
Microbiological Trends and Antibiotic Susceptibility Patterns in Patients with Periprosthetic Joint Infection of the Hip or Knee over 6 Years
 , , , and
, , , and
Abstract
:1. Introduction
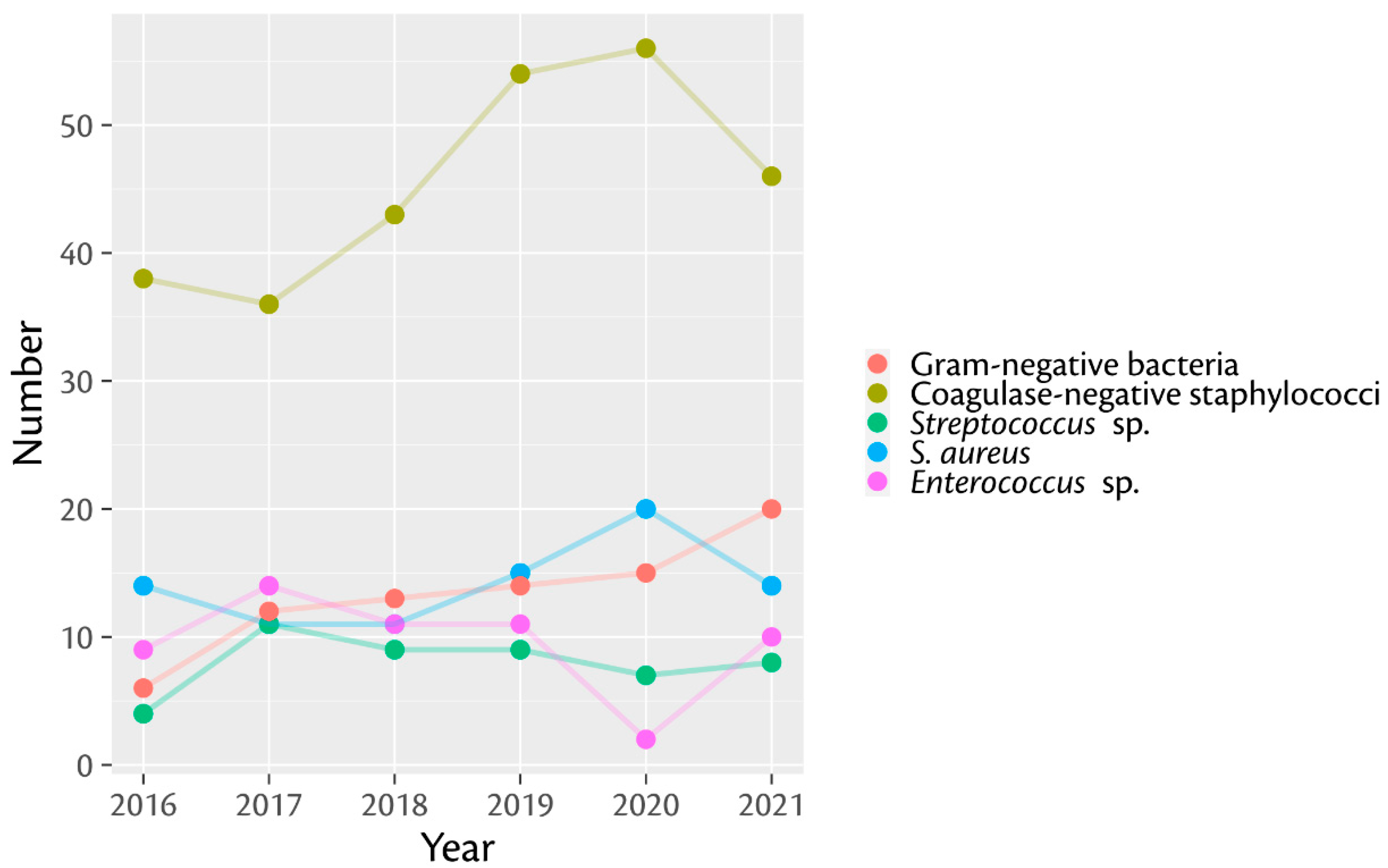
2. Results
3. Discussion
4. Materials and Methods
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kamath, A.F.; Ong, K.L.; Lau, E.; Chan, V.; Vail, T.P.; Rubash, H.E.; Berry, D.J.; Bozic, K.J. Quantifying the Burden of Revision Total Joint Arthroplasty for Periprosthetic Infection. J. Arthroplast. 2015, 30, 1492–1497. [Google Scholar] [CrossRef] [PubMed]
- Wimmer, M.D.; Hischebeth, G.T.R.; Randau, T.M.; Gathen, M.; Schildberg, F.A.; Fröschen, F.S.; Kohlhof, H.; Gravius, S. Difficult-to-Treat Pathogens Significantly Reduce Infection Resolution in Periprosthetic Joint Infections. Diagn. Microbiol. Infect. Dis. 2020, 98, 115114. [Google Scholar] [CrossRef] [PubMed]
- Fröschen, F.S.; Randau, T.M.; Franz, A.; Molitor, E.; Hischebeth, G.T.R. Microbiological Profiles of Patients with Periprosthetic Joint Infection of the Hip or Knee. Diagnostics 2022, 12, 1654. [Google Scholar] [CrossRef] [PubMed]
- Fröschen, F.S.; Randau, T.M.; Hischebeth, G.T.R.; Gravius, N.; Gravius, S.; Walter, S.G. Mid-Term Results after Revision Total Hip Arthroplasty with Custom-Made Acetabular Implants in Patients with Paprosky III Acetabular Bone Loss. Arch. Orthop. Trauma Surg. 2019, 140, 263–273. [Google Scholar] [CrossRef]
- Renz, N.; Perka, C.; Trampuz, A. Management of periprosthetic infections of the knee. Orthopade 2016, 45, 65–71. [Google Scholar] [CrossRef]
- Zimmerli, W.; Trampuz, A.; Ochsner, P.E. Prosthetic-Joint Infections. N. Engl. J. Med. 2004, 351, 1645–1654. [Google Scholar] [CrossRef]
- Fröschen, F.S.; Walter, S.G.; Randau, T.M.; Gravius, N.; Gravius, S.; Hischebeth, G.T.R. The Use of Negative Pressure Wound Therapy Increases Failure Rate in Debridement and Implant Retention for Acute Prosthetic Joint Infection. Technol. Health Care 2020, 28, 721–731. [Google Scholar] [CrossRef]
- Garvin, K.L.; Miller, R.E.; Gilbert, T.M.; White, A.M.; Lyden, E.R. Late Reinfection May Recur More Than 5 Years after Reimplantation of THA and TKA: Analysis of Pathogen Factors. Clin. Orthop. 2018, 476, 345–352. [Google Scholar] [CrossRef]
- Moore, A.J.; Blom, A.W.; Whitehouse, M.R.; Gooberman-Hill, R. Deep Prosthetic Joint Infection: A Qualitative Study of the Impact on Patients and Their Experiences of Revision Surgery. BMJ Open 2015, 5, e009495. [Google Scholar] [CrossRef]
- Stevoska, S.; Himmelbauer, F.; Stiftinger, J.; Stadler, C.; Gotterbarm, T.; Heyse, T.J.; Klasan, A. Significant Difference in Antimicrobial Resistance of Coagulase Negative Periprosthetic Joint Infection in Septic Revision Total Knee Arthroplasty between Two Major Orthopedic Centers. J. Arthroplast. 2022, 37, S306–S312. [Google Scholar] [CrossRef]
- Sebastian, S.; Sezgin, E.A.; Stučinskas, J.; Tarasevičius, Š.; Liu, Y.; Raina, D.B.; Tägil, M.; Lidgren, L.; W-Dahl, A. Different Microbial and Resistance Patterns in Primary Total Knee Arthroplasty Infections—A Report on 283 Patients from Lithuania and Sweden. BMC Musculoskelet. Disord. 2021, 22, 800. [Google Scholar] [CrossRef] [PubMed]
- Tsai, Y.; Chang, C.-H.; Lin, Y.-C.; Lee, S.-H.; Hsieh, P.-H.; Chang, Y. Different Microbiological Profiles between Hip and Knee Prosthetic Joint Infections. J. Orthop. Surg. 2019, 27. [Google Scholar] [CrossRef] [PubMed]
- Peng, H.-M.; Zhou, Z.-K.; Wang, F.; Yan, S.-G.; Xu, P.; Shang, X.-F.; Zheng, J.; Zhu, Q.-S.; Cao, L.; Weng, X.-S. Microbiology of Periprosthetic Hip and Knee Infections in Surgically Revised Cases from 34 Centers in Mainland China. Infect. Drug Resist. 2021, 14, 2411–2418. [Google Scholar] [CrossRef] [PubMed]
- Bjerke-Kroll, B.T.; Christ, A.B.; McLawhorn, A.S.; Sculco, P.K.; Jules-Elysée, K.M.; Sculco, T.P. Periprosthetic Joint Infections Treated with Two-Stage Revision over 14 Years: An Evolving Microbiology Profile. J. Arthroplast. 2014, 29, 877–882. [Google Scholar] [CrossRef] [PubMed]
- Hu, L.; Fu, J.; Zhou, Y.; Chai, W.; Zhang, G.; Hao, L.; Chen, J. Trends in Microbiological Profiles and Antibiotic Resistance in Periprosthetic Joint Infections. J. Int. Med. Res. 2021, 49. [Google Scholar] [CrossRef]
- Kurtz, S.M. Future Clinical and Economic Impact of Revision Total Hip and Knee Arthroplasty. J. Bone Jt. Surg. Am. 2007, 89, 144. [Google Scholar] [CrossRef]
- Stevoska, S.; Himmelbauer, F.; Stiftinger, J.; Stadler, C.; Pisecky, L.; Gotterbarm, T.; Klasan, A. Significant Difference in Antimicrobial Resistance of Bacteria in Septic Revision between Total Knee Arthroplasty and Total Hip Arthroplasty. Antibiotics 2022, 11, 249. [Google Scholar] [CrossRef]
- Stefánsdóttir, A.; Johansson, D.; Knutson, K.; Lidgren, L.; Robertsson, O. Microbiology of the Infected Knee Arthroplasty: Report from the Swedish Knee Arthroplasty Register on 426 Surgically Revised Cases. Scand. J. Infect. Dis. 2009, 41, 831–840. [Google Scholar] [CrossRef]
- Izakovicova, P.; Borens, O.; Trampuz, A. Periprosthetic Joint Infection: Current Concepts and Outlook. EFORT Open Rev. 2019, 4, 482–494. [Google Scholar] [CrossRef]
- Charalambous, L.T.; Kim, B.I.; Schwartz, A.M.; Case, A.; Seidelman, J.L.; Hendershot, E.F.; Bolognesi, M.P.; Seyler, T.M.; Jiranek, W.A. Prosthetic Knee Infection with Coagulase-Negative Staphylococcus: A Harbinger of Poor Outcomes. J. Arthroplast. 2022, 37, S313–S320. [Google Scholar] [CrossRef]
- Zmistowski, B.; Fedorka, C.J.; Sheehan, E.; Deirmengian, G.; Austin, M.S.; Parvizi, J. Prosthetic Joint Infection Caused by Gram-Negative Organisms. J. Arthroplast. 2011, 26, 104–108. [Google Scholar] [CrossRef] [PubMed]
- Benito, N.; Franco, M.; Ribera, A.; Soriano, A.; Rodriguez-Pardo, D.; Sorlí, L.; Fresco, G.; Fernández-Sampedro, M.; Dolores del Toro, M.; Guío, L.; et al. Time Trends in the Aetiology of Prosthetic Joint Infections: A Multicentre Cohort Study. Clin. Microbiol. Infect. 2016, 22, 732.e1–732.e8. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Pardo, D.; Pigrau, C.; Lora-Tamayo, J.; Soriano, A.; del Toro, M.D.; Cobo, J.; Palomino, J.; Euba, G.; Riera, M.; Sánchez-Somolinos, M.; et al. Gram-Negative Prosthetic Joint Infection: Outcome of a Debridement, Antibiotics and Implant Retention Approach. A Large Multicentre Study. Clin. Microbiol. Infect. 2014, 20, O911–O919. [Google Scholar] [CrossRef] [PubMed]
- Parvizi, J.; Tan, T.L.; Goswami, K.; Higuera, C.; Della Valle, C.; Chen, A.F.; Shohat, N. The 2018 Definition of Periprosthetic Hip and Knee Infection: An Evidence-Based and Validated Criteria. J. Arthroplast. 2018, 33, 1309–1314.e2. [Google Scholar] [CrossRef]


{kind=link}
| Demographic Characteristics | 2016–2021 | 2016–2018 | 2019–2021 |
|---|---|---|---|
| Number of patients [n] | 493 | 220 | 273 |
| male | 243 (49.2%) | 107 (48.6%) | 135 (49.5%) |
| female | 250 (50.8%) | 113 (51.4%) | 138 (50.5%) |
| PJI of the hip | 293 (59.4%) | 120 (54.5%) | 173 (63.4%) |
| right | 125 (25.3%) | 54 (24.5%) | 71 (26.0%) |
| left | 168 (34.1%) | 66 (30.0%) | 102 (37.4 %) |
| PJI of the knee | 200 (40.4%) | 100 (45.5%) | 100 (36.6%) |
| right | 100 (20.2%) | 49 (22.3%) | 50 (18.3%) |
| left | 100 (20.2%) | 51 (23.2%) | 50 (18.3%) |
| Age (Mean ± SD) [years] | 69 ± 11 | 70 ± 11 | 69 ± 12 |
| BMI (Mean ± SD) [kg/m2] | 29.99 ± 8.85 | 30.06 ± 8.39 | 29.91 ± 8.73 |
| Preoperative Creatinine [mg/dL] | 1.02 ± 0.76 | 1.08 ± 0.99 | 0.98 ± 0.485 |
| Preoperative C-reactive Protein [mg/L] | |||
| -acute early onset [n = 90] | 84.16 ± 68.95 | 79.81 ± 57.55 [n = 42] | 89.44 ± 77.86 [n = 48] |
| -persisting early onset [n = 4] | 85.78 ± 43.54 | / | 85.78 ± 43.54 [n = 4] |
| -acute late onset [n = 90] | 131.65 ± 109.04 | 129.2 ± 102.64 [n = 34] | 51.40 ± 73.39 [n = 56] |
| -chronic late onset [n = 309] | 53.56 ± 79.62 | 55.94 ± 86.50 [n = 144] | 51.41 ± 73.39 [n = 165] |
| Number of previous surgeries | 4.71 ± 4.1 | 4.67 ± 4.23 | 4.75 ± 4.34 |
| Comorbidities | |||
| Hypertension | 437 (88.6%) | 203 (92.1%) | 234 (85.7%) |
| Smoking | 147 (29.8%) | 66 (30%) | 81 (29.6%) |
| Diabetes mellitus | 175 (35.5%) | 80 (36.3%) | 94 (34.4%) |
| Alcoholism | 51 (10.3%) | 25 (11.3%) | 26 (9.5%) |
| Cirrhosis | 41 (8.3%) | 18 (8.1%) | 23 (8.4%) |
| Malignancy | 72 (14.6%) | 36 (16.3%) | 36 (13.1%) |
| Rheumatoid arthritis | 54 (10.9%) | 20 (9.1%) | 34 (12.4%) |
| Immunosuppression | 100 (20.3%) | 50 (22.7%) | 50 (18.3%) |
| chron. kidney disease | 142 (28.8%) | 63 (28.6%) | 79 (28.9%) |
| 2016 | 2017 | 2018 | 2019 | 2020 | 2021 | Detection in PJI of the Hip | Detection in PJI of the Knee | Total by Species | |
|---|---|---|---|---|---|---|---|---|---|
| Aerobic Gram-positive | 66 | 74 | 76 | 90 | 88 | 81 | 276 | 199 | 475 (77.61%) |
| Coagulase-negative staphylococci | 38 | 36 | 43 | 54 | 56 | 48 | 174 | 101 | 275 (44.93%) |
| S. aureus | 15 | 11 | 11 | 15 | 20 | 14 | 44 | 42 | 86 (14.05%) |
| E. faecalis | 7 | 9 | 11 | 7 | 2 | 10 | 29 | 17 | 46 (7.52%) |
| E. faecium | 2 | 5 | 0 | 4 | 0 | 0 | 6 | 5 | 11 (1.8%) |
| Streptococcus species | 4 | 11 | 9 | 9 | 7 | 8 | 17 | 31 | 48 (7.84%) |
| Micrococcus | 0 | 1 | 1 | 0 | 1 | 1 | 3 | 1 | 4 (0.65%) |
| Granulicatella adiacens | 0 | 0 | 0 | 1 | 0 | 0 | 1 | 0 | 1 (0.16%) |
| Kocuria rhizophila | 0 | 0 | 0 | 0 | 1 | 0 | 1 | 0 | 1 (0.16%) |
| Corynebacterium species | 0 | 1 | 1 | 0 | 1 | 0 | 1 | 2 | 3 (0.49%) |
| Rod-shaped or anaerobic Gram-positive | 2 | 9 | 1 | 8 | 10 | 7 | 23 | 14 | 37 (0.61%) |
| C. acnes | 2 | 4 | 1 | 5 | 9 | 6 | 15 | 12 | 27 (4.41%) |
| C. avidum | 0 | 4 | 0 | 1 | 0 | 1 | 6 | 0 | 6 (0.98%) |
| C. tertium | 0 | 0 | 0 | 1 | 0 | 0 | 1 | 0 | 1 (0.16%) |
| Erysipelothrix rhusiopathiae | 0 | 1 | 0 | 0 | 0 | 0 | 1 | 0 | 1 (0.16%) |
| Pseudoarthrobacter sulfonivorans | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 1 | 1 (0.16%) |
| Peptoniphilus coxii | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 1 | 1 (0.16%) |
| Gram-negative | 6 | 12 | 13 | 14 | 15 | 20 | 52 | 28 | 80 (13.07%) |
| E. coli | 2 | 7 | 2 | 2 | 2 | 6 | 10 | 11 | 21 (3.43%) |
| P. mirabilis | 1 | 1 | 5 | 5 | 1 | 2 | 9 | 6 | 15 (2.45%) |
| P. vulgaris | 1 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 1 (0.16%) |
| E. cloacae complex | 1 | 1 | 0 | 1 | 2 | 3 | 8 | 0 | 8 (1.31%) |
| Serratia marcescens | 0 | 0 | 1 | 2 | 3 | 0 | 5 | 1 | 6 (0.98%) |
| P. aeruginosa | 0 | 1 | 0 | 2 | 1 | 3 | 6 | 1 | 7 (1.14%) |
| K. pneumoniae | 1 | 2 | 3 | 1 | 4 | 0 | 5 | 6 | 11 (1.8%) |
| K. aerugenes | 0 | 0 | 1 | 0 | 1 | 2 | 3 | 1 | 4 (0.65%) |
| K. oxytoca | 0 | 0 | 1 | 0 | 0 | 1 | 1 | 1 | 2 (0.33%) |
| Acinetobacter baumannii complex | 0 | 0 | 0 | 1 | 0 | 0 | 1 | 0 | 1 (0.16%) |
| Bacteroides vulgatus | 0 | 0 | 0 | 0 | 0 | 1 | 1 | 0 | 1 (0.16%) |
| Citrobacter koseri | 0 | 0 | 0 | 0 | 0 | 2 | 2 | 0 | 2 (0.33%) |
| Porphyromonas somerae | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 1 | 1 (0.16%) |
| Fungus (Candida species) | 1 | 3 | 4 | 2 | 3 | 2 | 10 | 5 | 15 (2.45%) |
| Bacillus species | 0 | 0 | 1 | 0 | 2 | 1 | 2 | 2 | 4 (0.65%) |
| Brevibacterium luteolum | 0 | 0 | 1 | 0 | 0 | 0 | 1 | 0 | 1 (0.16%) |
| Total by year | 75 | 98 | 96 | 114 | 118 | 111 | 364 | 248 | 612 (100%) |
| Pathogen | 2016 | 2017 | 2018 | 2019 | 2020 | 2021 | 2016–2021 | Total | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| r | s | r | s | r | s | r | s | r | s | r | s | r | s | |||
| S. aureus | oxacillin | 3 | 11 | 0 | 11 | 1 | 10 | 1 | 14 | 0 | 20 | 1 | 13 | 6 | 79 | 85 a |
| rifampicin | 3 | 11 | 1 | 10 | 1 | 10 | 0 | 15 | 0 | 20 | 1 | 13 | 6 | 79 | 85 a | |
| vancomycin | 0 | 14 | 0 | 11 | 0 | 11 | 0 | 15 | 0 | 20 | 0 | 14 | 0 | 85 | 85 a | |
| coagulase negative staphylococci | oxacillin | 24 | 13 | 22 | 14 | 33 | 10 | 26 | 27 | 34 | 19 | 22 | 25 | 161 | 108 | 269 b |
| rifampicin | 8 | 30 | 11 | 25 | 11 | 32 | 12 | 41 | 19 | 36 | 6 | 42 | 67 | 206 | 273 c | |
| vancomycin | 0 | 38 | 1 | 35 | 0 | 43 | 1 | 53 | 0 | 55 | 0 | 47 | 2 | 271 | 271 d | |
| Streptococcus species | penicillin G | 0 | 4 | 0 | 11 | 0 | 9 | 0 | 9 | 0 | 7 | 0 | 8 | 0 | 48 | 48 |
| Enterococcus species | ampicillin | 2 f | 7 | 5 f | 9 | 0 | 11 | 4 f | 7 | 0 | 2 | 0 | 10 | 11 | 46 | 57 a |
| vancomycin | 0 | 9 | 1 f | 13 | 0 | 11 | 1 f | 10 | 0 | 2 | 0 | 10 | 2 | 54 | 56 e | |
| Gram-negative bacteria | piperacillin-tazobactam | 3 | 3 | 0 | 12 | 1 | 12 | 4 | 9 | 8 | 6 | 8 | 12 | 24 | 54 | 78 e |
| ciprofloxacin | 0 | 6 | 3 | 9 | 1 | 12 | 5 | 9 | 3 | 11 | 6 | 13 | 18 | 60 | 78 e | |
| meropenem | 0 | 6 | 0 | 12 | 0 | 13 | 1 | 13 | 0 | 14 | 0 | 20 | 1 | 78 | 79 a | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fröschen, F.S.; Randau, T.M.; Franz, A.; Molitor, E.; Hoerauf, A.; Hischebeth, G.T.R. Microbiological Trends and Antibiotic Susceptibility Patterns in Patients with Periprosthetic Joint Infection of the Hip or Knee over 6 Years. Antibiotics 2022, 11, 1244. https://doi.org/10.3390/antibiotics11091244
Fröschen FS, Randau TM, Franz A, Molitor E, Hoerauf A, Hischebeth GTR. Microbiological Trends and Antibiotic Susceptibility Patterns in Patients with Periprosthetic Joint Infection of the Hip or Knee over 6 Years. Antibiotics. 2022; 11(9):1244. https://doi.org/10.3390/antibiotics11091244
Chicago/Turabian StyleFröschen, Frank Sebastian, Thomas Martin Randau, Alexander Franz, Ernst Molitor, Achim Hoerauf, and Gunnar Thorben Rembert Hischebeth. 2022. "Microbiological Trends and Antibiotic Susceptibility Patterns in Patients with Periprosthetic Joint Infection of the Hip or Knee over 6 Years" Antibiotics 11, no. 9: 1244. https://doi.org/10.3390/antibiotics11091244