
Microbiology of Healthcare-Associated Infections: Results of a Fourth National Point Prevalence Survey in Serbia

 , , , ,
, , , ,
Abstract
:1. Introduction
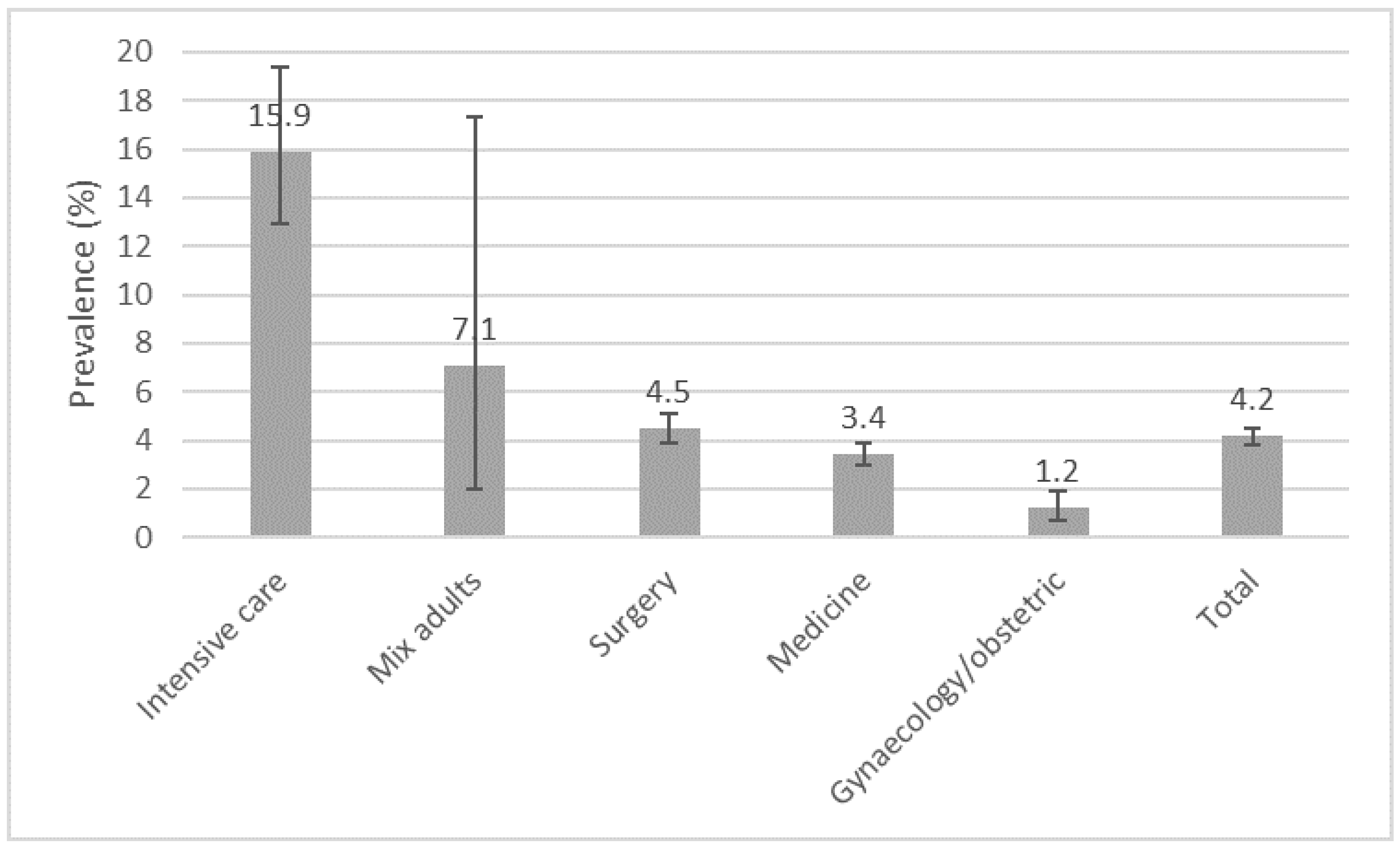
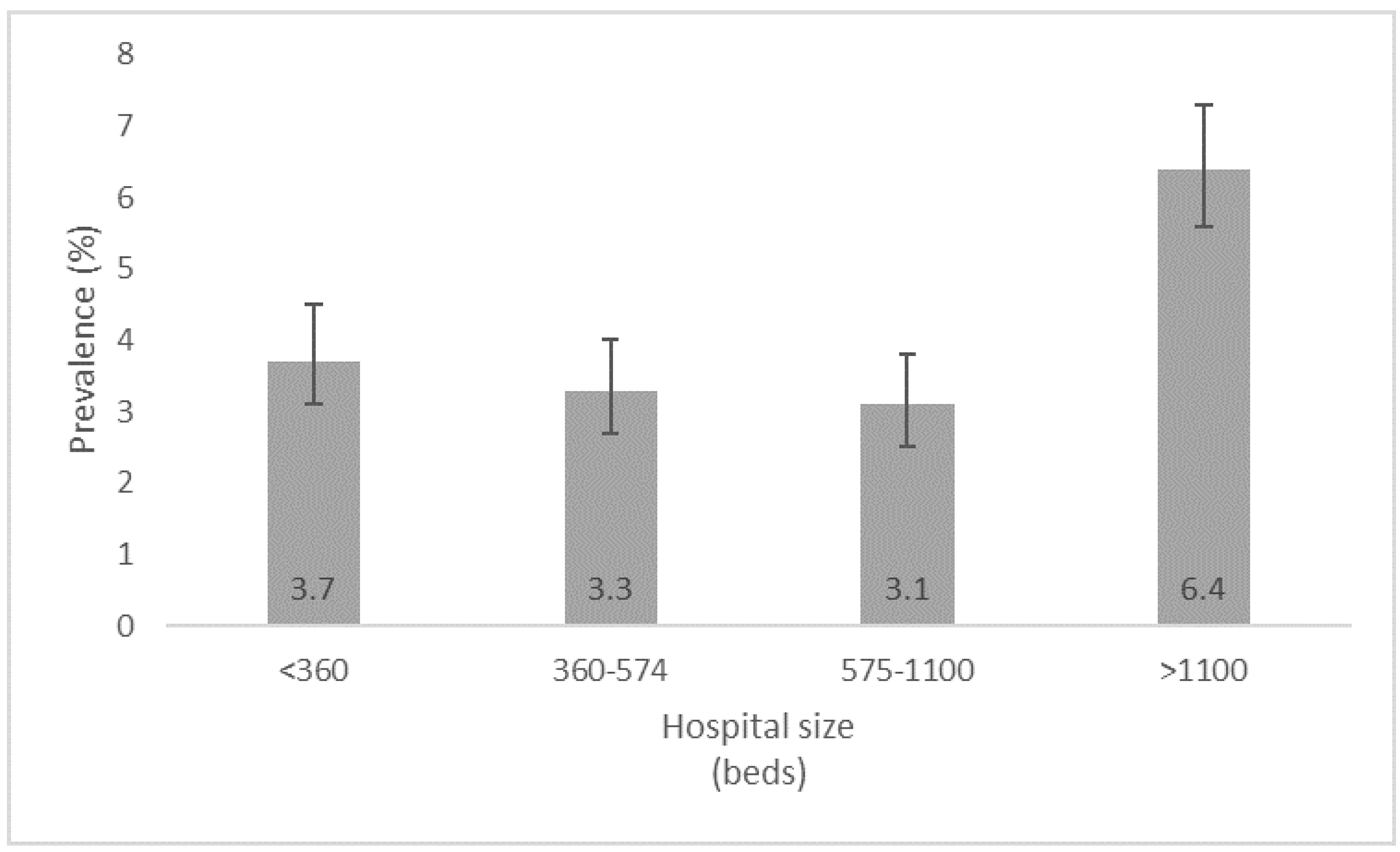
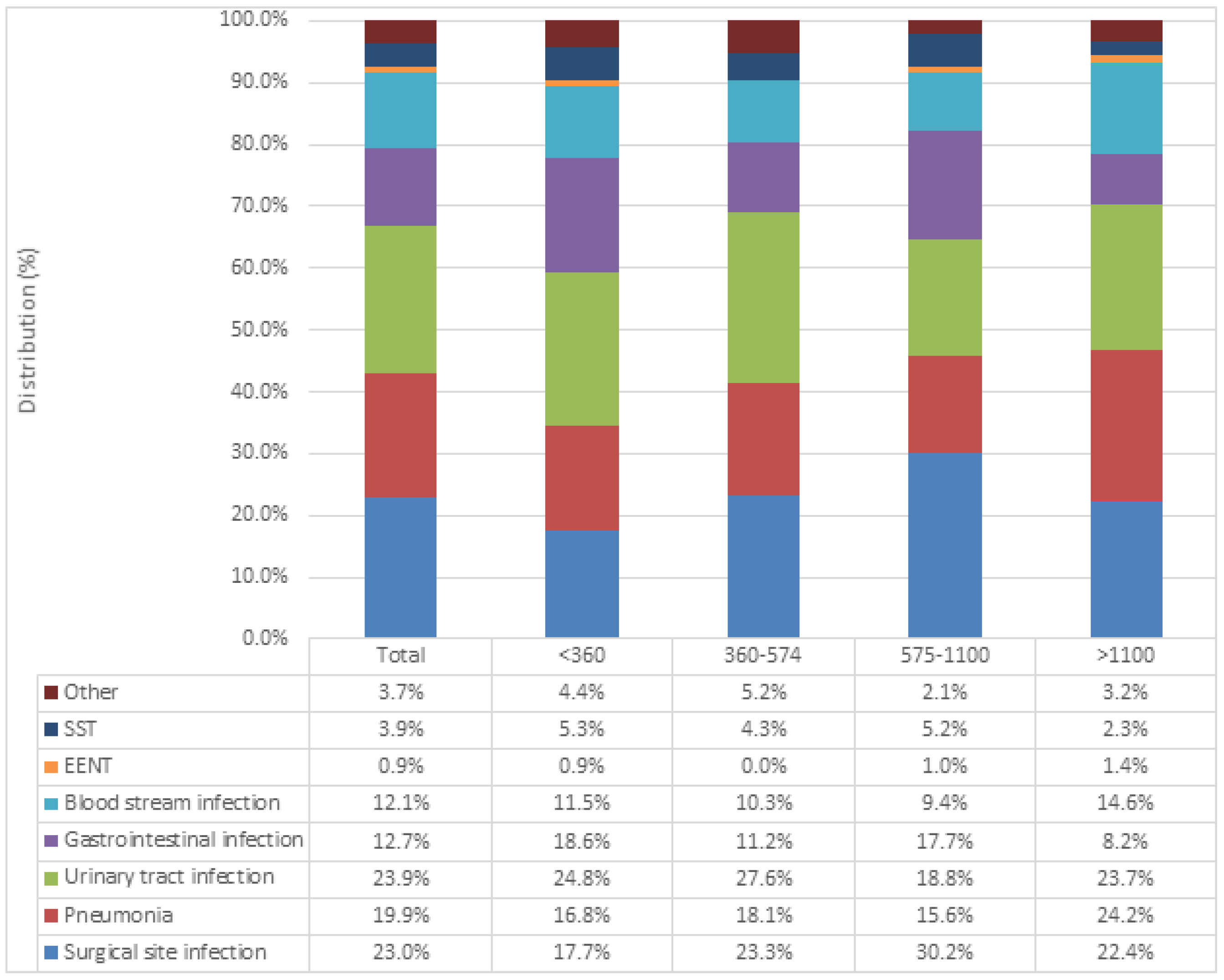
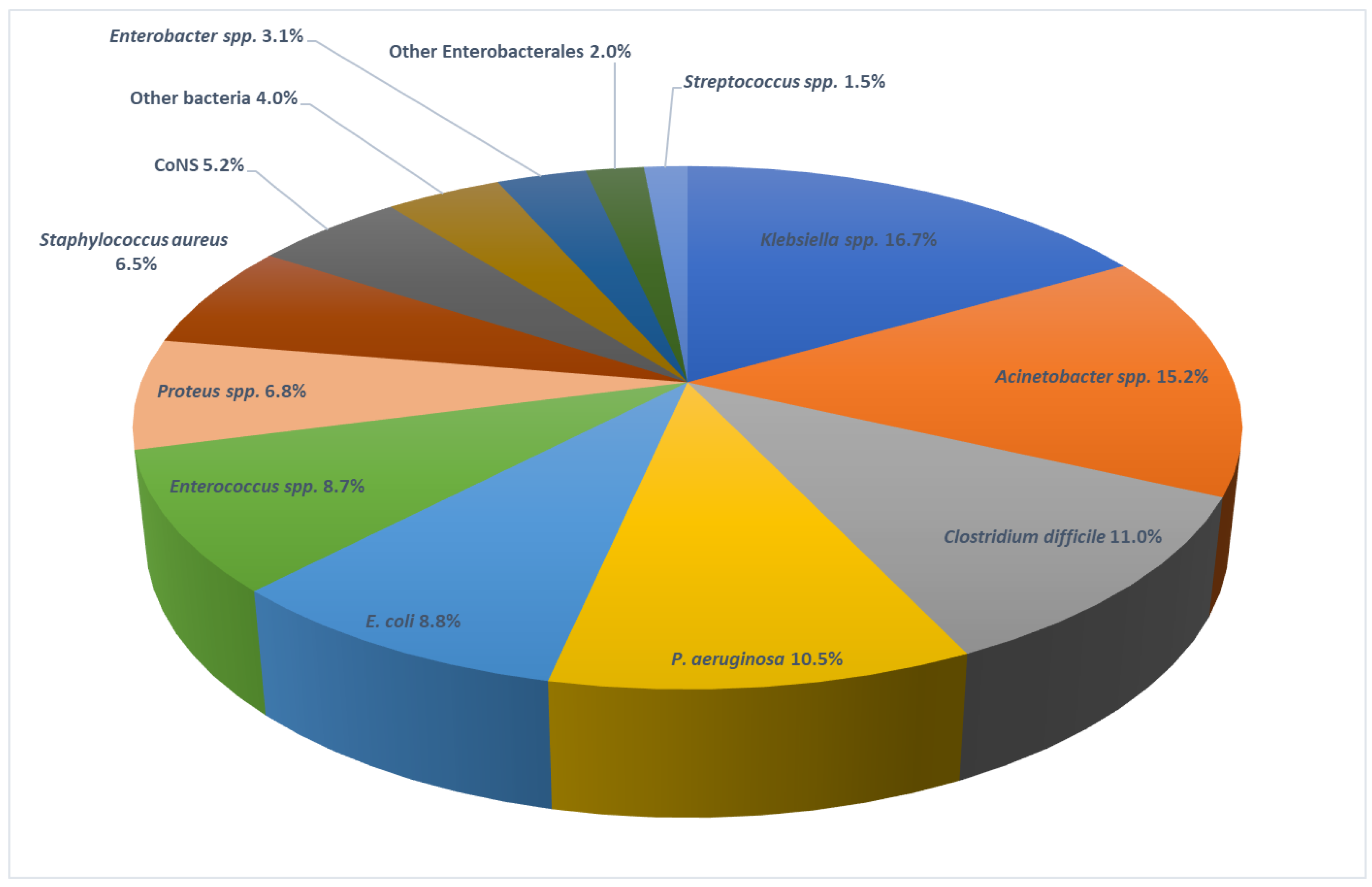
2. Results
3. Discussion
4. Materials and Methods
4.1. Design and Study Setting
4.2. Data Collection
4.3. Ethical Consideration
4.4. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kärki, T.; Plachouras, D.; Cassini, A.; Suetens, C. Burden of healthcare-associated infections in European acute care hospitals. Wien. Med. Wochenschr. 2019, 169, 3–5. [Google Scholar] [CrossRef] [PubMed]
- Fernando, S.A.; Gray, T.J.; Gottlieb, T. Healthcare-acquired infections: Prevention strategies. Intern. Med. J. 2017, 47, 1341–1351. [Google Scholar] [CrossRef] [PubMed]
- Arnoldo, L.; Smaniotto, C.; Celotto, D.; Brunelli, L.; Cocconi, R.; Tignonsini, D.; Faruzzo, A.; Brusaferro, S. Monitoring healthcare-associated infections and antimicrobial use at regional level through repeated point prevalence surveys: What can be learnt? J. Hosp. Infect. 2019, 101, 447–454. [Google Scholar] [CrossRef] [PubMed]
- Antimicrobial Resistance Collaborators. Global burden of bacterial antimicrobial resistance in 2019: A systematic analysis. Lancet 2022, 399, 629–655. [Google Scholar] [CrossRef]
- Friedrich, A.W. Control of hospital acquired infections and antimicrobial resistance in Europe: The way to go. Wien. Med. Wochenschr. 2019, 169, 25–30. [Google Scholar] [CrossRef]
- ECDC. Point Prevalence Survey of Healthcare-Associated Infections and Antimicrobial Use in European Acute Care Hospitals—ECDC PPS Validation Protocol Version 3.1.2; European Centre for Disease Prevention and Control: Stockholm, Sweden, 2019; Available online: https://www.ecdc.europa.eu/en/publications-data/point-prevalence-survey-healthcare-associated-infections-and-antimicrobial-use-4 (accessed on 15 June 2022).
- Suetens, C.; Latour, K.; Kärki, T.; Ricchizzi, E.; Kinross, P.; Moro, M.L.; Jans, B.; Hopkins, S.; Hansen, S.; Lyytikäinen, O.; et al. Prevalence of healthcare-associated infections, estimated incidence and composite antimicrobial resistance index in acute care hospitals and long-term care facilities: Results from two european point prevalence surveys, 2016 to 2017. Eurosurveillance 2018, 23, 1800516. [Google Scholar] [CrossRef]
- Klavs, I.; Serdt, M.; Korošec, A.; Lejko Zupanc, T.; Pečavar, B. Prevalence of And Factors Associated with Healthcare-associated Infections in Slovenian Acute Care Hospitals: Results of the Third National Survey. Zdr. Varst. 2019, 58, 62–69. [Google Scholar] [CrossRef]
- Kritsotakis, E.I.; Kontopidou, F.; Astrinaki, E.; Roumbelaki, M.; Ioannidou, E.; Gikas, A. Prevalence, incidence burden, and clinical impact of healthcare-associated infections and antimicrobial resistance: A national prevalent cohort study in acute care hospitals in Greece. Infect. Drug Resist. 2017, 10, 317–328. [Google Scholar] [CrossRef]
- Vandael, E.; Catry, B.; Latour, K. Point Prevalence Study of Healthcare—Associated Infections and Antimicrobial Use in Belgian Acute Care Hospitals: Results of the ECDC PPS 2017; Report Number: D/2018/14.440/37; Sciensano: Brussels, Belgium, 2018; 34p, Available online: https://www.sciensano.be/en/biblio/point-prevalence-study-healthcare-associated-infections-and-antimicrobial-use-belgian-acute-care (accessed on 15 June 2022).
- Pitkäpaasi, M.; Lehtinen, J.-M.; Kanerva, M. Point prevalence survey is useful for introducing effective surveillance of healthcare-associated infections. Infect. Prev. Pract. 2021, 3, 100182. [Google Scholar] [CrossRef]
- Zingg, W.; Metsini, A.; Balmelli, C.; Neofytos, D.; Behnke, M.; Gardiol, C.; Widmer, A.; Pittet, D.; Network, O.B.O.T.S. National point prevalence survey on healthcare-associated infections in acute care hospitals, Switzerland, 2017. Eurosurveillance 2019, 24, 1800603. [Google Scholar] [CrossRef] [Green Version]
- Markovic-Denic, L.; Drndarevic, D.; Milic, N.; Bukumirovic, K.; Jankovic, S. Prevalence study of hospital infections in Serbia. Glas. Inst. Zast. Zdr. Srb. 2000, 74, 37–80. (In Serbian) [Google Scholar]
- Šuljagić, V.; Bajčetić, M.; Mioljević, V.; Dragovac, G.; Mijović, B.; Janićijević, I.; Đorđević, Z.; Krtinić, G.; Rakić, V.; Ćirković, I.; et al. A nationwide assessment of the burden of healthcare-associated infections and antimicrobial use among surgical patients: Results from Serbian point prevalence survey, 2017. Antimicrob. Resist. Infect. Control 2021, 10, 47. [Google Scholar] [CrossRef] [PubMed]
- Markovic-Denic, L.; Milic, N.; Knezevic, T.; Prevalence Study Working Group. The second prevalence study of hospital infections in Serbia. Glas. Inst. Zast. Zdr. Srb. 2007, 79, 5–85. (In Serbian) [Google Scholar]
- Ministry of Health of Republic of Serbia. Third National Prevalence Study of Hospital Infections, 2010; Ministry of Health of Republic of Serbia: Belgrade, Serbia, 2012.
- European Centre for Disease Prevention and Control. Healthcare-Associated Infections Acquired in Intensive Care Units. Annual Epidemiological Report for 2017; ECDC: Stockholm, Sweden, 2019; Available online: https://www.ecdc.europa.eu/sites/default/files/documents/AER_for_2017-HAI.pdf (accessed on 20 June 2022).
- Deptuła, A.; Trejnowska, E.; Ozorowski, T.; Hryniewicz, W. Risk factors for healthcare-associated infection in light of two years of experience with the ECDC point prevalence survey of healthcare-associated infection and antimicrobial use in Poland. J. Hosp. Infect. 2015, 90, 310–315. [Google Scholar] [CrossRef] [PubMed]
- Salmanov, A.G.; Vdovychenko, S.Y.; Litus, O.I.; Litus, V.I.; Bisyuk, Y.A.; Bondarenko, T.M.; Davtian, L.L.; Olifirova, T.F.; Leleka, M.V.; Kovalchuk, O.I.; et al. Prevalence of health care-associated infections and antimicrobial resistance of the responsible pathogens in Ukraine: Results of a multicenter study (2014–2016). Am. J. Infect. Control 2019, 47, e15–e20. [Google Scholar] [CrossRef] [PubMed]
- The Centers for Disease Control and Prevention—CDC. Guideline for Prevention of Catheter-Associated Urinary Tract Infections (2009). HICPAC. Last Update: 6 June 2019. Available online: https://www.cdc.gov/infectioncontrol/pdf/guidelines/cautiguidelines-H.pdf (accessed on 20 June 2022).
- Cai, Y.; Venkatachalam, I.; Tee, N.W.; Tan, T.Y.; Kurup, A.; Wong, S.Y.; Low, C.Y.; Wang, Y.; Lee, W.; Liew, Y.X.; et al. Prevalence of Healthcare-Associated Infections and Antimicrobial Use Among Adult Inpatients in Singapore Acute-Care Hospitals: Results From the First National Point Prevalence Survey. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2017, 64, S61–S67. [Google Scholar] [CrossRef]
- Russo Fiorino, G.; Maniglia, M.; Marchese, V.; Aprea, L.; Torregrossa, M.V.; Campisi, F.; Favaro, D.; Calamusa, G.; Amodio, E. Healthcare-associated infections over an eight year period in a large university hospital in Sicily (Italy, 2011–2018). J. Infect. Prev. 2021, 22, 220–230. [Google Scholar] [CrossRef] [PubMed]
- Antonioli, P.; Bolognesi, N.; Valpiani, G.; Morotti, C.; Bernardini, D.; Bravi, F.; Di Ruscio, E.; Stefanati, A.; Gabutti, G. A 2-year point-prevalence surveillance of healthcare-associated infections and antimicrobial use in Ferrara University Hospital, Italy. BMC Infect. Dis. 2020, 20, 75. [Google Scholar] [CrossRef]
- Reilly, J.S.; Coignard, B.; Price, L.; Godwin, J.; Cairns, S.; Hopkins, S.; Lyytikäinen, O.; Hansen, S.; Malcolm, W.; Hughes, G.J. The reliability of the McCabe score as a marker of co-morbidity in healthcare-associated infection point prevalence studies. J. Infect. Prev. 2016, 17, 127–129. [Google Scholar] [CrossRef]
- Cassini, A.; Plachouras, D.; Eckmanns, T.; Abu Sin, M.; Blank, H.P.; Ducomble, T.; Haller, S.; Harder, T.; Klingeberg, A.; Sixtensson, M.; et al. Burden of Six Healthcare-Associated Infections on European Population Health: Estimating Incidence-Based Disability-Adjusted Life Years through a Population Prevalence-Based Modelling Study. PLoS Med. 2016, 13, e1002150. [Google Scholar] [CrossRef]
- Zarb, P.; Coignard, B.; Griskeviciene, J.; Muller, A.; Vankerckhoven, V.; Weist, K.; Goossens, M.M.; Vaerenberg, S.; Hopkins, S.; Catry, B.; et al. Point Prevalence Survey of Healthcare Associated Infections and Antimicrobial Use in European Acute Care Hospitals; ECDC: Stockholm, Sweden, 2012; Volume 17, ISBN 9789291934850. [Google Scholar]
- Savey, A.; Lepape European Centre for Disease Prevention and Control. Surveillance of Healthcare-Associated Infections and Prevention Indicators in European Intensive Care Units; European Centre for Disease Prevention and Control: Stockholm, Sweden, 2017; Available online: https://www.ecdc.europa.eu/en/publications-data/surveillance-healthcare-associated-infections-and-prevention-indicators-european (accessed on 20 June 2022).
- World Health Organization. Annual Report 2018. Central Asian and Eastern European Surveillance of Antimicrobial Resistance; WHO: Geneva, Switzerland, 2018; Available online: https://apps.who.int/iris/handle/10665/324806 (accessed on 20 June 2022).
- Wu, Q.; Sabokroo, N.; Wang, Y.; Hashemian, M.; Karamollahi, S.; Kouhsari, E. Systematic review and meta-analysis of the epidemiology of vancomycin-resistance Staphylococcus aureus isolates. Antimicrob. Resist. Infect. Control. 2021, 10, 101. [Google Scholar] [CrossRef] [PubMed]
- Brinkwirth, S.; Ayobami, O.; Eckmanns, T.; Markwart, R. Hospital-acquired infections caused by enterococci: A systematic review and meta-analysis, WHO European Region, 1 January 2010 to 4 February 2020. Eurosurveillance 2021, 26, 2001628. [Google Scholar] [CrossRef] [PubMed]
- Tomas, A.; Pavlović, N.; Stilinović, N.; Horvat, O.; Paut-Kusturica, M.; Dugandžija, T.; Tomić, Z.; Sabo, A. Increase and Change in the Pattern of Antibiotic Use in Serbia (2010–2019). Antibiotics 2021, 10, 397. [Google Scholar] [CrossRef] [PubMed]
- Tomas, A.; Paut Kusturica, M.; Tomić, Z.; Horvat, O.; Djurović Koprivica, D.; Bukumirić, D.; Sabo, A. Self-medication with antibiotics in Serbian households: A case for action? Int. J. Clin. Pharm. 2017, 39, 507–513. [Google Scholar] [CrossRef] [PubMed]
- Zingg, W.; Hopkins, S.; Gayet-Ageron, A.; Holmes, A.; Sharland, M.; Suetens, C. Health-care-associated infections in neonates, children, and adolescents: An analysis of paediatric data from the European Centre for Disease Prevention and Control pointprevalence survey. Lancet Infect. Dis. 2017, 17, 381–389. [Google Scholar] [CrossRef]
- Schreiber, P.W.; Sax, H.; Wolfensberger, A.; Clack, L.; Kuster, S.P.; Swissnoso. The preventable proportion of healthcare-associated infections 2005–2016: Systematic review and meta-analysis. Infect. Control Hosp. Epidemiol. 2018, 39, 1277–1295. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total n (%) | Non-HAI n (%) | HAI n (%) | p Value | |
|---|---|---|---|---|
| Total | 12,380 (100.0) | 11,865 (95.8) | 515 (4.2) | |
| Gender | ||||
| Female | 6573 (53.1) | 6355 (53.6) | 218 (42.3) | |
| Male | 5807 (46.9) | 5510 (46.4) | 297 (57.7) | <0.001 |
| Age (mean± SD) | 60.4 ± 17.1 | 60.3 ± 17.1 | 63.8 ± 15.3 | <0.001 |
| <40 years | 1963 (15.9) | 1918 (16.2) | 45 (8.7) | <0.001 |
| 40–59 | 2765 (22.3) | 2650 (22.3) | 115 (22.3) | 0.998 |
| 60–79 | 6346 (51.3) | 6056 (51.0) | 290 (56.3) | 0.019 |
| >80 | 1306 (10.5) | 1241 (10.5) | 65 (12.6) | 0.118 |
| Ward | ||||
| Surgery | 4896 (39.5) | 4675 (39.4) | 221 (42.9) | 0.111 |
| General Medicine | 5565 (45.0) | 5374 (45.3) | 191 (37.1) | <0.001 |
| Intensive care unit | 521 (4.2) | 438 (3.7) | 83 (16.1) | <0.001 |
| Gynecology | 1342 (10.8) | 1326 (11.2) | 16 (3.1) | <0.001 |
| Mix adults | 56 (0.5) | 52 (0.4) | 4 (0.8) | 0.263 |
| McCabe classification | ||||
| Nonfatal | 9714 (78.5) | 9417 (79.4) | 297 (57.7) | <0.001 |
| Fatal within 5 years | 654 (5.3) | 581 (4.9) | 73 (14.2) | <0.001 |
| Fatal within 1 year | 1663 (13.4) | 1532 (12.9) | 131 (25.4) | <0.001 |
| Unknown | 349 (2.8) | 335 (2.8) | 14 (2.7) | 0.888 |
| Extrinsic factors | ||||
| Invasive devices | ||||
| Urinary catheter | 2823 (22.8) | 2521 (21.2) | 302 (58.6) | <0.001 |
| Peripheral venous catheter | 7871 (63.6) | 7454 (62.8) | 417 (81.0) | <0.001 |
| Central venous catheter | 631 (5.1) | 485 (4.1) | 146 (28.3) | <0.001 |
| Mechanical ventilation | 268 (2.2) | 182 (1.5) | 86 (16.7) | <0.001 |
| Exposure to intensive care | 521 (4.2) | 438 (3.7) | 83 (16.1) | <0.001 |
| Prior antibiotics therapy | 5242 (42.3) | 4739 (39.9) | 503 (97.7) | <0.001 |
| Hospital size | ||||
| Small (<360 beds) | 2909 (23.5) | 2801 (23.6) | 108 (21.0) | 0.167 |
| Medium (360–574) | 3289 (26.6) | 3180 (26.8) | 109 (21.2) | 0.005 |
| Large (575–1100) | 2928 (23.7) | 2838 (23.9) | 90 (17.5) | 0.001 |
| Very large (>1100) | 3254 (26.3) | 3046 (25.7) | 208 (40.4) | <0.001 |
| SSI | PN | UTI | GI | BSI | EENT | SST | Other | Total | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | n | % | n | % | n | % | n | % | n | % | n | % | |
| Gram-positive cocci | 66 | 31.4 | 7 | 5.2 | 26 | 16.0 | 0 | 0.0 | 36 | 37.9 | 2 | 40.0 | 6 | 16.7 | 1 | 5.9 | 144 | 19.9 |
| Gram-positive bacilli | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 2 | 2.1 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 2 | 0.3 |
| Enterobacterales | 93 | 44.3 | 62 | 46.3 | 115 | 70.6 | 0 | 0.0 | 42 | 44.2 | 0 | 0.0 | 19 | 52.8 | 9 | 52.9 | 340 | 47.1 |
| Non-fermenting Gram-negative bacilli | 50 | 23.8 | 49 | 36.6 | 13 | 8.0 | 0 | 0.0 | 12 | 12.6 | 0 | 0.0 | 10 | 27.8 | 4 | 23.5 | 138 | 19.1 |
| Anaerobes | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 62 | 89.9 | 1 | 1.1 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 63 | 8.7 |
| Fungi | 1 | 0.5 | 1 | 0.7 | 1 | 0.6 | 0 | 0.0 | 1 | 1.1 | 0 | 0.0 | 0 | 0.0 | 1 | 5.9 | 5 | 0.7 |
| Microorganism not identified or not found | 0 | 0.0 | 15 | 11.2 | 7 | 4.3 | 0 | 0.0 | 1 | 1.1 | 1 | 20.0 | 1 | 2.8 | 2 | 11.8 | 27 | 3.7 |
| Sterile examination | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 2 | 2.9 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 2 | 0.3 |
| Result not available or missing | 0 | 0.0 | 0 | 0.0 | 1 | 0.6 | 5 | 7.2 | 0 | 0.0 | 2 | 40.0 | 0 | 0.0 | 0 | 0.0 | 1 | 0.1 |
| Total | 210 | 100 | 134 | 100 | 163 | 100 | 69 | 100 | 95 | 100.0 | 5 | 100 | 36 | 100 | 17 | 10 | 722 | 100 |
| Antibiotic | Non-Fermenting Gram-Negative Bacilli | Enterobacterales | Gram-Positive Cocci | Total | |
|---|---|---|---|---|---|
| Resistant/tested (%) | Resistant/tested (%) | Resistant/tested (%) | Resistant/tested (%) | ||
| Staphylococcus spp. | Enterococcus spp. | ||||
| CAR | 103/128 (80.5%) | 50/139 (35.9%) | N/A | 158/282 (56.0%) | |
| C3G | N/A | 95/151 (62.9%) | N/A | 105/168 (62.5%) | |
| OXA | N/A | N/A | 11/31 (35.5%) | 0/1 (0%) | 11/32 (34.4%) |
| GLY | N/A | N/A | 0/27 (0%) | 13/45 (28.9%) | 13/72 (18.1%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ćirković, I.; Marković-Denić, L.; Bajčetić, M.; Dragovac, G.; Đorđević, Z.; Mioljević, V.; Urošević, D.; Nikolić, V.; Despotović, A.; Krtinić, G.; et al. Microbiology of Healthcare-Associated Infections: Results of a Fourth National Point Prevalence Survey in Serbia. Antibiotics 2022, 11, 1161. https://doi.org/10.3390/antibiotics11091161
Ćirković I, Marković-Denić L, Bajčetić M, Dragovac G, Đorđević Z, Mioljević V, Urošević D, Nikolić V, Despotović A, Krtinić G, et al. Microbiology of Healthcare-Associated Infections: Results of a Fourth National Point Prevalence Survey in Serbia. Antibiotics. 2022; 11(9):1161. https://doi.org/10.3390/antibiotics11091161
Chicago/Turabian StyleĆirković, Ivana, Ljiljana Marković-Denić, Milica Bajčetić, Gorana Dragovac, Zorana Đorđević, Vesna Mioljević, Danijela Urošević, Vladimir Nikolić, Aleksa Despotović, Gordana Krtinić, and et al. 2022. "Microbiology of Healthcare-Associated Infections: Results of a Fourth National Point Prevalence Survey in Serbia" Antibiotics 11, no. 9: 1161. https://doi.org/10.3390/antibiotics11091161