
Antimicrobial Utilization among Neonates and Children: A Multicenter Point Prevalence Study from Leading Children’s Hospitals in Punjab, Pakistan

 ,
,  ,
,  ,
, 
Abstract
:1. Introduction
2. Results
2.1. Hospital, Ward, Patient, and Antibiotics Prevalence Related Information
2.2. Prevalence of Prescribed Antimicrobials According to Age Groups
2.3. Antibiotic Resistance Pattern of Identified Bacterial Species
2.4. Indications for Prescribed Antibiotics
2.5. Indications for Prescribed Antibiotics According to Age Groups
2.6. Details of Prescribed Antibiotics According to ATC Classification
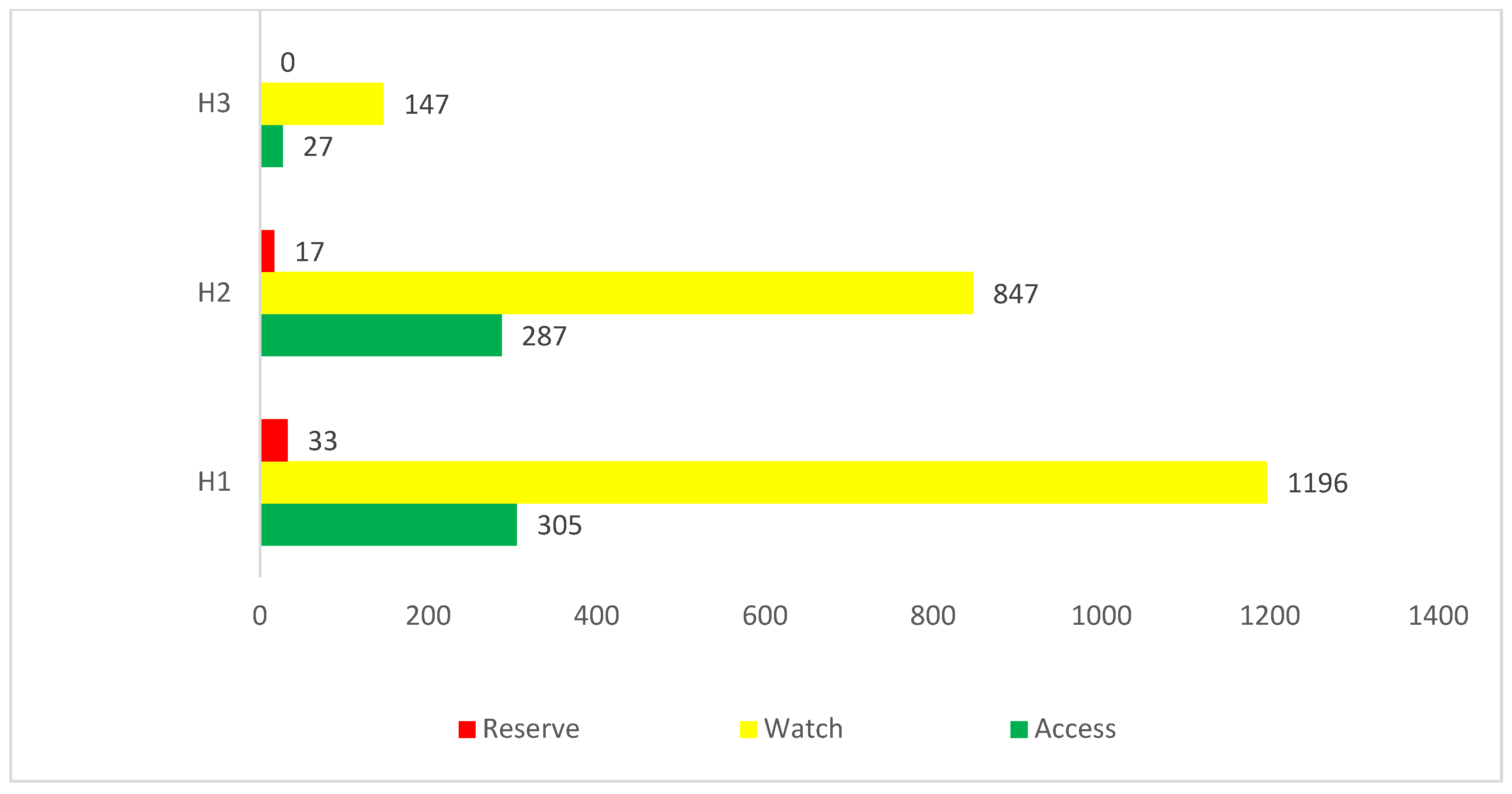
2.7. Detail of Prescribed Antibiotics According to WHO AwaRe Classification
3. Discussion
Strengths and Limitations
4. Materials and Methods
4.1. Study Design
4.2. Study Time and Settings
4.3. Data Collection Procedure
- Section I
- Section II
- Section III
4.4. Inclusion and Exclusion Criteria
4.5. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization (WHO). Antibiotic Resistance. Available online: https://www.who.int/news-room/fact-sheets/detail/antibiotic-resistance (accessed on 10 June 2022).
- World Health Organization (WHO). Antimicrobial Resistance. Available online: https://www.who.int/news-room/fact-sheets/detail/antimicrobial-resistance (accessed on 10 June 2022).
- Hofer, U. The cost of antimicrobial resistance. Nat. Rev. Microbiol. 2019, 17, 3. [Google Scholar] [CrossRef]
- Cassini, A.; Högberg, L.D.; Plachouras, D.; Quattrocchi, A.; Hoxha, A.; Simonsen, G.S.; Colomb-Cotinat, M.; Kretzschmar, M.E.; Devleesschauwer, B.; Cecchini, M.; et al. Attributable deaths and disability-adjusted life-years caused by infections with antibiotic-resistant bacteria in the EU and the European Economic Area in 2015: A population-level modelling analysis. Lancet Infect. Dis. 2019, 19, 56–66. [Google Scholar] [CrossRef] [Green Version]
- Murray, C.J.; Ikuta, K.S.; Sharara, F.; Swetschinski, L.; Aguilar, G.R.; Gray, A.; Han, C.; Bisignano, C.; Rao, P.; Wool, E.; et al. Global burden of bacterial antimicrobial resistance in 2019: A systematic analysis. Lancet 2022, 399, 629–655. [Google Scholar] [CrossRef]
- Ayukekbong, J.A.; Ntemgwa, M.; Atabe, A.N. The threat of antimicrobial resistance in developing countries: Causes and control strategies. Antimicrob. Resist. Infect. Control 2017, 6, 1–8. [Google Scholar] [CrossRef]
- Sulis, G.; Sayood, S.; Gandra, S. Antimicrobial resistance in low- and middle-income countries: Current status and future directions. Expert Rev. Anti-Infect. Ther. 2022, 20, 147–160. [Google Scholar] [CrossRef]
- Qamar, F.N.; Yousafzai, M.T.; Dehraj, I.F.; Shakoor, S.; Irfan, S.; Hotwani, A.; Hunzai, M.J.; Thobani, R.S.; Rahman, N.; Mehmood, J.; et al. Antimicrobial Resistance in Typhoidal Salmonella: Surveillance for Enteric Fever in Asia Project, 2016–2019. Clin. Infect. Dis. 2020, 71 (Suppl. 3), S276–S284. [Google Scholar] [CrossRef] [PubMed]
- Akram, J.; Khan, A.S.; Khan, H.A.; Gilani, S.A.; Akram, S.J.; Ahmad, F.; Mehboob, R. Extensively Drug-Resistant (XDR) Typhoid: Evolution, Prevention, and Its Management. BioMed Res. Int. 2020, 2020, 6432580. [Google Scholar] [CrossRef] [PubMed]
- Bilal, H.; Khan, M.N.; Rehman, T.; Hameed, M.F.; Yang, X. Antibiotic resistance in Pakistan: A systematic review of past decade. BMC Infect. Dis. 2021, 21, 244. [Google Scholar] [CrossRef]
- Saeed, D.K.; Farooqi, J.; Shakoor, S.; Hasan, R. Antimicrobial resistance among GLASS priority pathogens from Pakistan: 2006–2018. BMC Infect. Dis. 2021, 21, 1231. [Google Scholar] [CrossRef]
- Woll, C.; Neuman, M.I.; Pruitt, C.; Wang, M.E.; Shapiro, E.D.; Shah, S.S.; McCulloh, R.; Nigrovic, L.E.; Desai, S.; DePorre, A.G.; et al. Epidemiology and Etiology of Invasive Bacterial Infection in Infants ≤60 Days Old Treated in Emergency Departments. J. Pediatr. 2018, 200, 210–217. [Google Scholar] [CrossRef]
- Baig, M.T.; Sial, A.A.; Huma, A.; Ahmed, M.; Shahid, U.; Syed, N. Irrational antibiotic prescribing practice among children in critical care of tertiary hospitals. Pak. J. Pharm. Sci. 2017, 30, 1483–1489. [Google Scholar]
- Atif, M.; Zia, R.; Malik, I.; Ahmad, N.; Sarwar, S. Treatment outcomes, antibiotic use and its resistance pattern among neonatal sepsis patients attending Bahawal Victoria Hospital, Pakistan. PLoS ONE 2021, 16, e0244866. [Google Scholar] [CrossRef] [PubMed]
- Youngster, I.; Avorn, J.; Belleudi, V.; Cantarutti, A.; Diez-Domingo, J.; Kirchmayer, U.; Park, B.-J.; Peiró, S.; Sanfélix-Gimeno, G.; Schröder, H.; et al. Antibiotic Use in Children—A Cross-National Analysis of 6 Countries. J. Pediatr. 2017, 182, 239–244. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Fight Antimicrobial Resistance: Protect Mothers and Newborns. Available online: https://www.who.int/drugresistance/activities/Women-Deliver-AMR-side-event-Handout-May2016.pdf?ua=1 (accessed on 10 June 2022).
- Mustafa, Z.U.; Salman, M.; Yasir, M.; Godman, B.; Majeed, H.A.; Kanwal, M.; Iqbal, M.; Riaz, M.B.; Hayat, K.; Hasan, S.S. Antibiotic consumption among hospitalized neonates and children in Punjab province, Pakistan. Expert Rev. Anti-Infect. Ther. 2021, 20, 931–939. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Global Action Plan on Antimicrobial Resistance. Available online: https://www.who.int/publications/i/item/9789241509763 (accessed on 11 June 2022).
- Antimicrobial Resistance. National Action Plan Pakistan. Available online: https://www.nih.org.pk/wp-content/uploads/2018/08/AMR-National-Action-Plan-Pakistan.pdf (accessed on 11 June 2022).
- World Health Organization (WHO). Essential Medicines and Health Products. WHO Methodology for Point Prevalence Survey on Antibiotic Use in Hospitals. 2018. Available online: https://www.who.int/medicines/access/antimicrobial_resistance/WHO-EMP-IAU-2018_01/en/ (accessed on 11 June 2022).
- Versporten, A.; Zarb, P.; Caniaux, I.; Gros, M.-F.; Drapier, N.; Miller, M.; Jarlier, V.; Nathwani, D.; Goossens, H.; Koraqi, A.; et al. Antimicrobial consumption and resistance in adult hospital inpatients in 53 countries: Results of an internet-based global point prevalence survey. Lancet Glob. 2018, 6, e619–e629. [Google Scholar] [CrossRef] [Green Version]
- Saleem, Z.; Hassali, M.A.; Godman, B.; Versporten, A.; Hashmi, F.K.; Saeed, H.; Saleem, F.; Salman, M.; Rehman, I.U.; Khan, T.M. Point prevalence surveys of antimicrobial use: A systematic review and the implications. Expert Rev. Anti-Infect. Ther. 2020, 18, 897–910. [Google Scholar] [CrossRef]
- Sharland, M.; Pulcini, C.; Harbarth, S.; Zeng, M.; Gandra, S.; Mathur, S.; Magrini, N. Classifying antibiotics in the WHO Essential Medicines List for optimal use—be AWaRe. Lancet Infect. Dis. 2018, 18, 18–20. [Google Scholar] [CrossRef] [Green Version]
- Sharland, M.; Gandra, S.; Huttner, B.; Moja, L.; Pulcini, C.; Zeng, M.; Mendelson, M.; Cappello, B.; Cooke, G.; Magrini, N.; et al. Encouraging AWaRe-ness and discouraging inappropriate antibiotic use—The new 2019 Essential Medicines List becomes a global antibiotic stewardship tool. Lancet Infect. Dis. 2019, 19, 1278–1280. [Google Scholar] [CrossRef]
- Hsia, Y.; Lee, B.R.; Versporten, A.; Yang, Y.; Bielicki, J.; Jackson, C.; Newland, J.; Goossens, H.; Magrini, N.; Sharland, M.; et al. Use of the WHO Access, Watch, and Reserve classification to define patterns of hospital antibiotic use (AWaRe): An analysis of paediatric survey data from 56 countries. Lancet Glob. Health 2019, 7, e861–e871. [Google Scholar] [CrossRef] [Green Version]
- WHO Access, Watch, Reserve, Classification of Antibiotics for Evaluation and Monitoring of Use. Available online: https://www.who.int/publications/i/item/2021-aware-classification (accessed on 11 June 2022).
- Situation Analysis Report on Antimicrobial Resistance in Pakistan. Findings and Recommendations on Antibiotic Use and Resistance. Available online: https://cddep.org/wp-content/uploads/2018/03/Situational-Analysis-Report-on-Antimicrobial-Resistance-in-Pakistan.pdf (accessed on 11 June 2022).
- Saleem, Z.; Godman, B.; Azhar, F.; Kalungia, A.C.; Fadare, J.; Opanga, S.; Markovic-Pekovic, V.; Hoxha, I.; Saeed, A.; Al-Gethamy, M.; et al. Progress on the national action plan of Pakistan on antimicrobial resistance (AMR): A narrative review and the implications. Expert Rev. Anti-Infect. Ther. 2022, 20, 71–93. [Google Scholar] [CrossRef]
- Saleem, Z.; Hassali, M.A.; Hashmi, F.K. Pakistan’s national action plan for antimicrobial resistance: Translating ideas into reality. Lancet Infect. Dis. 2018, 18, 1066–1067. [Google Scholar] [CrossRef]
- Mustafa, Z.U.; Salman, M.; Aslam, N.; Asif, N.; Hussain, K.; Shehzadi, N.; Hayat, K. Antibiotic use among hospitalized children with lower respiratory tract infections: A multicenter, retrospective study from Punjab, Pakistan. Expert Rev. Anti-Infect. Ther. 2022, 20, 131–136. [Google Scholar] [CrossRef] [PubMed]
- Saleem, Z.; Hassali, M.A.; Versporten, A.; Godman, B.; Hashmi, F.K.; Goossens, H.; Saleem, F. A multicenter point prevalence survey of antibiotic use in Punjab, Pakistan: Findings and implications. Expert Rev. Anti-Infect. Ther. 2019, 17, 285–293. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saleem, Z.; Hassali, M.A.; Godman, B.; Hashmi, F.K.; Saleem, F. A multicenter point prevalence survey of healthcare–associated infections in Pakistan: Findings and implications. Am. J. Infect. Control 2019, 47, 421–424. [Google Scholar] [CrossRef] [Green Version]
- Mustafa, Z.U.; Saleem, M.S.; Ikram, M.N.; Salman, M.; Butt, S.A.; Khan, S.; Godman, B.; Seaton, R.A. Co-infections and antimicrobial use among hospitalized COVID-19 patients in Punjab, Pakistan: Findings from a multicenter, point prevalence survey. Pathog. Glob. Health 2021, 1–7. [Google Scholar] [CrossRef]
- Arif, S.; Sadeeqa, S.; Saleem, Z. Patterns of Antimicrobial Use in Hospitalized Children: A Repeated Point Prevalence Survey from Pakistan. J. Pediatr. Infect. Dis. Soc. 2021, 10, 970–974. [Google Scholar] [CrossRef]
- Wang, C.-N.; Tong, J.; Yi, B.; Huttner, B.D.; Cheng, Y.; Li, S.; Wan, C.; Zhu, Q.; Zhou, Q.; Zhao, S.; et al. Antibiotic Use among Hospitalized Children and Neonates in China: Results from Quarterly Point Prevalence Surveys in 2019. Front. Pharmacol. 2021, 12, 601561. [Google Scholar] [CrossRef]
- Skosana, P.; Schellack, N.; Godman, B.; Kurdi, A.; Bennie, M.; Kruger, D.; Meyer, J. A national, multicentre, web-based point prevalence survey of antimicrobial use and quality indices among hospitalised paediatric patients across South Africa. J. Glob. Antimicrob. Resist. 2021, 29, 542–550. [Google Scholar] [CrossRef]
- Gandra, S.; Singh, S.K.; Jinka, D.R.; Kanithi, R.; Chikkappa, A.K.; Sharma, A.; Dharmapalan, D.; Vasudevan, A.K.; Tunga, O.; Akula, A.; et al. Point Prevalence Surveys of Antimicrobial Use among Hospitalized Children in Six Hospitals in India in 2016. Antibiotics 2017, 6, 19. [Google Scholar] [CrossRef]
- Prusakov, P.; Goff, D.A.; Wozniak, P.S.; Cassim, A.; Scipion, C.E.; Urzúa, S.; Ronchi, A.; Zeng, L.; Ladipo-Ajayi, O.; Aviles-Otero, N.; et al. A global point prevalence survey of antimicrobial use in neonatal intensive care units: The no-more-antibiotics and resistance (NO-MAS-R) study. eClinicalMedicine 2021, 32, 100727. [Google Scholar] [CrossRef] [PubMed]
- Cyriac, J.M.; James, E. Switch over from intravenous to oral therapy: A concise overview. J. Pharmacol. Pharmacother. 2014, 5, 83–87. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shrayteh, Z.M.; Rahal, M.K.; Malaeb, D.N. Practice of switch from intravenous to oral antibiotics. SpringerPlus 2014, 3, 717. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gasparetto, J.; Tuon, F.F.; Oliveira, D.D.S.; Zequinao, T.; Pipolo, G.R.; Ribeiro, G.V.; Benincá, P.D.; Cruz, J.A.W.; Moraes, T.P. Intravenous-to-oral antibiotic switch therapy: A cross-sectional study in critical care units. BMC Infect. Dis. 2019, 19, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Nathwani, D.; Lawson, W.; Dryden, M.; Stephens, J.; Corman, S.; Solem, C.; Li, J.; Charbonneau, C.; Baillon-Plot, N.; Haider, S.; et al. Implementing criteria-based early switch/early discharge programmes: A European perspective. Clin. Microbiol. Infect. 2015, 21, S47–S55. [Google Scholar] [CrossRef] [Green Version]
- Smith, M.J.; Thurm, C.; Shah, S.S.; Patel, S.J.; Kronman, M.P.; Gerber, J.S.; Courter, J.D.; Lee, B.R.; Newland, J.G.; Hersh, A.L. Route of administration for antibiotics with high oral bioavailability. Infect. Control Hosp. 2019, 40, 248–249. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Versporten, A.; Bielicki, J.; Drapier, N.; Sharland, M.; Goossens, H.; ARPEC Project Group; Calle, G.M.; Garrahan, J.P.; Clark, J.; Cooper, C.; et al. The Worldwide Antibiotic Resistance and Prescribing in European Children (ARPEC) point prevalence survey: Developing hospital-quality indicators of antibiotic prescribing for children. J. Antimicrob. Chemother. 2016, 71, 1106–1117. [Google Scholar] [CrossRef] [Green Version]
- Zhang, J.-S.; Liu, G.; Zhang, W.-S.; Shi, H.-Y.; Lu, G.; Zhao, C.-A.; Li, C.-C.; Li, Y.-Q.; Shao, Y.-N.; Tian, D.-Y.; et al. Antibiotic usage in Chinese children: A point prevalence survey. World J. Pediatr. 2018, 14, 335–343. [Google Scholar] [CrossRef]
- Ceyhan, M.; Yildirim, I.; Ecevit, C.; Aydogan, A.; Ornek, A.; Salman, N.; Somer, A.; Hatipoğlu, N.; Camcioglu, Y.; Alhan, E.; et al. Inappropriate antimicrobial use in Turkish pediatric hospitals: A multicenter point prevalence survey. Int. J. Infect. Dis. 2010, 14, e55–e61. [Google Scholar] [CrossRef] [Green Version]
- Mwita, J.C.; Ogunleye, O.; Olalekan, A.; Kalungia, A.C.; Kurdi, A.; Saleem, Z.; Sneddon, J.; Godman, B. Key Issues Surrounding Appropriate Antibiotic Use for Prevention of Surgical Site Infections in Low- and Middle-Income Countries: A Narrative Review and the Implications. Int. J. Gen. Med. 2021, 14, 515. [Google Scholar] [CrossRef]
- Sviestina, I.; Mozgis, D. Antimicrobial usage among hospitalized children in Latvia: A neonatal and pediatric antimicrobial point prevalence survey. Medicina 2014, 50, 175–181. [Google Scholar] [CrossRef]
- Osowicki, J.; Gwee, A.; Noronha, J.; Palasanthiran, P.; McMullan, B.; Britton, P.N.; Isaacs, D.; Lai, T.; Nourse, C.; Avent, M.; et al. Australia-wide point prevalence survey of the use and appropriateness of antimicrobial prescribing for children in hospital. Med. J. Aust. 2014, 201, 657–662. [Google Scholar] [CrossRef] [PubMed]
- Chowdhury, K.; Haque, M.; Nusrat, N.; Adnan, N.; Islam, S.; Lutfor, A.B.; Begum, D.; Rabbany, A.; Karim, E.; Malek, A.; et al. Management of Children Admitted to Hospitals across Bangladesh with Suspected or Confirmed COVID-19 and the Implications for the Future: A Nationwide Cross-Sectional Study. Antibiotics 2022, 11, 105. [Google Scholar] [CrossRef] [PubMed]
- Ho, T.; Buus-Frank, M.E.; Edwards, E.M.; Morrow, K.A.; Ferrelli, K.; Srinivasan, A.; Pollock, D.A.; Dukhovny, D.; Zupancic, J.A.; Pursley, D.M.; et al. Adherence of Newborn-Specific Antibiotic Stewardship Programs to CDC Recommendations. Pediatrics 2018, 142, e20174322. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Afriyie, D.K.; Sefah, I.A.; Sneddon, J.; Malcolm, W.; McKinney, R.; Cooper, L.; Kurdi, A.; Godman, B.; Seaton, R.A. Antimicrobial point prevalence surveys in two Ghanaian hospitals: Opportunities for antimicrobial stewardship. JAC-Antimicrob. Resist. 2020, 2, dlaa001. [Google Scholar] [CrossRef] [Green Version]
- D’Amore, C.; degli Atti, M.L.C.; Zotti, C.; Prato, R.; Guareschi, G.; Spiazzi, R.; Petitti, G.; Moro, M.L.; Raponi, M. Use of multiple metrics to assess antibiotic use in Italian children’s hospitals. Sci. Rep. 2021, 11, 3543. [Google Scholar] [CrossRef]
- Oo, W.T.; Carr, S.D.; Marchello, C.S.; San, M.M.; Oo, A.T.; Oo, K.M.; Lwin, K.T.; Win, H.H.; Crump, J.A. Point-prevalence surveys of antimicrobial consumption and resistance at a paediatric and an adult tertiary referral hospital in Yangon, Myanmar. Infect. Prev. Pract. 2021, 4, 100197. [Google Scholar] [CrossRef]
- Mustafa, Z.U.; Salman, M.; Rao, A.Z.; Asif, N.; Butt, S.A.; Shehzadi, N.; Hussain, K. Assessment of antibiotics use for children upper respiratory tract infections: A retrospective, cross-sectional study from Pakistan. Infect. Dis. 2020, 52, 473–478. [Google Scholar] [CrossRef]
- Nebot, S.S.; López-Ramos, M.G.; Velasco-Arnaiz, E.; Jordan, I.; Fortuny, C.; Noguera-Julian, A. Impact and quality of antimicrobial use in a referral pediatric intensive care unit. Enferm. Infect. Microbiol. Clín. 2022, 40, 78–81. [Google Scholar] [CrossRef]
- Hsia, Y.; Sharland, M.; Jackson, C.; Wong, I.C.K.; Magrini, N.; Bielicki, J.A. Consumption of oral antibiotic formulations for young children according to the WHO Access, Watch, Reserve (AWaRe) antibiotic groups: An analysis of sales data from 70 middle-income and high-income countries. Lancet Infect. Dis. 2019, 19, 67–75. [Google Scholar] [CrossRef]
- Blackburn, J.; Barrowman, N.; Bowes, J.; Tsampalieros, A.; Le Saux, N. Establishing Benchmarks for Antimicrobial Use in Canadian Children’s Hospitals: Results From 2 National Point Prevalence Surveys. Pediatr. Infect. Dis. J. 2021, 40, 899–905. [Google Scholar] [CrossRef]
- European Centre for Disease Prevention and Control (ECDC). Point Prevalence Survey of Healthcare-Associated Infections and Antimicrobial Use in European Acute Care Hospitals. 2012. Available online: http://ecdc.europa.eu/en/publications/Publications/PPS-HAI-antimicrobial-use-EU-acute-carehospitals-V5-3.pdf (accessed on 11 June 2022).
- WHO Collaborating Centre for Drug Statistics Methodology. ATC/DDD Index. Available online: https://www.whocc.no/ (accessed on 11 June 2022).


{kind=link}
| Variables N (%) | H1 | H2 | H3 | Total N (%) |
|---|---|---|---|---|
| Total bed in hospital | 1050 | 570 | 250 | 1870 |
| Total bed in children ward | 1010 | 510 | 170 | 1690 |
| Total patients in children ward at 8:00 AM | 987 | 464 | 125 | 1576 (93.2) |
| Total No. of patients prescribed antibiotics and % | 936 (94.8) | 461 (99.4%) | 109 (87.2%) | 1506 (95.5) |
| Age (Number and %) | ||||
| Neonates (0–28 days) | 136 (14.5) | 142 (30.8) | 8 (7.3) | 286 (19.0) |
| Infants (29 days–1 year) | 337 (36.0) | 83 (18.0) | 42 (38.5) | 462 (30.7) |
| Young child (˃1–5 years) | 252 (26.9) | 113 (24.5) | 26 (23.8) | 391 (25.9) |
| Child (˃5–12 years) | 211 (22.6) | 123 (26.6) | 33 (30.3) | 367 (24.3) |
| Total no. of prescribed antibiotics and per patient | 1534 (1.64) | 1151 (2.50) | 174 (1.60) | 2859 (1.90) |
| No. (and %) of Antibiotics per patient | ||||
| One antibiotic | 354 (23.0) | 156 (13.5) | 51 (29.3) | 561 (19.6) |
| Two antibiotics | 1032 (67.3) | 572 (49.7) | 108 (62.0) | 1712 (59.9) |
| Three antibiotics or above | 148 (9.7) | 423 (36.8) | 15 (8.7) | 586 (20.4) |
| Other anti-infective agents | ||||
| Antiviral | 52 (32.0) | 23 (53.5) | 03 (60.0) | 78 (2.5) |
| Antifungal | 79 (48.8) | 04 (9.3) | 01 (20.0) | 84 (2.7) |
| Antiprotozoal | 31 (19.2) | 16 (37.2) | 01 (20.0) | 48 (1.5) |
| Gender | ||||
| Male | 526 (56.2) | 174 (37.8) | 64 (58.7) | 764 (50.7) |
| Female | 410 (43.8) | 287 (62.2) | 45 (41.3) | 742 (49.3) |
| Route of administration | ||||
| Oral | 164 (10.7) | 45 (4.0) | 13 (7.5) | 222 (7.7) |
| Parenteral | 1370 (89.3) | 1106 (96.0) | 161 ((92.5) | 2637 (92.3) |
| Sub-specialty | ||||
| Medical | 1267 (82.6) | 752 (65.3) | 126 (72.4) | 2145 (75.0) |
| Surgical | 175 (11.4) | 156 (13.6) | 36 (20.6) | 367 (12.8) |
| ICU | 92 (5.9) | 243 (21.1) | 12 (6.9) | 347 (12.2) |
| Indications | ||||
| Therapeutic use | 962 (62.7) | 571 (49.6) | 94 (54.0) | 1627 (56.9) |
| Prophylaxis use | 356 (23.2) | 468 (40.6) | 63 (36.2) | 887 (31.0) |
| Unknown | 216 (14.1) | 112 (9.8) | 17 (9.8) | 345 12.1) |
| Indications for prophylaxis | ||||
| Medical | 257 (72.2) | 327 (69.9) | 36 (57.1) | 620 (69.9) |
| Surgical | 99 (27.8) | 141 (30.1) | 27 (42.9) | 267 (31.1) |
| Surgical prophylaxis | ||||
| Single dose | 31 (31.3) | 0 | 0 | 31 (11.6) |
| One day | 17 (17.2) | 07 (4.9) | 04 (14.8) | 28 (10.4) |
| More than one day | 51 (51.5) | 134 (95.0) | 23 (85.2) | 208 (77.9) |
| Indication of infection | ||||
| Community acquired | 1457 (94.9) | 1113 (96.7) | 152 (87.3) | 2722 (95.2) |
| Hospital acquired | 77 (5.0) | 38 (3.3) | 22 (12.7) | 137 (4.8) |
| Reasons on notes | ||||
| No | 1387 (90.4) | 1097 (95.3) | 171 (98.2) | 2655 (92.9) |
| Yes | 147 (9.6) | 54 (4.7) | 03 (1.7) | 204 (7.1) |
| Stop date | ||||
| Yes | 573 (37.3) | 237 (20.6) | 41 (23.5) | 851 (29.7) |
| No | 961 (62.7) | 914 (79.4) | 133 (76.4) | 2008 (70.3) |
| Types of therapy | ||||
| Empirical therapy | 1480 (96.5) | 1118 (97.1) | 165 (94.8) | 2763 (96.6) |
| Targeted therapy | 54 (3.5) | 33 (2.9) | 09 (5.1) | 96 (3.4) |
| Variables N (%) | Neonates | Infants | Young Child | Child |
|---|---|---|---|---|
| No. of Antibiotics and per patient prescribed antibiotics | 569 (1.99) | 852 (1.84) | 771 (1.97) | 667 (1.82) |
| Sub-specialty (number and %) | ||||
| Medical | 436 (76.6) | 678 (79.6) | 565 (73.3) | 466 (69.8) |
| Surgical | 5 (0.9) | 68 (8.0) | 136 (17.6) | 158 (23.7) |
| ICU | 128 (22.5) | 106 (12.4) | 70(9.0) | 43 (6.4) |
| Indications for use | ||||
| Therapeutic use | 409 (71.9) | 612 (71.8) | 406 (52.6) | 200 (30.0) |
| Prophylaxis use | 118 (20.7) | 178 (20.9) | 281 (36.4) | 310 (46.5) |
| Unknown | 42 (7.4) | 62 (7.2) | 84 (10.9) | 157 (23.5) |
| Indications for prophylaxis | ||||
| Medical | 113 (95.7) | 130 (73.0) | 185 (65.9) | 192 (61.9) |
| Surgical | 5 (4.2) | 48 (27.0) | 96 (34.1) | 118 (38.0) |
| Surgical prophylaxis | ||||
| Single dose | 1 (20.0) | 7 (14.6) | 14 (14.6) | 09 (7.6) |
| One day | 1 (20.0) | 08 (16.7) | 16 (16.6) | 03 (2.5) |
| More one day | 3 (60.0) | 33 (3368.7) | 66 (68.8) | 106 (89.8) |
| Indication of infection | ||||
| Community acquired | 560 (98.4) | 826 (97.0) | 734 (95.2) | 602 (90.2) |
| Hospital acquired | 09 (1.6) | 26 (3.0) | 37 (4.8) | 65 (9.8) |
| Reasons on notes | ||||
| No | 508 (89.3) | 824 (96.7) | 718 (93.1) | 605 (90.7) |
| Yes | 61 (10.7) | 28 (3.3) | 53 (6.9) | 62 (9.3) |
| Stop date | ||||
| Yes | 213 (37.4) | 191 (22.4) | 153 (19.9) | 294 (44.0) |
| No | 356 (62.6) | 661 (77.6) | 618 (80.1) | 373 (56.0) |
| Types of therapy | ||||
| Empirical therapy | 556 (97.7) | 811 (95.1) | 744 (96.5) | 652 (97.7) |
| Targeted therapy | 13 (2.3) | 41 (4.8) | 27 (3.5) | 15 (2.2) |
| Common Identified Bacteria | Common Resistant Antibiotics | Common Sensitive Antibiotics | H1 | H2 | H3 | Total N (%) |
|---|---|---|---|---|---|---|
| Staphylococcus species | Ampicillin, amoxicillin, ciprofloxacin, levofloxacin, | Vancomycin, linezolid | 24 | 05 | - | 29 (30.2) |
| Pseudomonas species | Penicillins, 3rd generation cephalosporins, amikacin | Levofloxacin, cefepime | 11 | 10 | - | 21 (21.9) |
| Klebsiella species | 3rd generation cephalosporins such as cefotaxime, ceftriaxone | Cephoperazone + beta-lactamase inhibitor, meropenem, imipenem | 04 | 11 | 05 | 20 (20.9) |
| Escherichia coli | Penicillin, amoxicillin | Carbapenems such as meropenem, imipenem | 11 | - | 04 | 15 (15.7) |
| Shigella species | Ampicillin, amoxicillin | Ceftriaxone, ciprofloxacin | 05 | 05 (5.2) | ||
| Others | - | - | 04 | 02 | - | 06 (6.2) |
| Infection Type | H1 (%) | H2 (%) | H3 (%) | Total N (%) |
|---|---|---|---|---|
| Respiratory tract infections | 346 (66.0) | 147 (28.0) | 31 (5.9) | 524 (34.8) |
| Gastrointestinal infections | 152 (63.9) | 69 (28.9) | 17 (7.1) | 238 (15.8) |
| Prophylaxis for medical problems | 116 (53.7) | 87 (40.2) | 13 (6.0) | 216 (14.3) |
| Prophylaxis for surgical diseases | 96 (62.3) | 42 (27.3) | 16 (10.4) | 154 (10.2) |
| Blood stream infection | 48 (51.6) | 36 (38.7) | 09 (9.6) | 93 (6.1) |
| Skin and soft tissue infections | 57 (63.3) | 27 (30.0) | 06 (6.6) | 90 (6.0) |
| Sepsis | 46 (54.1) | 23 (27.0) | 16 (18.8) | 85 (5.6) |
| Urinary tract infections | 48 (71.6) | 19 (28.3) | 0 | 67 (4.4) |
| Others | 27 (69.2) | 11 (28.2) | 01 (2.5) | 39 (2.6) |
| Variables N (%) | Neonates (%) | Infants (%) | Young Child (%) | Child (%) |
|---|---|---|---|---|
| Respiratory tract infections | 138 (26.3) | 211 (40.2) | 103 (19.6) | 72 (13.7) |
| Gastrointestinal infections | 89 (37.4) | 52 (21.8) | 28 (11.7) | 69 (29.0) |
| Prophylaxis for medical problems | 41 (19.0) | 83 (38.4) | 47 (21.7) | 45 (20.8) |
| Prophylaxis for surgical diseases | 05 (3.2) | 64 (41.5) | 37 (24.0) | 48 (31.1) |
| Blood stream infection | 12 (12.9) | 11 (11.8) | 42 (45.1) | 31 (33.3) |
| Skin and soft tissue infections | 09 (10.0) | 23 (25.5) | 18 (20.0) | 40 (44.4) |
| Sepsis | 37 (43.5) | 14 (60.8) | 23 (27.0) | 11 (12.9) |
| Urinary tract infections | 09 (13.4) | 14 (20.9) | 27 (40.3) | 17 (25.4) |
| Others | 13 (33.3) | 08 (20.5) | 06 (15.4) | 12 (30.7) |
| ATC class | Name of Antibiotics (ATC code) | H1 | H2 | H3 | Total (%) |
|---|---|---|---|---|---|
| Third-generation cephalosporin | Ceftriaxone (J01DD04) | 419 | 277 | 44 | 740 (25.8) |
| Cefotaxime (J01DD01) | 119 | 83 | 28 | 230 (8.0) | |
| Ceftazidime (J01DD02) | 23 | 31 | 13 | 67 (2.3) | |
| Cefixime (J01DD08) | 27 | - | - | 27 (0.9) | |
| Cephoperazone + beta-lactamase inhibitor (salbactam) (J01DD12) | 20 | 73 | 14 | 107 (3.7) | |
| Aminoglycoside | Amikacin (D06AX12) | 13 | 112 | 21 | 264 (9.2) |
| Glycopeptide antibacterials | Vancomycin (J01XA01) | 177 | 46 | 05 | 228 (7.9) |
| Macrolides | Azithromycin (J01FA10) | 53 | 69 | 03 | 125(4.3) |
| Clarithromycin (J01FA09) | 24 | 27 | 07 | 58 (2.0) | |
| Piperacillin and enzyme inhibitor | Piperacillin + enzyme inhibitor (tazobactam) (J01CR05) | 89 | 71 | 11 | 171 (5.9) |
| Aminopenicillins | Ampicillin (J01CA01) | 64 | 82 | 02 | 148 (5.1) |
| Amoxicillin and beta-lactamase inhibitor | Amoxicillin + beta-lactamase inhibitors (clavulanate) (J01CR02) | 74 | 56 | - | 130 (4.5) |
| Carbapenems | Meropenem (J01DH02) | 49 | 57 | 12 | 118 (4.1) |
| Imipenem and cilastatin (J01DH51) | 09 | 04 | - | 13 (0.4) | |
| Fluoroquinolones | Ciprofloxacin (J01MA02) | 63 | 43 | 04 | 110 (3.8) |
| Moxifloxacin (J01MA14) | 14 | 03 | - | 17 (0.5) | |
| Imidazole derivatives | Metronidazole (J01XD01) | 58 | 26 | 02 | 86 (3.0) |
| Fourth-generation cephalosporins | Cefepime (J01DE01) | 53 | 30 | 04 | 87 (3.0) |
| Penicillins with extended spectrum | Amoxicillin (J01CA04) | 13 | 37 | 04 | 54 (1.8) |
| Other antibacterials | Linezolid (J01XX08) | 33 | 17 | - | 50 (1.7) |
| First generation cephalosporins | Cefradine (J01DB09) | 11 | - | - | 11 (0.3) |
| Others | - | 11 | 07 | - | 18 (0.6) |
| AwaRe Category | H1 | H2 | H3 | Total N (%) |
|---|---|---|---|---|
| Access | 305 | 287 | 27 | 619 (21.7) |
| Watch | 1196 | 847 | 147 | 2190 (76.6) |
| Reserve | 33 | 17 | 0 | 50 (1.7) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mustafa, Z.U.; Khan, A.H.; Salman, M.; Syed Sulaiman, S.A.; Godman, B. Antimicrobial Utilization among Neonates and Children: A Multicenter Point Prevalence Study from Leading Children’s Hospitals in Punjab, Pakistan. Antibiotics 2022, 11, 1056. https://doi.org/10.3390/antibiotics11081056
Mustafa ZU, Khan AH, Salman M, Syed Sulaiman SA, Godman B. Antimicrobial Utilization among Neonates and Children: A Multicenter Point Prevalence Study from Leading Children’s Hospitals in Punjab, Pakistan. Antibiotics. 2022; 11(8):1056. https://doi.org/10.3390/antibiotics11081056
Chicago/Turabian StyleMustafa, Zia Ul, Amer Hayat Khan, Muhammad Salman, Syed Azhar Syed Sulaiman, and Brian Godman. 2022. "Antimicrobial Utilization among Neonates and Children: A Multicenter Point Prevalence Study from Leading Children’s Hospitals in Punjab, Pakistan" Antibiotics 11, no. 8: 1056. https://doi.org/10.3390/antibiotics11081056