
Emerging Antibiotic Resistance Patterns Affect Visual Outcome Treating Acute Endophthalmitis

 ,
,
Abstract
:1. Introduction
2. Results
2.1. Antibiotic Resistance
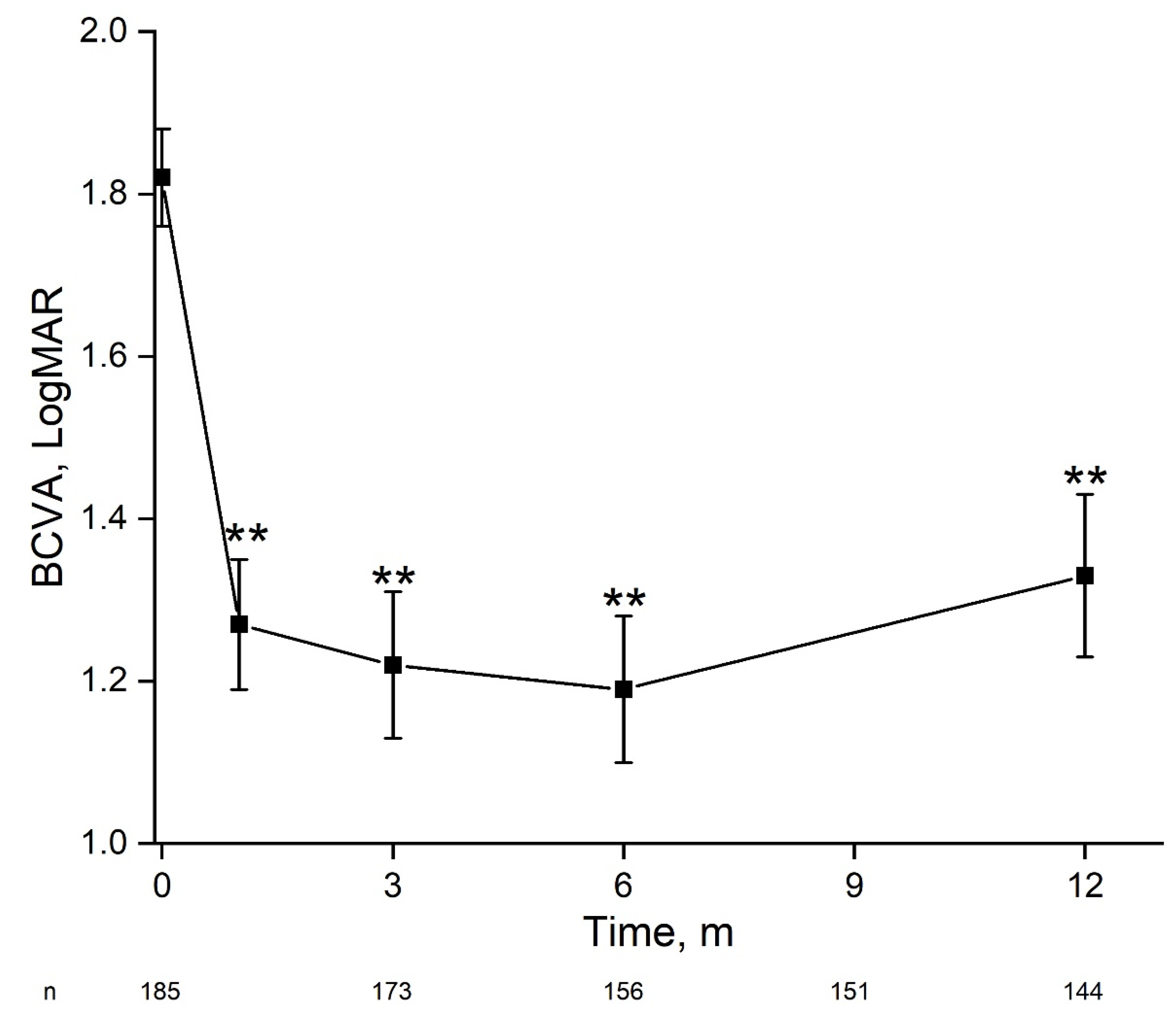
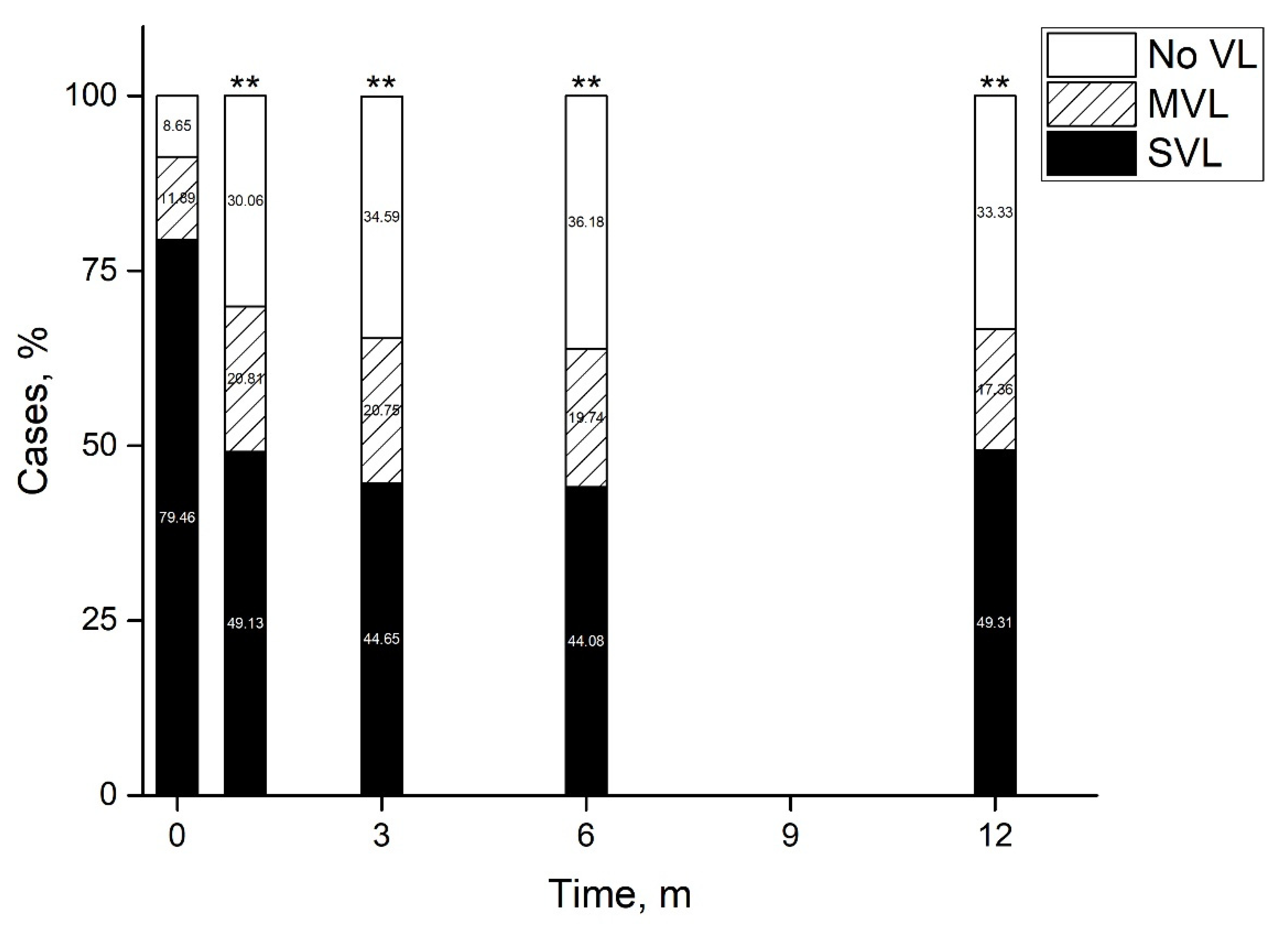
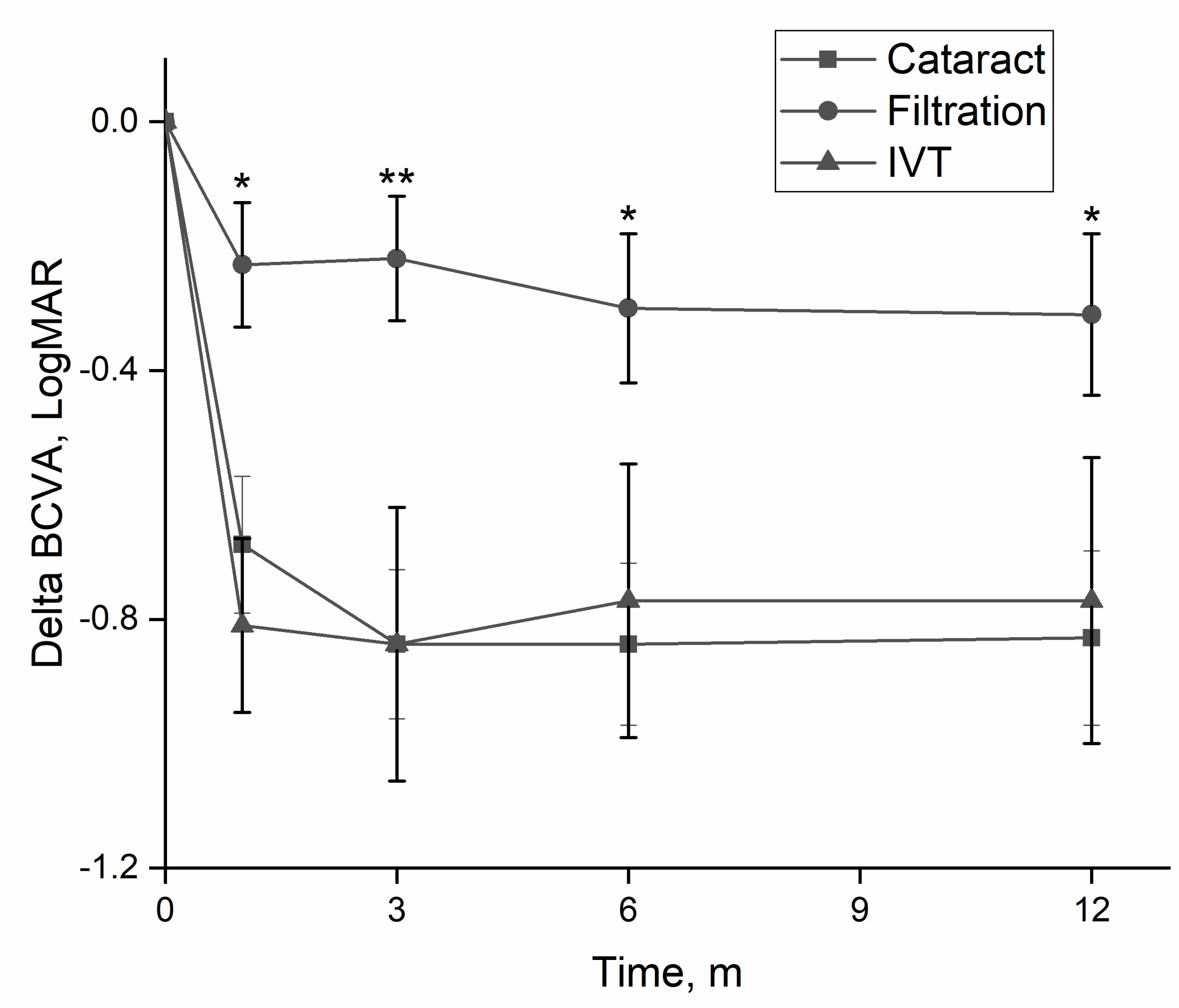
2.2. Early Treatment for Endophthalmitis
3. Discussion
4. Materials and Methods
4.1. Study Population
4.2. Statistical Analysis
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Results of the Endophthalmitis Vitrectomy Study. A randomized trial of immediate vitrectomy and of intravenous antibiotics for the treatment of postoperative bacterial endophthalmitis. Endophthalmitis Vitrectomy Study Group. Arch. Ophthalmol. 1995, 113, 1479–1496. [CrossRef]
- Kresloff, M.S.; Castellarin, A.A.; Zarbin, M.A. Endophthalmitis. Surv. Ophthalmol. 1998, 43, 193–224. [Google Scholar] [CrossRef]
- Pershing, S.; Lum, F.; Hsu, S.; Kelly, S.; Chiang, M.F.; Rich, W., III; Parke, D.W., II. Endophthalmitis after Cataract Surgery in the United States: A Report from the Intelligent Research in Sight Registry, 2013–2017. Ophthalmology 2020, 127, 151–158. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clarke, B.; Williamson, T.H.; Gini, G.; Gupta, B. Management of bacterial postoperative endophthalmitis and the role of vitrectomy. Surv. Ophthalmol. 2018, 63, 677–693. [Google Scholar] [CrossRef]
- Stevenson, L.J.; Dawkins, R.C.H.; Sheorey, H.; McGuinness, M.B.; Hurley, A.H.; Allen, P.J. Gram-negative endophthalmitis: A prospective study examining the microbiology, clinical associations and visual outcomes following infection. Clin. Exp. Ophthalmol. 2020, 48, 813–820. [Google Scholar] [CrossRef]
- Asbell, P.A.; Sanfilippo, C.M.; Mah, F.S. Antibiotic susceptibility of bacterial pathogens isolated from the aqueous and vitreous humour in the Antibiotic Resistance Monitoring in Ocular micRoorganisms (ARMOR) Surveillance Study: 2009–2020 update. J. Glob. Antimicrob. Resist. 2022, 23, 236–240. [Google Scholar] [CrossRef]
- Peck, T.J.; Patel, S.N.; Ho, A.C. Endophthalmitis after cataract surgery: An update on recent advances. Curr. Opin. Ophthalmol. 2021, 32, 62–68. [Google Scholar] [CrossRef]
- Relhan, N.; Albini, T.A.; Pathengay, A.; Kuriyan, A.E.; Miller, D.; Flynn, H.W. Endophthalmitis caused by Gram-positive organisms with reduced vancomycin susceptibility: Literature review and options for treatment. Br. J. Ophthalmol. 2016, 100, 446–452. [Google Scholar] [CrossRef] [Green Version]
- Chang, V.S.; Schwartz, S.G.; Davis, J.L.; Flynn, H.W. Endophthalmitis following cataract surgery and intracameral antibiotic: Moxifloxacin resistant Staphylococcus epidermidis. Am. J. Ophthalmol. Case Rep. 2018, 8, 127–130. [Google Scholar] [CrossRef]
- Kato, J.M.; Tanaka, T.; de Oliveira, L.M.S. Surveillance of post-cataract endophthalmitis at a tertiary referral center: A 10-year critical evaluation. Int. J. Retin. Vitr. 2021, 16, 14. [Google Scholar] [CrossRef]
- Hooper, C.Y.; Lightman, S.L.; Pacheco, P.; Tam, P.M.K.; Khan, A.; Taylor, S.R.J. Adjunctive antibiotics in the treatment of acute bacterial endophthalmitis following cataract surgery. Acta Ophthalmol. 2012, 90, e572–e573. [Google Scholar] [CrossRef] [PubMed]
- Ng, J.Q.; Morlet, N.; Pearman, J.W.; Constable, I.J.; McAllister, I.L.; Kennedy, C.J.; Isaacs, T.; Semmens, J.B.; Team EPSWA. Management and outcomes of postoperative endophthalmitis since the endophthalmitis vitrectomy study: The Endophthalmitis Population Study of Western Australia (EPSWA)’s fifth report. Ophthalmology 2005, 112, 1199–1206. [Google Scholar] [CrossRef] [PubMed]
- Robbins, C.B.; Ma, J.; Feng, H.L.; Fekrat, S. Clinical Decision Making and Visual Outcomes in Endophthalmitis Treated with Systemic Corticosteroids. Ophthalmol. Retin. 2020, 4, 1103–1108. [Google Scholar] [CrossRef] [PubMed]
- Roth, D.B.; Flynn, H.W., Jr. Antibiotic selection in the treatment of endophthalmitis: The significance of drug combinations and synergy. Surv. Ophthalmol. 1997, 41, 395–401. [Google Scholar] [CrossRef]
- Khera, M.; Pathengay, A.; Jindal, A.; Jalali, S.; Mathai, A.; Pappuru, R.R.; Relhan, N.; Das, T.; Sharma, S.; Flynn, H.W. Vancomycin-resistant Gram-positive bacterial endophthalmitis: Epidemiology, treatment options, and outcomes. J. Ophthalmic Inflamm. Infect. 2013, 3, 46. [Google Scholar] [CrossRef] [Green Version]
- Shivaramaiah, H.S.; Relhan, N.; Pathengay, A.; Mohan, N.; Flynn, H.W. Endophthalmitis caused by gram-positive bacteria resistant to vancomycin: Clinical settings, causative organisms, antimicrobial susceptibilities, and treatment outcomes. Am. J. Ophthalmol. Case Rep. 2018, 10, 211–214. [Google Scholar] [CrossRef]
- Murphy, C.C.; Nicholson, S.; Quah, S.A.; Batterbury, M.; Neal, T.; Kaye, S.B. Pharmacokinetics of vancomycin following intracameral bolus injection in patients undergoing phacoemulsification cataract surgery. Br. J. Ophthalmol. 2007, 91, 1350–1353. [Google Scholar] [CrossRef] [Green Version]
- Lott, M.N.; Fuller, J.J.; Hancock, H.A.; Singh, J.; Singh, H.; McGWIN, G.; Marcus, D.M. Vitreal penetration of oral moxifloxacin in humans. Retina 2008, 28, 473–476. [Google Scholar] [CrossRef]
- Hariprasad, S.M.; Shah, G.K.; Mieler, W.F.; Feiner, L.; Blinder, K.J.; Holekamp, N.M.; Gao, H.; Prince, R.A. Vitreous and aqueous penetration of orally administered moxifloxacin in humans. Arch. Ophthalmol. 2006, 124, 178–182. [Google Scholar] [CrossRef] [Green Version]
- Fuller, J.J.; Lott, M.N.; Henson, N.M.; Bhatti, A.A.; Singh, H.; McGwin, G.; Marcus, D.M. Vitreal penetration of oral and topical moxifloxacin in humans. Am. J. Ophthalmol. 2007, 143, 338–340. [Google Scholar] [CrossRef]
- Stringham, J.D.; Relhan, N.; Miller, D.; Flynn, H.W., Jr. Trends in Fluoroquinolone Nonsusceptibility Among Coagulase-Negative Staphylococcus Isolates Causing Endophthalmitis, 1995–2016. JAMA Ophthalmol. 2017, 135, 814–815. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chiquet, C.; Maurin, M.; Altayrac, J.; Aptel, F.; Boisset, S.; Vandenesch, F.; Cornut, P.; Romanet, J.; Gain, P.; Carricajo, A. Correlation between clinical data and antibiotic resistance in coagulase-negative Staphylococcus species isolated from 68 patients with acute post-cataract endophthalmitis. Clin. Microbiol. Infect. 2015, 21, 592.e1–592.e8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seal, D.; Reischl, U.; Behr, A.; Ferrer, C.; Alió, J.; Koerner, R.J.; Barry, P. Laboratory diagnosis of endophthalmitis: Comparison of microbiology and molecular methods in the European Society of Cataract & Refractive Surgeons multicenter study and susceptibility testing. J. Cataract Refract. Surg. 2008, 34, 1439–1450. [Google Scholar] [PubMed]
- Fan, K.C.; Lin, J.; Yannuzzi, N.A.; Al-Khersan, H.; Patel, N.A.; Maestre-Mesa, J.; Zaidi, M.; Miller, D.; Flynn, H.W., Jr. In vitro Susceptibilities of Methicillin-Susceptible and Resistant Staphylococci to Traditional Antibiotics Compared to a Novel Fluoroquinolone. J. Ophthalmic Inflamm. Infect. 2020, 10, 9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, D.; Nagiel, A.; Rahimy, E.; McCannel, C.A. Practice Patterns of Endophthalmitis Treatment: An International Survey of Retina Specialists. Ophthalmol. Retin. 2018, 2, 979–980. [Google Scholar] [CrossRef]
- Xu, K.; Chin, E.K.; Bennett, S.R.; Williams, D.F.; Ryan, E.H.; Dev, S.; Mittra, R.A.; Quiram, P.A.; Davies, J.B.; Parke, D.W., III; et al. Endophthalmitis after Intravitreal Injection of Vascular Endothelial Growth Factor Inhibitors: Management and Visual Outcomes. Ophthalmology 2018, 125, 1279–1286. [Google Scholar] [CrossRef]
- Vallejo-Garcia, J.L.; Asencio-Duran, M.; Pastora-Salvador, N.; Pastora-Salvador, N.; Vinciguerra, P.; Romano, M.R. Role of inflammation in endophthalmitis. Mediat. Inflamm. 2012, 2012, 196094. [Google Scholar] [CrossRef]
- Dar, N.; Pillar, S.; Friehmann, A.; Belkin, A.; Ofir, S. Endophthalmitis after intravitreal injections versus cataract surgery: A 15-year cohort. Int. Ophthalmol. 2020, 40, 73–79. [Google Scholar] [CrossRef]
- Tomkins-Netzer, O.; Talat, L.; Bar, A.; Lula, A.; Taylor, S.R.; Joshi, L.; Lightman, S. Long-term clinical outcome and causes of vision loss in patients with uveitis. Ophthalmology 2014, 121, 2387–2392. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Post-Cataract Surgery, n (%) | Post-Filtration Surgery, n (%) | Post-Intravitreal Injection, n (%) | p-Value | |
|---|---|---|---|---|
| Eyes, n | 71 | 63 | 39 | |
| Age at presentation, yrs, mean ± SEM | 69.5 ± 1.5 | 61.4 ± 2.2 | 71.5 ± 2.5 | 0.004 |
| Follow-up, m, mean ± SEM | 47.4 ± 4.9 | 46.48 ± 4.3 | 34.4 ± 5.3 | 0.13 |
| Culture-positive | 29 (40.9) | 25 (39.7) | 17 (43.6) | 0.42 |
| Moxifloxacin resistance | 4 (16.7) | 5 (25.0) | 1 (5.6) | 0.27 |
| Vancomycin resistance | 7 (26.9) | 8 (38.1) | 2 (10.5) | 0.14 |
| Amikacin resistance | 3 (14.0) | 9 (52.94) | 2 (11.1) | 0.007 |
| Final BCVA ≥20/40 | 33 (48.5) | 21 (34.4) | 9 (25) | 0.06 |
| Final BCVA >20/200 | 47 (69.1) | 30 (49.2) | 18 (50) | 0.18 |
| Crude OR (95% CI) | p-Value | Refined OR (95% CI) | p-Value | |
|---|---|---|---|---|
| Risk factor | ||||
| Age | 1.01 (0.99–1.02) | 0.23 | ||
| Cataract Sx | 1.4 (0.94–2.07) | 0.1 | 1.66 (1.04–2.66) | 0.03 |
| Post Intravitreal inj | 1.14 (0.67–1.94) | 0.64 | ||
| Culture Negative | 1.6 (1.02–2.49) | 0.04 | 1.67 (0.98–2.84) | 0.06 |
| Moxifloxacin sensitivity | 1.38 (0.5–3.76) | 0.53 | ||
| Vancomycin sensitivity | 1.04 (0.42–2.55) | 0.93 | ||
| Amikacin sensitivity | 0.92 (0.34–2.49) | 0.86 | ||
| IVT Vancomycin | 1.86 (0.88–3.93) | 0.1 | 3.15 (1.18–8.42) | 0.02 |
| IVT Amikacin | 1.44 (0.71–2.9) | 0.31 | ||
| PPV | 1.01 (0.62–1.65) | 0.97 | ||
| Early Prednisolone | 0.622 (0.35–1.12) | 0.11 | ||
| Oral Moxifloxacin | 0.91 (0.48–1.72) | 0.76 | ||
| IVT Corticosteroids | 0.95 (0.54–1.68) | 0.87 | ||
| Need for repeat Inj | 0.61 (0.35–1.07) | 0.08 | 0.56 (0.29–1.11) | 0.09 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wu, X.-N.; Chen, Y.-H.; Sharief, L.; Al-Janabi, A.; Al Qassimi, N.; Lightman, S.; Tomkins-Netzer, O. Emerging Antibiotic Resistance Patterns Affect Visual Outcome Treating Acute Endophthalmitis. Antibiotics 2022, 11, 843. https://doi.org/10.3390/antibiotics11070843
Wu X-N, Chen Y-H, Sharief L, Al-Janabi A, Al Qassimi N, Lightman S, Tomkins-Netzer O. Emerging Antibiotic Resistance Patterns Affect Visual Outcome Treating Acute Endophthalmitis. Antibiotics. 2022; 11(7):843. https://doi.org/10.3390/antibiotics11070843
Chicago/Turabian StyleWu, Xia-Ni, Yi-Hsing Chen, Lazha Sharief, Ahmed Al-Janabi, Nura Al Qassimi, Sue Lightman, and Oren Tomkins-Netzer. 2022. "Emerging Antibiotic Resistance Patterns Affect Visual Outcome Treating Acute Endophthalmitis" Antibiotics 11, no. 7: 843. https://doi.org/10.3390/antibiotics11070843