
Clostridioides difficile Toxin B PCR Cycle Threshold as a Predictor of Toxin Testing in Stool Specimens from Hospitalized Adults

Abstract
:1. Introduction
2. Results
2.1. Patient Demographics
2.2. Summary Statistics
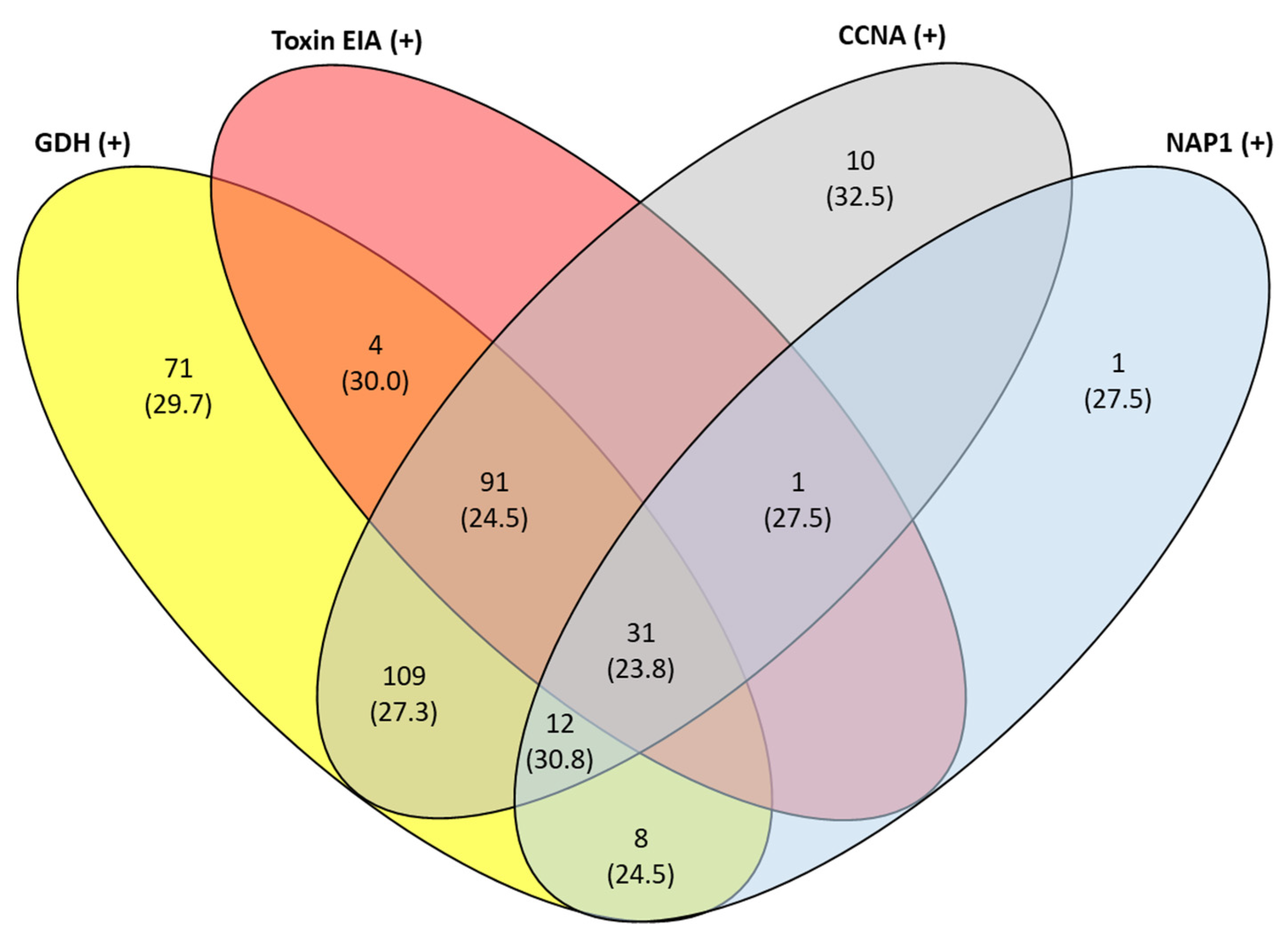
2.3. Cycle Threshold Value and GDH, Toxin EIA, and CCNA Results
2.4. Use of tcdB Ct Value as an Indicator of Toxin Results
3. Discussion
4. Materials and Methods
4.1. Specimen Inclusion Criteria
4.2. Data Collection and C. difficile Test Methods
4.3. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Magill, S.S.; Edwards, J.R.; Bamberg, W.; Beldavs, Z.G.; Dumyati, G.; Kainer, M.A.; Lynfield, R.; Maloney, M.; McAllister-Hollod, L.; Nadle, J.; et al. Multistate point-prevalence survey of health care-associated infections. N. Engl. J. Med. 2014, 370, 1198–1208. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Prehn, J.; Reigadas, E.; Vogelzang, E.H.; Bouza, E.; Hristea, A.; Guery, B.; Krutova, M.; Norén, T.; Allerberger, F.; Coia, J.; et al. European Society of Clinical Microbiology and Infectious Diseases: 2021 update on the treatment guidance document for Clostridioides difficile infection in adults. Clin. Microbiol. Infect. 2021, 27 (Suppl. S2), S1–S21. [Google Scholar] [CrossRef] [PubMed]
- Planche, T.D.; Davies, K.A.; Coen, P.G.; Finney, J.M.; Monahan, I.M.; Morris, K.A.; O’Connor, L.; Oakley, S.J.; Pope, C.F.; Wren, M.W.; et al. Differences in outcome according to Clostridium difficile testing method: A prospective multicentre diagnostic validation study of C difficile infection. Lancet Infect. Dis. 2013, 13, 936–945. [Google Scholar] [CrossRef] [Green Version]
- Planche, T.; Aghaizu, A.; Holliman, R.; Riley, P.; Poloniecki, J.; Breathnach, A.; Krishna, S. Diagnosis of Clostridium difficile in-fection by toxin detection kits: A systematic review. Lancet Infect. Dis. 2008, 8, 777–784. [Google Scholar] [CrossRef]
- Longtin, Y.; Trottier, S.; Brochu, G.; Paquet-Bolduc, B.; Garenc, C.; Loungnarath, V.; Beaulieu, C.; Goulet, D.; Longtin, J. Impact of the Type of Diagnostic Assay on Clostridium difficile Infection and Complication Rates in a Mandatory Reporting Program. Clin. Infect. Dis. 2012, 56, 67–73. [Google Scholar] [CrossRef] [Green Version]
- Dionne, L.L.; Raymond, F.; Corbeil, J.; Longtin, J.; Gervais, P.; Longtin, Y. Correlation between Clostridium difficile bacterial load, commercial real-time PCR cycle thresholds, and results of diagnostic tests based on enzyme immunoassay and cell culture cytotoxicity assay. J. Clin. Microbiol. 2013, 51, 3624–3630. [Google Scholar] [CrossRef] [Green Version]
- Leslie, J.L.; Cohen, S.H.; Solnick, J.V.; Polage, C.R. Role of fecal Clostridium difficile load in discrepancies between toxin tests and PCR: Is quantitation the next step in C. difficile testing? Eur. J. Clin. Microbiol. Infect. Dis. 2012, 31, 3295–3299. [Google Scholar] [CrossRef] [Green Version]
- Senchyna, F.; Gaur, R.L.; Gombar, S.; Truong, C.Y.; Schroeder, L.F.; Banaei, N. Clostridium difficile PCR Cycle Threshold Predicts Free Toxin. J. Clin. Microbiol. 2017, 55, 2651–2660. [Google Scholar] [CrossRef] [Green Version]
- Kamboj, M.; Brite, J.; McMillen, T.; Robilotti, E.; Herrera, A.; Sepkowitz, K.; Babady, N.E. Potential of real-time PCR threshold cycle (C(T)) to predict presence of free toxin and clinically relevant C. difficile infection (CDI) in patients with cancer. J. Infect. 2018, 76, 369–375. [Google Scholar] [CrossRef]
- Ashraf, Z.; Rahmati, E.; Bender, J.M.; Nanda, N.; She, R.C. GDH and toxin immunoassay for the diagnosis of Clostridioides (Clostridium) difficile infection is not a ‘one size fit all’ screening test. Diagn. Microbiol. Infect. Dis. 2018, 94, 109–112. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Short Summary: Testing for C. difficile and Standardized Infection Ratios, National Healthcare Safety Network. 2019. Available online: https://www.cdc.gov/nhsn/pdfs/ps-analysis-resources/Cdiff-testing-sir-508.pdf (accessed on 24 February 2022).
- Bagdasarian, N.; Rao, K.; Malani, P.N. Diagnosis and treatment of Clostridium difficile in adults: A systematic review. JAMA 2015, 313, 398–408. [Google Scholar] [CrossRef] [PubMed]
- Wilmore, S.; Goldenberg, S.D. Potential of real-time PCR threshold cycle (CT) to predict presence of free toxin and clinically relevant C. difficile infection (CDI) in patients with cancer: A reply. J. Infect. 2018, 76, 424–426. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tenover, F.C.; Novak-Weekley, S.; Woods, C.W.; Peterson, L.R.; Davis, T.; Schreckenberger, P.; Fang, F.C.; Dascal, A.; Gerding, D.N.; Nomura, J.H.; et al. Impact of Strain Type on Detection of Toxigenic Clostridium difficile: Comparison of Molecular Diagnostic and Enzyme Immunoassay Approaches. J. Clin. Microbiol. 2010, 48, 3719–3724. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rizzardi, K.; Åkerlund, T.; Norén, T.; Matussek, A. Impact of ribotype on Clostridioides difficile diagnostics. Eur. J. Clin. Microbiol. 2020, 39, 847–853. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Quinn, C.D.; Sefers, S.E.; Babiker, W.; He, Y.; Alcabasa, R.; Stratton, C.W.; Carroll, K.C.; Tang, Y.-W.C. Diff Quik Chek Complete Enzyme Immunoassay Provides a Reliable First-Line Method for Detection of Clostridium difficile in Stool Specimens. J. Clin. Microbiol. 2010, 48, 603–605. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chung, H.-S.; Lee, M. Evaluation of the performance of C. DIFF QUIK CHEK COMPLETE and its usefulness in a hospital setting with a high prevalence of Clostridium difficile infection. J. Investig. Med. 2017, 65, 88–92. [Google Scholar] [CrossRef]
- Larson, A.M.; Fung, A.M.; Fang, F.C. Evaluation of tcdB Real-Time PCR in a Three-Step Diagnostic Algorithm for Detection of Toxigenic Clostridium difficile. J. Clin. Microbiol. 2010, 48, 124–130. [Google Scholar] [CrossRef] [Green Version]
- Gomez, E.J.; Montgomery, S.; Alby, K.; Robinson, D.P.; Roundtree, S.S.; Blecker-Shelly, D.; Sullivan, K.V. Poor yield of Clostridium difficile testing algorithms using glutamate dehydrogenase antigen and C. difficile toxin enzyme immunoassays in a pediatric population with declining prevalence of clostridium difficile strain BI/NAP1/027. Diagn. Microbiol. Infect. Dis. 2018, 91, 229–232. [Google Scholar] [CrossRef]
- Shah, M.D.; Balada-Llasat, J.-M.; Coe, K.; Reed, E.; Sandlund, J.; Pancholi, P. Evaluation of Cycle Threshold, Toxin Concentration, and Clinical Characteristics of Clostridioides difficile Infection in Patients with Discordant Diagnostic Test Results. J. Clin. Microbiol. 2020, 58, e01681-19. [Google Scholar] [CrossRef]
- Hitchcock, M.M.; Holubar, M.; Hogan, C.A.; Tompkins, L.S.; Banaei, N. Dual Reporting of Clostridioides difficile PCR and Pre-dicted Toxin Result Based on PCR Cycle Threshold Reduces Treatment of Toxin-Negative Patients without Increases in Ad-verse Outcomes. J. Clin. Microbiol. 2019, 57, e01288-19. [Google Scholar] [CrossRef] [Green Version]
- Bai, Y.; Sun, X.; Jin, Y.; Wang, Y.; Li, J. Accuracy of Xpert Clostridium difficile assay for the diagnosis of Clostridium difficile infection: A meta analysis. PLoS ONE 2017, 12, e0185891. [Google Scholar] [CrossRef] [PubMed]
- Deshpande, A.; Pasupuleti, V.; Rolston, D.D.; Jain, A.; Deshpande, N.; Pant, C.; Hernandez, A.V. Diagnostic accuracy of re-al-time polymerase chain reaction in detection of Clostridium difficile in the stool samples of patients with suspected Clostridium difficile Infection: A meta-analysis. Clin. Infect. Dis. 2011, 53, e81–e90. [Google Scholar] [CrossRef] [PubMed]
- Reigadas, E.; Alcalá, L.; Valerio, M.; Marín, M.; Martin, A.; Bouza, E. Toxin B PCR cycle threshold as a predictor of poor out-come of Clostridium difficile infection: A derivation and validation cohort study. J. Antimicrob. Chemother. 2016, 71, 1380–1385. [Google Scholar] [CrossRef] [Green Version]
- De Francesco, M.A.; Lorenzin, G.; Piccinelli, G.; Corbellini, S.; Bonfanti, C.; Caruso, A. Correlation between tcdB gene PCR cycle threshold and severe Clostridium difficile disease. Anaerobe 2019, 59, 141–144. [Google Scholar] [CrossRef] [PubMed]
- Origüen, J.; Orellana, M.Á.; Fernández-Ruiz, M.; Corbella, L.; San Juan, R.; Ruiz-Ruigómez, M.; López-Medrano, F.; Lizasoain, M.; Ruiz-Merlo, T.; Maestro-de la Calle, G.; et al. Toxin B PCR Amplification Cycle Thresh-old Adds Little to Clinical Variables for Predicting Outcomes in Clostridium difficile Infection: A Retrospective Cohort Study. J. Clin. Microbiol. 2019, 57, e01125-18. [Google Scholar] [CrossRef] [Green Version]
- Garvey, M.I.; Bradley, C.W.; Wilkinson, M.A.; Holden, E. Can a toxin gene NAAT be used to predict toxin EIA and the severity of Clostridium difficile infection? Antimicrob. Resist Infect. Control 2017, 6, 127. [Google Scholar] [CrossRef] [Green Version]
- Doolan, C.P.; Louie, T.; Lata, C.; Larios, O.E.; Stokes, W.; Kim, J.; Brown, K.; Beck, P.; Deardon, R.; Pillai, D.R. Latent Class Analysis for the Diagnosis of Clostridioides difficile Infection. Clin. Infect. Dis. 2020, 73, e2673–e2679. [Google Scholar] [CrossRef]
- Scardina, T.; Labuszewski, L.; Pacheco, S.; Adams, W.; Schreckenberger, P.; Johnson, S. Clostridium difficile Infection (CDI) Severity and Outcome among Patients Infected with the NAP1/BI/027 Strain in a Non-Epidemic Setting. Infect. Control Hosp. Epidemiol. 2015, 36, 280–286. [Google Scholar] [CrossRef]
- Katz, K.C.; Golding, G.R.; Choi, K.B.; Pelude, L.; Amaratunga, K.R.; Taljaard, M.; Alexandre, S.; Collet, J.C.; Davis, I.; Du, T.; et al. The evolving epidemiology of Clostridium difficile infection in Canadian hospitals during a postepidemic period (2009–2015). Can. Med Assoc. J. 2018, 190, E758–E765. [Google Scholar] [CrossRef] [Green Version]
- Sirard, S.; Valiquette, L.; Fortier, L.-C. Lack of Association between Clinical Outcome of Clostridium difficile Infections, Strain Type, and Virulence-Associated Phenotypes. J. Clin. Microbiol. 2011, 49, 4040–4046. [Google Scholar] [CrossRef] [Green Version]
- Warny, M.; Pepin, J.; Fang, A.; Killgore, G.; Thompson, A.; Brazier, J.; Frost, E.; McDonald, L.C. Toxin production by an emerging strain of Clostridium difficile associated with outbreaks of severe disease in North America and Europe. Lancet 2005, 366, 1079–1084. [Google Scholar] [CrossRef]
- Kwon, J.H.; Reske, K.A.; Hink, T.; Burnham, C.-A.D.; Dubberke, E.R. Evaluation of Correlation between Pretest Probability for Clostridium difficile Infection and Clostridium difficile Enzyme Immunoassay Results. J. Clin. Microbiol. 2017, 55, 596–605. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caroff, D.A.; Edelstein, P.H.; Hamilton, K.; Pegues, D.A.; CDC Prevention Epicenters Program. The Bristol Stool Scale and Its Relationship to Clostridium difficile Infection. J. Clin. Microbiol. 2014, 52, 3437–3439. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Medical Condition | n (%) |
|---|---|
| Malignancy | 105 (28.5) |
| Hematologic | 15 (4.1) |
| Non-hematologic | 90 (24.5) |
| Solid organ transplant | 64 (17.4) |
| Hematopoietic stem cell transplant | 23 (6.3) |
| Surgical procedure | 97 (20.4) |
| Neurosurgery | 22 (6.0) |
| Abdominal | 29 (7.9) |
| Cardiovascular | 26 (7.1) |
| Orthopedic | 8 (1.6) |
| Urologic | 4 (1.1) |
| Other | 8 (2.2) |
| Cardiovascular disease | 20 (5.4) |
| Hepatic failure | 17 (4.6) |
| Inflammatory bowel disease | 15 (4.1) |
| Gastrointestinal disease (non-surgical) | 9 (2.4) |
| Non-cancerous neoplasm | 5 (1.4) |
| Other conditions | 13 (3.5) |
| Total | 368 (100) |
| n | Median (Mean) Ct | p-Value a | |
|---|---|---|---|
| GDH-positive | 326 | 27.5 (27.3) | <0.001 |
| GDH-negative | 42 | 32.9 (32.7) | |
| Toxin EIA-positive | 127 | 25.0 (24.5) b | <0.001 |
| Toxin EIA-negative | 241 | 29.5 (29.7) | |
| CCNA-positive | 254 | 25.8 (26.6) b | <0.001 |
| CCNA-negative | 114 | 31.5 (30.9) | |
| NAP1-presumptive positive | 53 | 25.3 (26.9) | 0.056 |
| NAP1-negative | 315 | 27.7 (28.1) | |
| All samples | 368 | 27.5 (27.9) | NA |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, S.; Nanda, N.; Yamaguchi, K.; Lee, Y.; She, R.C. Clostridioides difficile Toxin B PCR Cycle Threshold as a Predictor of Toxin Testing in Stool Specimens from Hospitalized Adults. Antibiotics 2022, 11, 576. https://doi.org/10.3390/antibiotics11050576
Lee S, Nanda N, Yamaguchi K, Lee Y, She RC. Clostridioides difficile Toxin B PCR Cycle Threshold as a Predictor of Toxin Testing in Stool Specimens from Hospitalized Adults. Antibiotics. 2022; 11(5):576. https://doi.org/10.3390/antibiotics11050576
Chicago/Turabian StyleLee, Sean, Neha Nanda, Kenichiro Yamaguchi, Yelim Lee, and Rosemary C. She. 2022. "Clostridioides difficile Toxin B PCR Cycle Threshold as a Predictor of Toxin Testing in Stool Specimens from Hospitalized Adults" Antibiotics 11, no. 5: 576. https://doi.org/10.3390/antibiotics11050576