
Steering Away from Current Amoxicillin Dose Reductions in Hospitalized Patients with Impaired Kidney Function to Avoid Subtherapeutic Drug Exposure
 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient and Data Collection
2.2. Population Pharmacokinetic Modelling
2.3. Dose Evaluations
3. Results
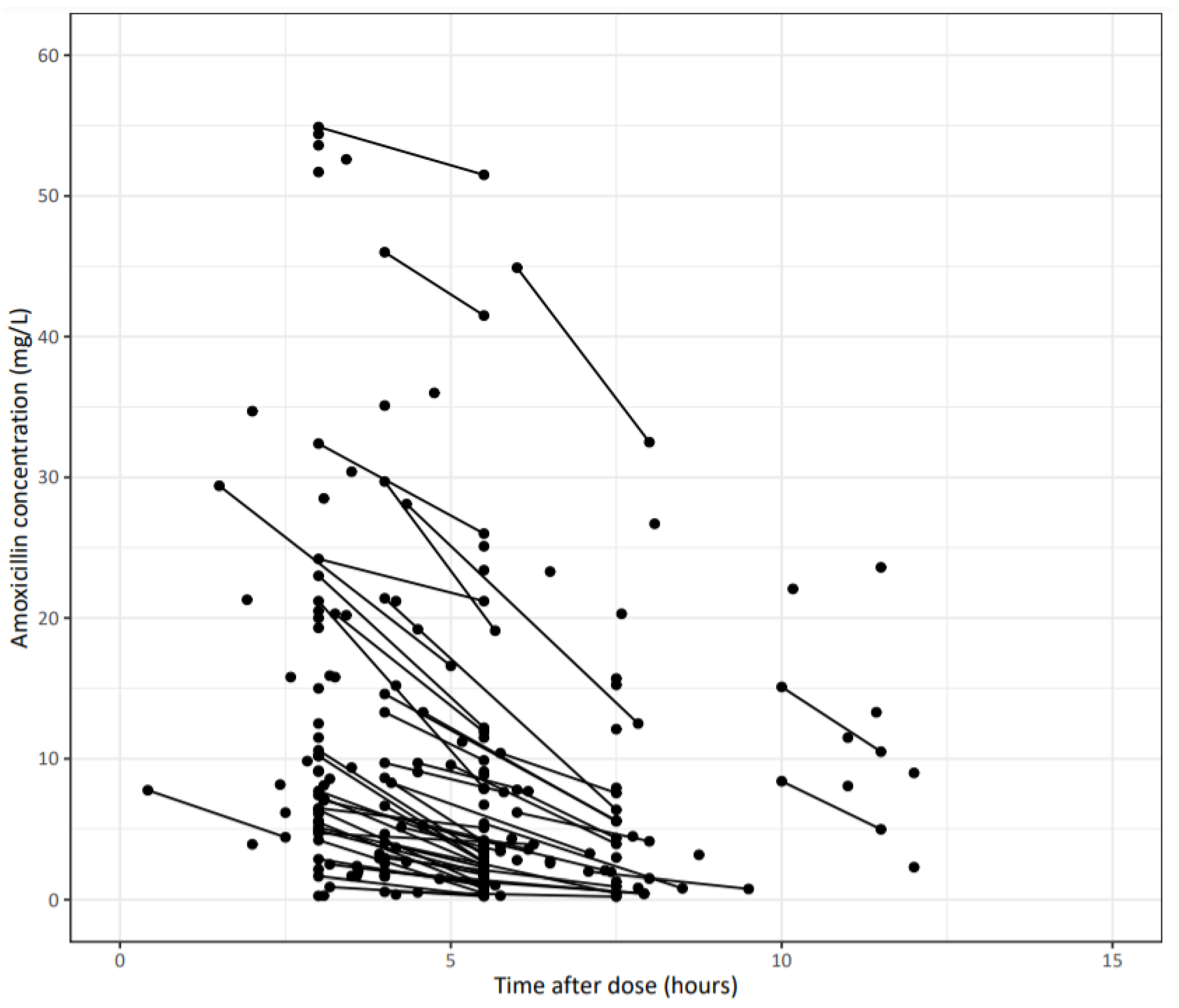
3.1. Dataset
3.2. Population Pharmacokinetic Modelling
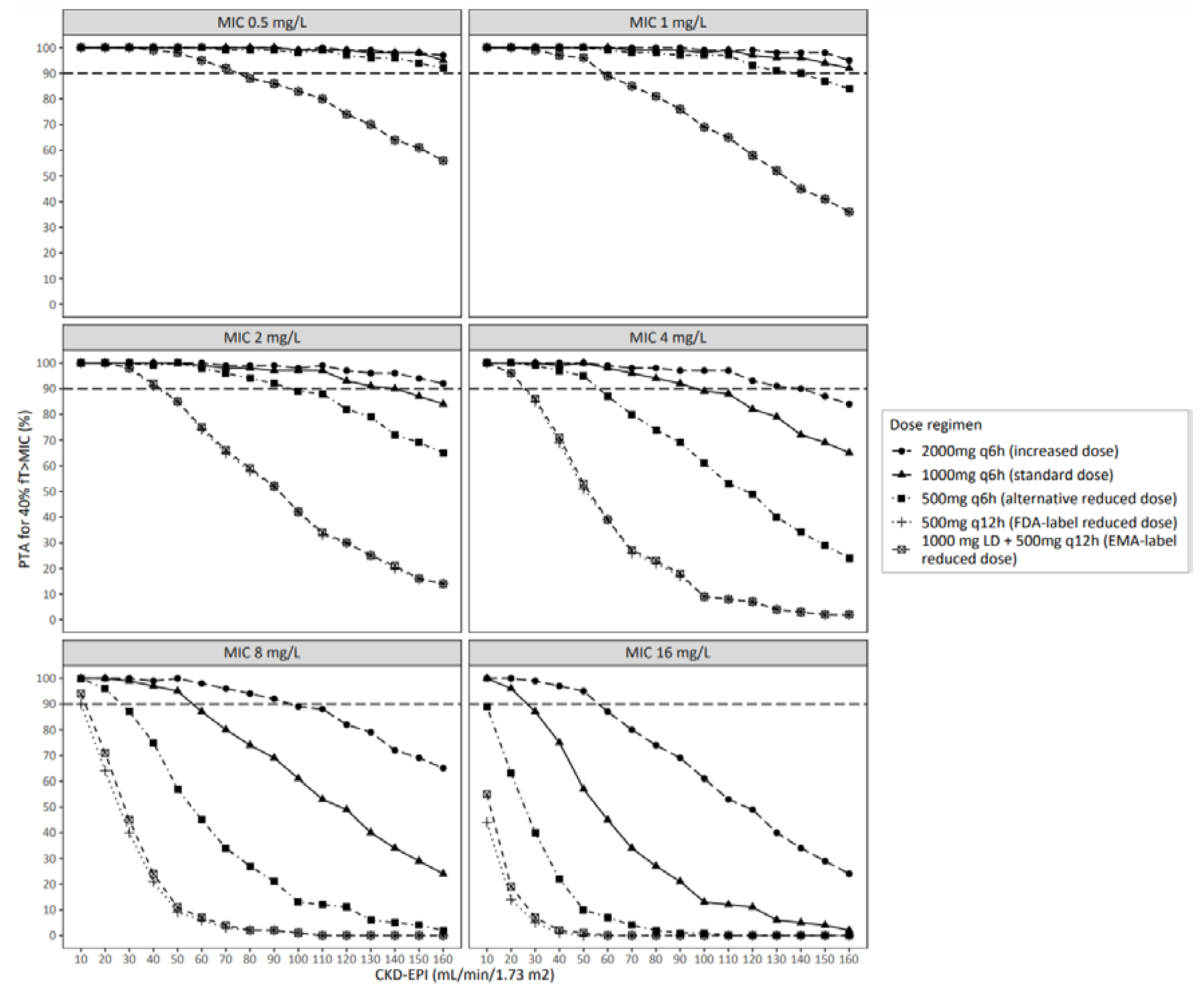
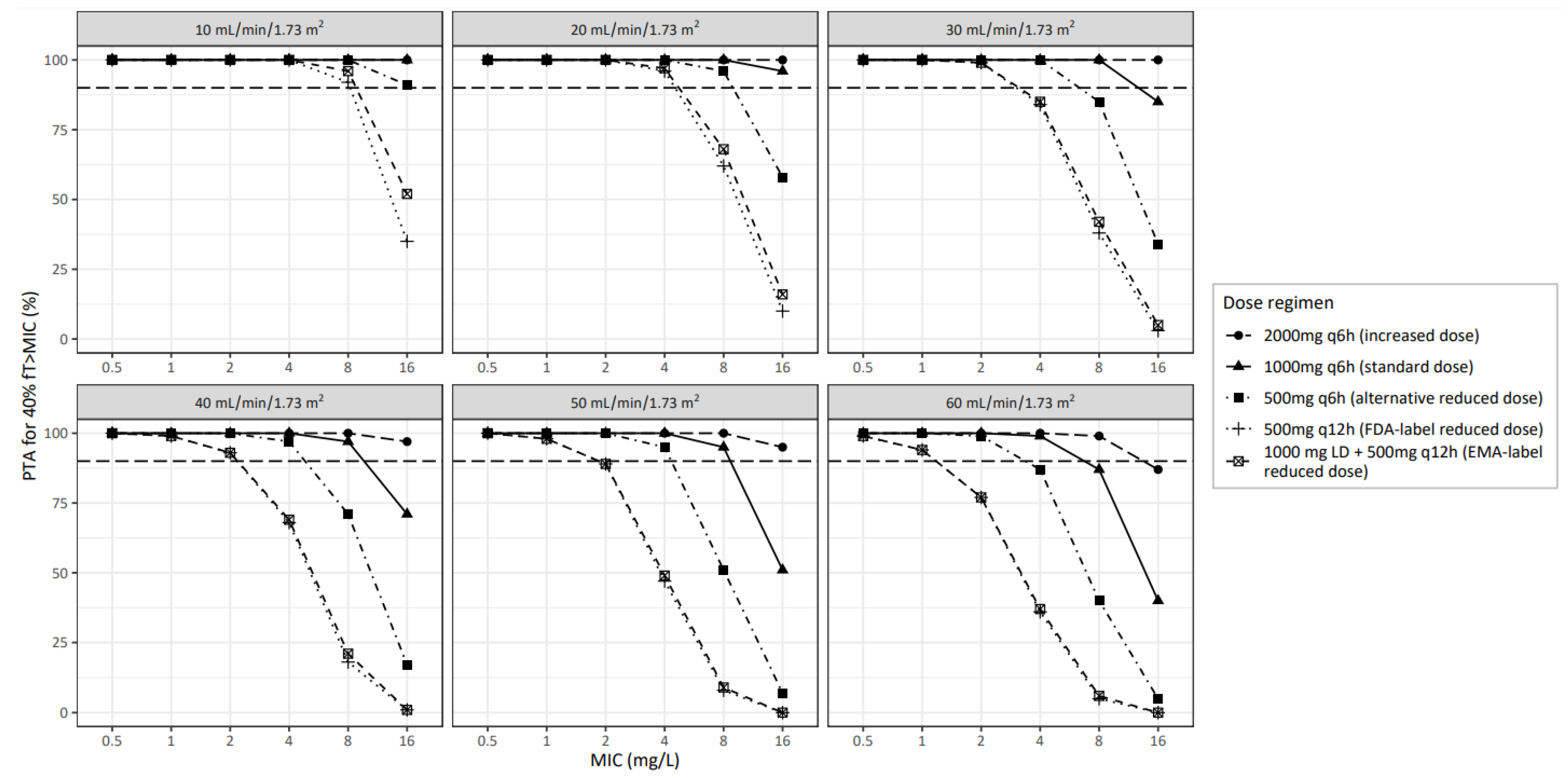
3.3. Dose Evaluations
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mouton, J.W.; Ambrose, P.G.; Canton, R.; Drusano, G.L.; Harbarth, S.; MacGowan, A.; Theuretzbacher, U.; Turnidge, J. Conserving Antibiotics for the Future: New Ways to Use Old and New Drugs from a Pharmacokinetic and Pharmacodynamic Perspective. Drug Resist. Updat. 2011, 14, 107–117. [Google Scholar] [CrossRef] [PubMed]
- Lonsdale, D.O.; Baker, E.H.; Kipper, K.; Barker, C.; Philips, B.; Rhodes, A.; Sharland, M.; Standing, J.F. Scaling Beta-Lactam Antimicrobial Pharmacokinetics from Early Life to Old Age. Br. J. Clin. Pharmacol. 2019, 85, 316–346. [Google Scholar] [CrossRef] [PubMed]
- De Schuyter, K.; Colin, P.J.; Vanommeslaeghe, F.; Delanghe, S.; De Cock, P.; Veys, N.; De Paepe, P.; Van Biesen, W.; Eloot, S. Optimizing Amoxicillin/Clavulanic Acid Dosing Regimens in Patients on Maintenance High-Flux Hemodialysis. Am. J. Kidney Dis. 2021, 78, 153–156. [Google Scholar] [CrossRef]
- Carlier, M.; Noë, M.; De Waele, J.J.; Stove, V.; Verstraete, A.G.; Lipman, J.; Roberts, J.A. Population Pharmacokinetics and Dosing Simulations of Amoxicillin/Clavulanic Acid in Critically Ill Patients. J. Antimicrob. Chemother. 2013, 68, 2600–2608. [Google Scholar] [CrossRef] [PubMed]
- De Cock, P.A.J.G.; Standing, J.F.; Barker, C.I.S.; De Jaeger, A.; Dhont, E.; Carlier, M.; Verstraete, A.G.; Delanghe, J.R.; Robays, H.; De Paepe, P. Augmented Renal Clearance Implies a Need for Increased Amoxicillin-Clavulanic Acid Dosing in Critically Ill Children. Antimicrob. Agents Chemother. 2015, 59, 7027–7035. [Google Scholar] [CrossRef]
- Van Donge, T.; Fuchs, A.; Leroux, S.; Pfister, M.; Rodieux, F.; Atkinson, A.; Giannoni, E.; Van Den Anker, J.; Bielicki, J. Amoxicillin Dosing Regimens for the Treatment of Neonatal Sepsis: Balancing Efficacy and Neurotoxicity. Neonatology 2021, 117, 619–627. [Google Scholar] [CrossRef] [PubMed]
- European Medicines Agency (EMA). Amoxil: Summary of Product Characteristics, Labelling and Package Leaflet 2016; EMA: Amsterdam, The Netherlands, 2016. [Google Scholar]
- Food and Drug Administration (FDA). Amoxil: Product Label; FDA: White Oak, MA, USA, 2006. [Google Scholar]
- Fournier, A.; Goutelle, S.; Que, Y.-A.; Eggimann, P.; Pantet, O.; Sadeghipour, F.; Voirol, P.; Csajka, C. Population Pharmacokinetic Study of Amoxicillin-Treated Burn Patients Hospitalized at a Swiss Tertiary-Care Center. Antimicrob. Agents Chemother. 2018, 62, e00505-18. [Google Scholar] [CrossRef] [PubMed]
- European Committee on Antimicrobial Susceptibility Testing (EUCAST). Amoxicillin. Rationale for the EUCAST Clinical Breakpoints, Version 1.0 2010; EUCAST: Stockholm, Sweden, 2010. [Google Scholar]
- Knaus, W.A.; Draper, E.A.; Wagner, D.P.; Zimmerman, J.E. APACHE II: A Severity of Disease Classification System. Crit. Care Med. 1985, 13, 818–829. [Google Scholar] [CrossRef]
- Seymour, C.W.; Liu, V.X.; Iwashyna, T.J.; Brunkhorst, F.M.; Rea, T.D.; Scherag, A.; Rubenfeld, G.; Kahn, J.M.; Shankar-Hari, M.; Singer, M.; et al. Assessment of Clinical Criteria for Sepsis: For the Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 762–774. [Google Scholar] [CrossRef]
- Cockcroft, D.W.; Gault, M.H. Prediction of Creatinine Clearance from Serum Creatinine. Nephron 1976, 16, 31–41. [Google Scholar] [CrossRef]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.L.; Castro, A.F.; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T.; et al. A New Equation to Estimate Glomerular Filtration Rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef]
- Levey, A.S.; Coresh, J.; Greene, T.; Stevens, L.A.; Zhang, Y.L.; Hendriksen, S.; Kusek, J.W.; Van Lente, F. Chronic Kidney Disease Epidemiology Collaboration Using Standardized Serum Creatinine Values in the Modification of Diet in Renal Disease Study Equation for Estimating Glomerular Filtration Rate. Ann. Intern. Med. 2006, 145, 247–254. [Google Scholar] [CrossRef]
- National Kidney Foundation K/DOQI. Clinical Practice Guidelines for Chronic Kidney Disease: Evaluation, Classification, and Stratification. Am. J. Kidney Dis. 2002, 39. [Google Scholar]
- Lixoft SAS Monolix, Version 2020R1; Lixoft: Anthony, France, 2020.
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2019. [Google Scholar]
- RStudio. Team RStudio: Integrated Development for R; RStudio: Boston, MA, USA, 2021. [Google Scholar]
- European Committee on Antimicrobial Susceptibility Testing (EUCAST). Clinical Breakpoints—Bacteria (v 11.0) 2021; EUCAST: Stockholm, Sweden, 2021. [Google Scholar]
- Arancibia, A.; Guttmann, J.; Gonzalez, C. Absorption and Disposition Kinetics of Amoxicillin in Normal Human Subjects. Antimicrob. Agents Chemother. 1980, 17, 199–202. [Google Scholar] [CrossRef]
- Paintaud, G.; Alván, G.; Dahl, M.L.; Grahnén, A.; Sjövall, J.; Svensson, J.O. Nonlinearity of Amoxicillin Absorption Kinetics in Human. Eur. J. Clin. Pharmacol. 1992, 43, 283–288. [Google Scholar] [CrossRef] [PubMed]
- De Velde, F.; de Winter, B.C.M.; Koch, B.C.P.; van Gelder, T.; Mouton, J.W. Non-Linear Absorption Pharmacokinetics of Amoxicillin: Consequences for Dosing Regimens and Clinical Breakpoints. J. Antimicrob. Chemother. 2016, 71, 2909–2917. [Google Scholar] [CrossRef]
- Marti, C.; Stirnemann, J.; Lescuyer, P.; Tonoli, D.; von Dach, E.; Huttner, A. Therapeutic Drug Monitoring and Clinical Outcomes in Severely Ill Patients Receiving Amoxicillin: A Single-Centre Prospective Cohort Study. Int. J. Antimicrob. Agents 2022, 59, 106601. [Google Scholar] [CrossRef] [PubMed]
- Haeseker, M.; Havenith, T.; Stolk, L.; Neef, C.; Bruggeman, C.; Verbon, A. Is the Standard Dose of Amoxicillin-Clavulanic Acid Sufficient? BMC Pharmacol. Toxicol. 2014, 15, 38. [Google Scholar] [CrossRef] [PubMed]
- Roberts, J.A.; Paul, S.K.; Akova, M.; Bassetti, M.; De Waele, J.J.; Dimopoulos, G.; Kaukonen, K.M.; Koulenti, D.; Martin, C.; Montravers, P.; et al. DALI: Defining Antibiotic Levels in Intensive Care Unit Patients: Are Current β-Lactam Antibiotic Doses Sufficient for Critically Ill Patients? Clin. Infect. Dis. 2014, 58, 1072–1083. [Google Scholar] [CrossRef] [PubMed]
- Humbert, G.; Spyker, D.A.; Fillastre, J.P.; Leroy, A. Pharmacokinetics of Amoxicillin: Dosage Nomogram for Patients with Impaired Renal Function. Antimicrob. Agents Chemother. 1979, 15, 28–33. [Google Scholar] [CrossRef]
- Teo, S.H.; Endre, Z.H. Biomarkers in Acute Kidney Injury (AKI). Best Pract. Res. Clin. Anaesthesiol. 2017, 31, 331–344. [Google Scholar] [CrossRef] [PubMed]
- Yang, H.S.; Hur, M.; Lee, K.R.; Kim, H.; Kim, H.Y.; Kim, J.W.; Chua, M.T.; Kuan, W.S.; Chua, H.R.; Kitiyakara, C.; et al. Biomarker Rule-in or Rule-out in Patients with Acute Diseases for Validation of Acute Kidney Injury in the Emergency Department (BRAVA): A Multicenter Study Evaluating Urinary TIMP-2/IGFBP7. Ann. Lab. Med. 2022, 42, 178–187. [Google Scholar] [CrossRef] [PubMed]
- Jacobsen, E.; Sawhney, S.; Brazzelli, M.; Aucott, L.; Scotland, G.; Aceves-Martins, M.; Robertson, C.; Imamura, M.; Poobalan, A.; Manson, P.; et al. Cost-Effectiveness and Value of Information Analysis of NephroCheck and NGAL Tests Compared to Standard Care for the Diagnosis of Acute Kidney Injury. BMC Nephrol. 2021, 22, 399. [Google Scholar] [CrossRef] [PubMed]
- Jia, L.; Sheng, X.; Zamperetti, A.; Xie, Y.; Corradi, V.; Chandel, S.; De Cal, M.; Montin, D.P.; Caprara, C.; Ronco, C. Combination of Biomarker with Clinical Risk Factors for Prediction of Severe Acute Kidney Injury in Critically Ill Patients. BMC Nephrol. 2020, 21, 540. [Google Scholar] [CrossRef]
- Teaford, H.R.; Barreto, J.N.; Vollmer, K.J.; Rule, A.D.; Barreto, E.F. Cystatin C: A Primer for Pharmacists. Pharmacy 2020, 8, 35. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Patient Characteristic | Value a |
|---|---|
| Age (years) | 72 (54–80) (16–93) |
| Gender (female, n (%)) | 51 (33) |
| Weight (kg) | 70 (61–83) (30–140) |
| Route of administration (n (%)) | IV: 141 (91) Oral: 9 (6) IV + oral: 5 (3) |
| Admitted to ICU (n (%)) | 107 (69) |
| Indication for amoxicillin treatment (n (%)) | (Suspected) pneumonia: 113 (73) Wound infection: 15 (10) Catheter infection: 2 (1) Urinary tract infection: 1 (1) Other: 24 (15) |
| APACHE II score b | 26 (20–30) (3–45) |
| qSOFA score (n (%)) | 0: 23 (15) 1: 56 (36) 2: 55 (35) 3: 21 (14) |
| Serum creatinine (mcmol/L) d | 78 (59–106) (36–413) |
| Chronic kidney disease class (based on K/DOQI criteria, n (%)) [16] c | Normal (CKD-EPI >90): 85 (54) Mild (CKD-EPI 60–89): 33 (21) Moderate (CKD-EPI 30–59): 25 (16) Severe (CKD-EPI 15–29): 9 (6) Kidney failure (CKD–EPI <15): 3 (2) |
| CKD-EPI (mL/min/1.73 m2) | 94.4 (67.0–115.6) (11.5–165.8) |
| MDRD (mL/min/1.73 m2) | 81.5 (54.9–110.9) (10.1–202.7) |
| CG (mL/min) | 78.8 (44.1–108.3) (10.5–220.9) |
| Parameter | Estimate (%RSE) | Bootstrap Estimate (95% CI) |
|---|---|---|
| Population parameters | ||
| F (%) | 49.8 (15) | 56.4 (29.6–100) |
| Ka (h−1) | 1.02 FIX | 1.02 FIX |
| CLi = CLpop × (WT/70)0.75 × (CKD-EPI/94) | ||
| CLpop (L/h) | 17.2 (5) | 16.9 (14.7–19.2) |
| Vd,i = Vd,pop × (WT/70)0.75 | ||
| Vd,pop (L) | 56.6 (6) | 53.6 (41.3–69.7) |
| Interindividual variability | ||
| ωKa | 0.2 FIX | 0.2 FIX |
| ωCL | 0.481 (8) | 0.473 (0.376–0.572) |
| ωVd | 0.226 (20) | 0.339 (0.180–0.610) |
| Residual variability | ||
| Additional error (mg/L) | 0.146 (36) | 0.206 (0.012–0.53) |
| Proportional error (SD) | 0.226 (15) | 0.175 (0.029–0.307) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Smit, C.; Sen, S.; von Dach, E.; Karmime, A.; Lescuyer, P.; Tonoli, D.; Bielicki, J.; Huttner, A.; Pfister, M. Steering Away from Current Amoxicillin Dose Reductions in Hospitalized Patients with Impaired Kidney Function to Avoid Subtherapeutic Drug Exposure. Antibiotics 2022, 11, 1190. https://doi.org/10.3390/antibiotics11091190
Smit C, Sen S, von Dach E, Karmime A, Lescuyer P, Tonoli D, Bielicki J, Huttner A, Pfister M. Steering Away from Current Amoxicillin Dose Reductions in Hospitalized Patients with Impaired Kidney Function to Avoid Subtherapeutic Drug Exposure. Antibiotics. 2022; 11(9):1190. https://doi.org/10.3390/antibiotics11091190
Chicago/Turabian StyleSmit, Cornelis, Swapnoleena Sen, Elodie von Dach, Abderrahim Karmime, Pierre Lescuyer, David Tonoli, Julia Bielicki, Angela Huttner, and Marc Pfister. 2022. "Steering Away from Current Amoxicillin Dose Reductions in Hospitalized Patients with Impaired Kidney Function to Avoid Subtherapeutic Drug Exposure" Antibiotics 11, no. 9: 1190. https://doi.org/10.3390/antibiotics11091190