
Assessment of the Impact of a Meningitis/Encephalitis Panel on Hospital Length of Stay: A Systematic Review and Meta-Analysis

 , , ,
, , ,
Abstract
:1. Introduction
Objective
2. Materials and Methods
2.1. Electronic Search and Inclusion Criteria
2.2. Data Extraction and Meta-Analysis
2.3. Stratification by Age
2.4. Quality Assessment
2.5. Ethics Compliance
3. Results
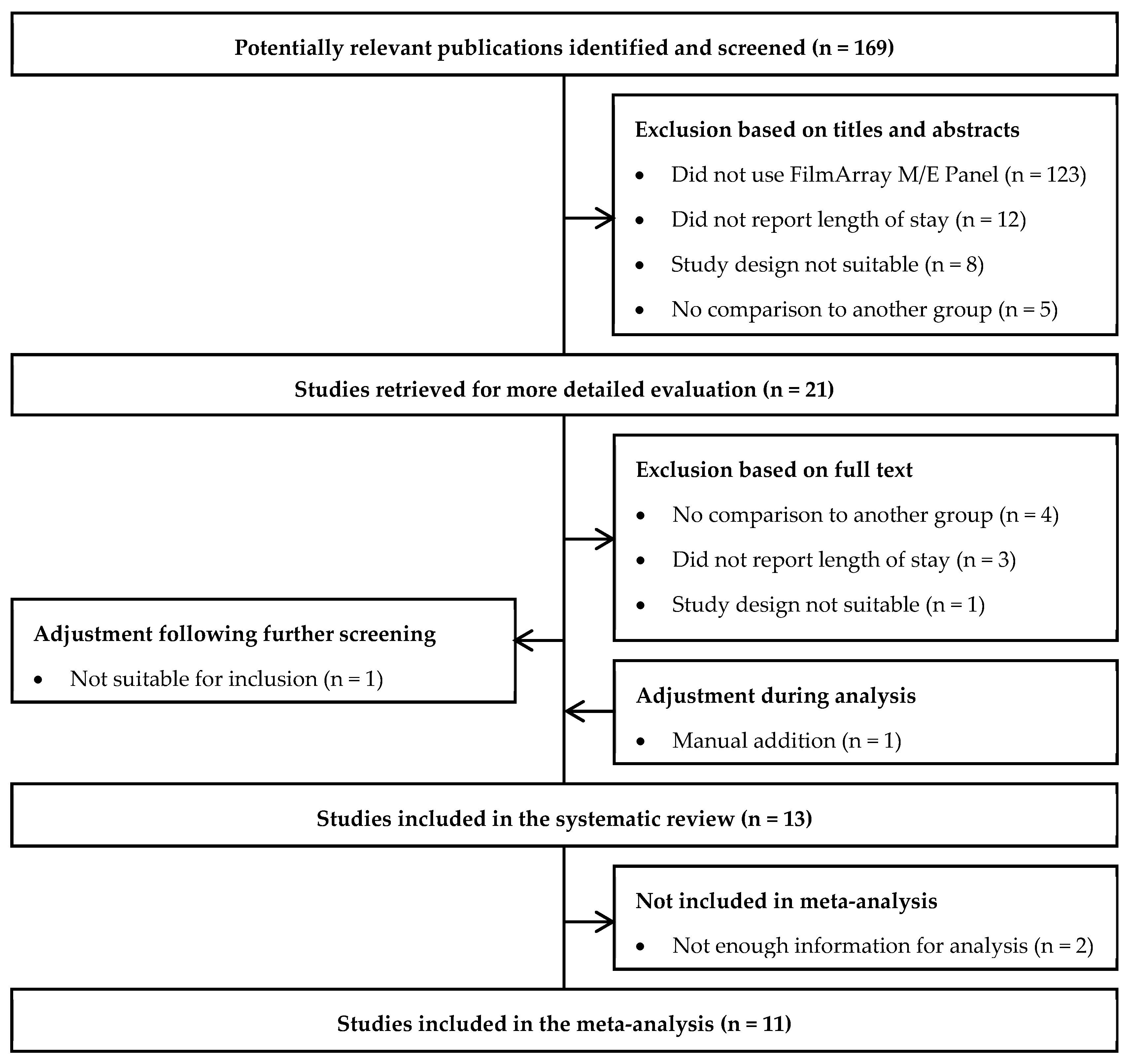
3.1. Study Selection and Characteristics
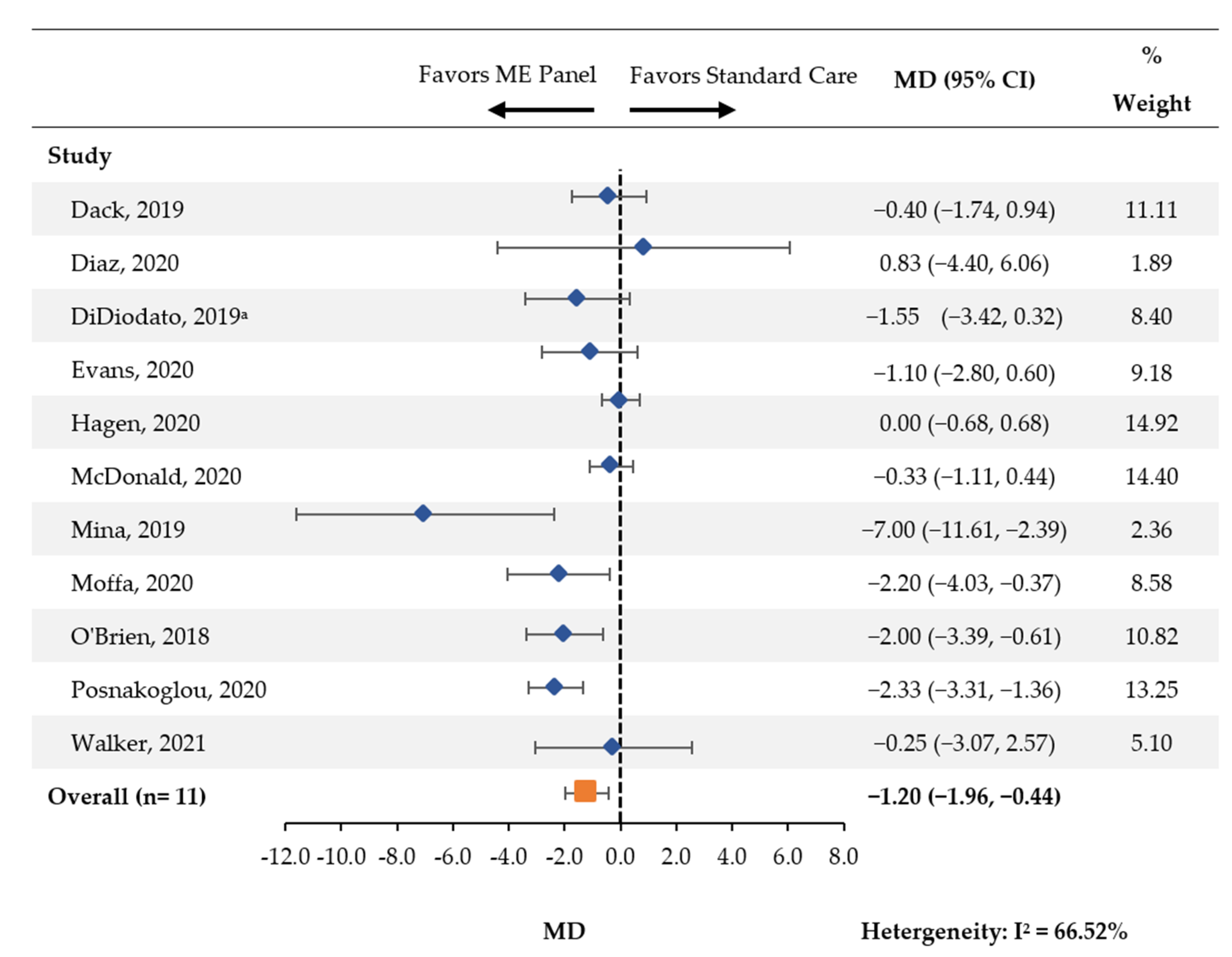
3.2. Length of Hospital Stay
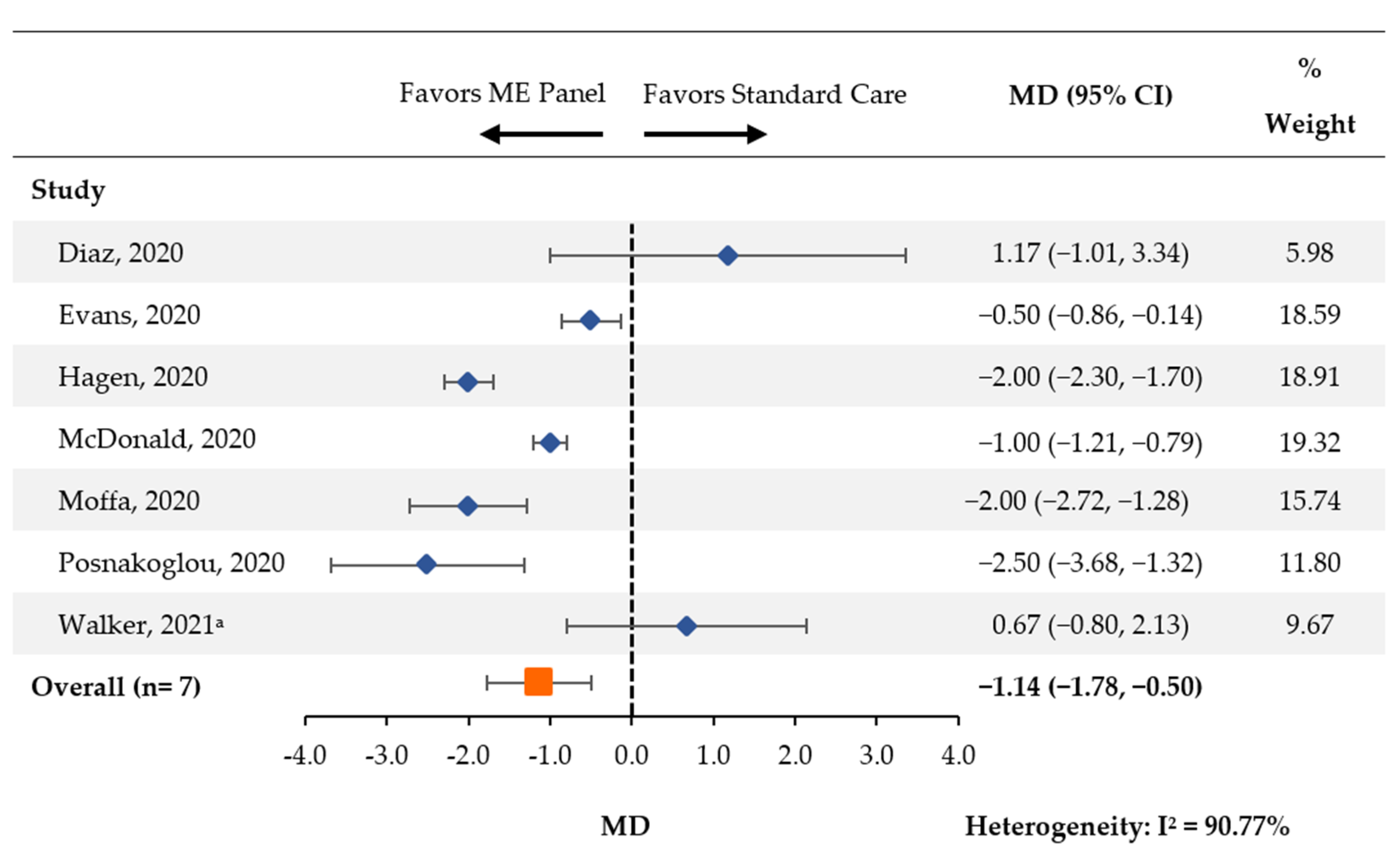
3.3. Length of Acyclovir Therapy
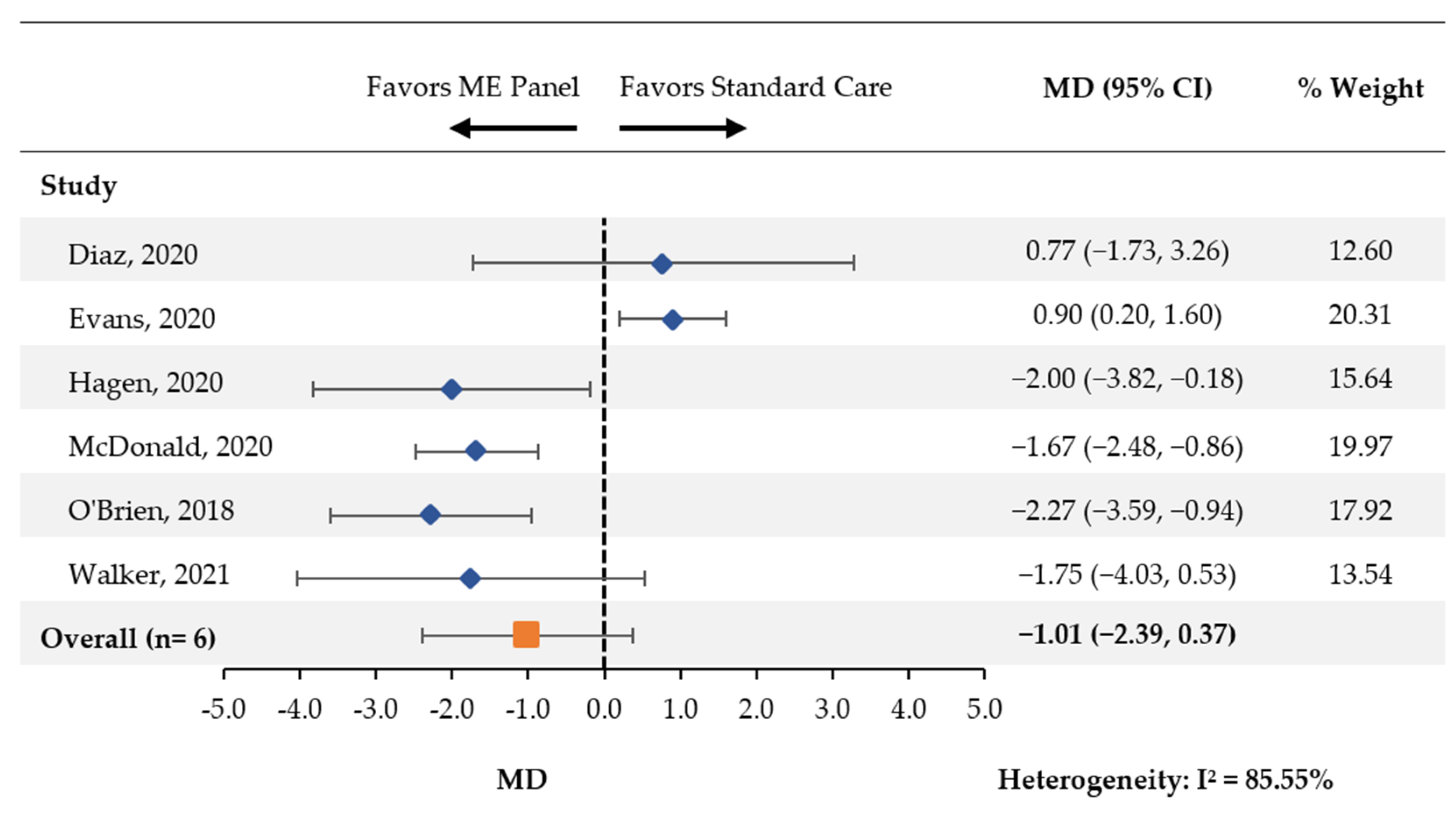
3.4. Days with Antibiotic Therapy
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tansarli, G.S.; Chapin, K.C. Diagnostic test accuracy of the BioFire® FilmArray® meningitis/encephalitis panel: A systematic review and meta-analysis. Clin. Microbiol. Infect. Off. Publ. Eur. Soc. Clin. Microbiol. Infect. Dis. 2020, 26, 281–290. [Google Scholar] [CrossRef] [PubMed]
- Greenlee, J.E. Acute Bacterial Meningitis. Medical Topics & Chapters, Volume 2021. Merck Manual Professional Version, 2020. Available online: https://www.msdmanuals.com/en-sg/home/brain,-spinal-cord,-and-nerve-disorders/meningitis/introduction-to-meningitis (accessed on 21 July 2022).
- van de Beek, D.; Cabellos, C.; Dzupova, O.; Esposito, S.; Klein, M.; Kloek, A.T.; Leib, S.L.; Mourvillier, B.; Ostergaard, C.; Pagliano, P.; et al. ESCMID guideline: Diagnosis and treatment of acute bacterial meningitis. Clin. Microbiol. Infect. 2016, 22, S37–S62. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tunkel, A.R.; Glaser, C.A.; Bloch, K.C.; Sejvar, J.J.; Marra, C.M.; Roos, K.L.; Hartman, B.J.; Kaplan, S.L.; Scheld, W.M.; Whitley, R.J. The Management of Encephalitis: Clinical Practice Guidelines by the Infectious Diseases Society of America. Clin. Infect. Dis. 2008, 47, 303–327. [Google Scholar] [CrossRef] [PubMed]
- Zunt, J.R.; Kassebaum, N.J.; Blake, N.; Glennie, L.; Wright, C.; Nichols, E.; Abd-Allah, F.; Abdela, J.; Abdelalim, A.; Adamu, A.A.; et al. Global, regional, and national burden of meningitis, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2018, 17, 1061–1082. [Google Scholar] [CrossRef] [Green Version]
- Vora, N.M.; Holman, R.C.; Mehal, J.M.; Steiner, C.A.; Blanton, J.; Sejvar, J. Burden of encephalitis-associated hospitalizations in the United States, 1998–2010. Neurology 2014, 82, 443–451. [Google Scholar] [CrossRef]
- Trujillo-Gomez, J.; Tsokani, S.; Arango-Ferreira, C.; Atehortua-Munoz, S.; Jimenez-Villegas, M.J.; Serrano-Tabares, C.; Veroniki, A.A.; Florez, I.D. Biofire FilmArray Meningitis/Encephalitis panel for the aetiological diagnosis of central nervous system infections: A systematic review and diagnostic test accuracy meta-analysis. eClinicalMedicine 2022, 44, 101275. [Google Scholar] [CrossRef]
- Goodlet, K.J.; Tan, E.; Knutson, L.; Nailor, M.D. Impact of the FilmArray meningitis/encephalitis panel on antimicrobial duration among patients with suspected central nervous system infection. Diagn. Microbiol. Infect. Dis. 2021, 100, 115394. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions Version 6.3 (updated February 2022); John Wiley & Sons: Hoboken, NJ, USA, 2022. [Google Scholar]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, 71. [Google Scholar] [CrossRef]
- Wan, X.; Wang, W.; Liu, J.; Tong, T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med. Res. Methodol. 2014, 14, 135. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ottawa Hospital and Research Institute. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analysis; Ottawa Hospital and Research Institute: Ottawa, Canada, 2011. [Google Scholar]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [Green Version]
- Walker, M.; Taylor, K.; Beaulieu, R., 3rd; Laurent, M.; Hamer, D.; O’Neal, C. The Clinical Impact of the FilmArray Meningitis/Encephalitis (ME) Panel on Antimicrobial Utilization in a Tertiary Hospital Setting. Am. J. Med. Sci. 2021, 361, 550–552. [Google Scholar] [CrossRef]
- Nabower, A.M.; Miller, S.; Biewen, B.; Lyden, E.; Goodrich, N.; Miller, A.; Gollehon, N.; Skar, G.; Snowden, J. Association of the FilmArray Meningitis/Encephalitis Panel With Clinical Management. Hosp. Pediatrics 2019, 9, 763–769. [Google Scholar] [CrossRef]
- Mostyn, A.; Lenihan, M.; O’Sullivan, D.; Woods, S.; O’Hara, M.; Powell, J.; Power, L.; O’Connell, N.H.; Dunne, C.P. Assessment of the FilmArray® multiplex PCR system and associated meningitis/encephalitis panel in the diagnostic service of a tertiary hospital. Infect. Prev. Pract. 2020, 2, 100042. [Google Scholar] [CrossRef] [PubMed]
- Dack, K.; Pankow, S.; Ablah, E.; Zackula, R.; Assi, M. Contribution of the BioFire(®) FilmArray(®) Meningitis/Encephalitis Panel: Assessing Antimicrobial Duration and Length of Stay. Kans. J. Med. 2019, 12, 1–3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Díaz, K.M.O.; Piedrahíta, J.A.A.; Suárez Brochero, O.F.; Granada, D.O.; Barón, L.M.; Bonilla, I.C.; Hasbun, R. Impact of the Film Array Meningitis/Encephalitis panel in adults with meningitis and encephalitis in Colombia. Epidemiol Infect. 2020, 148, e173. [Google Scholar] [CrossRef] [PubMed]
- Evans, M.; Merkel, K.G.; Harder, J.; Rose, D.T. Impact of the implementation of a rapid meningitis/encephalitis multiplex polymerase chain reaction panel on IV acyclovir duration: Multicenter, retrospective cohort of adult and pediatric patients. Diagn Microbiol Infect. Dis. 2020, 96, 114935. [Google Scholar] [CrossRef] [PubMed]
- Hagen, A.; Eichinger, A.; Meyer-Buehn, M.; Schober, T.; Huebner, J. Comparison of antibiotic and acyclovir usage before and after the implementation of an on-site FilmArray meningitis/encephalitis panel in an academic tertiary pediatric hospital: A retrospective observational study. BMC Pediatrics 2020, 20, 56. [Google Scholar] [CrossRef] [PubMed]
- McDonald, D.; Gagliardo, C.; Chiu, S.; Di Pentima, M.C. Impact of a Rapid Diagnostic Meningitis/Encephalitis Panel on Antimicrobial Use and Clinical Outcomes in Children. Antibiotics 2020, 9, 822. [Google Scholar] [CrossRef]
- Mina, Y.; Schechner, V.; Savion, M.; Yahav, D.; Bilavsky, E.; Sorek, N.; Ben-Zvi, H.; Adler, A. Clinical benefits of FilmArray meningitis-encephalitis PCR assay in partially-treated bacterial meningitis in Israel. BMC Infect. Dis. 2019, 19, 713. [Google Scholar] [CrossRef] [PubMed]
- Moffa, M.A.; Bremmer, D.N.; Carr, D.; Buchanan, C.; Shively, N.R.; Elrufay, R.; Walsh, T.L. Impact of a Multiplex Polymerase Chain Reaction Assay on the Clinical Management of Adults Undergoing a Lumbar Puncture for Suspected Community-Onset Central Nervous System Infections. Antibiotics 2020, 9, 282. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, M.P.; Francis, J.R.; Marr, I.M.; Baird, R.W. Impact of Cerebrospinal Fluid Multiplex Assay on Diagnosis and Outcomes of Central Nervous System Infections in Children: A Before and After Cohort Study. Pediatric Infect. Dis. J. 2018, 37, 868–871. [Google Scholar] [CrossRef] [PubMed]
- Posnakoglou, L.; Siahanidou, T.; Syriopoulou, V.; Michos, A. Impact of cerebrospinal fluid syndromic testing in the management of children with suspected central nervous system infection. Eur. J. Clin. Microbiol. Infect. Dis. Off. Publ. Eur. Soc. Clin. Microbiol. 2020, 39, 2379–2386. [Google Scholar]
- 26 van Zeggeren, I.E.; Bijlsma, M.W.; Tanck, M.W.; van de Beek, D.; Brouwer, M.C. Systematic review and validation of diagnostic prediction models in patients suspected of meningitis. J. Infect. 2020, 80, 143–151. [Google Scholar] [CrossRef] [PubMed]
- 27 DiDiodato, G.; Bradbury, N. Cerebrospinal Fluid Analysis With the BioFire FilmArray Meningitis/Encephalitis Molecular Panel Reduces Length of Hospital Stay in Patients With Suspected Central Nervous System Infections. Open Forum Infect. Dis. 2019, 6, 119. [Google Scholar] [CrossRef] [PubMed]
- Archimbaud, C.; Chambon, M.; Bailly, J.L.; Petit, I.; Henquell, C.; Mirand, A.; Aublet-Cuvelier, B.; Ughetto, S.; Beytout, J.; Clavelou, P.; et al. Impact of rapid enterovirus molecular diagnosis on the management of infants, children, and adults with aseptic meningitis. J. Med. Virol. 2009, 81, 42–48. [Google Scholar] [CrossRef] [PubMed]
- Radmard, S.; Reid, S.; Ciryam, P.; Boubour, A.; Ho, N.; Zucker, J. Clinical Utilization of the FilmArray Meningitis/Encephalitis (ME) Multiplex Polymerase Chain Reaction (PCR) Assay. Front. Neurol. 2019, 10, 281. [Google Scholar] [CrossRef] [Green Version]
- Barry, R.; Dempsey, C.; Barry, L.; Hooton, C.; O’ Connor, A.; Reynolds, C.; Cremin, M.; Felsenstein, S.; Cunney, R.; Dean, J.; et al. On-site Multiplex PCR for CSF diagnostics in an Acute Hospital versus Referral to Reference Laboratories: Assessing Economic Factors, Length of Stay and Antimicrobial Stewardship. J. Infect. 2021, 82, 414–451. [Google Scholar] [CrossRef]
- Rao, S.; Abzug, M.J.; Carosone-Link, P.; Peterson, T.; Child, J.; Siparksy, G.; Soranno, D.; Cadnapaphornchai, M.A.; Simões, E.A.F. Intravenous acyclovir and renal dysfunction in children: A matched case control study. J. Pediatr 2015, 166, 1462–1468. [Google Scholar] [CrossRef]
- Mason, W.J.; Nickols, H.H. Crystalluria from Acyclovir Use. N. Engl. J. Med. 2008, 358, 14. [Google Scholar] [CrossRef]
- Vomiero, G.; Carpenter, B.; Robb, I.; Filler, G. Combination of ceftriaxone and acyclovir-an underestimated nephrotoxic potential? Pediatr Nephrol 2002, 17, 633–637. [Google Scholar] [CrossRef]
- Ryan, L.; Heed, A.; Foster, J.; Valappil, M.; Schmid, M.L.; Duncan, C.J.A. Acute kidney injury (AKI) associated with intravenous aciclovir in adults: Incidence and risk factors in clinical practice. Int. J. Infect. Dis. 2018, 74, 97–99. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Samannodi, M.; Hansen, M.; Allana, A.; Hasbun, R. Compliance with international guidelines in adults with encephalitis. J. Clin. Virol. 2020, 127, 104369. [Google Scholar] [CrossRef] [PubMed]
- Lindström, J.; Elfving, K.; Lindh, M.; Westin, J.; Studahl, M. Assessment of the FilmArray ME panel in 4199 consecutively tested cerebrospinal fluid samples. Clin. Microbiol. Infect. Off. Publ. Eur. Soc. Clin. Microbiol. Infect. Dis. 2022, 28, 79–84. [Google Scholar] [CrossRef] [PubMed]
- Wells, G.A.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. Available online: https://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 21 July 2022).





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| First Author, Year | Population | Reported Control Testing | Month[s] and Year[s] Captured | ME Group | Control Group | ||
|---|---|---|---|---|---|---|---|
| N | Age, mean ± SD * (Years) | N | Age, mean ± SD * (Years) | ||||
| Dack K, 2019 | Adult Patients | CSF culture and GS | 7/8/2015−8/6/2017 | 47 | − | 50 | − |
| Diaz KMO, 2020 | Adult Patients | CSF culture and GS, CSF fungal culture, blood cultures, CT and MRI imaging (suspected encephalitis cases), India ink stain, CMV PCR and CrAg (patients with HIV diagnosis). | Before and after implementation of panel (May 2016) | 46 | 43.75 ± 5.25 | 52 | 35.75 ± 5 |
| DiDiodato G, 2019 | Unspecified | CSF cell count, CSF glucose and protein, CSF culture and GS, CSF fungal culture and stains, HSV PCR (send-out), EV PCR (send-out) | 4/1/2016−31/3/2018 | 53 | 43.99 ± 25.7 | 64 | 51.3 ± 20.7 |
| Evans M, 2020 | Adult and Pediatric Patients | CSF cell count, CSF glucose and protein, CSF bacterial/fungal culture, HSV PCR (batched testing), EV PCR (in-house), CMV PCR (send-out), HHV-6 PCR (send-out), EBV PCR (send-out) | 04/01/2016−12/01/2017 | 76 | Min age: 0 Max age: 89 | 132 | Min age: 0 Max age: 89 |
| Hagen A, 2020 | Pediatric Patients | Viral PCR send-out tests (HSV-1/2, EV, and HHV-6) | 01/2012−02/2017 | 46 | 0.8 ± 1.4 | 46 | 0.7 ± 1.3 |
| McDonald D, 2020 | Pediatric Patients | CSF cell count, culture, molecular respiratory pathogen panel | 01/2015−09/2018 | 61 | 1.3 ± 1.0 | 186 | 1.2 ± 0.9 |
| Mina Y, 2019 | Unspecified | CSF cell count, CSF culture, blood culture | 01/2010−06/2018 | 8 | 40 ± 26 | 23 | 43 ± 20 |
| Moffa MA, 2020 | Adult Patients | CSF cell count, CSF glucose and protein, CSF culture, HSV PCR (send-out), VSV PCR (send-out), CMV PCR (send-out) | 10/2016−9/2018 | 79 | 49.9 ± 17.5 | 81 | 50.6 ± 20.1 |
| Mostyn A, 2020 | Unspecified | CSF cell count, CSF culture and GS, latex agglutination tests (N. meningitidis A, B, C, Y, and W135; E. coli K1; H. influenzae Type B; S. pneumoniae; S. agalactiae), bacterial PCR send-out tests (N. meningitidis, E. coli K1, H. influenzae, S. pneumoniae, S. agalactiae), viral PCR send out tests (HSV 1, HSV 2, VZV, HHV-6), CrAg | 12/2016−07/2017 | 16 | − | 18 | − |
| Nabower AM, 2019 | Pediatric Patients | CSF cell count, CSF culture, EV PCR, HSV PCR | 6/2015−7/2017 | 223 | <30 days: 67 (30.0%) 30−90 days: 100 (44.8%) >90 days: 57 (25.6%) | 348 | <30 days: 121 (34.8%) 30−90 days: 129 (37.1%) >90 days: 98 (28.2%) |
| O’Brien MP, 2018 | Pediatric Patients | CSF cell count, CSF glucose and protein, CSF culture, viral PCR on-site tests (HSV and VZV), viral PCR send-out tests (HPeV and EV) | 11/2014−5/2017 | 29 | − | 36 | − |
| Posnakoglou L, 2020 | Pediatric Patients | CSF cell count, CSF glucose and protein, CSF culture and GS, viral PCR send-out tests (not defined, ordered at physician discretion) | 4/2018−4/2019 | 71 | 2.1 ± 4.4 | 71 | 1.1 ± 2.2 |
| Walker M, 2021 | Adult Patients | CSF cell count, CSF diagnostics (not defined) | 6/2015−9/2016 | 91 | − | 72 | − |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hueth, K.D.; Thompson-Leduc, P.; Totev, T.I.; Milbers, K.; Timbrook, T.T.; Kirson, N.; Hasbun, R. Assessment of the Impact of a Meningitis/Encephalitis Panel on Hospital Length of Stay: A Systematic Review and Meta-Analysis. Antibiotics 2022, 11, 1028. https://doi.org/10.3390/antibiotics11081028
Hueth KD, Thompson-Leduc P, Totev TI, Milbers K, Timbrook TT, Kirson N, Hasbun R. Assessment of the Impact of a Meningitis/Encephalitis Panel on Hospital Length of Stay: A Systematic Review and Meta-Analysis. Antibiotics. 2022; 11(8):1028. https://doi.org/10.3390/antibiotics11081028
Chicago/Turabian StyleHueth, Kyle D., Philippe Thompson-Leduc, Todor I. Totev, Katherine Milbers, Tristan T. Timbrook, Noam Kirson, and Rodrigo Hasbun. 2022. "Assessment of the Impact of a Meningitis/Encephalitis Panel on Hospital Length of Stay: A Systematic Review and Meta-Analysis" Antibiotics 11, no. 8: 1028. https://doi.org/10.3390/antibiotics11081028