
Studying Factors Affecting Success of Antimicrobial Resistance Interventions through the Lens of Experience: A Thematic Analysis

 ,
,  , , , and
, , , and
Abstract
:1. Introduction
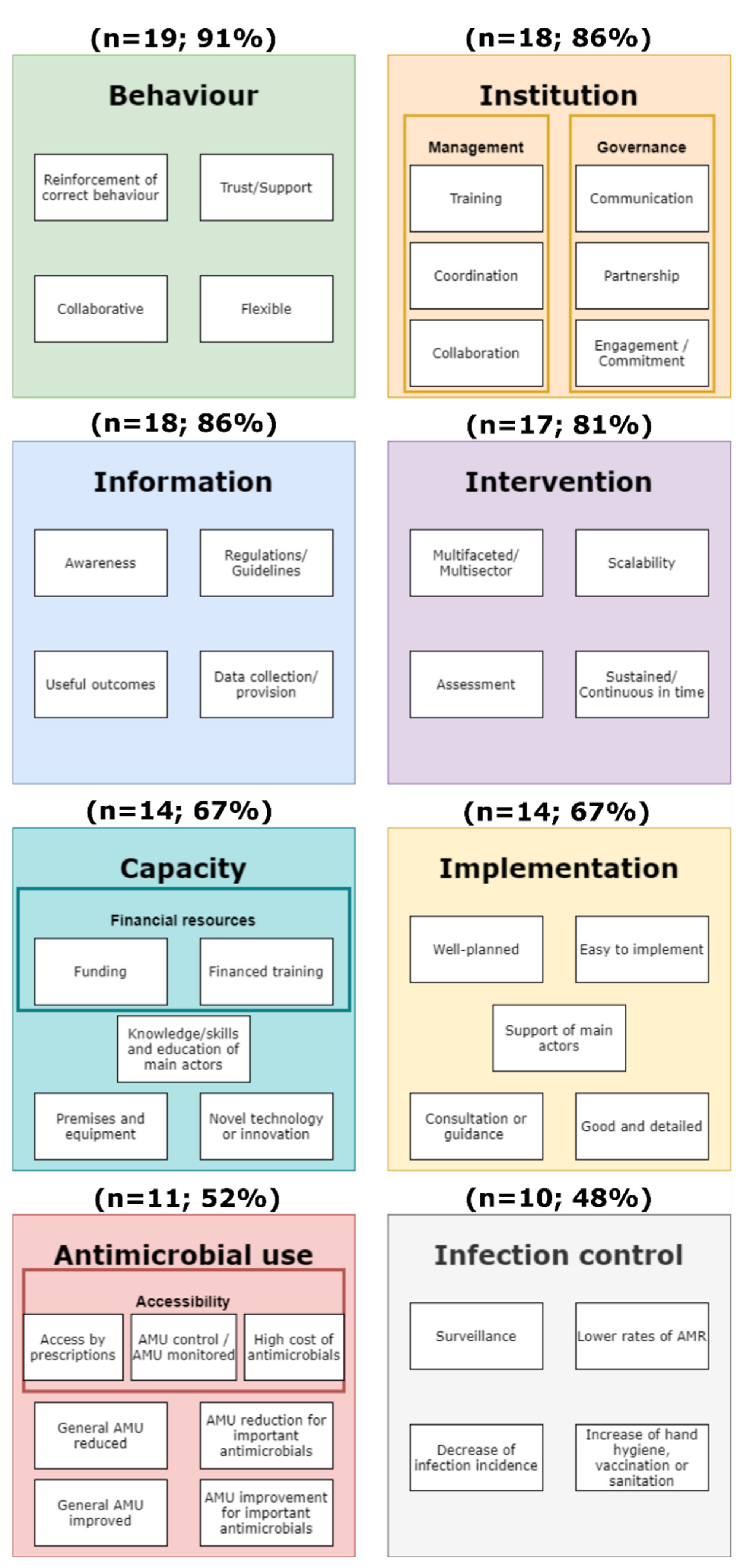
2. Results
3. Discussion
4. Materials and Methods
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
References
- Aslam, B.; Wang, W.; Arshad, M.I.; Khurshid, M.; Muzammil, S.; Rasool, M.H.; Nisar, M.A.; Alvi, R.F.; Aslam, M.A.; Qamar, M.U.; et al. Antibiotic resistance: A rundown of a global crisis. Infect. Drug Resist. 2018, 11, 1645–1658. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vila, J.; Moreno-Morales, J.; Ballesté-Delpierre, C. Current landscape in the discovery of novel antibacterial agents. Clin. Microbiol. Infect. 2020, 26, 596–603. [Google Scholar] [CrossRef] [PubMed]
- Laxminarayan, R.; Matsoso, P.; Pant, S.; Brower, C.; Røttingen, J.-A.; Klugman, K.; Davies, S. Access to effective antimicrobials: A worldwide challenge. Lancet 2016, 387, 168–175. [Google Scholar] [CrossRef]
- US CDC Antibiotic resistance threats in the United States. Centers Dis. Control Prev. 2019, 148, 1–150.
- Murray, C.J.; Ikuta, K.S.; Sharara, F.; Swetschinski, L.; Robles Aguilar, G.; Gray, A.; Han, C.; Bisignano, C.; Rao, P.; Wool, E.; et al. Global burden of bacterial antimicrobial resistance in 2019: A systematic analysis. Lancet 2022, 399, 629–655. [Google Scholar] [CrossRef]
- Wernli, D.; Jørgensen, P.S.; Harbarth, S.; Carroll, S.P.; Laxminarayan, R.; Levrat, N.; Røttingen, J.-A.A.; Pittet, D. Antimicrobial resistance: The complex challenge of measurement to inform policy and the public. PLoS Med. 2017, 14, 1–9. [Google Scholar] [CrossRef]
- Kousouli, E.; Zarkotou, O.; Polimeri, K.; Themeli-Digalaki, K.; Pournaras, S. Impact of bloodstream infections caused by carbapenem-resistant Gram-negative pathogens on ICU costs, mortality and length of stay. Infect. Prev. Pract. 2019, 1, 100020. [Google Scholar] [CrossRef]
- Robinson, T.P.; Bu, D.P.; Carrique-Mas, J.; Fèvre, E.M.; Gilbert, M.; Grace, D.; Hay, S.I.; Jiwakanon, J.; Kakkar, M.; Kariuki, S.; et al. Antibiotic resistance is the quintessential One Health issue. Trans. R. Soc. Trop. Med. Hyg. 2016, 110, 377–380. [Google Scholar] [CrossRef]
- Jørgensen, P.S.; Aktipis, A.; Brown, Z.; Carrière, Y.; Downes, S.; Dunn, R.R.; Epstein, G.; Frisvold, G.B.; Hawthorne, D.; Gröhn, Y.T.; et al. Antibiotic and pesticide susceptibility and the Anthropocene operating space. Nat. Sustain. 2018, 1, 632–641. [Google Scholar]
- OECD Building Resilience to the COVID-19 Pandemic: The Role of Centres of Government. Available online: http://www.oecd.org/coronavirus/policy-responses/building-resilience-to-the-covid-19-pandemic-the-role-of-centres-of-government-883d2961 (accessed on 2 February 2021).
- Wernli, D.; Søgaard Jørgensen, P.; Parmley, E.J.; Troell, M.; Majowicz, S.; Harbarth, S.; Léger, A.; Lambraki, I.; Graells, T.; Henriksson, P.J.G.; et al. Evidence for action: A One Health learning platform on interventions to tackle antimicrobial resistance. Lancet Infect. Dis. 2020, 3099, 1–5. [Google Scholar] [CrossRef]
- Rogers Van Katwyk, S.; Grimshaw, J.M.; Nkangu, M.; Mendelson, M.; Taljaard, M.; Hoffman, S.J. Study reporting quality among interventions to reduce antibiotic use is a barrier to evidence-informed policymaking on antimicrobial resistance: Systematic review. J. Antimicrob. Chemother. 2020, 75, 1091–1098. [Google Scholar] [CrossRef]
- Nilsen, P. Making sense of implementation theories, models and frameworks. Implement. Sci. 2015, 10, 53. [Google Scholar] [CrossRef] [Green Version]
- Rogers Van Katwyk, S.; Hoffman, S.J.; Mendelson, M.; Taljaard, M.; Grimshaw, J.M. Strengthening the science of addressing antimicrobial resistance: A framework for planning, conducting and disseminating antimicrobial resistance intervention research. Health Res. Policy Syst. 2020, 18, 60. [Google Scholar] [CrossRef]
- Léger, A.; Lambraki, I.; Graells, T.; Cousins, M.; Henriksson, P.J.G.; Harbarth, S.; Carson, C.; Majowicz, S.; Troell, M.; Parmley, E.J.; et al. AMR-Intervene: A social-ecological framework to capture the diversity of actions to tackle antimicrobial resistance from a One Health perspective. J. Antimicrob. Chemother. 2021, 76, 1–21. [Google Scholar] [CrossRef]
- Lambraki, I.A.; Majowicz, S.; Parmley, E.J.; Wernli, D.; Léger, A.; Graells, T.; Cousins, M.; Harbarth, S.; Carson, C.; Henriksson, P.; et al. Building social-ecological system resilience to tackle antimicrobial resistance across the One Health spectrum: Protocol for a mixed-methods study. (Preprint). JMIR Res. Protoc. 2020, 10, e24378. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef] [Green Version]
- Alban, L.; Dahl, J.; Andreasen, M.; Petersen, J.V.; Sandberg, M. Possible impact of the “ yellow card” antimicrobial scheme on meat inspection lesions in Danish finisher pigs. Prev. Vet. Med. 2013, 108, 334–341. [Google Scholar] [CrossRef] [Green Version]
- Cheng, A.C.; Turnidge, J.; Collignon, P.; Looke, D.; Barton, M.; Gottlieb, T. Control of Fluoroquinolone Resistance through Successful Regulation, Australia. Emerg. Infect. Dis. 2012, 18, 1453. [Google Scholar] [CrossRef]
- Hammerum, A.M.; Heuer, O.E.; Emborg, H.D.; Bagger-Skjøt, L.; Jensen, V.F.; Rogues, A.M.; Skov, R.L.; Agersø, Y.; Brandt, C.T.; Seyfarth, A.M.; et al. Danish Integrated Antimicrobial Resistance Monitoring and Research Program. Emerg. Infect. Dis. 2007, 13, 1633. [Google Scholar] [CrossRef]
- Hersberger, K.E.; Botomino, A.; Sarkar, R.; Tschudi, P.; Bucher, H.C.; Briel, M. Prescribed medications and pharmacy interventions for acute respiratory tract infections in Swiss primary care. J. Clin. Pharm. Ther. 2009, 34, 387–395. [Google Scholar] [CrossRef]
- Hiki, M.; Kawanishi, M.; Abo, H.; Kojima, A.; Koike, R.; Hamamoto, S.; Asai, T. Decreased Resistance to Broad-Spectrum Cephalosporin in Escherichia coli from Healthy Broilers at Farms in Japan After Voluntary Withdrawal of Ceftiofur. Foodborne Pathog. Dis. 2015, 12, 639–643. [Google Scholar] [CrossRef]
- Huttner, B.; Harbarth, S. “Antibiotics Are Not Automatic Anymore”-The French National Campaign To Cut Antibiotic Overuse. PLoS Med. 2009, 6, e1000080. [Google Scholar] [CrossRef] [Green Version]
- Karp, B.E.; Tate, H.; Plumblee, J.R.; Dessai, U.; Whichard, J.M.; Thacker, E.L.; Hale, K.R.; Wilson, W.; Friedman, C.R.; Griffin, P.M.; et al. National antimicrobial resistance monitoring system: Two decades of advancing public health through integrated surveillance of antimicrobial resistance. Foodborne Pathog. Dis. 2017, 14, 545–557. [Google Scholar] [CrossRef]
- MacKinnon, M.C.; Pearl, D.L.; Carson, C.A.; Parmley, E.J.; McEwen, S.A. Comparison of annual and regional variation in multidrug resistance using various classification metrics for generic Escherichia coli isolated from chicken abattoir surveillance samples in Canada. Prev. Vet. Med. 2018, 154, 9–17. [Google Scholar] [CrossRef]
- Malla, S.; Dumre, S.P.; Shakya, G.; Kansakar, P.; Rai, B.; Hossain, A.; Nair, G.B.; Albert, M.J.; Sack, D.; Baker, S.; et al. The challenges and successes of implementing a sustainable antimicrobial resistance surveillance programme in Nepal. BMC Public Health 2014, 14, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Meyer, E.; Lapatschek, M.; Bechtold, A.; Schwarzkopf, G.; Gastmeier, P.; Schwab, F. Impact of restriction of third generation cephalosporins on the burden of third generation cephalosporin resistant K. pneumoniae and E. coli in an ICU. Intensive Care Med. 2009, 35, 862–870. [Google Scholar] [CrossRef]
- Micallef, C.; Ashiru-Oredope, D.; Hansraj, S.; Denning, D.W.; Agrawal, S.G.; Manuel, R.J.; Schelenz, S.; Guy, R.; Muller-Pebody, B.; Patel, R.; et al. An investigation of antifungal stewardship programmes in England. J. Med. Microbiol. 2017, 66, 1581–1589. [Google Scholar] [CrossRef]
- Postma, M.; Vanderhaeghen, W.; Sarrazin, S.; Maes, D.; Dewulf, J. Reducing Antimicrobial Usage in Pig Production without Jeopardizing Production Parameters. Zoonoses Public Health 2017, 64, 63–74. [Google Scholar] [CrossRef]
- Clerc, O.; Prod’hom, G.; Senn, L.; Jaton, K.; Zanetti, G.; Calandra, T.; Greub, G. Matrix-assisted laser desorption ionization time-of-flight mass spectrometry and PCR-based rapid diagnosis of Staphylococcus aureus bacteraemia. Clin. Microbiol. Infect. 2014, 20, 355–360. [Google Scholar] [CrossRef] [Green Version]
- Nathwani, D.; Sneddon, J.; Malcolm, W.; Wiuff, C.; Patton, A.; Hurding, S.; Eastaway, A.; Seaton, R.A.; Watson, E.; Gillies, E.; et al. Scottish Antimicrobial Prescribing Group (SAPG): Development and impact of the Scottish National Antimicrobial Stewardship Programme. Int. J. Antimicrob. Agents 2011, 38, 16–26. [Google Scholar] [CrossRef] [Green Version]
- Altorf-van der Kuil, W.; Schoffelen, A.F.; de Greeff, S.C.; Thijsen, S.F.; Alblas, H.J.; Notermans, D.W.; Vlek, A.L.; van der Sande, M.A.; Leenstra, T.; Cohen-Stuart, J.W.T.; et al. National laboratory-based surveillance system for antimicrobial resistance: A successful tool to support the control of antimicrobial resistance in the Netherlands. Eurosurveillance 2017, 22, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deuster, S.; Roten, I.; Muehlebach, S. Implementation of treatment guidelines to support judicious use of antibiotic therapy. J. Clin. Pharm. Ther. 2010, 35, 71–78. [Google Scholar] [CrossRef] [PubMed]
- Fuertes, E.I.; Henry, B.; Marra, F.; Wong, H.; Patrick, D.M. Trends in Antibiotic Utilization in Vancouver Associated With a Community Education Program on Antibiotic Use. Can. J. Public Health 2010, 101, 304. [Google Scholar] [CrossRef]
- Fukuda, T.; Watanabe, H.; Ido, S.; Shiragami, M. Contribution of antimicrobial stewardship programs to reduction of antimicrobial therapy costs in community hospital with 429 Beds --before-after comparative two-year trial in Japan. J. Pharm. Policy Pract. 2014, 7, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Fürst, J.; Čižman, M.; Mrak, J.; Kos, D.; Campbell, S.; Coenen, S.; Gustafsson, L.L.; Fürst, L.; Godman, B. The influence of a sustained multifaceted approach to improve antibiotic prescribing in Slovenia during the past decade: Findings and implications. Expert Rev. Anti. Infect. Ther. 2015, 13, 279–289. [Google Scholar] [CrossRef]
- Gaube, S.; Tsivrikos, D.; Dollinger, D.; Lermer, E. How a smiley protects health: A pilot intervention to improve hand hygiene in hospitals by activating injunctive norms through emoticons. PLoS ONE 2018, 13, e0197465. [Google Scholar] [CrossRef] [Green Version]
- Gottesman, B.S.; Carmeli, Y.; Shitrit, P.; Chowers, M. Impact of quinolone restriction on resistance patterns of Escherichia coli isolated from urine by culture in a community setting. Clin. Infect. Dis. 2009, 49, 869–875. [Google Scholar] [CrossRef] [Green Version]
- Othieno, J.O.; Njagi, O.; Azegele, A. Opportunities and challenges in antimicrobial resistance behavior change communication. One Health 2020, 11, 100171. [Google Scholar] [CrossRef]
- Tompson, A.C.; Chandler, C.I.R. Addressing Antibiotic Use: Insights from Social Science Around the World. A Report Collated with Social Scientists of the Antimicrobials in Society Hub; London School of Hygiene and Tropical Medicine: London, UK, 2021. [Google Scholar]
- Haenssgen, M.J.; Charoenboon, N.; Zanello, G.; Mayxay, M.; Reed-Tsochas, F.; Jones, C.O.H.; Kosaikanont, R.; Praphattong, P.; Manohan, P.; Lubell, Y.; et al. Antibiotics and activity spaces: Protocol of an exploratory study of behaviour, marginalisation and knowledge diffusion. BMJ Glob. Health 2018, 3, 621. [Google Scholar] [CrossRef] [Green Version]
- Lundborg, C.S.; Tamhankar, A.J. Understanding and changing human behaviour-antibiotic mainstreaming as an approach to facilitate modification of provider and consumer behaviour. Ups. J. Med. Sci. 2014, 119, 125–133. [Google Scholar] [CrossRef]
- Rawson, T.M.; Moore, L.S.P.; Tivey, A.M.; Tsao, A.; Gilchrist, M.; Charani, E.; Holmes, A.H. Behaviour change interventions to influence antimicrobial prescribing: A cross-sectional analysis of reports from UK state-of-the-art scientific conferences. Antimicrob. Resist. Infect. Control 2017, 6, 11. [Google Scholar] [CrossRef] [Green Version]
- Kirchhelle, C.; Atkinson, P.; Broom, A.; Chuengsatiansup, K.; Ferreira, J.P.; Fortané, N.; Frost, I.; Gradmann, C.; Hinchliffe, S.; Hoffman, S.J.; et al. Setting the standard: Multidisciplinary hallmarks for structural, equitable and tracked antibiotic policy. BMJ Glob. Health 2020, 5, 1–14. [Google Scholar] [CrossRef]
- Lorencatto, F.; Charani, E.; Sevdalis, N.; Tarrant, C.; Davey, P. Driving Sustainable Change in Antimicrobial Prescribing Practice: How Can Social and Behavioural Sciences Help? Oxford University Press: Oxford, UK, 2018; Volume 73. [Google Scholar]
- Adam, C.J.M.; Fortané, N.; Ducrot, C.; Paul, M.C. Transition Pathways Toward the Prudent Use of Antimicrobials: The Case of Free-Range Broiler Farmers in France. Front. Vet. Sci. 2020, 7, 687. [Google Scholar] [CrossRef]
- Haenssgen, M.J.; Charoenboon, N.; Thavethanutthanawin, P.; Wibunjak, K. Tales of treatment and new perspectives for global health research on antimicrobial resistance. Med. Humanit. 2021, 47, 1–18. [Google Scholar] [CrossRef]
- Duncan, E.M.; Charani, E.; Clarkson, J.E.; Francis, J.J.; Gillies, K.; Grimshaw, J.M.; Kern, W.V.; Lorencatto, F.; Marwick, C.A.; McEwen, J.; et al. A behavioural approach to specifying interventions: What insights can be gained for the reporting and implementation of interventions to reduce antibiotic use in hospitals? J. Antimicrob. Chemother. 2020, 75, 1338–1346. [Google Scholar] [CrossRef]
- Papoutsi, C.; Mattick, K.; Pearson, M.; Brennan, N.; Briscoe, S.; Wong, G. Social and professional influences on antimicrobial prescribing for doctors-in-training: A realist review. J. Antimicrob. Chemother. 2017, 72, 2418–2430. [Google Scholar] [CrossRef] [Green Version]
- Ashley, E.A.; Recht, J.; Chua, A.; Dance, D.; Dhorda, M.; Thomas, N.V.; Ranganathan, N.; Turner, P.; Guerin, P.J.; White, N.J.; et al. An inventory of supranational antimicrobial resistance surveillance networks involving low- and middle-income countries since 2000. J. Antimicrob. Chemother. 2018, 73, 1737–1749. [Google Scholar] [CrossRef]
- Fournier, C.; Nordmann, P.; Pittet, O.; Poirel, L. Does an Antibiotic Stewardship Applied in a Pig Farm Lead to Low ESBL Prevalence? Antibiotics 2021, 10, 574. [Google Scholar] [CrossRef]
- Jonas, O.B.; Irwin, A.; Berthe, F.C.J.; Le Gall, F.G.; Marquez, P.V. Drug-Resistant Infections: A Threat to our Economic Future: Final Report; World Bank Group: Washington, DC, USA, 2017; Volume 2. [Google Scholar]
- Nowell, L.S.; Norris, J.M.; White, D.E.; Moules, N.J. Thematic Analysis: Striving to Meet the Trustworthiness Criteria. Int. J. Qual. Methods 2017, 16, 160940691773384. [Google Scholar] [CrossRef]
- Burnham, J.P.; Geng, E.; Venkatram, C.; Colditz, G.A.; McKay, V.R. Putting the dissemination and implementation in infectious diseases. Clin. Infect. Dis. 2020, 71, 218–225. [Google Scholar] [CrossRef]
- Tabak, R.G.; Khoong, E.C.; Chambers, D.A.; Brownson, R.C. Bridging research and practice: Models for dissemination and implementation research. Am. J. Prev. Med. 2012, 43, 337–350. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hanefeld, J.; Mayhew, S.; Legido-Quigley, H.; Martineau, F.; Karanikolos, M.; Blanchet, K.; Liverani, M.; Yei Mokuwa, E.; McKay, G.; Balabanova, D. Towards an understanding of resilience: Responding to health systems shocks. Health Policy Plan. 2018, 33, 355–367. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Brien, B.C.; Harris, I.B.; Beckman, T.J.; Reed, D.A.; Cook, D.A. Standards for reporting qualitative research: A synthesis of recommendations. Acad. Med. 2014, 89, 1245–1251. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Component [15] | Variables [15] | Categories | N | Percentage | ||||
|---|---|---|---|---|---|---|---|---|
| Respondent * | Profile | Medical doctor and University Professor | 7 | 33% | ||||
| Researcher | 6 | 29% | ||||||
| Public Health Epidemiologist | 4 | 19% | ||||||
| University Professor (Pharmacist/Veterinarian) | 2 | 10% | ||||||
| Medical doctor | 2 | 10% | ||||||
| Publication | Year | Before 2010 | 5 | 24% | ||||
| 2010–2014 | 8 | 38% | ||||||
| 2015–2019 | 8 | 38% | ||||||
| Quality of description | Sufficient | (Detailed) | 14 | 5 | 67% | 24% | ||
| (Good) | 5 | 24% | ||||||
| (Succinct) | 4 | 19% | ||||||
| Vague | 7 | 33% | ||||||
| Social system | Economic scale | High-income countries | 20 | 95% | ||||
| Low-middle-income countries (Nepal) | 1 | 5% | ||||||
| Spatial scale | Europe | 13 | 62% | |||||
| Asia (Japan, Israel, and Nepal) | 4 | 19% | ||||||
| North America (US and CA) | 3 | 14% | ||||||
| Australia | 1 | 5% | ||||||
| Sector scale | Human sector | 14 | 67% | |||||
| Animal sector | 3 | 14% | ||||||
| Human, Animal, Food sectors (“OH”) | 3 | 14% | ||||||
| Animal and Food sectors | 1 | 5% | ||||||
| Time scale | Start | Before 2010 | 14 | 67% | ||||
| 2010–2014 | 5 | 24% | ||||||
| 2015–2019 | 2 | 10% | ||||||
| End | Delimited | 9 | 43% | |||||
| Ongoing/without end | 12 | 57% | ||||||
| Governance | Agents responsible | Public sector (government owned) | 17 | 81% | ||||
| Private sector (private owned) | 1 | 5% | ||||||
| Academic sector (research/scientific sector) | 1 | 5% | ||||||
| Public and Private sector | 1 | 5% | ||||||
| Public and academic sector | 1 | 5% | ||||||
| Level of funding | Specific funding | Public funding | 11 | 10 | 52% | 48% | ||
| Private funding | 1 | 5% | ||||||
| Without funding | 10 | 48% | ||||||
| Constitution | Positive: initiate or improve | 18 | 86% | |||||
| Negative: refrain or prevent | 3 | 14% | ||||||
| Policy instrument | Information/awareness | 14 | 67% | |||||
| Regulations | 4 | 19% | ||||||
| Information/awareness and regulations | 3 | 14% | ||||||
| Trigger/goals | Trigger of the intervention | Pressure on AMR (high AMU) | 6 | 29% | ||||
| State of AMR (increase of AMR) | 4 | 19% | ||||||
| Driver of AMR | 3 | 14% | ||||||
| Impact of AMR (mortality/morbidity) | 3 | 14% | ||||||
| Pressure and impact of AMR | 3 | 14% | ||||||
| Pressure and state of AMR | 2 | 10% | ||||||
| Trigger type | Reactive | 12 | 57% | |||||
| Preventive | 9 | 43% | ||||||
| Main goal towards intervention | Initiate an action | 15 | 71% | |||||
| Improve an action | 5 | 24% | ||||||
| Maintain an action | 1 | 5% | ||||||
| Main strategy | Reduce AMU | 12 | 57% | |||||
| Surveillance | 6 | 29% | ||||||
| Infection prevention | 2 | 10% | ||||||
| Innovation | 1 | 5% | ||||||
| System intervention | Low leverage point | 20 | 95% | |||||
| High leverage point | 1 | 5% | ||||||
| Level of implementation | National | 13 | 62% | |||||
| Local | 5 | 24% | ||||||
| Sub-national or Regional | 3 | 14% | ||||||
| Bio-ecological scale | Type of microorganism | Bacteria | 16 | 76% | ||||
| No specific | 4 | 19% | ||||||
| Fungi | 1 | 5% | ||||||
| Level of resistance | Unknown | 12 | 57% | |||||
| MDR | 8 | 38% | ||||||
| SDR | 1 | 5% | ||||||
| Resistance coming from plasmids | Unknown or not specified | 15 | 71% | |||||
| Yes | 5 | 24% | ||||||
| No | 1 | 5% | ||||||
| Host carrier of AMR microorganism | Human | 14 | 67% | |||||
| Animal | 4 | 19% | ||||||
| Human, animal, and/or food | 3 | 14% | ||||||
| Main transmission of resistance | Human to human | 10 | 48% | |||||
| Unknown/Not specified | 7 | 33% | ||||||
| Animal or Food to human | 2 | 10% | ||||||
| Human, animal, or food to human | 1 | 5% | ||||||
| Environment or human to human | 1 | 5% | ||||||
| Origin of infection | Not applicable | 11 | 52% | |||||
| Healthcare associated | 6 | 29% | ||||||
| Community acquired | 3 | 14% | ||||||
| Healthcare or community acquired | 1 | 5% | ||||||
| Climate | Temperate | 19 | 91% | |||||
| Arid/Temperate | 2 | 10% | ||||||
| Assessment | Cost-effectiveness | Not evaluated | 17 | 81% | ||||
| Evaluated | 4 | 19% | ||||||
| Main outcome | Pressure: Reduction in AMU | 10 | 48% | |||||
| State: Reduction in AMR prevalence | 6 | 29% | ||||||
| Impact: Less morbidity and mortality | 3 | 14% | ||||||
| Drivers: Improvement in sanitation | 2 | 10% | ||||||
| Outcome(s) perception or evaluation | Positive | 16 | 76% | |||||
| Positive and negative | 4 | 19% | ||||||
| Not reported/neutral | 1 | 5% | ||||||
| Unintended outcomes | Not reported | 14 | 67% | |||||
| Reported | 7 | 33% | ||||||
| Sub-Theme | Theme | Total FREQ | Partial FREQ | Meaning and Assumptions | Implications | Quotes | |
|---|---|---|---|---|---|---|---|
| SF | OB | ||||||
| Reinforcement of correct behaviour, new mentality, or changes | Behaviour | 10 | 6 | 4 | New routines or ideas must be reinforced to ensure their continuity. Habituation needs time and going back to old routines due to inertia is usual. | Training and guidance are essential to make changes in the long term. Follow-up and regular feedback maintain motivation. Sustained efforts and sustained interventions are needed to avoid old habits. Use of new technologies (emoticons or mass media) as reminders. | “change in mentality should also be seen as one of the key success factors of this study” // “There is a human tendency to return to previous practices in the absence of constant motivation and reminders” // “Inertia among prescribers” |
| Financial resources * | Capacity | 10 | 5 | 5 | Enough budget and funding to carry out the intervention. Funding for teaching and training the main actors responsible for the intervention. | Good level of funding is crucial for implementing interventions. Costs can be very high including training, personnel, or resources and, without a proper budget, many of them are not going forward. | “Coaching of farmers” // “clinically oriented education through symposia, workshops and focused meetings at the regional and local levels” // “funding” // “budget to begin with” or “very costly to establish” |
| Assessment | Intervention | 9 | 9 | 0 | After the intervention has taken place or, for a defined period of the ongoing intervention, checking or measuring outcomes of the actions applied can help to elucidate the usefulness of the intervention or its possible gaps. | Results from assessment can help to maintain motivation and to identify new goals and opportunities to improve outcomes or to promote actions impacting AMR. | “results from the monitoring were used when writing guidelines” // “a decline of 26.5% in the number of antibiotic prescriptions was observed over 5 years” // “significantly increased the usage of hand-rub dispensers in patient rooms, in comparison to the three other tested conditions” |
| Awareness | Information | 9 | 6 | 3 | Knowledge about AMR and people aware of the problem of untreatable infections enhance positive outcomes. Ignorance of the problem may lead to opposition of public opinion or citizenship (e.g., lack of prescription thought as cutback in health system) | Society may behave differently following and finishing prescribed antimicrobial treatments. Prescribers less pressured to prescribe treatments to please patients or farmers. Citizenship engage to preserve antimicrobial effectiveness. | “Patients who insisted on receiving antibiotics” // “Health beliefs by the general populations” // “general reluctance amongst farmers and veterinarians to change their existing antimicrobial treatment practices” // “advisor/coach helps the farmer with explaining what he/she could be improving and what the risk is when certain practices are not performed correctly” |
| Knowledge, skills and education | Capacity | 9 | 9 | 0 | Deep and detailed knowledge or education increases system capacity to carry out the intervention. | Contribution and expansion of skills and knowledge to new staff or new performers of interventions. Impede waning of the intervention. | “investment in technical and epidemiological knowledge” // “The programme created a pool of trained technicians who can compensate for transfer and separation of staff and contribute to expansion of programme staff”// “advisor/coach helps the farmer with explaining what he/she could be improving and what the risk is when certain practices are not performed correctly” |
| Trust and support | Behaviour | 8 | 4 | 4 | Trust and support of main actors. On the contrary, prejudices and scepticism hamper good outcomes. | They enhance implementation and maintenance of interventions. | “supported by the key doctors of the ICU” // “Sustained efforts and trust of infectious disease pharmacists” // “Perception of the farmer that interventions cost money and time (although often not the case as proven in our studies) |
| Training | Institution | 8 | 8 | 0 | Professional training of the actions to improve or initiate in the intervention. | Training empower and increase self-esteem to carry out interventions, especially when actors are not familiar on a daily basis with AMR. Often, this training is funded. | “Training of GPs”// “The programme created a pool of trained technicians who can compensate for transfer and separation of staff and contribute to expansion of programme staff” // “farmers keep control over the health situation and are less reluctant to change certain AMU treatment procedures” // “pump priming investment to support development of pharmacists” |
| Multifaceted/Multisector | Intervention | 8 | 8 | 0 | Intervention is composed or carried out by different sectors, settings, departments, or professionals | Interventions not only affect one type of actors or sectors. Joining efforts from different backgrounds and perspectives may have bigger impacts, reach, and redundancy of interventions. Some tasks can be carried out or complemented by different agents for completion | “Involving community pharmacists, care homes, nursing homes staff in this process and using training and care pathways” // “Intensive collaboration between the surveillance team and the medical microbiologists” // “close collaboration between the animal and human sector and between experts and political stakeholders or authorities” |
| Consultation and guidance | Implementation | 8 | 7 | 1 | Consultation or guidance for intervention implementation clarify actions and objectives of the intervention. Consultation and guidance available for actors. When lacking, often implies insecurity towards the intervention and actors can go back to old habits | This tool during implementation or during the intervention enhances positive outcomes as they can rely on experts or other professionals’ criteria when doubts arise. It promotes self-esteem and motivation of executors due to continuous knowledge, feedback and follow-ups | “development of practical implementation guidance” // “advice from the Expert Advisory Group on Antimicrobial Resistance ceased in 2004” // “to achieve this (AMU) reduction, it is important to assist and guide farmers in this process” |
| Collaborative | Behaviour | 7 | 4 | 3 | Collaboration between main actors enhances implementation and communication. In contrast, reluctance to participate due to fear of consequences that may not reflect reality hinder implementation | A collaborative behaviour is crucial to involve individuals into the fight of AMR, especially those coming from private sectors. Popular beliefs and ignorance can jeopardise the designed intervention | “It came from industry and therefore was well adopted” // “There still exist hesitance among slaughterhouses to participate due to the fear of losing customers, if resistant bacteria are found” // “recruitment of herds was difficult, despite the efforts made to promote this study and the possibility for farmers to collaborate free of charge” |
| Engagement/support | Institution | 7 | 6 | 1 | Compromise towards the intervention not only from individuals but also from the institutions designing, implementing, or performing the intervention | Ensures effort from the institution to maintain or to carry out the intervention, independently of individual governances. | “Implementation had the support of heads of both departments” or “the veterinarian has often already been the advisor for years resulting in the loss of motivation due to, for example persistent disease problems” |
| Data collection and provision | Information | 7 | 5 | 2 | Data collection and provision standardised, available, and shared. In contrast, data collected or provided from different sites, with heterogeneous criteria or not shared hinders availability of knowledge | Data of interventions that are shared, with standard reporting, can clarify the exact situation of the epidemiological state; these can be used by different settings or sectors and can clarify and/or quantify assessments. | “This integrated program was made possible because access to all relevant data and samples that were already systematically collected from animals, food, and humans has been shared” // “number of tools to make surveillance findings transparent and accessible to both scientists and non-specialists” // “Diversity in coding in laboratory information systems” |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Graells, T.; Lambraki, I.A.; Cousins, M.; Léger, A.; Lillepold, K.; Henriksson, P.J.G.; Troell, M.; Carson, C.A.; Parmley, E.J.; Majowicz, S.E.; et al. Studying Factors Affecting Success of Antimicrobial Resistance Interventions through the Lens of Experience: A Thematic Analysis. Antibiotics 2022, 11, 639. https://doi.org/10.3390/antibiotics11050639
Graells T, Lambraki IA, Cousins M, Léger A, Lillepold K, Henriksson PJG, Troell M, Carson CA, Parmley EJ, Majowicz SE, et al. Studying Factors Affecting Success of Antimicrobial Resistance Interventions through the Lens of Experience: A Thematic Analysis. Antibiotics. 2022; 11(5):639. https://doi.org/10.3390/antibiotics11050639
Chicago/Turabian StyleGraells, Tiscar, Irene A. Lambraki, Melanie Cousins, Anaïs Léger, Kate Lillepold, Patrik J. G. Henriksson, Max Troell, Carolee A. Carson, Elizabeth Jane Parmley, Shannon E. Majowicz, and et al. 2022. "Studying Factors Affecting Success of Antimicrobial Resistance Interventions through the Lens of Experience: A Thematic Analysis" Antibiotics 11, no. 5: 639. https://doi.org/10.3390/antibiotics11050639