
Epidemiology, Clinical Characteristics, Risk Factors, and Outcomes of Candidemia in a Large Tertiary Teaching Hospital in Western China: A Retrospective 5-Year Study from 2016 to 2020

Abstract
:1. Introduction
2. Results
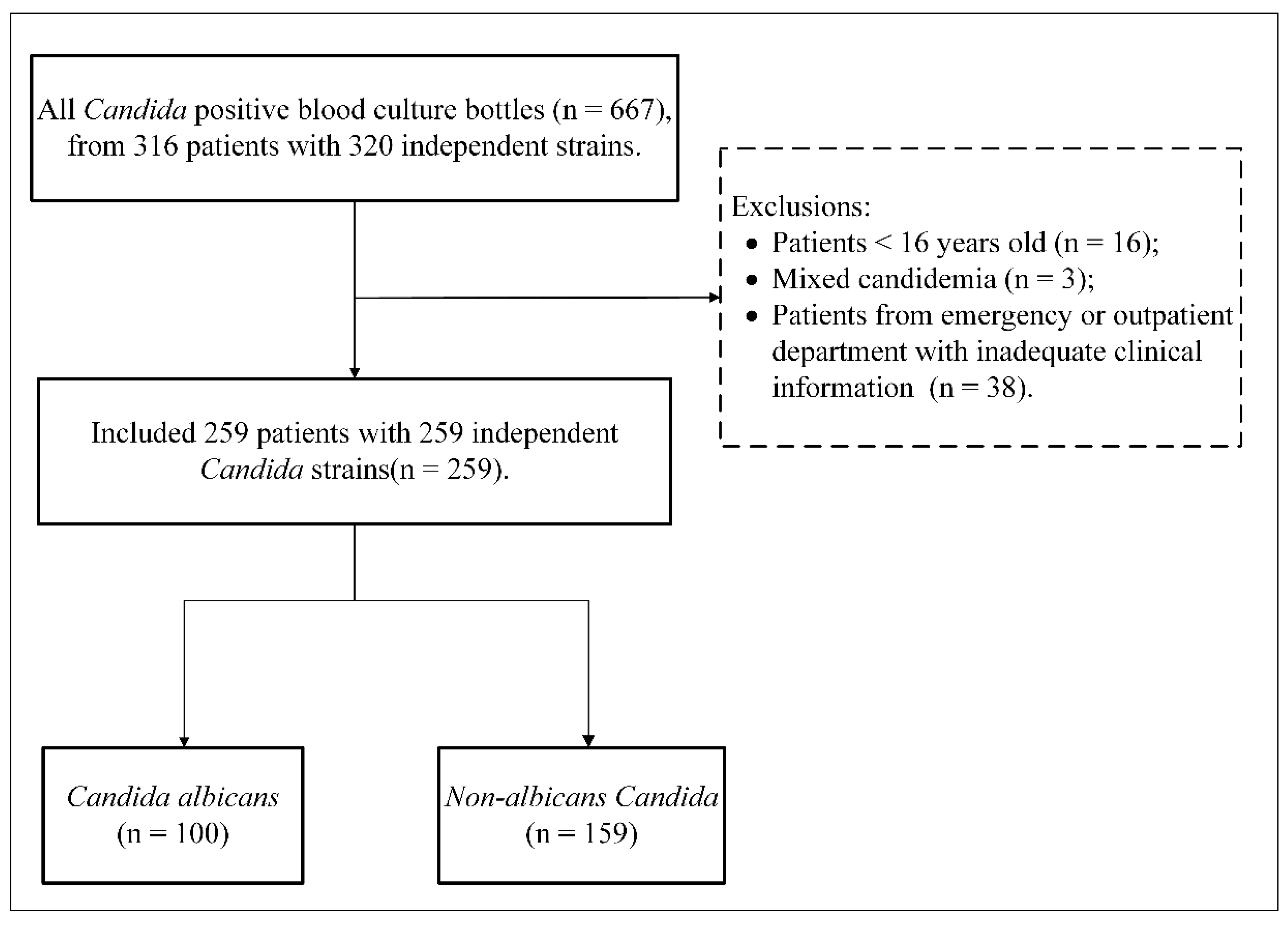
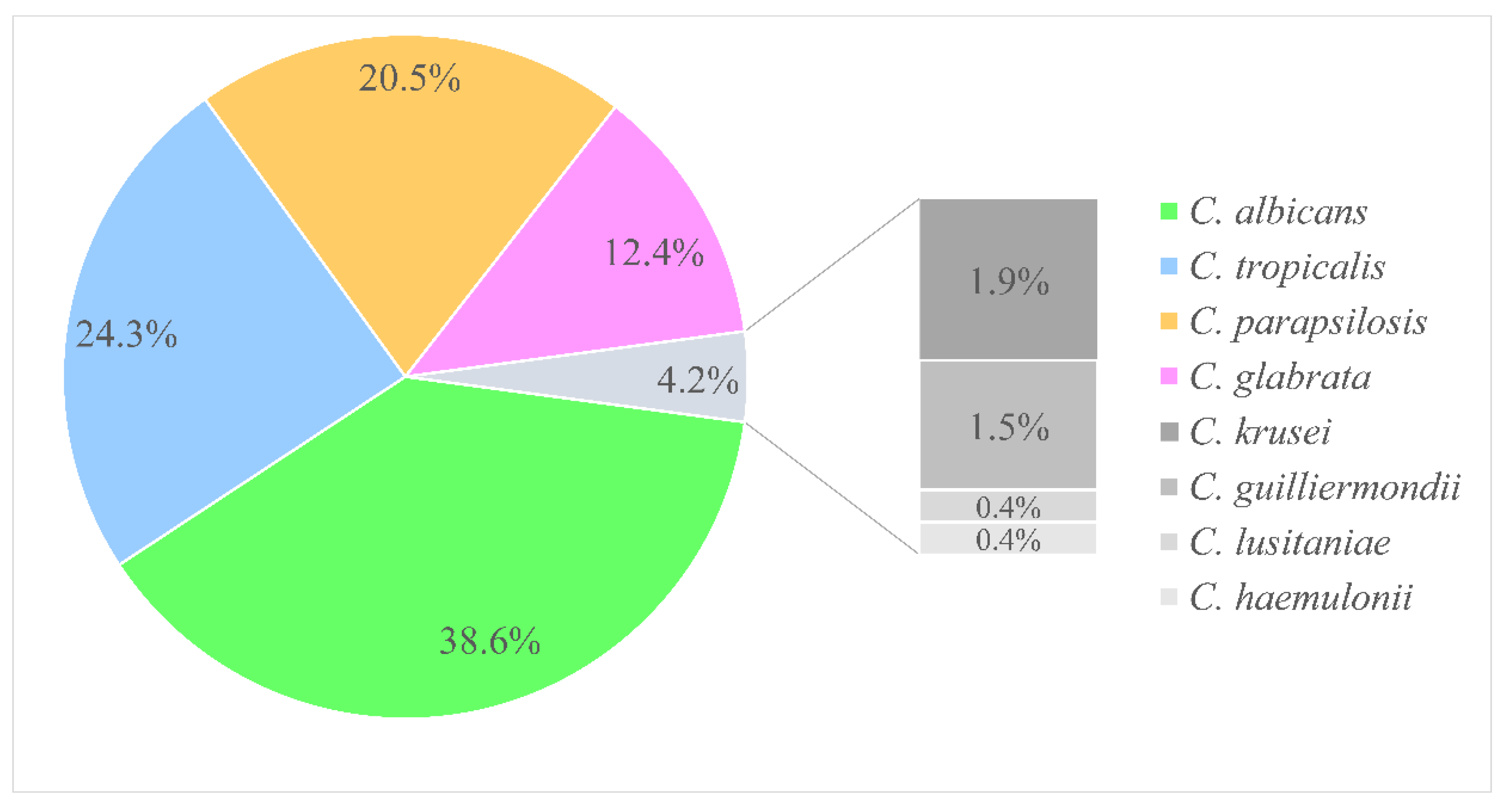
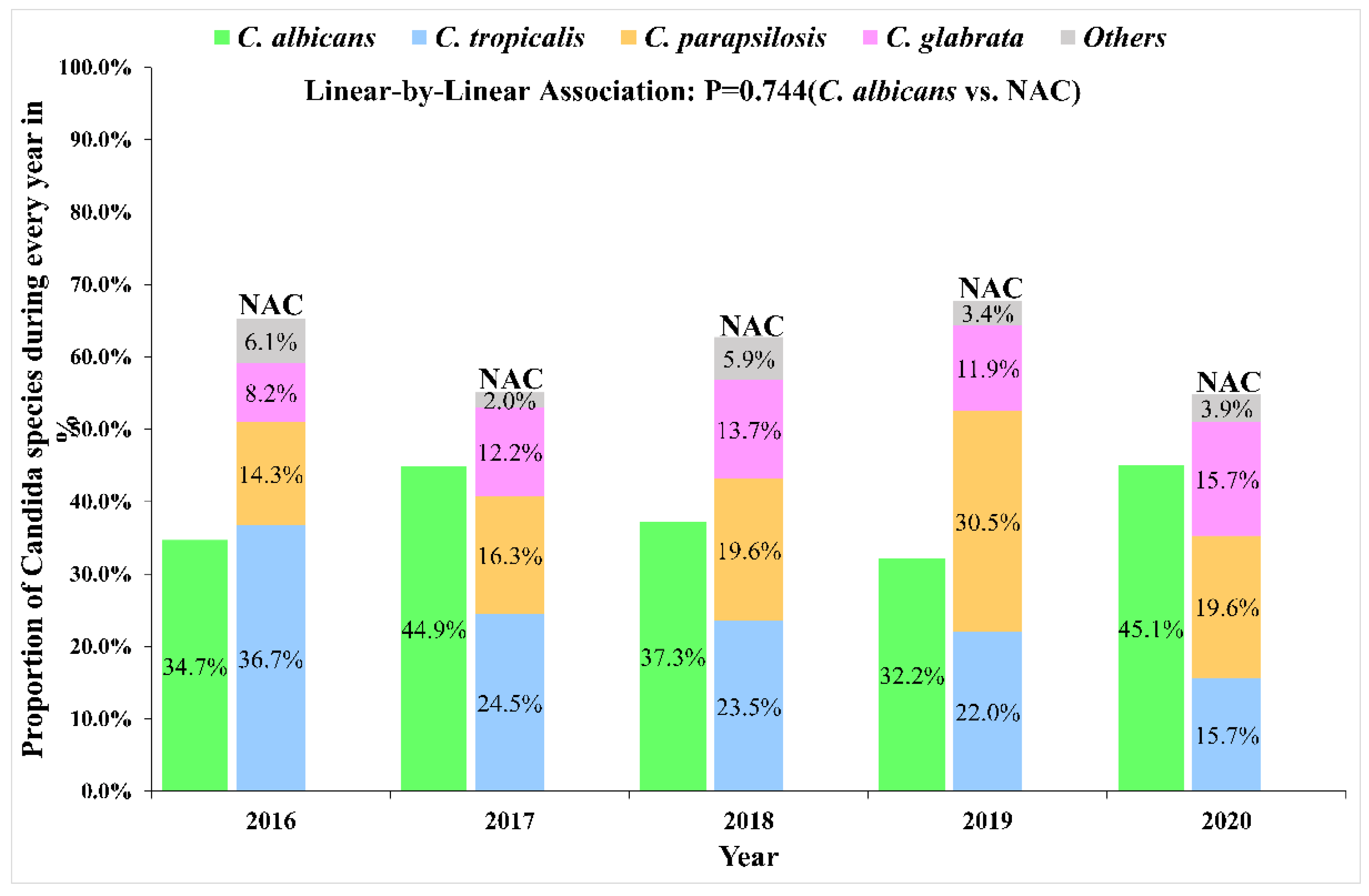
2.1. Species Distribution
2.2. Antifungal Susceptibility Testing
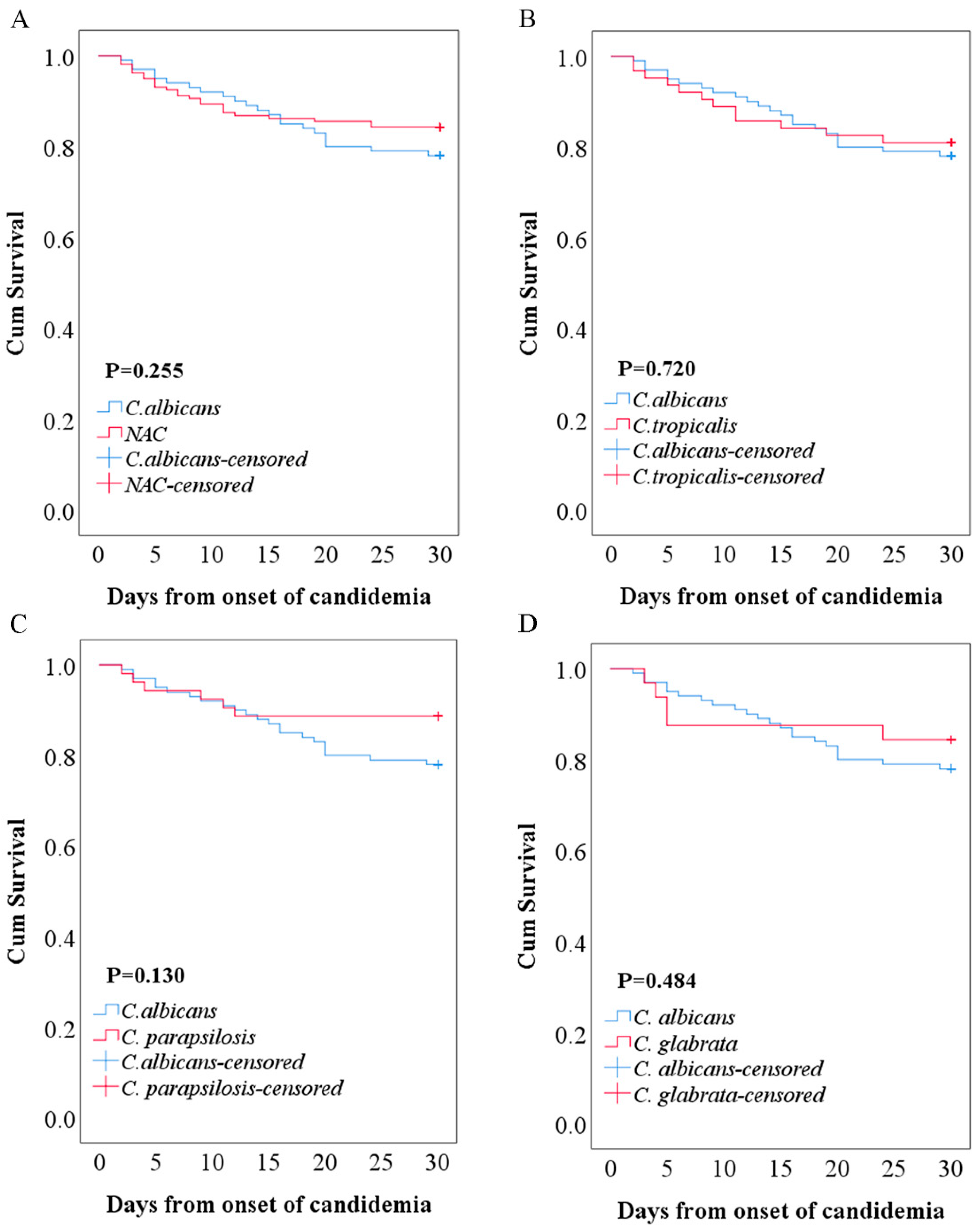
2.3. Clinical Characteristics and Outcomes
2.4. C. albicans vs. Non-albicans Candida
3. Discussion
4. Materials and Methods
4.1. Setting, Study Design, and Data Collection
4.2. Definitions
4.3. Microbiological Analysis
4.4. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Pappas, P.G.; Lionakis, M.S.; Arendrup, M.C.; Ostrosky-Zeichner, L.; Kullberg, B.J. Invasive candidiasis. Nat. Rev. Dis. Primers 2018, 4, 18026. [Google Scholar] [CrossRef]
- Kullberg, B.J.; Arendrup, M.C. Invasive Candidiasis. N. Engl. J. Med. 2015, 373, 1445–1456. [Google Scholar] [CrossRef] [Green Version]
- Enoch, D.A.; Yang, H.; Aliyu, S.H.; Micallef, C. The Changing Epidemiology of Invasive Fungal Infections. Methods Mol. Biol. 2017, 1508, 17–65. [Google Scholar] [CrossRef]
- Pappas, P.G.; Kauffman, C.A.; Andes, D.R.; Clancy, C.J.; Marr, K.A.; Ostrosky-Zeichner, L.; Reboli, A.C.; Schuster, M.G.; Vazquez, J.A.; Walsh, T.J.; et al. Clinical Practice Guideline for the Management of Candidiasis: 2016 Update by the Infectious Diseases Society of America. Clin. Infect. Dis. 2016, 62, e1–e50. [Google Scholar] [CrossRef]
- Arendrup, M.C.; Patterson, T.F. Multidrug-Resistant Candida: Epidemiology, Molecular Mechanisms, and Treatment. J. Infect. Dis. 2017, 216, S445–S451. [Google Scholar] [CrossRef] [Green Version]
- Cornely, O.A.; Bassetti, M.; Calandra, T.; Garbino, J.; Kullberg, B.J.; Lortholary, O.; Meersseman, W.; Akova, M.; Arendrup, M.C.; Arikan-Akdagli, S.; et al. ESCMID* guideline for the diagnosis and management of Candida diseases 2012: Non-neutropenic adult patients. Clin. Microbiol. Infect. 2012, 18 (Suppl. 7), 19–37. [Google Scholar] [CrossRef] [Green Version]
- Sriphannam, C.; Nuanmuang, N.; Saengsawang, K.; Amornthipayawong, D.; Kummasook, A. Anti-fungal susceptibility and virulence factors of Candida spp. isolated from blood cultures. J. Mycol. Med. 2019, 29, 325–330. [Google Scholar] [CrossRef]
- Giacobbe, D.R.; Maraolo, A.E.; Simeon, V.; Magne, F.; Pace, M.C.; Gentile, I.; Chiodini, P.; Viscoli, C.; Sanguinetti, M.; Mikulska, M.; et al. Changes in the relative prevalence of candidaemia due to non-albicans Candida species in adult in-patients: A systematic review, meta-analysis and meta-regression. Mycoses 2020, 63, 334–342. [Google Scholar] [CrossRef]
- Xiao, M.; Chen, S.C.; Kong, F.; Xu, X.L.; Yan, L.; Kong, H.S.; Fan, X.; Hou, X.; Cheng, J.W.; Zhou, M.L.; et al. Distribution and Antifungal Susceptibility of Candida Species Causing Candidemia in China: An Update From the CHIF-NET Study. J. Infect. Dis. 2020, 221, S139–S147. [Google Scholar] [CrossRef]
- Xu, H.; Yu, S.Y.; Zhou, M.L.; Ning, Y.T.; Xiao, M.; Li, X.G.; Chen, M.; Kong, F.; Chen, S.; Ming, L.; et al. Epidemiology and Antifungal Susceptibility Patterns of Invasive Fungal Infections From 2012 To 2014 In A Teaching Hospital in Central China. Infect. Drug Resist. 2019, 12, 3641–3651. [Google Scholar] [CrossRef] [Green Version]
- Zhang, W.; Song, X.; Wu, H.; Zheng, R. Epidemiology, risk factors and outcomes of Candida albicans vs. non-albicans candidaemia in adult patients in Northeast China. Epidemiol. Infect. 2019, 147, e277. [Google Scholar] [CrossRef] [Green Version]
- Koehler, P.; Stecher, M.; Cornely, O.A.; Koehler, D.; Vehreschild, M.; Bohlius, J.; Wisplinghoff, H.; Vehreschild, J.J. Morbidity and mortality of candidaemia in Europe: An epidemiologic meta-analysis. Clin. Microbiol. Infect. 2019, 25, 1200–1212. [Google Scholar] [CrossRef]
- Zhang, A.Y.; Shrum, S.; Williams, S.; Petnic, S.; Nadle, J.; Johnston, H.; Barter, D.; Vonbank, B.; Bonner, L.; Hollick, R.; et al. The Changing Epidemiology of Candidemia in the United States: Injection Drug Use as an Increasingly Common Risk Factor-Active Surveillance in Selected Sites, United States, 2014–2017. Clin. Infect. Dis. 2020, 71, 1732–1737. [Google Scholar] [CrossRef]
- Guinea, J. Global trends in the distribution of Candida species causing candidemia. Clin. Microbiol. Infect. 2014, 20 (Suppl. 6), 5–10. [Google Scholar] [CrossRef] [Green Version]
- Zuza-Alves, D.L.; Silva-Rocha, W.P.; Francisco, E.C.; de Araujo, M.C.B.; de Azevedo Melo, A.S.; Chaves, G.M. Candida tropicalis geographic population structure maintenance and dispersion in the coastal environment may be influenced by the climatic season and anthropogenic action. Microb. Pathog. 2019, 128, 63–68. [Google Scholar] [CrossRef]
- Liu, F.; Zhong, L.; Zhou, F.; Zheng, C.; Zhang, K.; Cai, J.; Zhou, H.; Tang, K.; Dong, Z.; Cui, W.; et al. Clinical Features, Strain Distribution, Antifungal Resistance and Prognosis of Patients with Non-albicans Candidemia: A Retrospective Observational Study. Infect. Drug Resist. 2021, 14, 3233–3246. [Google Scholar] [CrossRef]
- Ngamchokwathana, C.; Chongtrakool, P.; Waesamaae, A.; Chayakulkeeree, M. Risk Factors and Outcomes of Non-albicans Candida Bloodstream Infection in Patients with Candidemia at Siriraj Hospital-Thailand’s Largest National Tertiary Referral Hospital. J. Fungi 2021, 7, 269. [Google Scholar] [CrossRef]
- Fan, X.; Xiao, M.; Liao, K.; Kudinha, T.; Wang, H.; Zhang, L.; Hou, X.; Kong, F.; Xu, Y.C. Notable Increasing Trend in Azole Non-susceptible Candida tropicalis Causing Invasive Candidiasis in China (August 2009 to July 2014): Molecular Epidemiology and Clinical Azole Consumption. Front. Microbiol. 2017, 8, 464. [Google Scholar] [CrossRef]
- Clinical and Laboratory Standards Institute (CLSI). Performance Standards for Antifungal Susceptibility Testing of Yeasts, 2nd ed.; CLSI M60; Clinical and Laboratory Standards Institute: Wayne, PA, USA, 2020. [Google Scholar]
- Clinical and Laboratory Standards Institute (CLSI). Epidemiological Cutoff Values for Antifungal Susceptibility Testing, 2nd ed.; CLSI M59; Clinical and Laboratory Standards Institute: Wayne, PA, USA, 2018. [Google Scholar]
- Xiao, M.; Sun, Z.Y.; Kang, M.; Guo, D.W.; Liao, K.; Chen, S.C.; Kong, F.; Fan, X.; Cheng, J.W.; Hou, X.; et al. Five-Year National Surveillance of Invasive Candidiasis: Species Distribution and Azole Susceptibility from the China Hospital Invasive Fungal Surveillance Net (CHIF-NET) Study. J. Clin. Microbiol. 2018, 56, e00577-18. [Google Scholar] [CrossRef] [Green Version]
- Oliveira, J.S.; Pereira, V.S.; Castelo-Branco, D.; Cordeiro, R.A.; Sidrim, J.J.C.; Brilhante, R.S.N.; Rocha, M.F.G. The yeast, the antifungal, and the wardrobe: A journey into antifungal resistance mechanisms of Candida tropicalis. Can. J. Microbiol. 2020, 66, 377–388. [Google Scholar] [CrossRef]
- Perlin, D.S.; Rautemaa-Richardson, R.; Alastruey-Izquierdo, A. The global problem of antifungal resistance: Prevalence, mechanisms, and management. Lancet Infect. Dis. 2017, 17, e383–e392. [Google Scholar] [CrossRef]
- Donnelly, J.P.; Chen, S.C.; Kauffman, C.A.; Steinbach, W.J.; Baddley, J.W.; Verweij, P.E.; Clancy, C.J.; Wingard, J.R.; Lockhart, S.R.; Groll, A.H.; et al. Revision and Update of the Consensus Definitions of Invasive Fungal Disease from the European Organization for Research and Treatment of Cancer and the Mycoses Study Group Education and Research Consortium. Clin. Infect. Dis. 2020, 71, 1367–1376. [Google Scholar] [CrossRef] [Green Version]
- Chandra, J.; Mukherjee, P.K. Candida Biofilms: Development, Architecture, and Resistance. Microbiol. Spectr. 2015, 3, 9. [Google Scholar] [CrossRef] [Green Version]
- Ding, X.; Yan, D.; Sun, W.; Zeng, Z.; Su, R.; Su, J. Epidemiology and risk factors for nosocomial Non-Candida albicans candidemia in adult patients at a tertiary care hospital in North China. Med. Mycol. 2015, 53, 684–690. [Google Scholar] [CrossRef] [Green Version]
- Wu, J.Q.; Zhu, L.P.; Ou, X.T.; Xu, B.; Hu, X.P.; Wang, X.; Weng, X.H. Epidemiology and risk factors for non-Candida albicans candidemia in non-neutropenic patients at a Chinese teaching hospital. Med. Mycol. 2011, 49, 552–555. [Google Scholar] [CrossRef] [Green Version]
- Chow, J.K.; Golan, Y.; Ruthazer, R.; Karchmer, A.W.; Carmeli, Y.; Lichtenberg, D.; Chawla, V.; Young, J.; Hadley, S. Factors associated with candidemia caused by non-albicans Candida species versus Candida albicans in the intensive care unit. Clin. Infect. Dis. 2008, 46, 1206–1213. [Google Scholar] [CrossRef] [Green Version]
- Dimopoulos, G.; Ntziora, F.; Rachiotis, G.; Armaganidis, A.; Falagas, M.E. Candida albicans versus non-albicans intensive care unit-acquired bloodstream infections: Differences in risk factors and outcome. Anesth. Analg. 2008, 106, 523–529. [Google Scholar] [CrossRef]
- Gong, X.; Luan, T.; Wu, X.; Li, G.; Qiu, H.; Kang, Y.; Qin, B.; Fang, Q.; Cui, W.; Qin, Y.; et al. Invasive candidiasis in intensive care units in China: Risk factors and prognoses of Candida albicans and non-albicans Candida infections. Am. J. Infect. Control 2016, 44, e59–e63. [Google Scholar] [CrossRef]
- Nash, A.K.; Auchtung, T.A.; Wong, M.C.; Smith, D.P.; Gesell, J.R.; Ross, M.C.; Stewart, C.J.; Metcalf, G.A.; Muzny, D.M.; Gibbs, R.A.; et al. The gut mycobiome of the Human Microbiome Project healthy cohort. Microbiome 2017, 5, 153. [Google Scholar] [CrossRef]
- Chen, X.C.; Xu, J.; Wu, D.P. Clinical characteristics and implications of mixed candida/bacterial bloodstream infections in patients with hematological diseases. Eur. J. Clin. Microbiol. Infect. Dis. 2020, 39, 1445–1452. [Google Scholar] [CrossRef]
- Puig-Asensio, M.; Padilla, B.; Garnacho-Montero, J.; Zaragoza, O.; Aguado, J.M.; Zaragoza, R.; Montejo, M.; Munoz, P.; Ruiz-Camps, I.; Cuenca-Estrella, M.; et al. Epidemiology and predictive factors for early and late mortality in Candida bloodstream infections: A population-based surveillance in Spain. Clin. Microbiol. Infect. 2014, 20, O245. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Candida spp. | Antifungal a | MIC (μg/mL) | Antifungal Susceptibility | ||||
|---|---|---|---|---|---|---|---|
| Ranges | MIC50 | MIC90 | S/WT % | SDD/I % | R/NWT% | ||
| C. albicans | Amphotericin B | 0.12–1 | 0.5 | 0.5 | 100(100%) | - | 0 |
| 5-Flucytosine | 0.008–4 | 0.015 | 4 | 100(100%) | - | 0 | |
| Fluconazole | 0.12–256 | 0.5 | 1 | 92(92.0%) | 2(2.0%) | 6(6.0%) | |
| Voriconazole | 0.008–8 | 0.008 | 0.125 | 92(92.0%) | 4(4.0%) | 4(4.0%) | |
| Itraconazole | 0.008–16 | 0.06 | 0.125 | 91(91.0%) | - | 9(9.0%) | |
| Posaconazole | ≤0.008–8 | 0.015 | 0.03 | 72(93.5%) | - | 5(6.5%) | |
| Anidulafungin | 0.015–0.5 | 0.03 | 0.12 | 77(100%) | 0 | 0 | |
| Caspofungin | 0.008–0.25 | 0.06 | 0.12 | 77(100%) | 0 | 0 | |
| Micafungin | ≤0.008–0.5 | 0.008 | 0.015 | 77(100%) | 0 | 0 | |
| C. tropicalis | Amphotericin B | 0.25–1 | 0.5 | 1 | 63(100%) | - | 0 |
| 5-Flucytosine | 0.008–4 | 0.015 | 4 | 63(100%) | - | 0 | |
| Fluconazole | 0.25–256 | 1 | 128 | 32(50.8%) | 1(1.6%) | 30(47.6%) | |
| Voriconazole | 0.008–8 | 0.25 | 8 | 31(49.2%) | 6(9.5%) | 26(41.3%) | |
| Itraconazole | 0.06–16 | 0.5 | 2 | 44(69.8%) | - | 19(30.2%) | |
| Posaconazole | 0.015–8 | 0.25 | 1 | 14(34.1%) | - | 27(65.9%) | |
| Anidulafungin | 0.015–0.5 | 0.12 | 0.25 | 39(95.1%) | 2(4.9%) | 0 | |
| Caspofungin | 0.015–0.25 | 0.06 | 0.25 | 41(100%) | 0 | 0 | |
| Micafungin | 0.015–0.5 | 0.03 | 0.06 | 40(97.6%) | 1(2.4%) | 0 | |
| C. parapsilosis | Amphotericin B | 0.12–1 | 0.25 | 0.5 | 53(100%) | - | 0 |
| 5-Flucytosine | 0.008–4 | 0.015 | 4 | 53(100%) | - | 0 | |
| Fluconazole | 0.12–128 | 0.5 | 4 | 45(84.9%) | 5(9.4%) | 3(5.7%) | |
| Voriconazole | 0.008–2 | 0.015 | 0.06 | 49(92.5%) | 0 | 4(7.5%) | |
| Itraconazole | 0.015–0.5 | 0.03 | 0.125 | 53(100%) | - | 0 | |
| Posaconazole | 0.008–0.5 | 0.015 | 0.06 | 45(100%) | - | 0 | |
| Anidulafungin | 0.12–2 | 1 | 2 | 45(100%) | 0 | 0 | |
| Caspofungin | 0.008–2 | 0.5 | 0.5 | 45(100%) | 0 | 0 | |
| Micafungin | 0.03–2 | 1 | 1 | 45(100%) | 0 | 0 | |
| C. glabrata | Amphotericin B | 0.12–2 | 0.5 | 2 | 32(100%) | - | 0 |
| 5-Flucytosine | 0.008–16 | 0.008 | 4 | 31(96.9%) | - | 1(3.1%) | |
| Fluconazole | 0.25–256 | 4 | 64 | - | 26(81.2%) | 6(18.8%) | |
| Voriconazole | 0.008–4 | 0.125 | 1 | 18(56.3%) | - | 14(43.8%) | |
| Itraconazole | 0.015–16 | 0.500 | 1 | 29(90.6%) | - | 3(9.4%) | |
| Posaconazole | 0.015–8 | 0.5 | 8 | 17(65.4%) | - | 9(34.6%) | |
| Anidulafungin | 0.125–2 | 0.03 | 0.06 | 24(92.3%) | 0 | 2(7.7%) | |
| Caspofungin | 0.008–0.5 | 0.03 | 0.25 | 21(80.8%) | 3(11.5%) | 2(7.7%) | |
| Micafungin | 0.008–1 | 0.015 | 0.03 | 24(92.3%) | 0 | 2(7.7%) | |
| Others b | Amphotericin B | 0.12–1 | 0.25 | 0.5 | 11(100%) | - | 0 |
| 5-Flucytosine | 0.008–16 | 1 | 4 | 11(100%) | - | 0 | |
| Fluconazole | 0.12–256 | 4 | 64 | 6(54.5%) | 0 | 5(45.5%) | |
| Voriconazole | 0.008–0.5 | 0.12 | 0.25 | 11(100%) | 0 | 0 | |
| Itraconazole | 0.03–1 | 0.25 | 0.5 | 11(100%) | - | 0 | |
| Posaconazole | 0.015–0.5 | 0.12 | 0.25 | 7(100%) | - | 0 | |
| Anidulafungin | 0.015–8 | 0.25 | 2 | 5(71.4%) | 0 | 2(28.6%) | |
| Caspofungin | 0.015–8 | 0.5 | 2 | 4(57.1%) | 1(14.3%) | 2(28.6%) | |
| Micafungin | 0.015–4 | 0.12 | 2 | 4(57.1%) | 2(28.6%) | 1(14.3%) | |
| Characteristic | Total (n = 259) | C. albicans (n = 100) | C. tropicalis (n = 63) | C. parapsilosis (n = 53) | Others a (n = 43) | p Value |
|---|---|---|---|---|---|---|
| Age | 53(43–66) | 56(46–67) | 50(33–63) | 56(44–68) | 47(30–63) | 0.008 |
| Age (≥65 years) | 73(28.2%) | 34(34.0%) | 14(22.2%) | 16(30.2%) | 9(20.9%) | 0.261 |
| Female | 82(31.7%) | 34(34.0%) | 18(28.6%) | 16(30.2%) | 14(32.6%) | 0.896 |
| Length of hospital stay | 32(18–56) | 29(19–49.5) | 39(21–62) | 27(15–49) | 32(17.5–67.5) | 0.378 |
| Length of ICU stay | 27(14–46) | 29(20–42) | 21(13–42) | 22(10–49) | 32(11–55) | 0.329 |
| Previous ICU stay | 139(53.7%) | 55(55.0%) | 31(49.2%) | 30(56.6%) | 23(53.5%) | 0.859 |
| Medical service | ||||||
| ICUs | 118(45.6%) | 51(51.0%) | 24(38.1%) | 22(41.5%) | 21(48.8%) | - |
| Medical wards | 63(24.3%) | 26(26.0%) | 14(22.2%) | 18(34.0%) | 5(11.6%) | - |
| Surgical wards | 34(13.1%) | 14(14.0%) | 5(7.9%) | 7(13.2%) | 8(18.6%) | - |
| Emergency departments | 28(10.8%) | 8(8.0%) | 8(12.7%) | 5(9.4%) | 7(16.3%) | - |
| Hematology wards | 16(6.2%) | 1(1.0%) | 12(19.0%) | 1(1.9%) | 2(4.7%) | - |
| Underlying conditions | ||||||
| CCI | 2(1–3) | 2(1–3) | 2(1–4) | 2(1–4) | 2(0–4) | 0.480 |
| aCCI | 3(2–5) | 3(1–5) | 3(2–5) | 4(2–6) | 3(1–5) | 0.334 |
| Gastrointestinal diseases | 134(51.7%) | 52(52.0%) | 26(41.3%) | 29(54.7%) | 27(62.8%) | 0.167 |
| Lung diseases | 133(51.4%) | 52(52.0%) | 27(42.9%) | 31(58.5%) | 23(53.5%) | 0.392 |
| Septic shock | 85(32.8%) | 40(40.0%) | 18(28.6%) | 13(24.5%) | 14(32.6%) | 0.212 |
| Kidney diseases | 73(28.2%) | 28(28.0%) | 14(22.2%) | 18(34.0%) | 13(30.2%) | 0.558 |
| Brain diseases | 62(23.9%) | 31(31.0%) | 11(17.5%) | 11(20.8%) | 9(20.9%) | 0.195 |
| Liver diseases | 59(22.8%) | 22(22.0%) | 15(23.8%) | 16(30.2%) | 6(14.0%) | 0.304 |
| Solid tumors | 50(19.3%) | 18(18.0%) | 12(19.0%) | 9(17.0%) | 11(25.6%) | 0.710 |
| Diabetes mellitus | 47(18.1%) | 21(21.0%) | 10(15.9%) | 6(11.3%) | 10(23.3%) | 0.364 |
| Heart diseases | 36(13.9%) | 16(16.0%) | 5(7.9%) | 11(20.8%) | 4(9.3%) | 0.166 |
| Neutropenia | 24(9.3%) | 4(4.0%) | 15(23.8%) | 2(3.8%) | 3(7.0%) | 0.000 |
| Leukemia and Lymphoma | 17(6.6%) | 1(1.0%) | 12(19.0%) | 2(3.8%) | 2(4.7%) | 0.000 |
| Transplantation | 10(3.9%) | 2(2.0%) | 6(9.5%) | 1(1.9%) | 1(2.3%) | 0.102 |
| Outcomes | ||||||
| 7-day mortality | 20(7.7%) | 6(6.0%) | 5(7.9%) | 3(5.7%) | 6(14.0%) | 0.392 |
| 30-day mortality | 47(18.1%) | 22(22.0%) | 12(19.0%) | 6(11.3%) | 7(16.3%) | 0.424 |
| In-hospital mortality b | 56(21.6%) | 23(23.0%) | 18(28.6%) | 6(11.3%) | 9(20.9%) | 0.128 |
| Characteristic | Total (n = 259) | C. albicans (n = 100) | C. tropicalis (n = 63) | C. parapsilosis (n = 53) | Others a (n = 43) | p Value |
|---|---|---|---|---|---|---|
| RBC (×1012/L) | 2.96(2.50–3.50) | 2.91(2.50–3.60) | 2.84(2.37–3.24) | 3.15(2.59–3.51) | 3.00(2.50–3.41) | 0.331 |
| HGB (g/L) | 86(75–100) | 86(75–105) | 83(71–99) | 89(80–103) | 86(75–96) | 0.298 |
| PLT (×109/L) | 127(67–230) | 153(73–260) | 87(19–159) | 139(94–220) | 141(69–230) | 0.003 |
| WBC (×109/L) | 8.86(5.01–13.00) | 10.86(7.67–14.21) | 8.76(2.19–13.00) | 5.89(3.91–8.95) | 8.98(5.12–13.40) | 0.000 |
| Neutrophils (×109/L) | 7.47(3.99–11.30) | 9.34(6.54–12.52) | 6.70(0.64–11.66) | 4.43(3.01–7.37) | 7.34(4.49–11.93) | 0.000 |
| Lymphocyte (×109/L) | 0.60(0.38–1.03) | 0.62(0.43–1.02) | 0.59(0.23–0.88) | 0.76(0.47–1.23) | 0.48(0.33–0.86) | 0.026 |
| Monocyte (×109/L) | 0.38(0.15–0.57) | 0.42(0.20–0.61) | 0.32(0.05–0.56) | 0.38(0.20–0.53) | 0.42(0.10–0.66) | 0.174 |
| Anemia | 241(93.1%) | 92(92.0%) | 58(92.1%) | 49(92.5%) | 42(97.7%) | 0.661 |
| Leukopenia | 43(16.6%) | 5(5.0%) | 19(30.2%) | 12(22.6%) | 7(16.3%) | 0.000 |
| Leukocytosis | 115(44.4%) | 61(61.0%) | 25(39.7%) | 11(20.8%) | 18(41.9%) | 0.000 |
| Thrombocytopenia | 98(37.8%) | 34(34.0%) | 34(54.0%) | 14(26.4%) | 16(37.2%) | 0.014 |
| Thrombocytosis | 26(10.0%) | 16(16.0%) | 3(4.8%) | 3(5.7%) | 4(9.3%) | 0.084 |
| Hepatitis B virus | 30(11.6%) | 11(11.0%) | 10(15.9%) | 4(7.5%) | 5(11.6%) | 0.573 |
| Tuberculosis | 12(4.6%) | 3(3.0%) | 2(3.2%) | 5(9.4%) | 2(4.7%) | 0.341 |
| Fluconazole NS | 84(32.4%) | 8(8.0%) | 31(49.2%) | 8(15.1%) | 37(86.0%) | 0.000 |
| Voriconazole NS | 58(22.4%) | 8(8.0%) | 32(50.8%) | 4(7.5%) | 14(32.6%) | 0.000 |
| Azole cross resistance | 53(20.5%) | 6(6.0%) | 30(47.6%) | 3(5.7%) | 14(32.6%) | 0.000 |
| Characteristic | Total (n = 259) | C. albicans (n = 100) | NAC (n = 159) | p Value |
|---|---|---|---|---|
| Age (≥65 years) | 73(28.2%) | 34(34.0%) | 39(24.5%) | 0.099 |
| Gastrointestinal hemorrhage | 54(20.8%) | 30(30.0%) | 24(15.1%) | 0.004 |
| Intra-abdominal infections | 54(20.8%) | 27(27.0%) | 27(17.0%) | 0.053 |
| Pancreatitis | 50(19.3%) | 22(22.0%) | 28(17.6%) | 0.384 |
| Peritonitis | 31(12.0%) | 17(17.0%) | 14(8.8%) | 0.048 |
| Gastrointestinal perforation | 25(9.7%) | 12(12.0%) | 13(8.2%) | 0.310 |
| Septic shock | 85(32.8%) | 40(40.0%) | 45(28.3%) | 0.051 |
| Solid tumors | 50(19.3%) | 18(18.0%) | 32(20.1%) | 0.673 |
| Diabetes mellitus | 47(18.1%) | 21(21.0%) | 26(16.4%) | 0.345 |
| Urinary tract infections | 37(14.3%) | 12(12.0%) | 25(15.7%) | 0.404 |
| Neutropenia | 24(9.3%) | 4(4.0%) | 20(12.6%) | 0.020 |
| Leukemia and lymphoma | 17(6.6%) | 1(1.0%) | 16(10.1%) | 0.004 |
| Transplantation | 10(3.9%) | 2(2.0%) | 8(5.0%) | 0.325 |
| Parenteral nutrition | 183(70.7%) | 72(72.0%) | 111(69.8%) | 0.706 |
| Central venous catheters | 152(58.7%) | 68(68.0%) | 84(52.8%) | 0.016 |
| Urinary catheters | 140(54.1%) | 65(65.0%) | 75(47.2%) | 0.005 |
| Previous ICU Stay | 139(53.7%) | 55(55.0%) | 84(52.8%) | 0.733 |
| Invasive mechanical ventilation | 138(53.3%) | 64(64.0%) | 74(46.5%) | 0.006 |
| Thoracoabdominal drainage Catheters | 119(45.9%) | 59(59.0%) | 60(37.7%) | 0.001 |
| Surgery | 114(44.0%) | 54(54.0%) | 60(37.7%) | 0.010 |
| Abdominal surgery | 69(26.6%) | 32(32.0%) | 37(23.3%) | 0.122 |
| Hemodialysis | 47(18.1%) | 15(15.0%) | 32(20.1%) | 0.297 |
| Antibiotics | 247(95.4%) | 94(94.0%) | 153(96.2%) | 0.545 |
| Carbapenems | 125(48.3%) | 48(48.0%) | 77(48.4%) | 0.947 |
| Piperacillin | 80(30.9%) | 26(26.0%) | 54(34.0%) | 0.177 |
| Cephalosporins (third and fourth) | 77(29.7%) | 27(27.0%) | 50(31.4%) | 0.446 |
| Cefoperazone-sulbactam | 58(22.4%) | 21(21.0%) | 37(23.3%) | 0.670 |
| Quinolones | 51(19.7%) | 15(15.0%) | 36(22.6%) | 0.132 |
| Vancomycin | 46(17.8%) | 20(20.0%) | 26(16.4%) | 0.455 |
| Tigecycline | 32(12.4%) | 12(12.0%) | 20(12.6%) | 0.890 |
| Antifungal drugs | 38(14.7%) | 11(11.0%) | 27(17.0%) | 0.185 |
| Azoles | 29(11.2%) | 9(9.0%) | 20(12.6%) | 0.374 |
| Echinocandins | 11(4.2%) | 3(3.0%) | 8(5.0%) | 0.538 |
| Glucocorticoids | 65(25.1%) | 4(4.0%) | 25(15.7%) | 0.001 |
| Cancer chemotherapy | 52(20.1%) | 12(12.0%) | 40(25.2%) | 0.010 |
| Immunosuppressants | 15(5.8%) | 14(14.0%) | 51(32.1%) | 0.127 |
| Variable | Unadjusted OR (95% CI) | p Value | Adjusted OR (95% CI) | p Value |
|---|---|---|---|---|
| Gastrointestinal hemorrhage | 0.415(0.226–0.763) | 0.005 | 0.397(0.209–0.755) | 0.005 |
| Surgery | 0.516(0.311–0.858) | 0.011 | 0.609(0.346–1.073) | 0.086 |
| Thoracoabdominal drainage catheters | 0.421(0.253–0.702) | 0.001 | 0.507(0.289–0.891) | 0.018 |
| Glucocorticoids | 2.901(1.506–5.588) | 0.001 | 3.076(1.543–6.131) | 0.001 |
| Characteristic | Total (n = 163) | C. albicans (n = 100) | C. tropicalis (n = 63) | p Value |
|---|---|---|---|---|
| Age (≥65 years) | 48(29.4%) | 34(34.0%) | 14(22.2%) | 0.108 |
| Gastrointestinal hemorrhage | 43(26.4%) | 30(30.0%) | 13(20.6%) | 0.186 |
| Intra-abdominal infections | 36(22.1%) | 27(27.0%) | 9(14.3%) | 0.057 |
| Pancreatitis | 35(21.5%) | 22(22.0%) | 13(20.6%) | 0.836 |
| Peritonitis | 19(11.7%) | 17(17.0%) | 2(3.2%) | 0.007 |
| Gastrointestinal perforation | 13(8.0%) | 12(12.0%) | 1(1.6%) | 0.017 |
| Septic shock | 58(35.6%) | 40(40.0%) | 18(28.6%) | 0.138 |
| Diabetes mellitus | 31(19.0%) | 21(21.0%) | 10(15.9%) | 0.417 |
| Solid tumors | 30(18.4%) | 18(18.0%) | 12(19.0%) | 0.867 |
| Urinary tract infections | 22(13.5%) | 12(12.0%) | 10(15.9%) | 0.481 |
| Neutropenia | 19(11.7%) | 4(4.0%) | 15(23.8%) | 0.000 |
| Leukemia and lymphoma | 13(8.0%) | 1(1.0%) | 12(19.0%) | 0.000 |
| Transplantation | 8(4.9%) | 2(2.0%) | 6(9.5%) | 0.056 |
| Parenteral nutrition | 112(68.7%) | 72(72.0%) | 40(63.5%) | 0.254 |
| Central venous catheters | 98(60.1%) | 68(68.0%) | 30(47.6%) | 0.010 |
| Urinary catheters | 95(58.3%) | 65(65.0%) | 30(47.6%) | 0.028 |
| Invasive mechanical ventilation | 91(55.8%) | 64(64.0%) | 27(42.9%) | 0.008 |
| Previous ICU stay | 86(52.8%) | 55(55.0%) | 31(49.2%) | 0.471 |
| Thoracoabdominal drainage Catheters | 74(45.4%) | 59(59.0%) | 15(23.8%) | 0.000 |
| Surgery | 73(44.8%) | 54(54.0%) | 19(30.2%) | 0.003 |
| Abdominal surgery | 42(25.8%) | 32(32.0%) | 10(15.9%) | 0.022 |
| Hemodialysis | 26(16.0%) | 15(15.0%) | 11(17.5%) | 0.676 |
| Antibiotics | 154(94.5%) | 94(94.0%) | 60(95.2%) | 1.000 |
| Carbapenems | 84(51.5%) | 48(48.0%) | 36(57.1%) | 0.255 |
| Piperacillin | 46(28.2%) | 26(26.0%) | 20(31.7%) | 0.427 |
| Cephalosporins (third and fourth) | 47(28.8%) | 27(27.0%) | 20(31.7%) | 0.515 |
| Cefoperazone-sulbactam | 35(21.5%) | 21(21.0%) | 14(22.2%) | 0.853 |
| Quinolones | 31(19.0%) | 15(15.0%) | 16(25.4%) | 0.100 |
| Vancomycin | 30(18.4%) | 20(20.0%) | 10(15.9%) | 0.508 |
| Tigecycline | 20(12.3%) | 12(12.0%) | 8(12.7%) | 0.895 |
| Antifungal drugs | 24(14.7%) | 11(11.0%) | 13(20.6%) | 0.091 |
| Azoles | 17(10.4%) | 9(9.0%) | 8(12.7%) | 0.452 |
| Echinocandins | 6(3.7%) | 3(3.0%) | 3(4.8%) | 0.677 |
| Glucocorticoids | 39(23.9%) | 14(14.0%) | 25(39.7%) | 0.000 |
| Cancer chemotherapy | 32(19.6%) | 12(12.0%) | 20(31.7%) | 0.002 |
| Immunosuppressants | 11(6.7%) | 3(3.0%) | 8(12.7%) | 0.023 |
| Variable | Unadjusted OR (95% CI) | p Value | Adjusted OR (95% CI) | p Value |
|---|---|---|---|---|
| Gastrointestinal perforation | 0.118(0.015–0.933) | 0.043 | 0.193(0.022–1.689) | 0.137 |
| Thoracoabdominal drainage catheters | 0.217(0.107–0.439) | 0.000 | 0.277(0.131–0.588) | 0.001 |
| Leukemia and lymphoma | 23.294(2.946–184.192) | 0.003 | 10.08(1.127–90.133) | 0.039 |
| Glucocorticoids | 4.041(1.895–8.620) | 0.000 | 2.788(1.147–6.773) | 0.024 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hou, J.; Deng, J.; Liu, Y.; Zhang, W.; Wu, S.; Liao, Q.; Ma, Y.; Kang, M. Epidemiology, Clinical Characteristics, Risk Factors, and Outcomes of Candidemia in a Large Tertiary Teaching Hospital in Western China: A Retrospective 5-Year Study from 2016 to 2020. Antibiotics 2022, 11, 788. https://doi.org/10.3390/antibiotics11060788
Hou J, Deng J, Liu Y, Zhang W, Wu S, Liao Q, Ma Y, Kang M. Epidemiology, Clinical Characteristics, Risk Factors, and Outcomes of Candidemia in a Large Tertiary Teaching Hospital in Western China: A Retrospective 5-Year Study from 2016 to 2020. Antibiotics. 2022; 11(6):788. https://doi.org/10.3390/antibiotics11060788
Chicago/Turabian StyleHou, Jie, Jin Deng, Ya Liu, Weili Zhang, Siying Wu, Quanfeng Liao, Ying Ma, and Mei Kang. 2022. "Epidemiology, Clinical Characteristics, Risk Factors, and Outcomes of Candidemia in a Large Tertiary Teaching Hospital in Western China: A Retrospective 5-Year Study from 2016 to 2020" Antibiotics 11, no. 6: 788. https://doi.org/10.3390/antibiotics11060788