
Tailoring Antimicrobial Stewardship (AMS) Interventions to the Cultural Context: An Investigation of AMS Programs Operating in Northern Italian Acute-Care Hospitals
 , , and
, , and
Abstract
:1. Introduction
2. Results
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wojcik, G.; Ring, N.; McCulloch, C.; Willis, D.S.; Williams, B.; Kydonaki, K. Understanding the Complexities of Antibiotic Prescribing Behaviour in Acute Hospitals: A Systematic Review and Meta-Ethnography. Arch. Public Health 2021, 79, 134. [Google Scholar] [CrossRef]
- Wagner, B.; Filice, G.A.; Drekonja, D.; Greer, N.; MacDonald, R.; Rutks, I.; Butler, M.; Wilt, T.J. Antimicrobial Stewardship Programs in Inpatient Hospital Settings: A Systematic Review. Infect. Control Hosp. Epidemiol. 2014, 35, 1209–1228. [Google Scholar] [CrossRef]
- Menichetti, F.; Falcone, M.; Lopalco, P.; Tascini, C.; Pan, A.; Busani, L.; Viaggi, B.; Rossolini, G.M.; Arena, F.; Novelli, A.; et al. The GISA Call to Action for the Appropriate Use of Antimicrobials and the Control of Antimicrobial Resistance in Italy. Int. J. Antimicrob. Agents 2018, 52, 127–134. [Google Scholar] [CrossRef] [PubMed]
- Barlam, T.F.; Cosgrove, S.E.; Abbo, L.M.; MacDougall, C.; Schuetz, A.N.; Septimus, E.J.; Srinivasan, A.; Dellit, T.H.; Falck-Ytter, Y.T.; Fishman, N.O.; et al. Executive Summary: Implementing an Antibiotic Stewardship Program: Guidelines by the Infectious Diseases Society of America and the Society for Healthcare Epidemiology of America. Clin. Infect. 2016, 62, 1197–1202. [Google Scholar] [CrossRef] [PubMed]
- Davey, P.; Scott, C.L.; Brown, E.; Charani, E.; Michie, S.; Ramsay, C.R.; Marwick, C.A. Interventions to Improve Antibiotic Prescribing Practices for Hospital Inpatients (Updated Protocol). Cochrane Database Syst. Rev. 2013, 2, CD003543. [Google Scholar] [CrossRef]
- Charani, E.; Ahmad, R.; Rawson, T.M.; Castro-Sanchèz, E.; Tarrant, C.; Holmes, A.H. The Differences in Antibiotic Decision-Making Between Acute Surgical and Acute Medical Teams: An Ethnographic Study of Culture and Team Dynamics. Clin. Infect. Dis 2019, 69, 12–20. [Google Scholar] [CrossRef]
- Reed, J.E.; Howe, C.; Doyle, C.; Bell, D. Successful Healthcare Improvements From Translating Evidence in Complex Systems (SHIFT-Evidence): Simple Rules to Guide Practice and Research. Int. J. Qual. Health Care 2019, 31, 238–244. [Google Scholar] [CrossRef]
- Thampi, N.; Szymczak, J.E.; Leis, J.A. Applying Behavioral Frameworks to Antimicrobial Stewardship. Infect. Control Hosp. Epidemiol. 2020, 41, 628–630. [Google Scholar] [CrossRef] [PubMed]
- Nampoothiri, V.; Bonaconsa, C.; Surendran, S.; Mbamalu, O.; Nambatya, W.; Ahabwe Babigumira, P.; Ahmad, R.; Castro-Sanchez, E.; Broom, A.; Szymczak, J.; et al. What Does Antimicrobial Stewardship Look like Where You Are? Global Narratives from Participants in a Massive Open Online Course. JAC-Antimicrob. Resist. 2022, 4, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Livorsi, D.; Comer, A.; Matthias, M.S.; Perencevich, E.N.; Bair, M.J. Factors Influencing Antibiotic-Prescribing Decisions Among Inpatient Physicians: A Qualitative Investigation. Infect. Control Hosp. Epidemiol. 2015, 36, 1065–1072. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Charani, E.; Smith, I.; Skodvin, B.; Perozziello, A.; Lucet, J.-C.; Lescure, F.-X.; Birgand, G.; Poda, A.; Ahmad, R.; Singh, S.; et al. Investigating the Cultural and Contextual Determinants of Antimicrobial Stewardship Programmes across Low-, Middle- and High-Income Countries—A Qualitative Study. PLoS ONE 2019, 14, e0209847. [Google Scholar] [CrossRef] [PubMed]
- Shallal, A.; Lahoud, C.; Merhej, D.; Youssef, S.; Verkler, J.; Kaljee, L.; Prentiss, T.; Joshi, S.; Zervos, M.; Matar, M. The Impact of a Post-Prescription Review and Feedback Antimicrobial Stewardship Program in Lebanon. Antibiotics 2022, 11, 642. [Google Scholar] [CrossRef] [PubMed]
- Tamma, P.D.; Avdic, E.; Keenan, J.F.; Zhao, Y.; Anand, G.; Cooper, J.; Dezube, R.; Hsu, S.; Cosgrove, S.E. What Is the More Effective Antibiotic Stewardship Intervention: Preprescription Authorization or Postprescription Review With Feedback? Clin. Infect. Dis. 2017, 64, 537–543. [Google Scholar] [CrossRef] [PubMed]
- Nasr, Z.; Paravattil, B.; Wilby, K.J. The Impact of Antimicrobial Stewardship Strategies on Antibiotic Appropriateness and Prescribing Behaviours in Selected Countries in the Middle East: A Systematic Review. East. Mediterr. Health J. 2017, 23, 430–440. [Google Scholar] [CrossRef] [PubMed]
- Plachouras, D.; Kärki, T.; Hansen, S.; Hopkins, S.; Lyytikäinen, O.; Moro, M.L.; Reilly, J.; Zarb, P.; Zingg, W.; Kinross, P.; et al. Antimicrobial Use in European Acute Care Hospitals: Results from the Second Point Prevalence Survey (PPS) of Healthcare-Associated Infections and Antimicrobial Use, 2016 to 2017. Eurosurveillance 2017, 23, 1800393. [Google Scholar] [CrossRef] [PubMed]
- Vicentini, C.; Quattrocolo, F.; D’Ambrosio, A.; Corcione, S.; Ricchizzi, E.; Moro, M.L.; De Rosa, F.G.; Zotti, C.M. Point Prevalence Data on Antimicrobial Usage in Italian Acute-Care Hospitals: Evaluation and Comparison of Results from Two National Surveys (2011–2016). Infect. Control Hosp. Epidemiol. 2020, 41, 579–584. [Google Scholar] [CrossRef] [PubMed]
- ECDC. ECDC Country Visit to Italy to Discuss Antimicrobial Resistance Issues; Mission Report; European Centre for Desease Prevention and Control: Solna, Sweeden, 2017. [Google Scholar]
- Piano Nazionale Di Contrasto dell’Antimicrobico-Resistenza (PNCAR). 2020. Available online: https://www.salute.gov.it/portale/documentazione/p6_2_2_1.jsp?lingua=italiano&id=2660 (accessed on 15 September 2022).
- Vicentini, C.; Blengini, V.; Libero, G.; Raso, R.; Zotti, C.M. Antimicrobial Stewardship Experiences in Acute-Care Hospitals of Northern Italy: Assessment of Structure, Process and Outcome Indicators, 2017–2019. Am. J. Infect. Control, 2022; in press. [Google Scholar] [CrossRef] [PubMed]
- Viale, P.; Giannella, M.; Bartoletti, M.; Tedeschi, S.; Lewis, R. Considerations About Antimicrobial Stewardship in Settings with Epidemic Extended-Spectrum β-Lactamase-Producing or Carbapenem-Resistant Enterobacteriaceae. Infect. Dis. Ther. 2015, 4, 65–83. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Hospitals Implementing Enabling AMS Strategies (ES), n = 7 | Hospitals Implementing Combined Enabling and Restrictive AMS Strategies (CS), n = 17 | |
|---|---|---|
| Characteristics | ||
| Ownership, N (%) | ||
| Public | 4 (57.14) | 15 (88.24) |
| Private | 3 (42.86) | 2 (11.76) |
| Level of care, N (%) | ||
| Secondary | 3 (42.86) | 6 (35.29) |
| Tertiary | 1 (14.29) | 8 (47.06) |
| Teaching | 0 | 3 (17.65) |
| Specialized | 3 (42.86) | 0 |
| N of beds, median (IQR) | 333 (135–432) | 526 (247.5–624.5) |
| Number of dedicated FTE infection control nurses per 100 beds, median (IQR) | 0.46 (0.3–0.58) | 0.53 (0.41–0.67) |
| Outcomes | ||
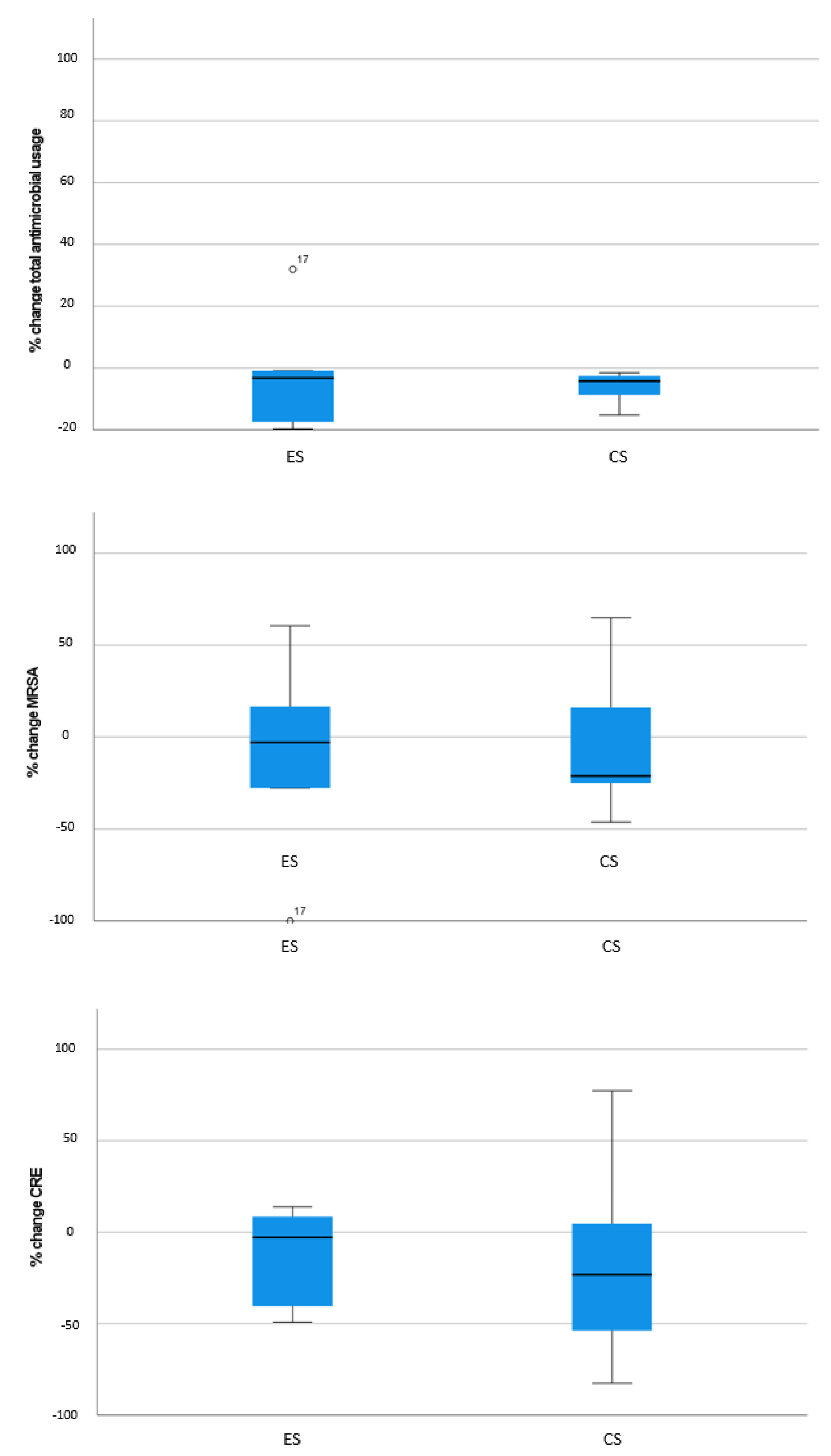
| Total antimicrobial usage, median (IQR) % change in DDD per 1000 pds | −3.23 (−18.54–15.57) | −4.21 (−9.89–−2.44) |
| MRSA, median (IQR) % change | −2.96 (−45.87–27.63) | −21.19 (−25.5–21.02) |
| CRE, median (IQR) % change | −2.77 (−44.8–11.21) | −23.23 (−57.43–10.35) |
| Percentage Change in Antimicrobial Usage | Percentage Change in MRSA | Percentage Change in CRE | ||||
|---|---|---|---|---|---|---|
| Coefficient (95% CI) | p Value | Coefficient (95% CI) | p Value | Coefficient (95% CI) | p Value | |
| Hospital size | ||||||
| >400 beds | Ref | Ref | Ref | |||
| 200–400 beds | −1.84 (−12.22–8.53) | 0.728 | 23.9 (−10.84–58.64) | 0.177 | 22.26 (−15.69–60.21) | 0.250 |
| <200 beds | 9.55 (−2.98–22.08) | 0.135 | −7.7 (−45.44–30.05) | 0.689 | 27.12 (−22.14–76.37) | 0.281 |
| Level of care | ||||||
| Tertiary | Ref | Ref | Ref | |||
| Secondary | 52.31 (0.38–104.24) | 0.048 | 6.82 (−25.09–38.74) | 0.675 | 38.23 (4.7–71.75) | 0.025 |
| Teaching | 9.03 (−61–79.05) | 0.177 | 10.44 (−33.34–54.23) | 0.64 | 2.23 (−45.18–49.64) | 0.259 |
| Specialized | −63.75 (−156.38–28.89) | 0.801 | −33.95 (−85.3–17.39) | 0.195 | 43.13 (−31.83–118.1) | 0.926 |
| Ownership | ||||||
| Private | Ref | Ref | Ref | |||
| Public | 43.99 (−34.07–122.05) | 0.269 | 14.33 (−23.64–52.3) | 0.459 | −20.09 (−69.27–29.1) | 0.423 |
| AMS strategy | ||||||
| Enabling (ES) | Ref | Ref | Ref | |||
| Combined (CS) | −48.96 (−113.46–15.54) | 0.137 | −3.48 (−36.74–29.78) | 0.837 | 3.5 (−37.33–44.33) | 0.867 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vicentini, C.; Blengini, V.; Libero, G.; Martella, M.; Zotti, C.M., on behalf of the Working Group “Unità Prevenzione Rischio Infettivo (UPRI), Regione Piemonte”. Tailoring Antimicrobial Stewardship (AMS) Interventions to the Cultural Context: An Investigation of AMS Programs Operating in Northern Italian Acute-Care Hospitals. Antibiotics 2022, 11, 1257. https://doi.org/10.3390/antibiotics11091257
Vicentini C, Blengini V, Libero G, Martella M, Zotti CM on behalf of the Working Group “Unità Prevenzione Rischio Infettivo (UPRI), Regione Piemonte”. Tailoring Antimicrobial Stewardship (AMS) Interventions to the Cultural Context: An Investigation of AMS Programs Operating in Northern Italian Acute-Care Hospitals. Antibiotics. 2022; 11(9):1257. https://doi.org/10.3390/antibiotics11091257
Chicago/Turabian StyleVicentini, Costanza, Valentina Blengini, Giulia Libero, Manuela Martella, and Carla Maria Zotti on behalf of the Working Group “Unità Prevenzione Rischio Infettivo (UPRI), Regione Piemonte”. 2022. "Tailoring Antimicrobial Stewardship (AMS) Interventions to the Cultural Context: An Investigation of AMS Programs Operating in Northern Italian Acute-Care Hospitals" Antibiotics 11, no. 9: 1257. https://doi.org/10.3390/antibiotics11091257