; Wielders, C.C.H.; Witteveen, S.; Santen-Verheuvel, A.F.; et al. National surveillance pilot study unveils a multicenter, clonal outbreak of VIM-2-producing Pseudomonas aeruginosa ST111 in the Netherlands between 2015 and 2017. Sci. Rep. 2021, 11, 21015. [Google Scholar] [CrossRef]
- Bilal, H.; Zhang, G.; Rehman, T.; Han, J.; Khan, S.; Shafiq, M.; Yang, X.; Yan, Z.; Yang, X. First report of blaNDM-1 bearing IncX3 plasmid in clinically isolated ST11 Klebsiella pneumoniae from Pakistan. Microorganisms 2021, 9, 951. [Google Scholar] [CrossRef]
- Magiorakos, A.-P.; Srinivasan, A.; Carey, R.B.; Carmeli, Y.; Falagas, M.E.; Giske, C.G.; Harbarth, S.; Hindler, J.F.; Kahlmeter, G.; Olsson-Liljequist, B.; et al. Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria: An international expert proposal for interim standard definitions for acquired resistance. Clin. Microbiol. Infect. 2012, 18, 268–281. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liang, Q.; Yan, C.; Xu, Z.; Huang, M. Preemptive isolation and active surveillance in the prevention and control of nosocomial infection reduce the incidence of carbapenem-resistant Enterobacteriaceae. Infect. Dis. 2019, 51, 377–379. [Google Scholar] [CrossRef] [PubMed]
- Abrar, S.; Hussain, S.; Khan, R.H.; Ain, N.U.; Haider, H.; Riaz, S. Prevalence of extended-spectrum-β-lactamase-producing Enterobacteriaceae: First systematic meta-analysis report from Pakistan. Antimicrob. Resist. Infect. Control. 2018, 7, 26. [Google Scholar] [CrossRef] [Green Version]
- Naeem, S.; Bilal, H.; Muhammad, H.; Khan, M.A.; Hameed, F.; Bahadur, S.; Rehman, T.U. Detection of blaNDM-1 gene in ESBL producing Escherichia coli and Klebsiella pneumoniae isolated from urine samples. J. Infect. Dev. Ctries. 2021, 15, 516–522. [Google Scholar] [CrossRef]
- Afridi, F.I.; Sani, A.I.; Khan, R.; Baig, S.; Zaidi, A.A.A.; Jamal, Q. Increasing frequency of New Delhi Metallo-beta-Lactamase and Klebsiella pneumoniae Carbapenemase resistant genes in a set of population of Karachi. J. Coll. Physicians Surg. Pak. JCPSP 2023, 33, 59–65. [Google Scholar] [PubMed]
- Kishimbo, P.; Sogone, N.M.; Kalokola, F.; Mshana, S.E. Prevalence of gram negative bacteria causing community acquired pneumonia among adults in Mwanza City, Tanzania. Pneumonia 2020, 12, 7. [Google Scholar] [CrossRef] [PubMed]
- Bourafa, N.; Chaalal, W.; Bakour, S.; Lalaoui, R.; Boutefnouchet, N.; Diene, S.M.; Rolain, J.M. Molecular characterization of carbapenem-resistant Gram-negative bacilli clinical isolates in Algeria. Infect. Drug Resist. 2018, 11, 735. [Google Scholar] [CrossRef] [Green Version]
- Siwakoti, S.; Subedi, A.; Sharma, A.; Baral, R.; Bhattarai, N.R.; Khanal, B. Incidence and outcomes of multidrug-resistant gram-negative bacteria infections in intensive care unit from Nepal-a prospective cohort study. Antimicrob. Resist. Infect. Control. 2018, 7, 114. [Google Scholar] [CrossRef] [Green Version]
- Al-Tawfiq, J.A.; Rabaan, A.A.; Saunar, J.V.; Bazzi, A.M. Antimicrobial resistance of gram-negative bacteria: A six-year longitudinal study in a hospital in Saudi Arabia. J. Infect. Public Health 2020, 13, 737–745. [Google Scholar] [CrossRef]
- Uddin, F.; Imam, S.H.; Khan, S.; Khan, T.A.; Ahmed, Z.; Sohail, M.; Einaggar, A.Y.; Fallatah, A.M.; El-Bahy, Z.M. NDM production as a dominant feature in carbapenem-resistant Enterobacteriaceae isolates from a Tertiary Care Hospital. Antibiotics 2021, 11, 48. [Google Scholar] [CrossRef] [PubMed]
- Habib, A.; Lo, S.; Villageois-Tran, K.; Petitjean, M.; Malik, S.A.; Armand-Lefevre, L.; Ruppe, E.; Zahra, R. Dissemination of carbapenemase-producing Enterobacterales in the community of Rawalpindi, Pakistan. PLoS ONE 2022, 17, e0270707. [Google Scholar] [CrossRef] [PubMed]
- Awan, M.; Rasheed, F.; Saeed, M.; Irum, S.; Ashraf, F.; Imran, A.A. Dissemination and detection of carbapenemases producing Gram-negative rods. Pak. Armed Forces Med. J. 2019, 69, 9–14. [Google Scholar]
- Karlsson, M.; Lutgring, J.D.; Ansari, U.; Lawsin, A.; Albrecht, V.; McAllister, G.; Daniels, J.; Lonsway, D.; McKay, S.; Beldavs, Z.; et al. Molecular characterization of carbapenem-resistant Enterobacterales collected in the United States. Microb. Drug Resist. 2022, 28, 389–397. [Google Scholar] [CrossRef]
- Yu, H.; Molina, M.K.G.; Cartaya, Y.C.; Casares, M.H.; Aung, M.S.; Kobayashi, N.; Perez, D.Q. Multicenter study of Carbapenemase-producing Enterobacterales in Havana, Cuba, 2016–2021. Antibiotics 2022, 11, 514. [Google Scholar] [CrossRef]
- Guo, B.; Guo, Z.; Zhang, H.; Shi, C.; Qin, B.; Wang, S.; Chang, Y.; Chen, J.; Chen, P.; Guo, L.; et al. Prevalence and risk factors of carbapenem-resistant Enterobacterales positivity by active screening in intensive care units in the Henan Province of China: A multi-center cross-sectional study. Front. Microbiol. 2022, 13, 894341. [Google Scholar] [CrossRef]
- Ain, N.U.; Iftikhar, A.; Bukhari, S.S.; Abrar, S.; Hussain, S.; Haider, M.H.; Rasheed, F.; Riaz, S. High frequency and molecular epidemiology of metallo-β-lactamase-producing gram-negative bacilli in a tertiary care hospital in Lahore, Pakistan. Antimicrob. Resist. Infect. Control. 2018, 7, 128. [Google Scholar] [CrossRef] [Green Version]
- Imtiaz, W.; Syed, Z.; Rafaque, Z.; Andrews, S.C.; Dasti, J.I. Analysis of antibiotic resistance and virulence traits (genetic and phenotypic) in Klebsiella pneumoniae clinical isolates from Pakistan: Identification of significant levels of carbapenem and colistin resistance. Infect. Drug Resist. 2021, 14, 227–236. [Google Scholar] [CrossRef] [PubMed]
- Bulens, S.N.; Reses, H.E.; Ansari, U.A.; Grass, J.E.; Carmon, C.; Albrecht, V.; Lawsin, A.; McAllister, G.; Daniels, J.; Lee, Y.K.; et al. Carbapenem-Resistant Enterobacterales in individuals with and without health care risk factors—Emerging infections program, United States, 2012–2015. Am. J. Infect. Control. 2023, 51, 70–77. [Google Scholar] [CrossRef] [PubMed]
- Fatima, A.; Naqvi, S.B.; Khaliq, S.A.; Perveen, S.; Jabeen, S. Antimicrobial susceptibility pattern of clinical isolates of Pseudomonas aeruginosa isolated from patients of lower respiratory tract infections. SpringerPlus 2012, 1, 70. [Google Scholar] [CrossRef] [Green Version]
- Ameen, N.; Memon, Z.; Shaheen, S.; Fatima, G.; Ahmed, F. Imipenem resistant Pseudomonas aeruginosa: The fall of the final quarterback. Pak. J. Med. Sci. 2015, 31, 561. [Google Scholar] [PubMed]
- Farooq, L.; Memon, Z.; Ismail, M.Q.; Sadiq, S. Frequency and antibiogram of multi-drug resistant Pseudomonas aeruginosa in a Tertiary Care Hospital of Pakistan. Pak. J. Med. Sci. 2019, 35, 1622. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saleem, S.; Bokhari, H. Resistance profile of genetically distinct clinical Pseudomonas aeruginosa isolates from public hospitals in central Pakistan. J. Infect. Public Health 2020, 13, 598–605. [Google Scholar] [CrossRef]
- Ishfaq, R.; Khan, H.R.; Javeed, M.; Tanveer, M.I.; Ashraf, A. Prevalence and evaluation of multidrug resistance pattern of Pseudomonas aeruginosa among critical and non-critical areas at a Tertiary care hospital of Multan. J. Bioresour. Manag. 2022, 9, 8. [Google Scholar]
- Javaid, N.; Sultana, Q.; Rasool, K.; Gandra, S.; Ahmad, F.; Chaudhary, S.U.; Mirza, S. Trends in antimicrobial resistance amongst pathogens isolated from blood and cerebrospinal fluid cultures in Pakistan (2011–2015): A retrospective cross-sectional study. PLoS ONE 2021, 16, e0250226. [Google Scholar] [CrossRef] [PubMed]
- Hasan, B.; Perveen, K.; Olsen, B.; Zahra, R. Emergence of carbapenem-resistant Acinetobacter baumannii in hospitals in Pakistan. J. Med. Microbiol. 2014, 63, 50–55. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Indhar, F.; Durrani, M.A.; Bux, A.; Sohail, M. Carbapenemases among Acinetobacter species isolated from NICU of a tertairy care hospital in Karachi. JPMA 2017, 67, 1547–1551. [Google Scholar]
- Ahsan, U.; Mushtaq, F.; Saleem, S.; Malik, A.; Sarfaraz, H.; Shahzad, M.; Uhlin, B.E.; Ahmad, I. Emergence of high colistin resistance in carbapenem resistant Acinetobacter baumannii in Pakistan and its potential management through immunomodulatory effect of an extract from Saussurea lappa. Front. Pharmacol. 2022, 13, 986802. [Google Scholar] [CrossRef]
- Tacconelli, E.; Carrara, E.; Savoldi, A.; Harbarth, S.; Mendelson, M.; Monnet, D.L.; Pulcini, C.; Kahlmeter, G.; Kluytmans, J.; Carmeli, Y.; et al. Discovery, research, and development of new antibiotics: The WHO priority list of antibiotic-resistant bacteria and tuberculosis. Lancet Infect. Dis. 2018, 18, 318–327. [Google Scholar] [CrossRef] [PubMed]
- Din, M.; Babar, K.M.; Ahmad, S.; Aleem, A.; Shah, D.; Ghilzai, D.; Ahmed, N. Prevalence of extensive drug resistance in bacterial isolates harboring blaNDM-1 in Quetta Pakistan. Pak. J. Med. Sci. 2019, 35, 1155. [Google Scholar]
- Khan, I.; Sarwar, N.; Ahmad, B.; Azam, S.; Rehman, N. Identification and antimicrobial susceptibility profile of bacterial pathogens isolated from wound infections in a teaching hospital, Peshawar, Pakistan. Adv. Life Sci. 2017, 5, 8–12. [Google Scholar]
- Gul, F.; Bacha, N.; Khan, Z.; Khan, S.A.; Mir, A.; Amin, I. Characterization and antibiotic susceptibility pattern of Uropathogens from Khyber Pakhtunkhwa, Pakistan. J. Med. Sci. 2017, 25 (Suppl. S1), 153–157. [Google Scholar]
- Nasir, A.; Iqbal, M.N.; Hassan, G.; Abbas, M.A.; Jawad, H.; Raheem, A.; Zahid, A. Frequency of most prevalent bacteria in wound of diabetic foot ulcers and their antimicrobial susceptibility to different antibiotics. Pak. J. Med. Health Sci. 2021, 15, 2223–2225. [Google Scholar]
- Tran, D.M.; Larsson, M.; Olsen, L.; Hoang, N.T.B.; Le, N.K.; Khu, D.T.K.; Nguyen, H.D.; Vu, T.V.; Trinh, T.H.; Le, T.Q.; et al. High prevalence of colonisation with carbapenem-resistant Enterobacteriaceae among patients admitted to Vietnamese hospitals: Risk factors and burden of disease. J. Infect. 2019, 79, 115–122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amalia, E.; Sabrina, T.; Patricia, V.; Husna, R.; Rosdah, A.A. Identification of carbapenemases Enterobacteriaceae producing gene blaVIM in clinical isolates. J. Phys. Conf. Ser. 2019, 1246, 012004. [Google Scholar] [CrossRef]
- Han, Y.H.; Bae, M.J.; Hur, Y.R.; Hwang, K. Prevalence and risk factors for carbapenem-resistant Enterobacteriaceae colonization in patients with stroke. Brain Neurorehabilit. 2019, 12, e16. [Google Scholar] [CrossRef]
- Biswas, S.; Bhat, V.; Kelkar, R. Carbapenem-resistant Enterobacteriaceae: A serious concern in cancer patients. Microbiol. Soc. 2020, 2, po0008. [Google Scholar] [CrossRef]
- Kotb, S.; Lyman, M.; Ismail, G.; Fattah, M.A.E.; Girgis, S.A.; Etman, A.; Hafez, S.; El-Kholy, J.; Zaki, M.E.S.; Rashed, H.A.G.; et al. Epidemiology of carbapenem-resistant Enterobacteriaceae in Egyptian intensive care units using National Healthcare–associated Infections Surveillance Data, 2011–2017. Antimicrob. Resist. Infect. Control. 2020, 9, 2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adesanya, O.A.; Igwe, H.A. Carbapenem-resistant Enterobacteriaceae (CRE) and Gram-negative bacterial infections in south-west Nigeria: A retrospective epidemiological surveillance study. AIMS Public Health 2020, 7, 804. [Google Scholar] [CrossRef]
- David, S.; Reuter, S.; Harris, S.R.; Glasner, C.; Feltwell, T.; Argimon, S.; Abudahab, K.; Goater, R.; Giani, T.; Errico, G.; et al. Epidemic of carbapenem-resistant Klebsiella pneumoniae in Europe is driven by nosocomial spread. Nat. Microbiol. 2019, 4, 1919–1929. [Google Scholar] [CrossRef] [PubMed]
- Gajdács, M.; Abrok, M.; Lazar, A.; Janvari, L.; Toth, A.; Terhes, G.; Burian, K. Detection of VIM, NDM and OXA-48 producing carbapenem resistant Enterobacterales among clinical isolates in Southern Hungary. Acta Microbiol. Immunol. Hung. 2020, 67, 209–215. [Google Scholar] [CrossRef]
- Wielders, C.C.H.; Schouls, L.M.; Woudt, S.H.S.; Notermans, D.W.; Hendrickx, A.P.A.; Bakker, J.; Kuijper, E.J.; Schoffelen, A.F.; Greeff, S.C. Epidemiology of carbapenem-resistant and carbapenemase-producing Enterobacterales in the Netherlands 2017–2019. Antimicrob. Resist. Infect. Control. 2022, 11, 57. [Google Scholar] [CrossRef]
- Yoon, E.-J.; Jeong, S.H. Mobile carbapenemase genes in Pseudomonas aeruginosa. Front. Microbiol. 2021, 12, 614058. [Google Scholar] [CrossRef]
- Rus, M.; Licker, M.; Musuroi, C.; Seclaman, E.; Muntean, D.; Cirlea, N.; Tamas, A.; Vulpie, S.; Horhat, F.G.; Baditoiu, L. Distribution of NDM1 carbapenemase-producing Proteeae strains on high-risk hospital wards. Infect. Drug Resist. 2020, 13, 4751–4761. [Google Scholar] [CrossRef] [PubMed]
- Ghaith, D.M.; Mohamed, Z.K.; Farhat, M.G.; Shahin, W.A.; Mohamed, H.O. Colonization of intestinal microbiota with carbapenemase-producing Enterobacteriaceae in paediatric intensive care units in Cairo, Egypt. Arab. J. Gastroenterol. 2019, 20, 19–22. [Google Scholar] [CrossRef]
- Soria-Segarra, C.; Soria-Segarra, C.; Catagua-Gonzalez, A.; Gutierrez-Fernandez, J. Carbapenemase producing Enterobacteriaceae in intensive care units in Ecuador: Results from a multicenter study. J. Infect. Public Health 2020, 13, 80–88. [Google Scholar] [CrossRef]
- Jean, S.-S.; Hsueh, P.-R. High burden of antimicrobial resistance in Asia. Int. J. Antimicrob. Agents 2011, 37, 291–295. [Google Scholar] [CrossRef]
- Cantón, R.; Huarte, R.; Morata, L.; Trillo-Mata, J.L.; Munoz, R.; Gonzalez, J.; Tort, M.; Badia, X. Determining the burden of infectious diseases caused by carbapenem-resistant Gram-negative bacteria in Spain. Enferm. Infecc. Microbiol. Clínica 2021, 39, 179–183. [Google Scholar] [CrossRef] [PubMed]
- Laxminarayan, R.; Sridhar, D.; Blaser, M.; Wang, M.; Woolhouse, M. Achieving global targets for antimicrobial resistance. Science 2016, 353, 874–875. [Google Scholar] [CrossRef] [Green Version]
- Du, D.; Wang-Kan, X.; Neuberger, A.; Veen, H.W.V.; Pos, K.M.; Piddock, L.J.V.; Luisi, B.F. Multidrug efflux pumps: Structure, function and regulation. Nat. Rev. Microbiol. 2018, 16, 523–539. [Google Scholar] [CrossRef]
- Braun, S.D.; Jamil, B.; Syed, M.A.; Abbasi, S.A.; Weisse, D.; Slickers, P.; Monecke, S.; Engelmann, I.; Ehricht, R. Prevalence of carbapenemase-producing organisms at the Kidney Center of Rawalpindi (Pakistan) and evaluation of an advanced molecular microarray-based carbapenemase assay. Future Microbiol. 2018, 13, 1225–1246. [Google Scholar] [CrossRef] [Green Version]
- Qamar, M.U.; Walsh, T.R.; Toleman, M.A.; Tyrrell, J.M.; Saleem, S.; Aboklaish, A.; Jahan, S. Dissemination of genetically diverse NDM-1,-5,-7 producing-Gram-negative pathogens isolated from pediatric patients in Pakistan. Future Microbiol. 2019, 14, 691–704. [Google Scholar] [CrossRef]
- Masseron, A.; Poirel, L.; Ali, B.J.; Syed, M.A.; Nordmann, P. Molecular characterization of multidrug-resistance in Gram-negative bacteria from the Peshawar teaching hospital, Pakistan. New Microbes New Infect. 2019, 32, 100605. [Google Scholar] [CrossRef] [PubMed]
- Haider, M.H.; McHugh, T.D.; Roulston, K.; Arruda, L.B.; Sadouki, Z.; Riaz, S. Detection of carbapenemases blaOXA48-blaKPC-blaNDM-blaVIM and extended-spectrum-β-lactamase blaOXA1-blaSHV-blaTEM genes in Gram-negative bacterial isolates from ICU burns patients. Ann. Clin. Microbiol. Antimicrob. 2022, 21, 18. [Google Scholar] [CrossRef] [PubMed]
- Akhtar, J.; Saleem, S.; Shahzad, N.; Waheed, A.; Jameel, I.; Rasheed, F.; Jahan, S. Prevalence of Metallo-β-lactamase IMP and VIM producing Gram negative bacteria in different hospitals of Lahore, Pakistan. Pak. J. Zool. 2018, 50, 2343–2349. [Google Scholar] [CrossRef]
- Hadjadj, L.; Syed, M.A.; Abbasi, S.A.; Rolain, J.M.; Jamil, B. Diversity of carbapenem resistance mechanisms in clinical Gram-negative bacteria in Pakistan. Microb. Drug Resist. 2021, 27, 760–767. [Google Scholar] [CrossRef]
- Zahra, N.; Zeshan, B.; Qadri, M.M.A.; Ishaq, M.; Afzal, M.; Ahmed, N. Phenotypic and genotypic evaluation of antibiotic resistance of Acinetobacter baumannii bacteria isolated from surgical intensive care unit patients in Pakistan. Jundishapur J. Microbiol. 2021, 14, e113008. [Google Scholar] [CrossRef]
- Aslam, B.; Chaudhary, T.H.; Arshad, M.I.; Muzammil, S.; Siddique, A.B.; Yasmeen, N.; Khurshid, M.; Amir, A.; Salman, M.; Rasool, M.H.; et al. Distribution and genetic diversity of multi-drug-resistant Klebsiella pneumoniae at the human–animal–environment interface in Pakistan. Front. Microbiol. 2022, 13, 898248. [Google Scholar] [CrossRef]
- European Committee on Antimicrobial Susceptibility Testing. European Committee on Antimicrobial Susceptibility Testing Breakpoint tables for interpretation of MICs and zone diameters, Version 5.0; European Committee on Antimicrobial Susceptibility Testing: Växjö, Sweden, 2015. [Google Scholar]
- Pierce, V.M.; Simner, P.J.; Lonsway, D.R.; Roe-Carpenter, D.E.; Johnson, J.K.; Brasso, W.B.; Bobenchik, A.M.; Lockett, Z.C.; Charnot-Katsikas, A.; Ferraro, M.J.; et al. Modified carbapenem inactivation method for phenotypic detection of carbapenemase production among Enterobacteriaceae. J. Clin. Microbiol. 2017, 55, 2321–2333. [Google Scholar] [CrossRef] [Green Version]
- Dashti, A.A.; Jadaon, M.M.; Abdulsamad, A.M.; Dashti, H.M. Heat treatment of bacteria: A simple method of DNA extraction for molecular techniques. Kuwait Med. J. 2009, 41, 117–122. [Google Scholar]
- Diancourt, L.; Passet, V.; Verhoef, J.; Grimont, P.A.D.; Brisse, S. Multilocus sequence typing of Klebsiella pneumoniae nosocomial isolates. J. Clin. Microbiol. 2005, 43, 4178–4182. [Google Scholar] [CrossRef] [Green Version]
- Jaureguy, F.; Landraud, L.; Passet, V.; Diancourt, L.; Frapy, E.; Guigon, G.; Carbonnelle, E.; Lortholary, O.; Clermont, O.; Denamur, E.; et al. Phylogenetic and genomic diversity of human bacteremic Escherichia coli strains. BMC Genom. 2008, 9, 560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carloni, E.; Andreoni, F.; Omiccioli, E.; Villa, L.; Magnani, M.; Carattoli, A. Comparative analysis of the standard PCR-Based Replicon Typing (PBRT) with the commercial PBRT-KIT. Plasmid 2017, 90, 10–14. [Google Scholar] [CrossRef]
- Brolund, A.; Rajer, F.; Giske, C.G.; Melefors, O.; Titelman, E.; Sandegren, L. Dynamics of resistance plasmids in extended-spectrum-β-lactamase-producing Enterobacteriaceae during postinfection colonization. Antimicrob. Agents Chemother. 2019, 63, e02201–e02218. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rajivgandhi, G.; Maruthupandy, M.; Ramachandran, G.; Priyanga, M.; Manoharan, N. Detection of ESBL genes from ciprofloxacin resistant Gram negative bacteria isolated from urinary tract infections (UTIs). Front. Lab. Med. 2018, 2, 5–13. [Google Scholar] [CrossRef]


{kind=link}
| K. pneumoniae | E. coli | Pseudomo- nas spp. | Acinetob- acter spp. | Citrobac- ter spp. | Proteus spp. | Morgane- lla spp. | Provide-ncia spp. | Burkhold- eria spp. | |
|---|---|---|---|---|---|---|---|---|---|
| Clinical specimens n (%) | |||||||||
| Wound | 187 (28.1) | 106 (19.5) | 126 (32.8) | 40 (24.5) | 39 (36.8) | 56 (32.0) | 13 (23.6) | 13 (27.1) | 7 (26.0) |
| Pus | 114 (17.1) | 111 (20.4) | 96 (25.0) | 47 (28.8) | 21 (19.8) | 47 (26.9) | 14 (25.4) | 18 (37.5) | 5 (18.5) |
| Blood | 92 (13.8) | 87 (16.1) | 29 (7.6) | 18 (11.0) | 9 (8.5) | 15 (8.6) | 5 (9.1) | 2 (4.2) | 4 (14.8) |
| Urine | 37 (5.5) | 105 (19.3) | 26 (6.8) | 7 (4.3) | 4 (3.8) | 8 (4.6) | 5 (9.1) | 5 (10.4) | 7 (26.0) |
| Sputum | 45 (6.7) | 30 (5.5) | 18 (4.7) | 8 (4.9) | 8 (7.5) | 5 (2.6) | 8 (14.5) | 2 (4.2) | 3 (11.1) |
| Tracheal secretion | 43 (6.4) | 21 (3.7) | 10 (2.6) | 13 (8.0) | 2 (1.9) | 7 (4.0) | - | 4 (8.3) | 1 (3.7) |
| ETT | 40 (6.1) | 10 (1.8) | 14 (3.6) | 3 (1.8) | 8 (7.5) | 3 (1.7) | - | 2 (4.2) | - |
| Tissue | 30 (4.5) | 20 (3.7) | 11 (2.9) | 5 (3.1) | 4 (3.8) | 2 (1.1) | - | 2 (4.2) | - |
| Tip cells | 20 (3.1) | 13 (2.4) | 19 (5.0) | 4 (2.5) | 1 (0.9) | 10 (5.7) | 3 (5.5) | - | - |
| Drain | 23 (3.4) | 15 (2.7) | 13 (3.4) | 4 (2.5) | 3 (2.8) | 4 (2.3) | 4 (7.3) | - | - |
| Pleural fluid | 18 (2.7) | 16 (3.1) | 13 (3.4) | 6 (3.7) | 3 (2.8) | 9 (5.1) | 1 (1.8) | - | - |
| CV line | 19 (2.8) | 10 (1.8) | 9 (2.3) | 8 (4.9) | 4 (3.8) | 9 (5.1) | 2 (3.6) | - | - |
| Total | 668 | 544 | 384 | 163 | 106 | 175 | 55 | 48 | 27 |
| Clinical wards n (%) | |||||||||
| General surgery | 182 (27.2) | 141 (26.0) | 120 (31.3) | 41 (25.2) | 24 (22.6) | 55 (31.4) | 20 (36.4) | 18 (37.5) | 7 (25.9) |
| ICU | 144 (21.5) | 139 (25.5) | 47 (12.2) | 24 (14.7) | 14 (13.2) | 21 (12.0) | 12 (21.8) | 6 (12.5) | 5 (18.5) |
| General medicine | 104 (15.6) | 91 (16.7) | 60 (15.6) | 39 (23.9) | 14 (13.2) | 30 (17.1) | 10 (18.2) | 7 (14.6) | 5 (18.5) |
| Dermatology | 60 (9.0) | 17 (3.1) | 33 (8.6) | 11 (6.7) | 11 (10.4) | 16 (9.1) | - | 1 (2.1) | - |
| Pediatric medicine | 44 (6.7) | 14 (2.6) | 39 (10.2) | 3 (1.8) | 12 (11.3) | 12 (6.9) | - | 3 (6.3) | 4 (14.8) |
| Cardiology | 28 (4.2) | 37 (6.8) | 19 (4.9) | 12 (7.4) | 7 (6.6) | 8 (4.6) | 4 (7.3) | 3 (6.3) | 3 (11.1) |
| Chest medicine | 46 (6.9) | 17 (3.1) | 19 (4.9) | 8 (4.9) | 6 (5.7) | 5 (2.9) | 5 (9.1) | 2 (4.2) | - |
| Nephrology | 20 (3.0) | 41 (7.5) | 15 (3.9) | 6 (3.7) | 4 (3.8) | 8 (4.6) | - | 2 (4.2) | 3 (11.1) |
| Orthopedic surgery | 28 (4.2) | 19 (3.5) | 17 (4.4) | 7 (4.3) | 5 (4.7) | 10 (5.7) | 4 (7.3) | 2 (4.2) | - |
| Oncology | 8 (1.2) | 25 (4.6) | 9 (2.3) | 7 (4.3) | 4 (3.8) | 5 (2.9) | - | 2 (4.2) | - |
| Neurology | 4 (0.6) | 3 (0.5) | 6 (1.0) | 5 (3.1) | 5 (4.7) | 5 (2.9) | - | 2 (4.2) | - |
| Total | 668 | 544 | 384 | 163 | 106 | 175 | 55 | 48 | 27 |
| K. pneumoniae | E. coli | Pseudomonas spp. | Acinetobacter spp. | Citrobacter spp. | Proteus spp. | Providencia spp. | Morganella spp. | Burkholderia spp. | |
|---|---|---|---|---|---|---|---|---|---|
| Antibiotics n (%) | |||||||||
| IMP/MEM | 309 (46.2) | 223 (41.1) | 169 (44.0) | 67 (41.1) | 45 (42.4) | 61 (34.8) | 19 (34.5) | 15 (31.2) | 5 (18.5) |
| CFZ | 569 (85.2) | 473 (86.9) | - | - | - | - | 36 (65.4) | - | 23 (85.1) |
| CXM | 592 (88.6) | 438 (80.5) | - | - | 78 (73.6) | 123 (70.3) | 31 (56.4) | - | 23 (85.1) |
| CAZ | 563 (84.3) | 440 (80.8) | 357 (92.9) | 153 (93.8) | 73 (68.8) | 129 (73.7) | 37 (67.3) | 23 (47.9) | 24 (88.9) |
| CTX | 547 (81.8) | 442 (81.2) | - | 145 (88.9) | 67 (63.2) | 119 (68.0) | 37 (67.3) | 23 (47.9) | 21 (77.7) |
| FEP | 573 (85.8) | 441 (81.0) | 367 (95.5) | 145 (88.9) | 73 (68.8) | 121 (69.1) | 36 (65.4) | 29 (60.4) | 23 (85.1) |
| FOX | 527 (78.8) | 438 (80.5) | - | - | - | 93 (53.1) | 36 (65.4) | 31 (64.6) | - |
| CPT | 483 (72.3) | 439 (80.7) | - | - | - | - | - | - | - |
| AMP | 598 (89.5) | 479 (88.0) | - | - | - | - | 47 (85.4.0) | - | 25 (92.6) |
| AMC | 581 (87.0) | 487 (89.5) | - | - | - | 116 (66.3) | 43 (78.1) | - | 24 (88.8) |
| ATM | 475 (71.1) | 469 (86.2) | 344 (89.6) | - | 57 (53.7) | 113 (64.6) | 33 (60.0) | 21 (43.7) | 24 (88.8) |
| CIP | 467 (70.0) | 402 (73.9) | 346 (90.1) | 135 (82.8) | 49 (46.2) | 97 (55.4) | 37 (67.3) | 25 (52.0) | 21 (77.7) |
| SXT | 392 (58.7) | 354 (65.1) | - | 158 (96.9) | - | - | - | - | - |
| TGC | 36 (5.4) | 51 (9.3) | - | - | 5 (4.7) | - | 7 (12.7) | - | - |
| FOS | - | 183 (33.6) | 167 (43.5) | - | - | - | - | - | - |
| PB | 22 (3.3) | - | 52 (13.5) | 17 (10.4) | - | - | - | - | - |
| DO | 232 (34.8) | 223 (41.0) | - | 30 (18.4) | - | - | - | - | - |
| AK | 275 (41.2) | 387 (71.1) | 256 (66.7) | 27 (16.5) | 35 (33.0) | 54 (30.8) | - | 19 (39.6) | 19 (70.1) |
| TZP | 297 (44.6) | 207 (38.0) | 223 (58.0) | 29 (17.8) | 49 (46.2) | 23 (13.1) | 21 (38.1) | 23 (47.9) | 23 (85.1) |
| SAM | - | - | - | 63 (38.6) | - | - | - | - | - |
| K. pneumoniae | E. coli | Pseudomonas spp. | Acinetobacter spp. | Citrobacter spp. | Proteus spp. | Morganella spp. | Providencia spp. | Burkholderia spp. | p-Value | |
|---|---|---|---|---|---|---|---|---|---|---|
| Clinical specimens n (%) | ||||||||||
| Wound | 107 (34.6) | 51 (22.9) | 67 (39.6) | 18 (26.9) | 16 (35.6) | 19 (31.1) | 6 (40.0) | 7 (36.8) | 1 (20.0) | 0.00001 |
| Pus | 56 (18.1) | 43 (19.3) | 38 (22.5) | 21 (31.3) | 13 (28.9) | 21 (34.4) | 4 (26.7) | 8 (42.1) | 2 (40.0) | 0.461 |
| Urine | 20 (6.5) | 63 (28.3) | 13 (7.7) | 1 (1.5) | 1 (2.2) | 4 (6.6) | 1 (6.7) | - | - | 0.010 |
| Blood | 29 (9.4) | 29 (13.0) | 17 (10.1) | 7 (10.4) | 4 (8.9) | 9 (14.8) | - | - | 2 (40.0) | 0.086 |
| Sputum | 19 (6.1) | 11 (4.9) | 5 (3.0) | 4 (6.0) | 3 (6.7) | 2 (3.3) | 2 (13.3) | - | - | 0.168 |
| Tracheal secretion | 24 (7.8) | 6 (2.7) | 2 (1.2) | 5 (7.5) | - | 2 (3.3) | - | 2 (10.5) | - | 0.757 |
| ETT | 13 (4.2) | 5 (2.2) | 6 (3.6) | 2 (3.0) | 3 (6.7) | - | - | 2 (10.5) | - | 0.539 |
| Pleural fluid | 8 (2.6) | 4 (1.8) | 3 (1.8) | 3 (4.5) | 1 (2.2) | 2 (3.3) | 1 (6.7) | - | - | 0.144 |
| Tip cells | 9 (2.9) | 3 (1.3) | 6 (3.6) | 1 (1.5) | - | 2 (3.3) | - | - | - | 0.037 |
| Drain | 14 (4.5) | 2 (0.9) | 5 (3.0) | - | - | - | - | - | - | 0.086 |
| CV line | 6 (1.9) | 3 (1.3) | 4 (2.4) | 4 (6.0) | 2 (4.4) | - | 1 (6.7) | - | - | 0.136 |
| Tissue | 4 (1.3) | 3 (1.3) | 3 (1.8) | 1 (1.5) | 2 (4.4) | - | - | - | - | 0.00001 |
| Total | 309 | 223 | 169 | 67 | 45 | 61 | 15 | 19 | 5 | |
| Clinical wards n (%) | ||||||||||
| General surgery | 83 (26.9) | 57 (25.6) | 53 (31.4) | 21 (31.3) | 13 (28.9) | 20 (32.8) | 6 (40.0) | 8 (42.1) | 1 (20.0) | 0.548 |
| General medicine | 81 (26.2) | 35 (15.7) | 27 (16.0) | 13 (19.4) | 7 (15.6) | 13 (21.3) | 2 (13.3) | 2 (10.5) | - | 0.0008 |
| ICU | 55 (17.8) | 41 (18.4) | 27 (16.0) | 13 (19.4) | 5 (11.1) | 9 (14.8) | 4 (26.7) | 2 (10.5) | 1 (20.0) | 0.069 |
| Dermatology | 17 (5.5) | 11 (4.9) | 16 (9.5) | 6 (9.0) | 5 (11.1) | 4 (6.6) | - | - | - | 0.525 |
| Cardiology | 19 (6.1) | 19 (8.5) | 5 (3.0) | 2 (3.0) | 3 (6.7) | 3 (4.9) | - | 2 (10.5) | 2 (40.0) | 0.438 |
| Pediatric medicin | 17 (5.5) | 7 (3.1) | 15 (8.9) | 3 (4.5) | 5 (11.1) | 4 (6.6) | - | 2 (10.5) | 1 (20.0) | 0.838 |
| Nephrology | 11 (3.6) | 28 (12.6) | 7 (4.1) | - | 1 (2.2) | 3 (4.9) | - | - | - | 0.081 |
| Chest medicine | 12 (3.9) | 11 (4.9) | 11 (6.5) | 3 (4.5) | 1 (2.2) | 1 (1.6) | 3 (20.0) | - | - | 0.491 |
| Orthopedic surgery | 11 (3.6) | 4 (1.8) | 6 (3.6) | 4 (6.0) | 2 (4.4) | 2 (3.3) | - | 1 (5.3) | - | 0.060 |
| Oncology | 1 (0.3) | 9 (4.0) | 1 (0.6) | 2 (3.0) | 1 (2.2) | - | - | 1 (5.3) | - | 0.006 |
| Neurology | 2 (0.6) | 1 (0.4) | 1 (0.6) | - | 2 (4.4) | 2 (3.3) | - | 1 (5.3) | - | 0.177 |
| Total | 309 | 223 | 169 | 67 | 45 | 61 | 15 | 19 | 5 | |
| Strains | Resistance Profile | Carbapenemase Genes n (%) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| XDR | MDR | blaNDM-1 | blaOXA-48 | blaKPC-2 | blaVIM | blaIMP | blaNDM-1/ blaOXA-48 | blaOXA-48/ blaVIM | blaOXA-48/ blaIMP | blaVIM/ blaIMP | |
| K. pneumoniae | 27 (11.5) | 197 (88.5) | 83 (35.5) | 69 (29.5) | 36 (15.4) | 4 (1.7) | - | 37 (15.8) | 5 (2.1) | - | - |
| E. coli | 19 (13.4) | 124 (86.6) | 68 (47.5) | 53 (37.1) | - | 3 (2.1) | - | 13 (9.1) | 6 (4.2) | - | - |
| Pseudomonas spp. | 21 (15.7) | 112 (84.3) | 37 (27.8) | 41 (30.8) | - | 11 (8.3) | 16 (12.0) | 16 (12.0) | 9 (6.7) | 1 (0.7) | 2 (1.5) |
| Proteus spp. | 3 (6.5) | 43 (93.5) | 25 (54.3) | 17 (39.5) | - | - | 1 (2.2) | 3 (6.5) | - | - | - |
| Acinetobacter spp. | 9 (19.1) | 38 (80.9) | 29 (61.7) | 14 (29.7) | - | 1 (2.1) | - | 3 (6.4) | - | - | - |
| Citrobacter spp. | 2 (7.6) | 24 (92.4) | 17 (65.4) | 9 (34.6) | - | - | - | - | - | - | - |
| Providencia spp. | 1 (9.1) | 10 (90.9) | 5 (45.4) | 4 (36.4) | - | - | - | 2 (18.2) | - | - | - |
| Morganella spp. | - | 6 (100) | 2 (33.3) | 3 (50.0) | - | - | 1 (16.6) | - | - | - | - |
| Burkholderia spp. | - | 3 (100) | 1 (33.3) | 2 (66.7) | - | - | - | - | - | - | - |
| Total | 92 | 557 | 267 | 212 | 36 | 19 | 18 | 74 | 20 | 1 | 2 |
| blaNDM-1 | blaOXA-48 | blaKPC-2 | blaVIM | blaIMP | blaNDM-1/ blaOXA-48 | blaOXA-48/ blaVIM | blaOXA-48/ blaIMP | blaVIM/ blaIMP | |
|---|---|---|---|---|---|---|---|---|---|
| Clinical specimens n (%) | |||||||||
| Wound | 82 (30.7) p = 0.041 | 78 (36.8) p = 0.575 | 17 (47.2) p = 0.123 | 7 (36.8) p = 0.885 | - | 38 (51.4) p = 0.002 | 6 (30.0) p = 0.615 | - | 1 (50.0) p = 0.662 |
| Pus | 69 (25.8) p = 0.223 | 49 (23.1) p = 0.897 | 4 (11.1) p = 0.072 | 2 (10.5) p = 0.177 | 9 (50.0) p = 0.006 | 15 (20.3) p = 0.496 | 3 (15.0) p = 0.366 | - | 1 (50.0) p = 0.374 |
| Blood | 21 (7.9) p = 0.221 | 15 (7.1) p = 0.134 | 6 (16.7) p = 0.135 | 2 (10.5) p = 0.883 | 2 (11.1) p = 0.819 | 13 (17.6) p = 0.012 | 2 (10.0) p = 0.944 | 1 (100) | - |
| Tracheal secretion | 11 (4.1) p = 0.965 | 8 (3.8) p = 0.731 | - | 5 (26.3) p < 0.001 | 2 (11.1) p = 0.134 | 1 (1.4) p = 0.198 | - | - | - |
| Sputum | 14 (5.2) p = 0.641 | 14 (6.6) p = 0.128 | - | 1 (5.3) p = 0.919 | - | 2 (2.7) p = 0.374 | - | - | - |
| Urine | 37 13.9) p = 0.154 | 19 (9.0) p = 0.129 | 7 (19.4) p = 0.137 | - | 3 (16.7) p = 0.507 | 1 (1.4) p = 0.003 | 9 (45.0) p < 0.001 | - | - |
| Tissue | 3 (1.1) p = 0.657 | 2 (0.9) p = 0972 | - | - | - | 1 (1.4) p = 0.683 | - | - | - |
| Drain | 4 (1.5) p = 0.745 | 4 (1.9) p = 0.791 | - | - | - | 3 (4.1) p = 0.094 | - | - | - |
| CV line | 3 (1.1) p = 0.926 | 2 (0.9) p = 0.816 | - | - | 2 (11.1) p < 0.001 | - | - | - | - |
| ETT | 10 (3.7) p = 0.301 | 7 (3.3) p = 0.693 | 2 (5.6) p = 0.335 | - | - | - | - | - | - |
| Pleural fluid | 8 (3.0) p = 0.131 | 5 (2.4) p = 0.652 | - | - | - | - | - | - | - |
| Tip cells | 5 (1.9) p = 0.415 | 9 (4.2) p = 0.041 | - | 2 (10.5) p = 0.021 | - | - | - | - | - |
| Total | 267 | 212 | 36 | 19 | 18 | 74 | 20 | 1 | 2 |
| Clinical wards n (%) | |||||||||
| General surgery | 67 (25.1) p = 0.170 | 43 (20.3) p = 0.001 | 16 (44.4) p = 0.029 | 9 (47.4) p = 0.064 | 7 (38.9) p = 0.322 | 36 (48.6) p < 0.001 | 4 (20.0) p = 0.392 | 1 (100) | 2 (100) |
| ICU | 74 (27.7) p < 0.001 | 23 (10.8) p < 0.001 | 7 (19.4) p = 0.286 | 2 (10.5) p = 0.313 | 5 (27.8) p = 0.373 | 15 (20.3) p = 0.871 | 1 (5.0) p = 0.095 | - | - |
| General medicine | 57 (21.3) p = 0.971 | 59 (27.8) p = 0.005 | 6 (16.7) p = 0.474 | - | 1 (5.6) p = 0.096 | 13 (17.6) p = 0.391 | 3 (15.0) p = 0.477 | - | - |
| Dermatology | 19 (7.1) p = 0.321 | 14 (6.6) p = 0.657 | 4 (11.1) p = 0.185 | 2 (10.5) p = 0.401 | - | - | - | - | - |
| Nephrology | 11 (4.1) p = 0.901 | 3 (1.4) p = 0.020 | - | 2 (10.5) p = 0.141 | - | 3 (4.1) p = 0.982 | 7 (35.0) p < 0.001 | - | - |
| Chest medicine | 9 (3.4) p = 0.870 | 9 (4.2) p = 0.311 | - | - | 3 (16.7) p = 0.001 | - | - | - | - |
| Cardiology | 9 (3.4) p = 0.042 | p = 19 (9.0) p = 0.008 | - | - | - | 5 (6.8) p = 0.629 | 3 (15.0) p = 0.060 | - | - |
| Pediatric medicine | 9 (3.4) p = 0.013 | 23 (10.8) p < 0.001 | 3 (8.3) p = 0.577 | 1 (5.3) p = 0.868 | 2 (11.1) p = 0.376 | - | 2 (10.0) p = 0.468 | - | - |
| Neurology | 2 (0.7) p = 0.958 | 3 (1.4) p = 0.190 | - | - | - | - | - | - | - |
| Oncology | 3 (1.1) p = 0.631 | 3 (1.4) p = 0.965 | - | 3 (15.8) p < 0.001 | - | - | - | - | - |
| Orthopedic surgery | 7 (2.6) p = 0.365 | p = 13 (6.1) p = 0.007 | - | - | - | 2 (2.7) p = 0.728 | - | - | - |
| Total | 267 | 212 | 36 | 19 | 18 | 74 | 20 | 1 | 2 |
| Sequence Type (n) | Carbapenemases | ESBL Resistance Genes | Replicon Type | |
|---|---|---|---|---|
| K. pneumoniae | ST147 (4) | blaKPC-2 | blaSHV/blaTEM | IncFII, IncA/C, IncN, IncL/M |
| ST147 (9) | blaKPC-2 | blaSHV/blaCTX-M | IncFII, IncA/C, IncN, IncL/M | |
| ST147 (3) | blaKPC-2 | blaSHV/blaCTX-M/blaTEM | IncFII, IncA/C, IncN, IncL/M | |
| ST147 (13) | blaNDM-1 | blaSHV/blaCTX-M | IncFII, IncFIIK, IncA/C, IncN, IncL/M | |
| ST147 (7) | blaNDM-1 | blaSHV/blaTEM | IncFII, IncA/C, IncN, IncL/M | |
| ST147 (3) | blaNDM-1 | blaSHV | IncFII, IncA/C, IncN, IncL/M | |
| ST147 (5) | blaNDM-1 | blaSHV/blaCTX-M/blaTEM | IncFII, IncA/C, IncN, IncL/M | |
| ST147 (2) | blaNDM-1 | blaCTX-M | IncFII, IncA/C, IncN, IncL/M | |
| ST147 (5) | blaNDM-1 | blaCTX-M/blaTEM | IncFII, IncA/C, IncN, IncL/M | |
| ST147 (9) | blaNDM-1/blaOXA-48 | blaSHV/blaCTX-M | IncL/M, IncFII, IncA/C | |
| ST147 (3) | blaNDM-1/blaOXA-48 | blaSHV | IncL/M, IncFII, IncA/C | |
| ST147 (5) | blaNDM-1/blaOXA-48 | blaCTX-M | IncL/M, IncFII, IncA/C | |
| ST258 (7) | blaKPC-2 | blaSHV/blaCTX-M | IncFIIA, IncA/C, IncL/M | |
| ST258 (3) | blaKPC-2 | blaCTX-M/blaTEM | IncFIIA, IncA/C, IncL/M | |
| ST258 (7) | blaNDM-1/blaOXA-48 | blaSHV/blaCTX-M | IncL/M, IncFII | |
| ST340 (5) | blaNDM-1 | blaSHV/blaCTX-M | IncFII, IncA/C | |
| ST340 (3) | blaNDM-1 | blaSHV | IncFII, IncA/C | |
| ST11 (2) | blaKPC-2 | blaCTX-M | IncFIIA, IncA/C, IncL/M | |
| ST11 (5) | blaKPC-2 | blaSHV/blaCTX-M | IncFIIA, IncA/C, IncL/M | |
| ST11 (3) | blaKPC-2 | blaSHV | IncFIIA, IncA/C, IncL/M | |
| ST11 (11) | blaNDM-1 | blaCTX-M | IncFII, IncA/C, IncN, IncL/M | |
| ST11 (7) | blaNDM-1 | blaSHV/blaCTX-M | IncFII, IncA/C, IncN, IncL/M | |
| ST11 (3) | blaNDM-1 | blaSHV/blaCTX-M/blaTEM | IncFII, IncA/C, IncN, IncL/M | |
| ST11 (1) | blaNDM-1 | blaSHV | IncFII, IncA/C, IncN, IncL/M | |
| ST11 (13) | blaNDM-1/blaOXA-48 | blaSHV | IncL/M, IncFII, IncN | |
| ST14 (7) | blaNDM-1 | blaSHV/blaCTX-M | IncFII, IncA/C, IncN, IncL/M, IncFIIK | |
| ST14 (5) | blaNDM-1 | blaCTX-M | IncFII, IncA/C | |
| ST14 (3) | blaNDM-1 | blaSHV | IncFII, IncA/C | |
| ST14 (3) | blaNDM-1 | blaTEM | IncFII, IncA/C | |
| E. coli | ST405 (11) | blaNDM-1 | blaCTX-M | IncFII, IncA/C, IncN, IncL/M |
| ST405 (4) | blaNDM-1 | blaSHV/blaCTX-M | IncFII, IncA/C, IncN, IncL/M | |
| ST405 (7) | blaNDM-1 | blaCTX-M/blaTEM | IncFII, IncA/C, IncN, IncL/M | |
| ST405 (3) | blaNDM-1/blaOXA-48 | blaSHV/blaCTX-M/blaTEM | IncFII, IncL/M | |
| ST405 (3) | blaNDM-1/blaOXA-48 | blaSHV/blaCTX-M | IncFII, IncL/M | |
| ST405 (2) | blaNDM-1/blaOXA-48 | blaCTX-M/blaTEM | IncFII, IncL/M | |
| ST131 (5) | blaNDM-1 | blaSHV/blaCTX-M | IncFII, IncA/C, IncN, IncL/M | |
| ST131 (3) | blaNDM-1 | blaSHV | IncFII, IncA/C, IncN, IncL/M | |
| ST131 (1) | blaNDM-1 | blaCTX-M/blaTEM | IncFII, IncA/C, IncN, IncL/M | |
| ST131 (1) | blaNDM-1/blaOXA-48 | blaSHV/blaCTX-M | IncFII, IncL/M | |
| ST101 (7) | blaNDM-1 | blaSHV/blaCTX-M | IncFII, IncN | |
| ST101 (9) | blaNDM-1 | blaCTX-M | IncFII, IncN | |
| ST101 (2) | blaNDM-1/blaOXA-48 | blaSHV | IncFII, IncN, IncL/M | |
| ST69 (7) | blaNDM-1 | blaTEM | IncFII, IncA/C, IncN, IncL/M | |
| ST69 (3) | blaNDM-1 | blaSHV/blaCTX-M/blaTEM | IncFII, IncA/C, IncN, IncL/M | |
| ST69 (1) | blaNDM-1/blaOXA-48 | blaSHV | IncFII, IncA/C, IncN, IncL/M | |
| ST10 (1) | blaNDM-1/blaOXA-48 | blaSHV/blaCTX-M | IncFII, IncN, IncL/M | |
| ST10 (4) | blaNDM-1 | blaSHV | IncFII, IncA/C, IncN, IncL/M | |
| ST10 (7) | blaNDM-1 | blaCTX-M | IncFII, IncA/C, IncN, IncL/M |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gondal, A.J.; Choudhry, N.; Bukhari, H.; Rizvi, Z.; Jahan, S.; Yasmin, N. Estimation, Evaluation and Characterization of Carbapenem Resistance Burden from a Tertiary Care Hospital, Pakistan. Antibiotics 2023, 12, 525. https://doi.org/10.3390/antibiotics12030525
Gondal AJ, Choudhry N, Bukhari H, Rizvi Z, Jahan S, Yasmin N. Estimation, Evaluation and Characterization of Carbapenem Resistance Burden from a Tertiary Care Hospital, Pakistan. Antibiotics. 2023; 12(3):525. https://doi.org/10.3390/antibiotics12030525
Chicago/Turabian StyleGondal, Aamir Jamal, Nakhshab Choudhry, Hina Bukhari, Zainab Rizvi, Shah Jahan, and Nighat Yasmin. 2023. "Estimation, Evaluation and Characterization of Carbapenem Resistance Burden from a Tertiary Care Hospital, Pakistan" Antibiotics 12, no. 3: 525. https://doi.org/10.3390/antibiotics12030525