
Syndromic Testing in Infectious Diseases: From Diagnostic Stewardship to Antimicrobial Stewardship
 ,
,
Abstract
:1. Introduction
2. Case Reports
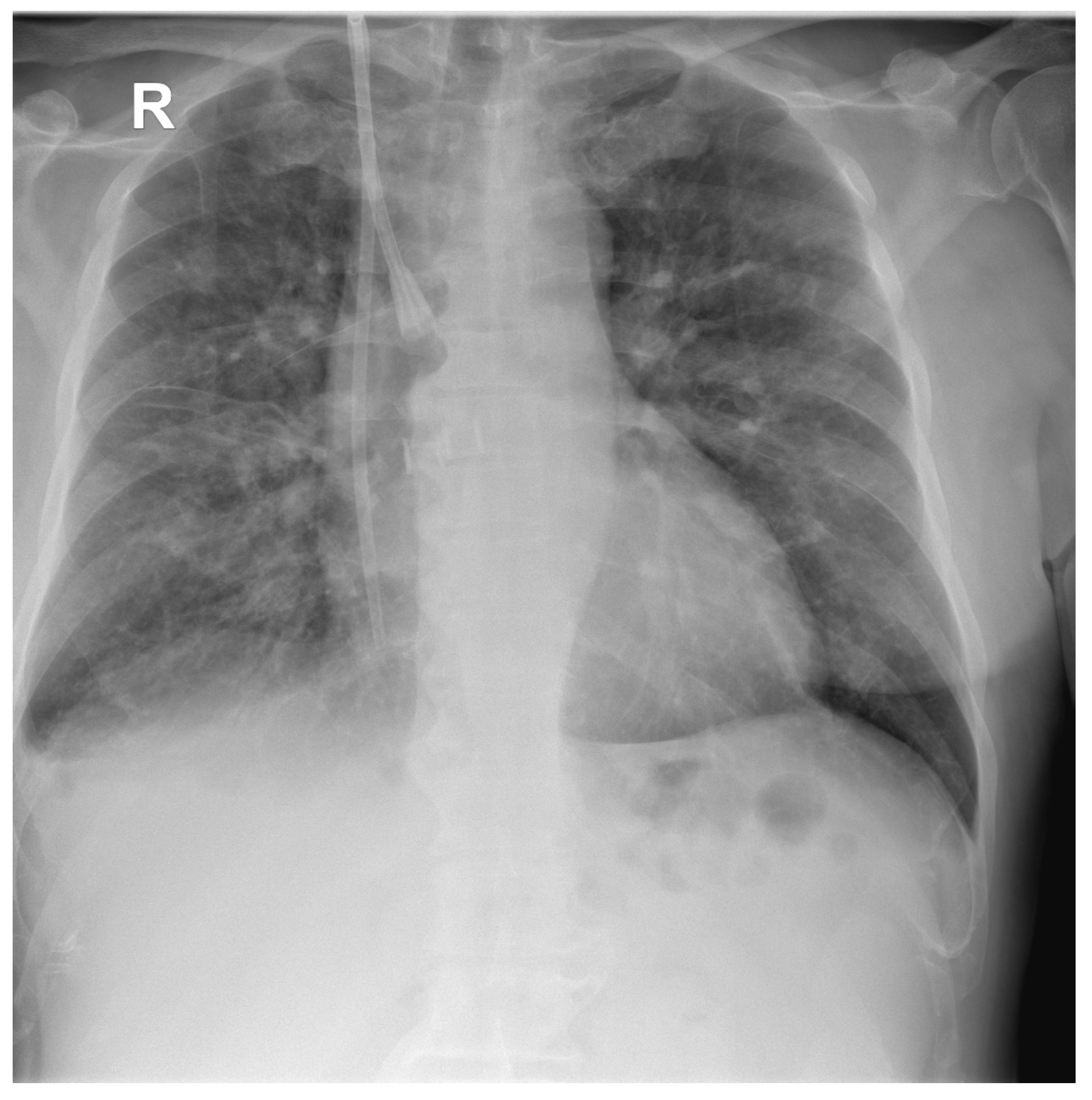
2.1. Case Report 1
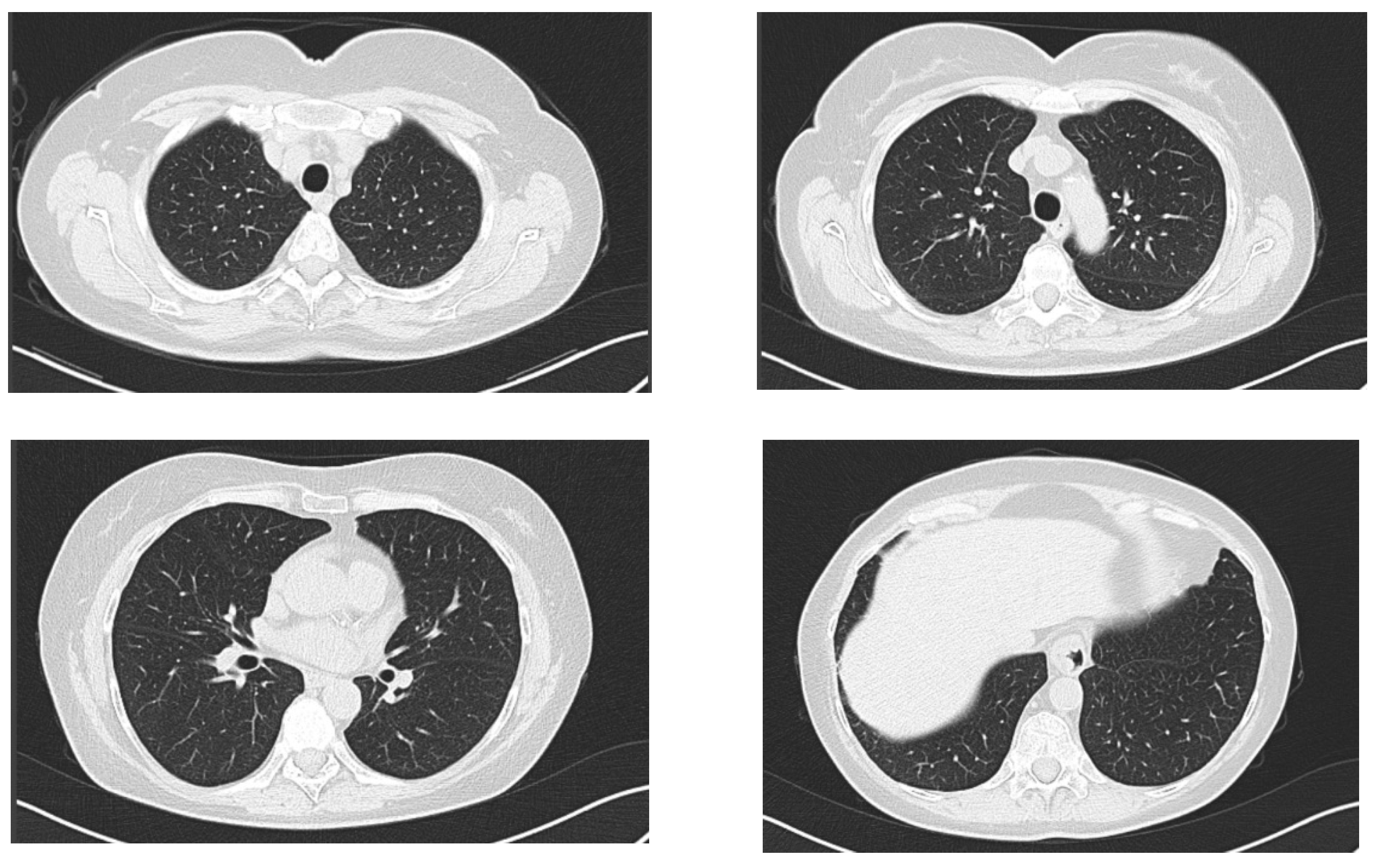
2.2. Case Report 2
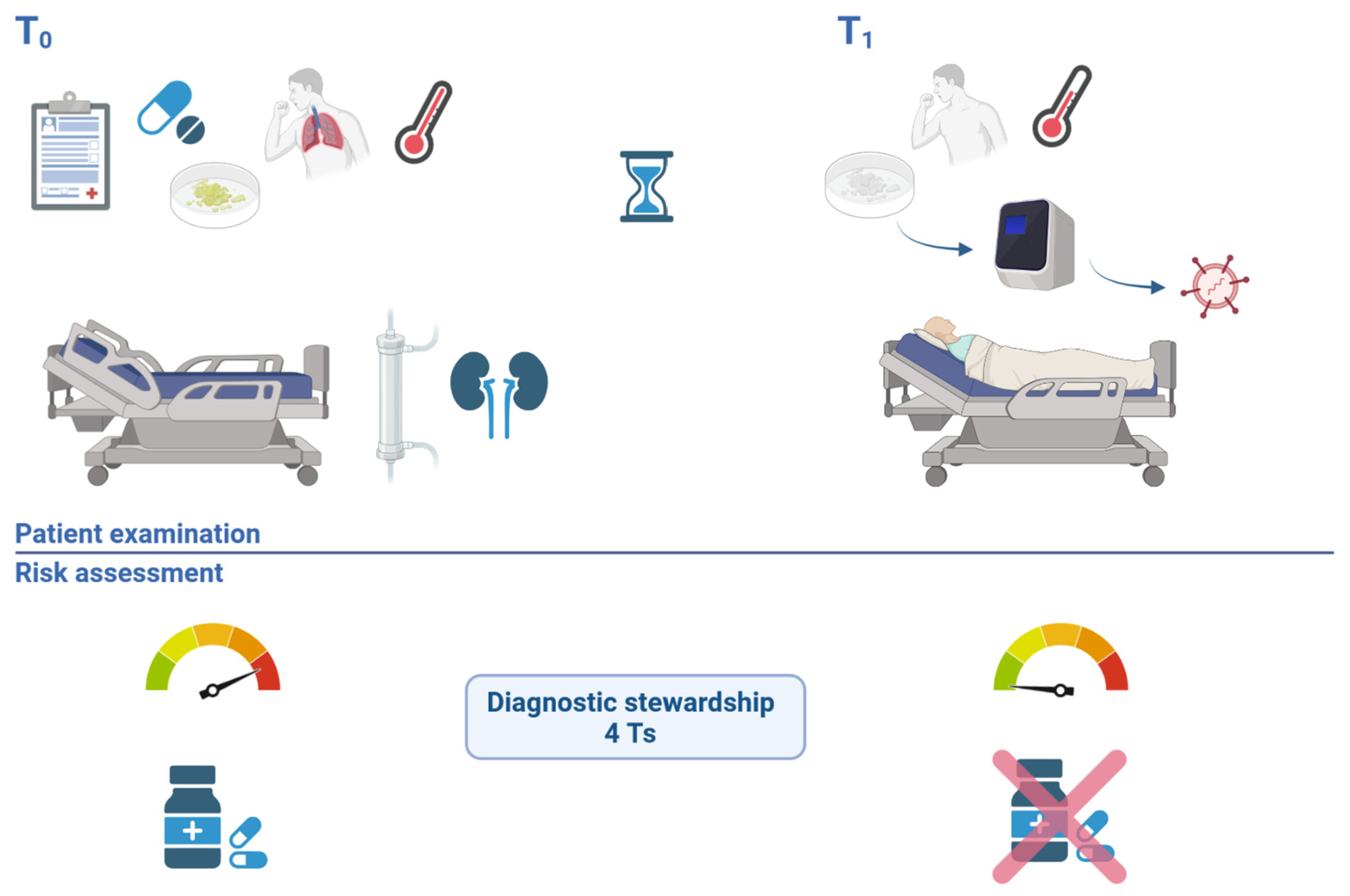
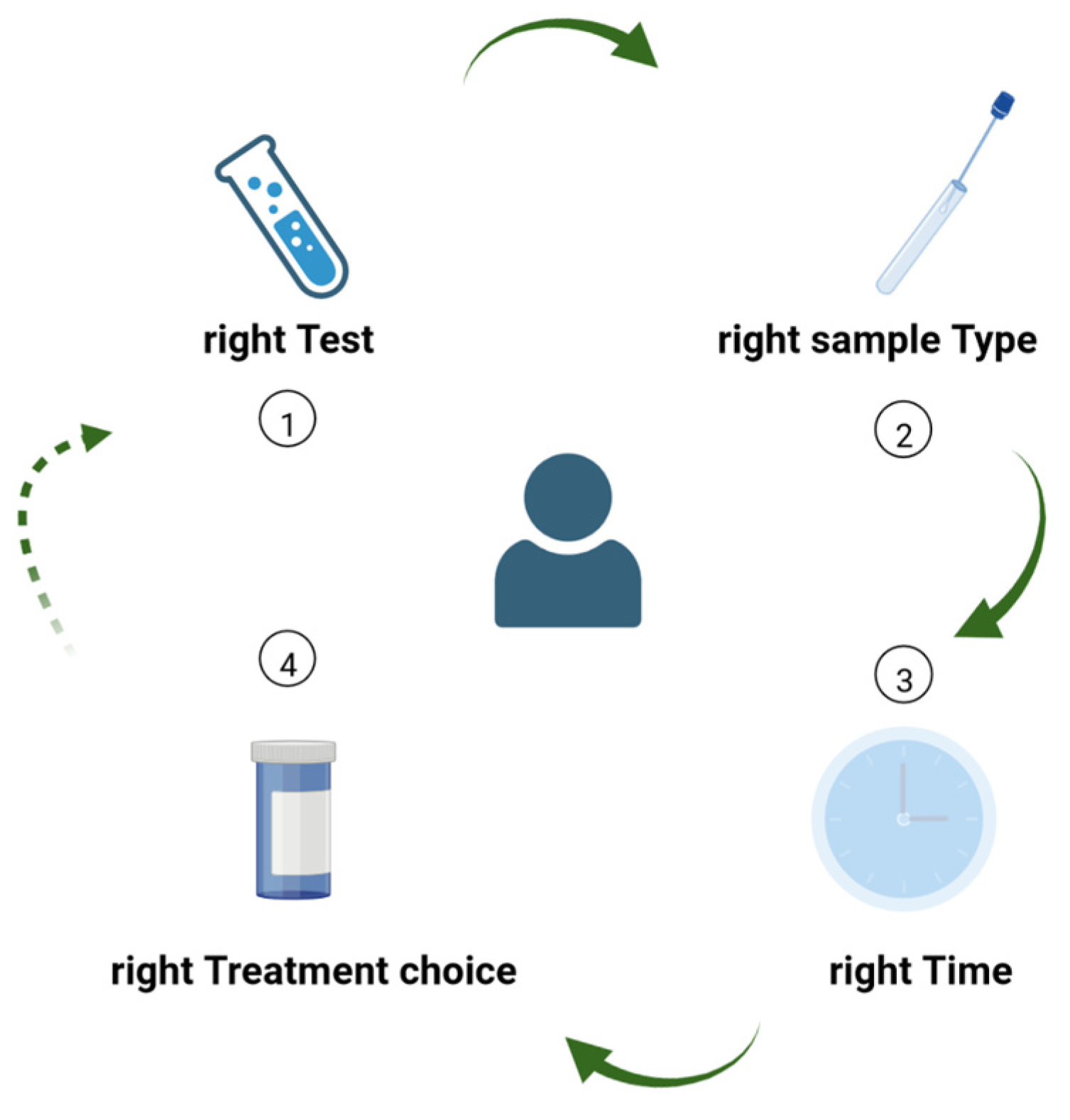
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hanson, K.E.; Couturier, M.R. Multiplexed Molecular Diagnostics for Respiratory, Gastrointestinal, and Central Nervous System Infections. Clin. Infect. Dis. 2016, 63, 1361–1367. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stafylaki, D.; Maraki, S.; Vaporidi, K.; Georgopoulos, D.; Kontoyiannis, D.P.; Kofteridis, D.P.; Chamilos, G. Impact of Molecular Syndromic Diagnosis of Severe Pneumonia in the Management of Critically Ill Patients. Microbiol. Spectr. 2022, 10, e0161622. [Google Scholar] [CrossRef] [PubMed]
- Foschi, C.; Zignoli, A.; Gaibani, P.; Vocale, C.; Rossini, G.; Lafratta, S.; Liberatore, A.; Turello, G.; Lazzarotto, T.; Ambretti, S. Respiratory bacterial co-infections in intensive care unit-hospitalized COVID-19 patients: Conventional culture vs BioFire FilmArray pneumonia Plus panel. J. Microbiol. Methods 2021, 186, 106259. [Google Scholar] [CrossRef]
- Webber, D.M.; Wallace, M.A.; Burnham, C.A.; Anderson, N.W. Evaluation of the BioFire FilmArray Pneumonia Panel for Detection of Viral and Bacterial Pathogens in Lower Respiratory Tract Specimens in the Setting of a Tertiary Care Academic Medical Center. J. Clin. Microbiol. 2020, 58, e00343-20. [Google Scholar] [CrossRef] [PubMed]
- Kamel, N.A.; Alshahrani, M.Y.; Aboshanab, K.M.; El Borhamy, M.I. Evaluation of the BioFire FilmArray Pneumonia Panel Plus to the Conventional Diagnostic Methods in Determining the Microbiological Etiology of Hospital-Acquired Pneumonia. Biology 2022, 11, 377. [Google Scholar] [CrossRef] [PubMed]
- Murphy, C.N.; Fowler, R.; Balada-Llasat, J.M.; Carroll, A.; Stone, H.; Akerele, O.; Buchan, B.; Windham, S.; Hopp, A.; Ronen, S.; et al. Multicenter evaluation of the BioFire FilmArray Pneumonia/Pneumonia Plus panel for detection and quantification of agents of lower respiratory tract infection. J. Clin. Microbiol. 2020, 58, e00128-20. [Google Scholar] [CrossRef] [PubMed]
- Săndulescu, O.; Viziteu, I.; Streinu-Cercel, A.; Miron, V.; Preoțescu, L.; Chirca, N.; Albu, S.; Craiu, M.; Streinu-Cercel, A. Novel Antimicrobials, Drug Delivery Systems and Antivirulence Targets in the Pipeline—From Bench to Bedside. Appl. Sci. 2022, 12, 11615. [Google Scholar] [CrossRef]
- Rolston, K.V. Neoplastic fever: All who shiver are not infected. Support Care Cancer 2005, 13, 863–864. [Google Scholar] [CrossRef] [PubMed]
- Carsons, S.E. Fever in rheumatic and autoimmune disease. Infect. Dis. Clin. N. Am. 1996, 10, 67–84. [Google Scholar] [CrossRef] [PubMed]
- Miron, V.; Craiu, M. "Red throat" or acute pharyngitis–Challenges in real life clinical practice. Germs 2021, 11, 351–353. [Google Scholar] [CrossRef] [PubMed]
- Thakur, L.; Singh, S.; Singh, R.; Kumar, A.; Angrup, A.; Kumar, N. The potential of 4D’s approach in curbing antimicrobial resistance among bacterial pathogens. Expert. Rev. Anti-Infect. Ther. 2022, 20, 1401–1412. [Google Scholar] [CrossRef] [PubMed]
- Joseph, J.; Rodvold, K.A. The role of carbapenems in the treatment of severe nosocomial respiratory tract infections. Expert. Opin. Pharmacother. 2008, 9, 561–575. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Title 1 | Day 1 | Day 3 | Day 5 |
|---|---|---|---|
| White blood cell count (normal range: 3600–9600 cells/µL) | 7600 | 3300 | 4100 |
| Neutrophil count (normal range: 1400–6500 cells /µL) | 5200 | 1800 | 1700 |
| Lymphocyte count (normal range: 1200–3400 cells/µL) | 1800 | 1100 | 1700 |
| Hemoglobin (normal range: 12.1–17.2 g/dL) | 7.5 | 7.9 | 8.1 |
| Platelet count (normal range: 200,000–400,000 cells/µL) | 122,000 | 118,000 | 138,000 |
| Fibrinogen (normal range: 200–393 mg/dL) | 379 | 372 | 386 |
| C-reactive protein (normal range: (0–3 mg/L) | 82.6 | 21.5 | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Săndulescu, O.; Streinu-Cercel, A.; Moțoi, M.M.; Streinu-Cercel, A.; Preoțescu, L.L. Syndromic Testing in Infectious Diseases: From Diagnostic Stewardship to Antimicrobial Stewardship. Antibiotics 2023, 12, 6. https://doi.org/10.3390/antibiotics12010006
Săndulescu O, Streinu-Cercel A, Moțoi MM, Streinu-Cercel A, Preoțescu LL. Syndromic Testing in Infectious Diseases: From Diagnostic Stewardship to Antimicrobial Stewardship. Antibiotics. 2023; 12(1):6. https://doi.org/10.3390/antibiotics12010006
Chicago/Turabian StyleSăndulescu, Oana, Anca Streinu-Cercel, Maria Magdalena Moțoi, Adrian Streinu-Cercel, and Liliana Lucia Preoțescu. 2023. "Syndromic Testing in Infectious Diseases: From Diagnostic Stewardship to Antimicrobial Stewardship" Antibiotics 12, no. 1: 6. https://doi.org/10.3390/antibiotics12010006