
Current Trends in Antimicrobial Resistance Patterns in Bacterial Pathogens among Adult and Pediatric Patients in the Intensive Care Unit in a Tertiary Care Hospital in Kolkata, India

 , ,
, ,
Abstract
:1. Introduction
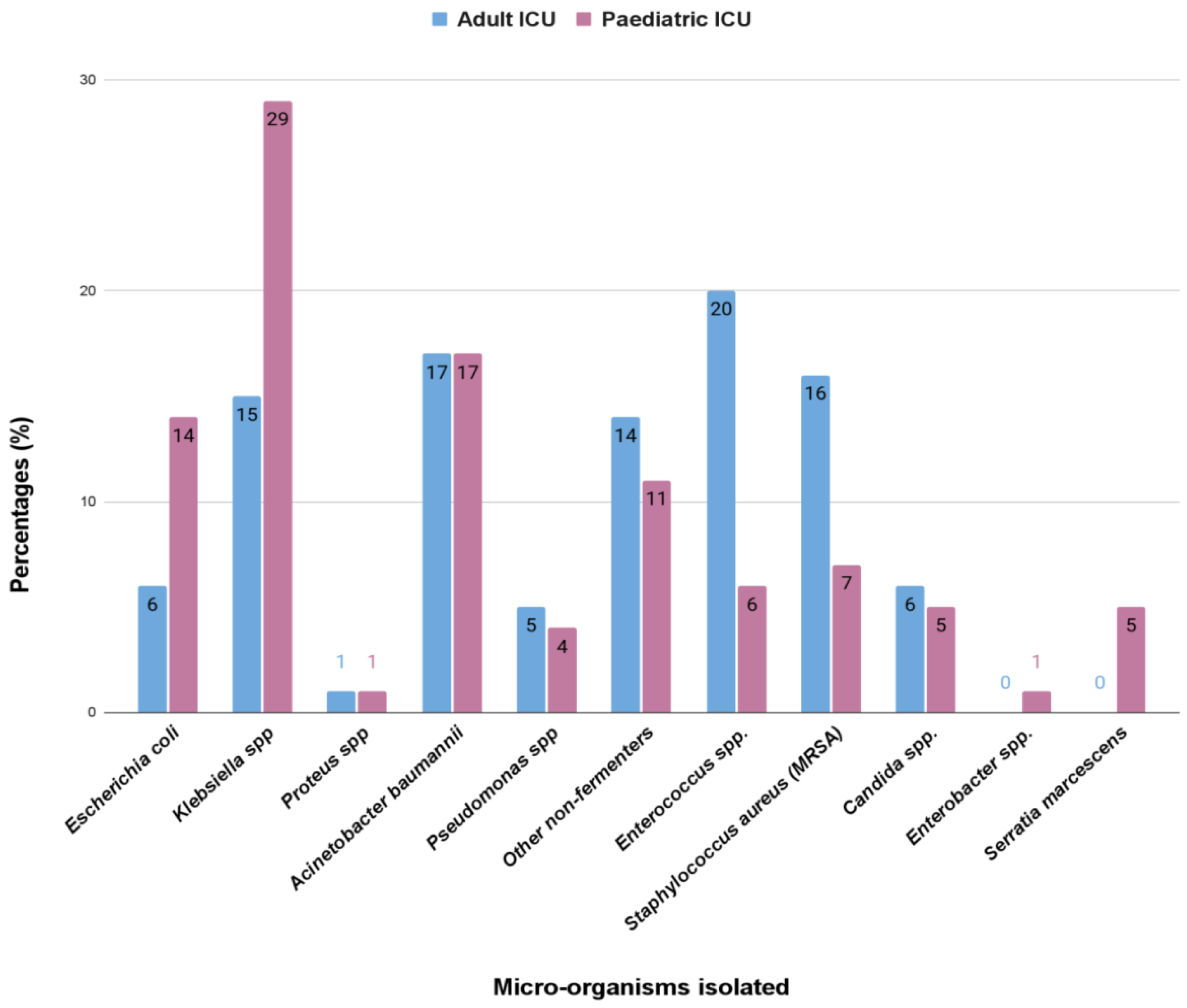
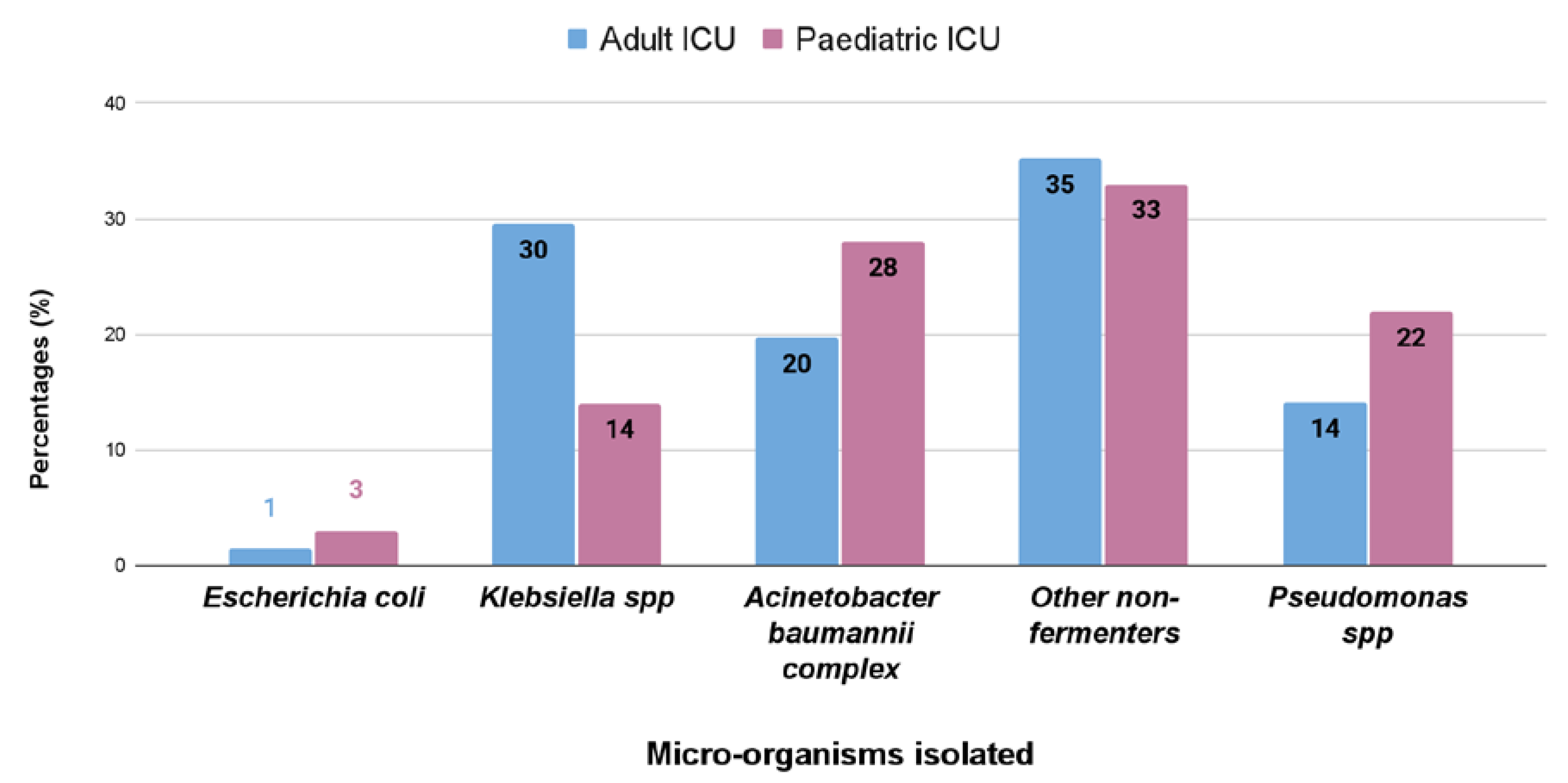
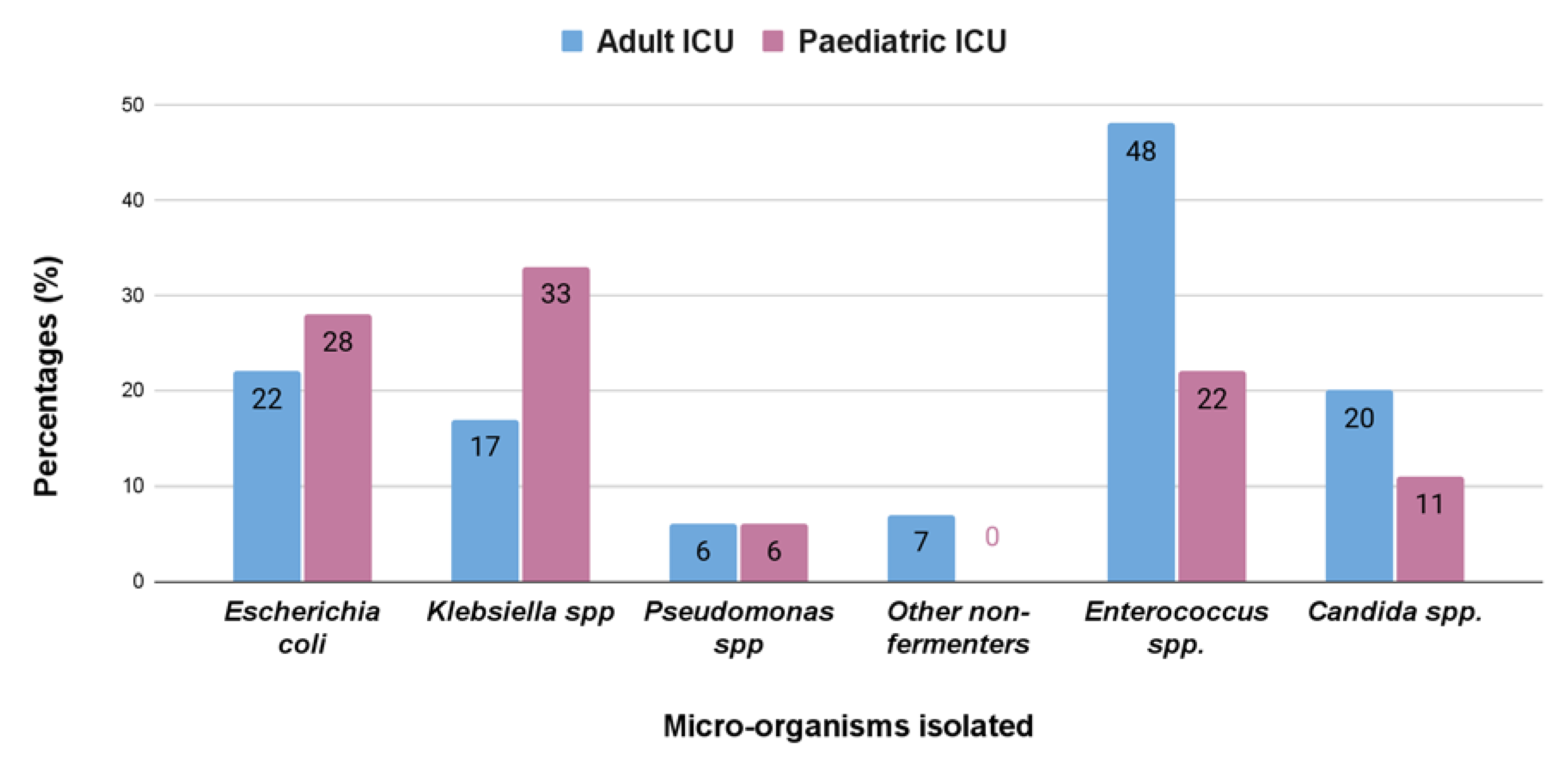
2. Results
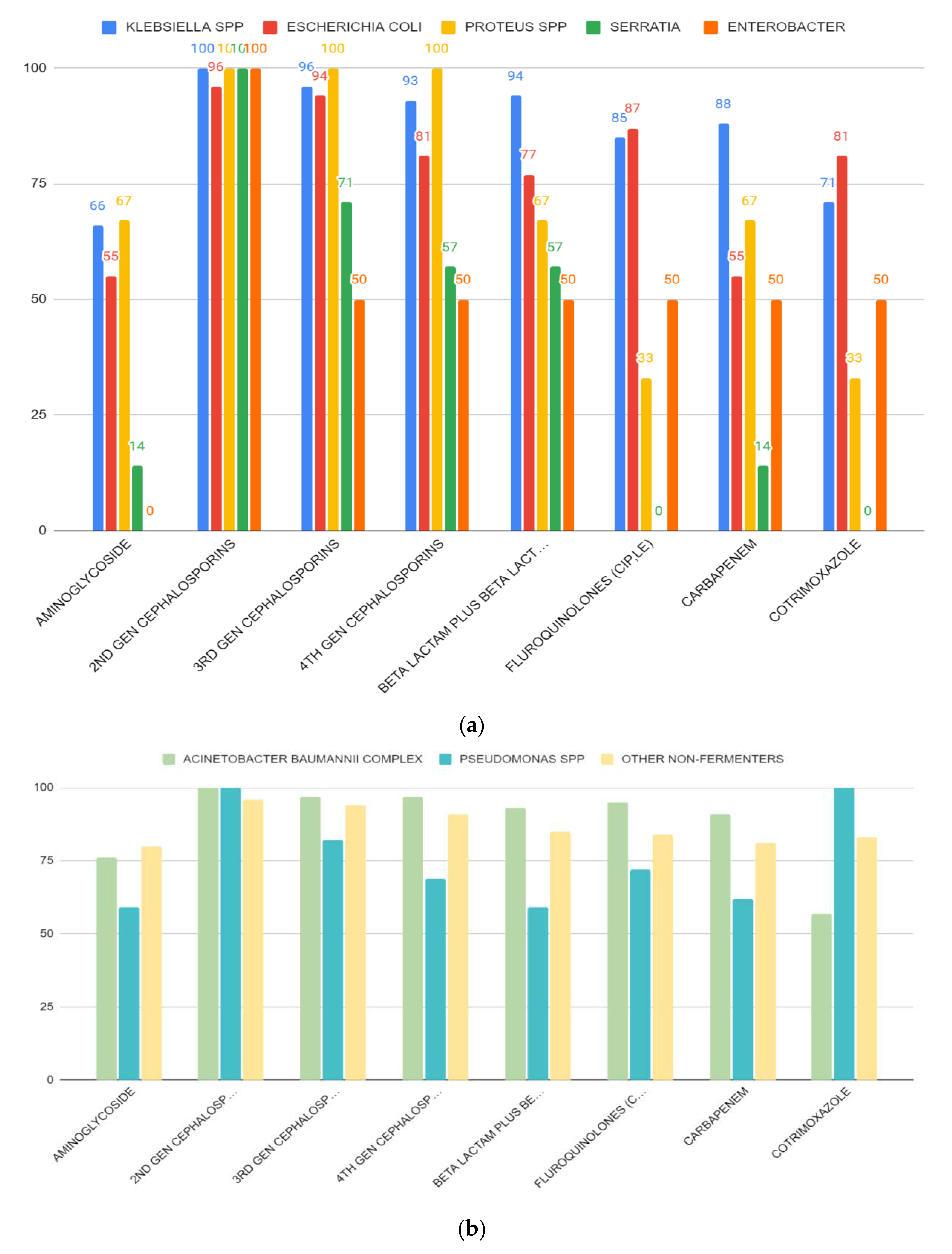
Antibiotic Resistance Patterns
3. Discussion
4. Materials and Methods
4.1. Sample Collection
4.2. Bacterial Culture
4.3. Antibiotic Susceptibility Test (AST)
4.4. Data Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lambert, M.-L.; Suetens, C.; Savey, A.; Palomar, M.; Hiesmayr, M.; Morales, I.; Agodi, A.; Frank, U.; Mertens, K.; Schumacher, M.; et al. Clinical outcomes of health-care-associated infections and antimicrobial resistance in patients admitted to European intensive-care units: A cohort study. Lancet Infect. Dis. 2011, 11, 30–38. [Google Scholar] [CrossRef] [PubMed]
- Bereket, W.; Hemalatha, K.; Getenet, B.; Wondwossen, T.; Solomon, A.; Zeynudin, A.; Kannan, S. Update on bacterial nosocomial infections. Eur. Rev. Med. Pharmacol. Sci. 2012, 16, 1039–1044. [Google Scholar] [PubMed]
- World Health Organization. Prevention of Hospital-Acquired Infection: A Practical Guide (2nd Edition). 2002. Available online: https://apps.who.int/iris/handle/10665/67350 (accessed on 29 April 2018).
- Blot, S.; Depuydt, P.; Vandewoude, K.; De Bacquer, D. Measuring the impact of multidrug resistance in nosocomial infection. Curr. Opin. Infect. Dis. 2007, 20, 391–396. [Google Scholar] [CrossRef] [PubMed]
- Carlet, J.; Ben Ali, A.; Tabah, A.; Willems, V.; Philippart, F.; Chafine, A.; Garrouste-Orgeas, M.; Misset, B. Multidrug resistant infections in the ICU: Mechanisms, prevention and treatment. In 25 Years of Progress and Innovation in Intensive Care Medicine; Kuhlen, R., Moreno, R., Ranieri, V.M., Rhodes, A., Eds.; Medizinisch Wissenschaftliche Verlagsgesellschaft: Berlin, Germany, 2007; Volume 25, pp. 199–211. [Google Scholar]
- Pittet, D.; Tarara, D.; Wenzel, R.P. Nosocomial bloodstream infection in critically ill patients. Excess length of stay, extra costs, and attributable mortality. JAMA 1994, 271, 1598–1601. [Google Scholar] [CrossRef]
- Anand, N.; Nayak, I.M.; Advaitha, M.V.; Thaikattil, N.J.; Kantanavar, K.A.; Anand, S. Antimicrobial agents’ utilization and cost pattern in an intensive care unit of ateaching hospital in South India. Indian J. Crit. Care Med. 2016, 20, 274–279. [Google Scholar] [CrossRef]
- Campion, M.; Scully, G. Antibiotic Use in the Intensive Care Unit: Optimization and De-Escalation. J. Intensive Care Med. 2018, 33, 647–655. [Google Scholar] [CrossRef]
- Torres, A.; Aznar, R.; Gatell, J.M.; Jiménez, P.; González, J.; Ferrer, A.; Celis, R.; Rodriguez-Roisin, R. Incidence, Risk, and Prognosis Factors of Nosocomial Pneumonia in Mechanically Ventilated Patients. Am. Rev. Respir. Dis. 1990, 142, 523–528. [Google Scholar] [CrossRef]
- Young, L.S. Nosocomial infections in the immunocompromised adult. Am. J. Med. 1981, 70, 398–404. [Google Scholar] [CrossRef]
- Hanson, L.C.; Weber, D.J.; Rutala, W.A.; Samsa, G.P. Risk factors for nosocomial pneumonia in the elderly. Am. J. Med. 1992, 92, 161–166. [Google Scholar] [CrossRef]
- Hazra, A.; Dasgupta, S.; Das, S.; Chawan, N.S. Nosocomial infections in the intensive care unit: Incidence, risk factors, outcome and associated pathogens in a public tertiary teaching hospital of Eastern India. Indian J. Crit. Care Med. 2015, 19, 14–20. [Google Scholar] [CrossRef]
- Santajit, S.; Indrawattana, N. Mechanisms of Antimicrobial Resistance in ESKAPE Pathogens. BioMed Res. Int. 2016, 2016, 2475067. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mulani, M.S.; Kamble, E.E.; Kumkar, S.N.; Tawre, M.S.; Pardesi, K.R. Emerging Strategies to Combat ESKAPE Pathogens in the Era of Antimicrobial Resistance: A Review. Front. Microbiol. 2019, 10, 539. [Google Scholar] [CrossRef] [PubMed]
- De Oliveira, D.M.; Forde, B.M.; Kidd, T.J.; Harris, P.N.; Schembri, M.A.; Beatson, S.A.; Paterson, D.L.; Walker, M.J. Antimicrobial Resistance in ESKAPE Pathogens. Clin. Microbiol. Rev. 2020, 33, e00181-19. [Google Scholar] [CrossRef]
- Rice, L.B. Federal Funding for the Study of Antimicrobial Resistance in Nosocomial Pathogens: No ESKAPE. J. Infect. Dis. 2008, 197, 1079–1081. [Google Scholar] [CrossRef] [PubMed]
- Navidinia, M. The clinical importance of emerging ESKAPE pathogens in nosocomial infections. J. Paramed. Sci. 2016, 7, 43–57. [Google Scholar] [CrossRef]
- European Centre for Disease Prevention and Control. Surveillance of Healthcare-Associated Infections and Prevention Indicators in European Intensive Care Units: HAI-Net ICU Protocol, Version 2.2; European Centre for Disease Prevention and Control: Maastricht, The Netherlands, 2017. [Google Scholar]
- Branstetter, J.W.; Barker, L.; Yarbrough, A.; Ross, S.; Stultz, J.S. Challenges of Antibiotic Stewardship in the Pediatric and Neonatal Intensive Care Units. J. Pediatr. Pharmacol. Ther. 2021, 26, 659–668. [Google Scholar] [CrossRef] [PubMed]
- Kollef, M.H.; Fraser, V.J. Antibiotic resistance in the intensive care unit. Ann. Intern. Med. 2001, 134, 298–314. [Google Scholar] [CrossRef]
- Silveira, F.; Fujitani, S.; Paterson, D.L. Antibiotic-resistant infections in the critically ill adult. Clin. Lab. Med. 2004, 24, 329–341. [Google Scholar] [CrossRef]
- Brusselaers, N.; Vogelaers, D.; Blot, S. The rising problem of antimicrobial resistance in the intensive care unit. Ann. Intensive Care 2011, 1, 47. [Google Scholar] [CrossRef] [Green Version]
- Pons, M.J.; Ruiz, J. Current trends in epidemiology and antimicrobial resistance in intensive care units. J. Emerg. Crit. Care Med. 2019, 3, 5. [Google Scholar] [CrossRef]
- Krivoy, N.; El-Ahal, W.A.; Bar-Lavie, Y.; Haddad, S. Antibiotic prescription and costpatterns in a general intensive care unit. Pharm. Pract. 2007, 5, 67–73. [Google Scholar]
- O’Neill, J. Review on Antimicrobial Resistance: Tackling a Crisis for the Health and Wealth of Nations; UK Government: London, UK, 2014. [Google Scholar]
- Centres for Disease Control and Prevention (CDC). Antibiotic Resistance Threats in the United States; U.S. Department of Health & Human Services: Atlanta, GA, USA, 2019. [Google Scholar]
- World Health Organization. Global Action Plan on Antimicrobial Resistance; WHO: Geneva, Switzerland, 2015. [Google Scholar]
- French, G.L. Clinical impact and relevance of antibiotic resistance. Adv. Drug Deliv. Rev. 2005, 57, 1514–1527. [Google Scholar] [CrossRef]
- Michael, C.A.; Dominey-Howes, D.; Labbate, M. The Antimicrobial Resistance Crisis: Causes, Consequences, and Management. Front. Public Health 2014, 2, 145. [Google Scholar] [CrossRef]
- Savanur, S.S.; Gururaj, H. Study of Antibiotic Sensitivity and Resistance Pattern of Bacterial Isolates in Intensive Care Unit Setup of a Tertiary Care Hospital. Indian J. Crit. Care Med. 2019, 23, 547–555. [Google Scholar] [CrossRef]
- Vincent, J.-L.; Bassetti, M.; François, B.; Karam, G.; Chastre, J.; Torres, A.; Roberts, J.A.; Taccone, F.S.; Rello, J.; Calandra, T.; et al. Advances in antibiotic therapy in the critically ill. Crit. Care 2016, 20, 133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hilnani, G.C.; Zirpe, K.; Hadda, V.; Mehta, Y.; Madan, K.; Kulkarni, A.; Mohan, A.; Dixit, S.; Guleria, R.; Bhattacharya, P. Guidelines for Antibiotic Prescription in Intensive Care Unit. Indian J. Crit. Care Med. 2019, 23 (Suppl. S1), S1–S63. [Google Scholar] [CrossRef]
- Luyt, C.E.; Bréchot, N.; Trouillet, J.L.; Chastre, J. Antibiotic stewardship in the intensive care unit. Critical Care 2014, 18, 480. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qadeer, A.; Akhtar, A.; Ain, Q.U.; Saadat, S.; Mansoor, S.; Assad, S.; Ishtiaq, W.; Ilyas, A.; Khan, A.Y.; Ajam, Y. Antibiogram of Medical Intensive Care Unit at Tertiary Care Hospital Setting of Pakistan. Cureus 2016, 8, e809. [Google Scholar] [CrossRef] [Green Version]
- Richards, M.J.; Edwards, J.R.; Culver, D.H.; Gaynes, R.P.; National Nosocomial Infections Surveillance System. Nosocomial Infections in Combined Medical-Surgical Intensive Care Units in the United States. Infect. Control. Hosp. Epidemiol. 2000, 21, 510–515. [Google Scholar] [CrossRef]
- Vincent, J.L.; Rello, J.; Marshall, J.; Siva, E.; Anzueto, A.; Martin, C.D.; Moreno, R.; Lipman, J.; Sakr, Y.; Reinhart, K. The extended prevalence of infection in the ICU study: EPIC II. JAMA 2009, 302, 1–49. [Google Scholar]
- Chia, P.Y.; Sengupta, S.; Kukreja, A.; Ponnampalavanar, S.S.; Ng, O.T.; Marimuthu, K. The role of hospital environment in transmissions of multidrug-resistant gram-negative organisms. Antimicrob. Resist. Infect. Control 2020, 9, 29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gastmeier, P.; Sohr, D.; Just, H.-M.; Nassauer, A.; Daschner, F.; Ruden, H. How to Survey Nosocomial Infections. Infect. Control. Hosp. Epidemiol. 2000, 21, 366–370. [Google Scholar] [CrossRef] [PubMed]
- Alberti, C.; Brun-Buisson, C.; Burchardi, H.; Martin, C.; Goodman, S.; Artigas, A.; Sicignano, A.; Palazzo, M.; Moreno, R.; Boulmé, R.; et al. Epidemiology of sepsis and infection in ICU patients from an international multicentre cohort study. Intensive Care Med. 2002, 28, 108–121. [Google Scholar] [CrossRef] [PubMed]
- Rebollo, M.H.; Bernal, J.M.; Llorca, J.; Rabasa, J.M.; Revuelta, J.M. Nosocomial infections in patients having cardiovascular operations: A multivariate analysis of risk factors. J. Thorac. Cardiovasc. Surg. 1996, 112, 908–913. [Google Scholar] [CrossRef] [Green Version]
- Papia, G.; McLellan, B.A.; El-Helou, P.; Louie, M.; Rachlis, A.; Szalai, J.-P.; Simor, A.E. Infection in Hospitalized Trauma Patients: Incidence, Risk Factors, and Complications. J. Trauma Acute Care Surg. 1999, 47, 923–927. [Google Scholar] [CrossRef] [PubMed]
- Negm, E.M.; Mowafy, S.M.S.; Mohammed, A.A.; Amer, M.G.; Tawfik, A.E.; Ibrahim, A.E.S.; Hassan, T.H. Antibiograms of intensive care units at an Egyptian tertiary care hospital. Egypt. J. Bronchol. 2021, 15, 15. [Google Scholar] [CrossRef]
- Shao, L.-W.; Ni, L.-M.; Gao, C.-H.; Wei, J.-H.; Zhong, Z.-F.; Meng, S.-Q.; Yang, W.-B.; Liu, J.H. The incidence and risk factors of nosocomial infections in intensive care unit in China: An epidemiological study of 1718 patients. Int. J. Clin. Exp. Med. 2016, 9, 23642–23649. [Google Scholar]
- Tran, G.M.; Ho-Le, T.P.; Ha, D.T.; Tran-Nguyen, C.H.; Nguyen, T.S.M.; Pham, T.T.N.; Nguyen, D.A.; Hoang, H.Q.; Tran, N.V.; Nguyen, T.V. Patterns of antimicrobial resistance in intensive care unit patients: A study in Vietnam. BMC Infect. Dis. 2017, 17, 429. [Google Scholar] [CrossRef]
- Yadav, S.K.; Bhujel, R.; Mishra, S.K.; Sharma, S.; Sherchand, J.B. Emergence of multidrug-resistant non-fermentative gram negative bacterial infection in hospitalized patients in a tertiary care center of Nepal. BMC Res. Notes 2020, 13, 319. [Google Scholar] [CrossRef]
- Uc-Cachón, A.H.; Gracida-Osorno, C.; Luna-Chi, I.G.; Jiménez-Guillermo, J.G.; Molina-Salinas, G.M. High Prevalence of Antimicrobial Resistance among Gram-Negative Isolated Bacilli in Intensive Care Units at a Tertiary-Care Hospital in Yucatán Mexico. Medicina 2019, 55, 588. [Google Scholar] [CrossRef] [Green Version]
- Patricia, M.T. Bailey & Scott’s Diagnostic Microbiology, 15th ed.; Elsevier: Amsterdam, The Netherlands, 2021. [Google Scholar]
- Kouchak, F.; Askarian, M. Nosocomial Infections: The Definition Criteria. Iran. J. Med. Sci. 2012, 37, 72–73. [Google Scholar] [PubMed]
- CLSI. Performance Standards for Antimicrobial Susceptibility Testing, 30th ed.; CLSI Supplement M100; Clinical and Laboratory Standards Institute: Wayne, PA, USA, 2020. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Adult ICUs | Pediatric ICUs | |||
|---|---|---|---|---|
| Microorganisms | Numbers Obtained (Total = 258) | Percentage (%) | Numbers Obtained (Total = 222) | Percentage (%) |
| Enterobacteriaceae | 69 | 27 | 94 | 42 |
| Non-fermenters | 100 | 39 | 96 | 43 |
| Gram-positive cocci | 71 | 28 | 23 | 10 |
| Candida | 18 | 6 | 9 | 4 |
| a | |||||
|---|---|---|---|---|---|
| Blood | Urine | Respiratory Sample | |||
| Adult ICU | 122 | 65 | 71 | ||
| Pediatric ICU | 146 | 18 | 58 | ||
| Total (n) | 268 | 83 | 129 | ||
| Percentage (%) | 56 | 17 | 27 | ||
| b | |||||
| Type of ICU | Total Number of Positive Cultures (n) | Number of Positive Samples in Male | Percentage Positivity in Male (%) | Number of Positive Samples in Female | Percentage Positivity in Female (%) |
| Adult ICU | 258 | 124 | 48 (124/258) | 134 | 52 (134/258) |
| Pediatric ICU | 222 | 121 | 55 (121/222) | 101 | 45 (101/222) |
| Microorganisms | Antibiotic Classes | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Aminoglycosides | 2nd Generation Cephalosporins | 3rd Generation Cephalosporins | 4th Generation Cephalosporins | Beta Lactam-Beta Lactam Inhibitors | Fluoroquinolones | Carbapenems | Cotrimoxazole | |||||||||
| Adult ICU | Pediatric ICU | Adult ICU | Pediatric ICU | Adult ICU | Pediatric ICU | Adult ICU | Pediatric ICU | Adult ICU | Pediatric ICU | Adult ICU | Pediatric ICU | Adult ICU | Pediatric ICU | Adult ICU | Pediatric ICU | |
| Escherichia coli | 75 (15/20) | 41 (11/27) | 95 (19/20) | 96 (26/27) | 95 (19/20) | 93 (25/27) | 95 (19/20) | 70 (19/27) | 95 (19/20) | 63 (17/27) | 95 (19/20) | 81 (22/27) | 75 (15/20) | 41 (11/27) | 85 (17/20) | 78 (21/27) |
| Klebsiella spp. | 75 (36/48) | 59 (33/56) | 100 (48/48) | 100 (56/56) | 96 (46/48) | 96 (54/56) | 92 (44/48) | 95 (53/56) | 94 (45/48) | 95 (53/56) | 92 (44/48) | 79 (44/56) | 88 (42/48) | 88 (49/56) | 83 (40/48) | 61 (34/56) |
| Proteus spp. | 0 (0/1) | 100 (2/2) | 100 (1/1) | 100 (2/2) | 100 (1/1) | 100 (2/2) | 100 (1/1) | 100 (2/2) | 0 (0/1) | 100 (2/2) | 0 (0/1) | 50 (1/2) | 0 (0/1) | 100 (2/2) | 0 (0/1) | 50 (1/2) |
| Serratia spp. | n/a | 14 (1/7) | n/a | 100 (7/7) | n/a | 71 (5/7) | n/a | 57 (4/7) | n/a | 57 (4/7) | n/a | 0 (0/7) | n/a | 14 (1/7) | n/a | 0 (0/7) |
| Enterobacter spp. | n/a | 0 (0/2) | n/a | 100 (2/2) | n/a | 50 (1/2) | n/a | 50 (1/2) | n/a | 50 (1/2) | n/a | 50 (1/2) | n/a | 50 (1/2) | n/a | 50 (1/2) |
| Acinetobacter baumannii complex | 66 (23/35) | 85 (35/41) | 100 (35/35) | 100 (41/41) | 97 (34/35) | 98 (40/41) | 97 (34/35) | 98 (40/41) | 91 (32/35) | 95 (39/41) | 97 (34/35) | 93 (38/41) | 89 (31/35) | 93 (38/41) | 86 (30/35) | 32 (13/41) |
| Pseudomonas spp. | 36 (12/19) | 55 (11/20) | n/a | n/a | 100 (12/19) | 65 (13/20) | 79 (15/19) | 60 (12/20) | 74 (14/19) | 45 (9/20) | 74 (14/19) | 70 (14/20) | 89 (17/19) | 35 (7/20) | n/a | n/a |
| Other non-fermenters | 83 (38/46) | 77 (27/35) | 100 (46/46) | 91 (32/35) | 93 (43/46) | 94 (33/35) | 91 (42/46) | 91 (32/35) | 91 (42/46) | 77 (27/35) | 85 (39/46) | 83 (29/35) | 89 (41/46) | 71 (25/35) | 87 (40/46) | 77 (27/35) |
| Antibiotic Classes | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Microoganisms | Ampicillin | Cotrimoxazole | Vancomycin | Linezolid | Aminoglycosides | High Level Gentamicin | Fluoroquinolones | |||||||
| Adult ICU | Pediatric ICU | Adult ICU | Pediatric ICU | Adult ICU | Pediatric ICU | Adult ICU | Pediatric ICU | Adult ICU | Pediatric ICU | Adult ICU | Pediatric ICU | Adult ICU | Pediatric ICU | |
| Staphylococcus aureus (MRSA) | n/a | n/a | 55 (11/20) | 0 (0/10) | 0 (0/20) | 0 (0/10) | 0 (0/20) | 0 (0/10) | 30 (6/20) | 40 (4/10) | n/a | n/a | 65 (13/20) | 60 (6/10) |
| Enterococcus spp. | 96 (49/51) | 92 (12/13) | 0 (51/51) | 0 (13/13) | 33 (17/51) | 31 (4/13) | 8 (4/51) | 0 (0/13) | n/a | n/a | 43 (22/51) | 31 (4/13) | 98 (90/95) | 77 (10/13) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chakraborty, M.; Sardar, S.; De, R.; Biswas, M.; Mascellino, M.T.; Miele, M.C.; Biswas, S.; Mitra, A.N. Current Trends in Antimicrobial Resistance Patterns in Bacterial Pathogens among Adult and Pediatric Patients in the Intensive Care Unit in a Tertiary Care Hospital in Kolkata, India. Antibiotics 2023, 12, 459. https://doi.org/10.3390/antibiotics12030459
Chakraborty M, Sardar S, De R, Biswas M, Mascellino MT, Miele MC, Biswas S, Mitra AN. Current Trends in Antimicrobial Resistance Patterns in Bacterial Pathogens among Adult and Pediatric Patients in the Intensive Care Unit in a Tertiary Care Hospital in Kolkata, India. Antibiotics. 2023; 12(3):459. https://doi.org/10.3390/antibiotics12030459
Chicago/Turabian StyleChakraborty, Mandira, Sayani Sardar, Rituparna De, Malabika Biswas, Maria Teresa Mascellino, Maria Claudia Miele, Silpak Biswas, and Anita Nandi Mitra. 2023. "Current Trends in Antimicrobial Resistance Patterns in Bacterial Pathogens among Adult and Pediatric Patients in the Intensive Care Unit in a Tertiary Care Hospital in Kolkata, India" Antibiotics 12, no. 3: 459. https://doi.org/10.3390/antibiotics12030459