
Comparative Risk of Acute Kidney Injury Following Concurrent Administration of Vancomycin with Piperacillin/Tazobactam or Meropenem: A Systematic Review and Meta-Analysis of Observational Studies

 , ,
, ,
Abstract
:1. Introduction
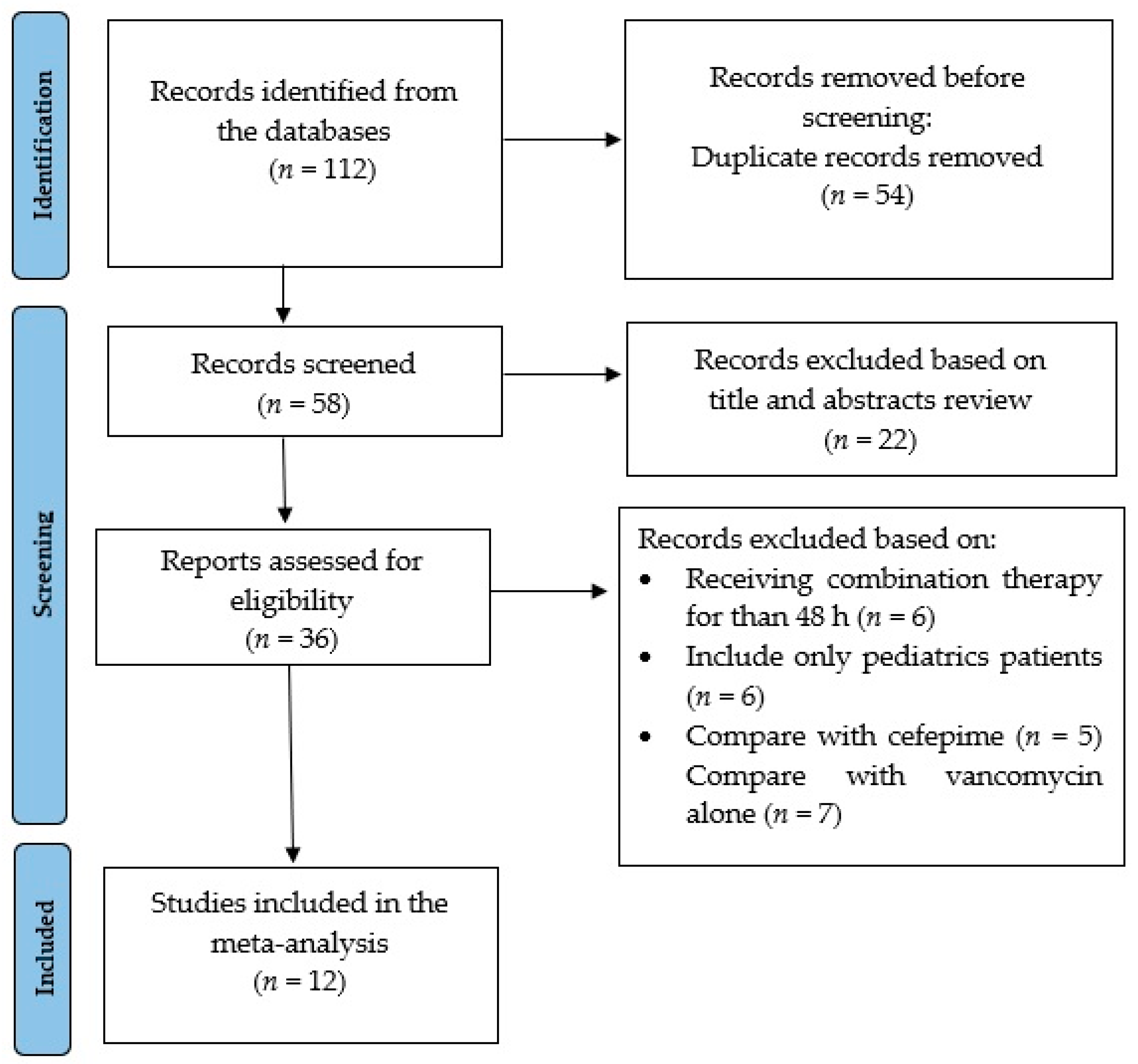
2. Materials and Methods
2.1. Data Source and Search Strategy
2.2. Study Selection
2.3. Data Extraction, Risk of Bias Assessment, and Statistical Analysis
3. Results
3.1. Study Characteristics
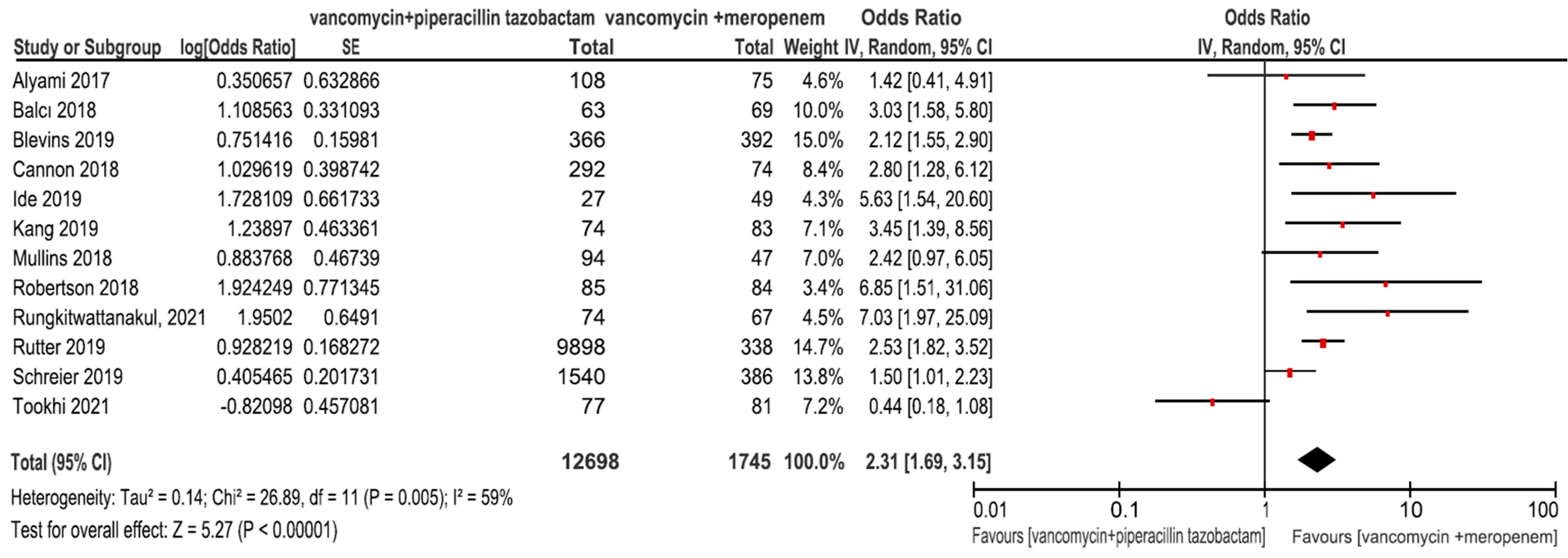
3.2. Outcomes from the Main Analysis
3.2.1. AKI
3.2.2. LOS in Hospital
3.2.3. Renal Replacement Therapy (RRT)
3.2.4. Mortality
3.3. Outcomes from the Subgroup Analyses Based on Clinical Setting
3.3.1. AKI
3.3.2. LOS in Hospital
3.3.3. Renal Replacement Therapy (RRT)
3.3.4. Mortality
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Disclaimer
References
- Sawada, A.; Kawanishi, K.; Morikawa, S.; Nakano, T.; Kodama, M.; Mitobe, M.; Taneda, S.; Koike, J.; Ohara, M.; Nagashima, Y.; et al. Biopsy-proven vancomycin-induced acute kidney injury: A case report and literature review. BMC Nephrol. 2018, 19, 72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dasta, J.F.; Kane-Gill, S. Review of the Literature on the Costs Associated with Acute Kidney Injury. J. Pharm. Pract. 2019, 32, 292–302. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.E.; Muntner, P.; Chertow, G.M.; Warnock, D.G. Acute kidney injury and mortality in hospitalized patients. Am. J. Nephrol. 2012, 35, 349–355. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liangos, O.; Wald, R.; O’Bell, J.W.; Price, L.; Pereira, B.J.; Jaber, B.L. Epidemiology and outcomes of acute renal failure in hospitalized patients: A national survey. Clin. J. Am. Soc. Nephrol. 2006, 1, 43–51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Uchino, S.; Kellum, J.A.; Bellomo, R.; Doig, G.S.; Morimatsu, H.; Morgera, S.; Schetz, M.; Tan, I.; Bouman, C.; Macedo, E.; et al. Acute renal failure in critically ill patients: A multinational, multicenter study. JAMA 2005, 294, 813–818. [Google Scholar] [CrossRef] [Green Version]
- Chertow, G.M.; Burdick, E.; Honour, M.; Bonventre, J.V.; Bates, D.W. Acute kidney injury, mortality, length of stay, and costs in hospitalized patients. J. Am. Soc. Nephrol. 2005, 16, 3365–3370. [Google Scholar] [CrossRef] [Green Version]
- Metnitz, P.G.H.; Krenn, C.G.; Steltzer, H.; Lang, T.; Ploder, J.; Lenz, K.; Le Gall, J.-R.; Druml, W. Effect of acute renal failure requiring renal replacement therapy on outcome in critically ill patients. Crit. Care Med. 2002, 30, 2051–2058. [Google Scholar] [CrossRef]
- Coca, S.G.; Yalavarthy, R.; Concato, J.; Parikh, C.R. Biomarkers for the diagnosis and risk stratification of acute kidney injury: A systematic review. Kidney Int. 2008, 73, 1008–1016. [Google Scholar] [CrossRef] [Green Version]
- Davies, S.W.; Guidry, C.A.; Petroze, R.T.; Hranjec, T.; Sawyer, R.G. Vancomycin and nephrotoxicity: Just another myth? J. Trauma Acute Care Surg. 2013, 75, 830–835. [Google Scholar] [CrossRef] [Green Version]
- Elyasi, S.; Khalili, H.; Dashti-Khavidaki, S.; Mohammadpour, A. Vancomycin-induced nephrotoxicity: Mechanism, incidence, risk factors and special populations. A literature review. Eur. J. Clin. Pharmacol. 2012, 68, 1243–1255. [Google Scholar] [CrossRef]
- Contreiras, C.; Legal, M.; Lau, T.T.; Thalakada, R.; Shalansky, S.; Ensom, M.H. Identification of risk factors for nephrotoxicity in patients receiving extended-duration, high-trough vancomycin therapy. Can. J. Hosp. Pharm. 2014, 67, 126–132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bourget, P.; Hulin, A.; Reveillé, R.; Bever, H.; Carsin, H. Clinical pharmacokinetics of piperacillin-tazobactam combination in patients with major burns and signs of infection. Antimicrob. Agents Chemother. 1996, 40, 139–145. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, T.; Kandiah, S.; Patel, M.; Rab, S.; Wong, J.; Xue, W.; Easley, K.; Anderson, A.M. Risk factors for kidney injury during vancomycin and piperacillin/tazobactam administration, including increased odds of injury with combination therapy. BMC Res. Notes 2015, 8, 579. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meaney, C.J.; Hynicka, L.M.; Tsoukleris, M.G. Vancomycin-associated nephrotoxicity in adult medicine patients: Incidence, outcomes, and risk factors. Pharmacotherapy 2014, 34, 653–661. [Google Scholar] [CrossRef]
- Bailie, G.R.; Neal, D. Vancomycin ototoxicity and nephrotoxicity. A review. Med. Toxicol. Advers. Drug Exp. 1988, 3, 376–386. [Google Scholar] [CrossRef]
- Burgess, L.D.; Drew, R.H. Comparison of the incidence of vancomycin-induced nephrotoxicity in hospitalized patients with and without concomitant piperacillin-tazobactam. Pharmacotherapy 2014, 34, 670–676. [Google Scholar] [CrossRef]
- Gomes, D.M.; Smotherman, C.; Birch, A.; DuPree, L.; Della Vecchia, B.J.; Kraemer, D.F.; Jankowski, C.A. Comparison of acute kidney injury during treatment with vancomycin in combination with piperacillin-tazobactam or cefepime. Pharmacotherapy 2014, 34, 662–669. [Google Scholar] [CrossRef]
- Moenster, R.P.; Linneman, T.W.; Finnegan, P.M.; Hand, S.; Thomas, Z.; McDonald, J.R. Acute renal failure associated with vancomycin and β-lactams for the treatment of osteomyelitis in diabetics: Piperacillin-tazobactam as compared with cefepime. Clin. Microbiol. Infect. 2014, 20, 384–389. [Google Scholar] [CrossRef] [Green Version]
- Hammond, D.A.; Smith, M.N.; Painter, J.T.; Meena, N.K.; Lusardi, K. Comparative Incidence of Acute Kidney Injury in Critically Ill Patients Receiving Vancomycin with Concomitant Piperacillin-Tazobactam or Cefepime: A Retrospective Cohort Study. Pharmacotherapy 2016, 36, 463–471. [Google Scholar] [CrossRef]
- Lorenz, M.A.; Moenster, R.P.; Linneman, T.W. Effect of piperacillin/tazobactam restriction on usage and rates of acute renal failure. J. Med. Microbiol. 2016, 65, 195–199. [Google Scholar] [CrossRef] [Green Version]
- Al Yami, M.S. Comparison of the incidence of acute kidney injury during treatment with vancomycin in combination with piperacillin-tazobactam or with meropenem. J. Infect. Public Health 2017, 10, 770–773. [Google Scholar] [CrossRef] [PubMed]
- Navalkele, B.; Pogue, J.M.; Karino, S.; Nishan, B.; Salim, M.; Solanki, S.; Pervaiz, A.; Tashtoush, N.; Shaikh, H.; Koppula, S.; et al. Risk of Acute Kidney Injury in Patients on Concomitant Vancomycin and Piperacillin-Tazobactam Compared to Those on Vancomycin and Cefepime. Clin. Infect. Dis. 2017, 64, 116–123. [Google Scholar] [CrossRef] [PubMed]
- Peyko, V.; Smalley, S.; Cohen, H. Prospective Comparison of Acute Kidney Injury during Treatment with the Combination of Piperacillin-Tazobactam and Vancomycin Versus the Combination of Cefepime or Meropenem and Vancomycin. J. Pharm. Pract. 2017, 30, 209–213. [Google Scholar] [CrossRef] [PubMed]
- Rutter, W.C.; Burgess, D.R.; Talbert, J.C.; Burgess, D.S. Acute kidney injury in patients treated with vancomycin and piperacillin-tazobactam: A retrospective cohort analysis. J. Hosp. Med. 2017, 12, 77–82. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rutter, W.C.; Cox, J.N.; Martin, C.A.; Burgess, D.R.; Burgess, D.S. Nephrotoxicity during Vancomycin Therapy in Combination with Piperacillin-Tazobactam or Cefepime. Antimicrob. Agents Chemother. 2017, 61, e02089-16. [Google Scholar] [CrossRef] [Green Version]
- Anderson, C.W.; Cazares, K.S.; Lustik, M.B.; Patel, S.M.; Denunzio, T.M. Vancomycin vs. Vancomycin/Piperacillin-Tazobactam-Associated Acute Kidney Injury in Noncritically Ill Patients at a Tertiary Care Military Treatment Facility. Mil. Med. 2017, 182, e1773–e1778. [Google Scholar] [CrossRef] [Green Version]
- Hundeshagen, G.; Herndon, D.N.; Capek, K.D.; Branski, L.K.; Voigt, C.D.; Killion, E.A.; Cambiaso-Daniel, J.; Sljivich, M.; De Crescenzo, A.; Mlcak, R.P.; et al. Co-administration of vancomycin and piperacillin-tazobactam is associated with increased renal dysfunction in adult and pediatric burn patients. Crit. Care 2017, 21, 318. [Google Scholar] [CrossRef] [Green Version]
- Robertson, A.D.; Li, C.; Hammond, D.A.; Dickey, T.A. Incidence of Acute Kidney Injury among Patients Receiving the Combination of Vancomycin with Piperacillin-Tazobactam or Meropenem. Pharmacotherapy 2018, 38, 1184–1193. [Google Scholar] [CrossRef]
- Carreno, J.; Smiraglia, T.; Hunter, C.; Tobin, E.; Lomaestro, B. Comparative incidence and excess risk of acute kidney injury in hospitalised patients receiving vancomycin and piperacillin/tazobactam in combination or as monotherapy. Int. J. Antimicrob. Agents 2018, 52, 643–650. [Google Scholar] [CrossRef]
- Rutter, W.C.; Burgess, D.S. Incidence of Acute Kidney Injury among Patients Treated with Piperacillin-Tazobactam or Meropenem in Combination with Vancomycin. Antimicrob. Agents Chemother. 2018, 62, e00264-18. [Google Scholar] [CrossRef] [Green Version]
- Schreier, D.J.; Kashani, K.B.; Sakhuja, A.; Mara, K.C.; Tootooni, M.S.; Personett, H.A.; Nelson, S.; Rule, A.D.; Steckelberg, J.M.; Tande, A.J.; et al. Incidence of Acute Kidney Injury Among Critically Ill Patients with Brief Empiric Use of Antipseudomonal β-Lactams with Vancomycin. Clin. Infect. Dis. 2019, 68, 1456–1462. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cannon, J.M.; Douce, R.W.; Grubbs, E.R.; Wills, C.B.; Khan, A.; Schmidt, E.M.; Wang, M.S. Comparison of Acute Kidney Injury during Treatment with Vancomycin and either Piperacillin-Tazobactam or Meropenem. Spartan Med. Res. J. 2017, 2, 6440. [Google Scholar] [CrossRef]
- Balcı, C.; Uzun, Ö.; Arıcı, M.; Hayran, S.A.; Yüce, D.; Ünal, S. Nephrotoxicity of piperacillin/tazobactam combined with vancomycin: Should it be a concern? Int. J. Antimicrob. Agents 2018, 52, 180–184. [Google Scholar] [CrossRef] [PubMed]
- Mullins, B.P.; Kramer, C.J.; Bartel, B.J.; Catlin, J.S.; Gilder, R.E. Comparison of the Nephrotoxicity of Vancomycin in Combination with Cefepime, Meropenem, or Piperacillin/Tazobactam: A Prospective, Multicenter Study. Ann. Pharmacother. 2018, 52, 639–644. [Google Scholar] [CrossRef] [PubMed]
- Blevins, A.; Lashinsky, J.; McCammon, C.; Kollef, M.; Micek, S.; Juang, P. Incidence of Acute Kidney Injury in Critically Ill Patients Receiving Vancomycin with Concomitant Piperacillin/Tazobactam, Cefepime, or Meropenem. Antimicrob. Agents Chemother. 2019, 63, e02658-18. [Google Scholar] [CrossRef] [Green Version]
- Kang, S.; Park, J.; Yu, Y.M.; Park, M.S.; Han, E.; Chang, M.J. Comparison of acute kidney injury and clinical prognosis of vancomycin monotherapy and combination therapy with beta-lactams in the intensive care unit. PLoS ONE 2019, 14, e0217908. [Google Scholar] [CrossRef] [Green Version]
- Ide, N.; Sato, S.; Sawaguchi, K. Risk of Acute Kidney Injury in Patients Treated with Vancomycin and Piperacillin/Tazobactam Compared to Vancomycin and Meropenem or Doripenem: A Retrospective Cohort Study Risk of Acute Kidney Injury in Patients Treated with Vancomycin and Piperacillin/Tazobactam Compared to Vancomycin and Meropenem or Doripenem: A Retrospective Cohort Study. YAKUGAKU ZASSHI 2019, 139, 1609–1614. [Google Scholar] [CrossRef] [Green Version]
- Tookhi, R.F.; Kabli, N.A.; Huntul, M.A.; Thabit, A.K. Impact of combining vancomycin with piperacillin/tazobactam or with meropenem on vancomycin-induced nephrotoxicity. Intern. Emerg. Med. 2021, 16, 975–979. [Google Scholar] [CrossRef]
- Rungkitwattanakul, D.; Ives, A.L.; Harriott, N.G.; Pan-Chen, S.; Duong, L. Comparative incidence of acute kidney injury in patients on vancomycin therapy in combination with cefepime, piperacillin-tazobactam or meropenem. J. Chemother. 2021, 34, 103–109. [Google Scholar] [CrossRef]
- Wells GA, S.B.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle–Ottawa Scale (NOS) for Assessing the Quality of Non-Randomized Studies in Meta-Analysis. 2000. Available online: http//www.ohrica/programs/clinical_epidemiology/nosgen.pdf (accessed on 11 April 2022).
- Brooke, B.S.; Schwartz, T.A.; Pawlik, T.M. MOOSE Reporting Guidelines for Meta-analyses of Observational Studies. JAMA Surg. 2021, 156, 787–788. [Google Scholar] [CrossRef]
- Cattran, D.C.; Feehally, J.; Cook, H.T.; Liu, Z.H.; Fervenza, F.; Mezzano, S.A.; Floege, J.; Nachman, P.H.; Gipson, D.S.; Praga, M.; et al. Kidney disease: Improving global outcomes (KDIGO) glomerulonephritis work group. KDIGO clinical practice guideline for glomerulonephritis. Kidney Int. Suppl. 2012, 2, 139–274. [Google Scholar] [CrossRef] [Green Version]
- Mehta, R.L.; Kellum, J.A.; Shah, S.V.; Molitoris, B.A.; Ronco, C.; Warnock, D.G.; Levin, A. Acute Kidney Injury Network: Report of an initiative to improve outcomes in acute kidney injury. Crit. Care 2007, 11, R31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bellomo, R.; Ronco, C.; Kellum, J.A.; Mehta, R.L.; Palevsky, P.; Acute Dialysis Quality Initiative Workgroup. Acute renal failure—Definition, outcome measures, animal models, fluid therapy and information technology needs: The Second International Consensus Conference of the Acute Dialysis Quality Initiative (ADQI) Group. Crit. Care 2004, 8, R204–R212. [Google Scholar] [CrossRef] [Green Version]
- Chen, X.Y.; Xu, R.X.; Zhou, X.; Liu, Y.; Hu, C.Y.; Xie, X.F. Acute kidney injury associated with concomitant vancomycin and piperacillin/tazobactam administration: A systematic review and meta-analysis. Int. Urol. Nephrol. 2018, 50, 2019–2026. [Google Scholar] [CrossRef] [PubMed]
- Giuliano, C.A.; Patel, C.R.; Kale-Pradhan, P.B. Is the Combination of Piperacillin-Tazobactam and Vancomycin Associated with Development of Acute Kidney Injury? A Meta-analysis. Pharmacotherapy 2016, 36, 1217–1228. [Google Scholar] [CrossRef]
- Watkins, R.R.; Deresinski, S. Increasing Evidence of the Nephrotoxicity of Piperacillin/Tazobactam and Vancomycin Combination Therapy—What Is the Clinician to Do? Clin. Infect. Dis. 2017, 65, 2137–2143. [Google Scholar] [CrossRef]
- Bellos, I.; Karageorgiou, V.; Pergialiotis, V.; Perrea, D.N. Acute kidney injury following the concurrent administration of antipseudomonal β-lactams and vancomycin: A network meta-analysis. Clin. Microbiol. Infect. 2020, 26, 696–705. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Year | Type | Country | AKI Definition | Proportion of Critically Ill Patients | Patients with AKI History or CKD | Sample Size | Incidence | p-Value | |
|---|---|---|---|---|---|---|---|---|---|---|
| V + PT | V + M | |||||||||
| Studies including critically and non-critically ill patients | ||||||||||
| Alyami et al. | 2017 | Retrospective cohort | USA | KDIGO | 17.5% | Excluded | 183 | 8/108 (7.4%) | 4/75 (5.3%) | 0.4 |
| Cannon et al. | 2018 | Retrospective cohort | USA | An absolute 0.5 mg/dL increase in SCr or at least 50% increase in SCr from baseline | 18.9% | Excluded | 366 | 74/292 (25.3%) | 8/74 (9.5%) | 0.008 |
| Tookhi et al. | 2021 | Retrospective cohort | SA | KDIGO | 24.6% | Excluded | 158 | 8/77 (10.3%) | 17/81 (20.9%) | 0.07 |
| Rungkitwattanakul et al. | 2021 | Retrospective cohort | USA | KDIGO | N/A | Excluded | 207 | 16/74 (21.6%) | 5/67 (7.4%) | 0.002 |
| Studies including non-critically ill patients only | ||||||||||
| Balcı et al. | 2018 | Retrospective cohort | Turkey | AKIN | NA | CKD: 14.4% AKI: 25% | 132 | 26/63 (41.3%) | 7/69 (10.1%) | <0.001 |
| Robertson et al. | 2018 | Retrospective cohort | USA | An absolute 0.5 mg/dL increase in SCr or at least 50% increase in SCr from baseline | NA | Excluded | 169 | 14/85 (16.5%) | 3/84 (3.6%) | 0.009 |
| Mullins et al. | 2018 | Prospective cohort | USA | 1.5-fold increase in SCr (baseline vs. within first 7 days of antimicrobial therapy) | NA | Excluded | 143 | 28/94 (29.8%) | 7/49 (14.3%) | <0.001 |
| Rutter et al. | 2019 | Retrospective cohort | USA | RIFLE | NA | Excluded | 10,236 | 2713/9898 (27.4%) | 52/338 (15.4%) | <0.001 |
| Ide et al. | 2019 | Retrospective cohort | Japan | KDIGO | NA | Not reported | 76 | 9/27 (33.3%) | 4/49 (8.2%) | 0.015 * |
| Studies including critically ill patients only | ||||||||||
| Schreier et al. | 2019 | Retrospective cohort | USA | AKIN | 100% | CKD: 13.7% AKI: 29.3% | 1926 | 601/1540 (39.0%) | 135/386 (34.9%) | 0.49 |
| Blevins et al. | 2019 | Retrospective cohort | USA | KDIGO | 100% | Excluded | 758 | 144/366 (39.3%) | 92/392 (23.5%) | <0.0001 |
| Kang et al. | 2019 | Retrospective cohort | SK | KDIGO | 100% | Excluded | 157 | 39/74 (52.7%) | 23/83 (27.7%) | <0.0001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alshehri, A.M.; Alzahrani, M.Y.; Abujamal, M.A.; Abdalla, M.H.; Alowais, S.A.; Alfayez, O.M.; Alyami, M.S.; Almutairi, A.R.; Almohammed, O.A. Comparative Risk of Acute Kidney Injury Following Concurrent Administration of Vancomycin with Piperacillin/Tazobactam or Meropenem: A Systematic Review and Meta-Analysis of Observational Studies. Antibiotics 2022, 11, 526. https://doi.org/10.3390/antibiotics11040526
Alshehri AM, Alzahrani MY, Abujamal MA, Abdalla MH, Alowais SA, Alfayez OM, Alyami MS, Almutairi AR, Almohammed OA. Comparative Risk of Acute Kidney Injury Following Concurrent Administration of Vancomycin with Piperacillin/Tazobactam or Meropenem: A Systematic Review and Meta-Analysis of Observational Studies. Antibiotics. 2022; 11(4):526. https://doi.org/10.3390/antibiotics11040526
Chicago/Turabian StyleAlshehri, Abdulmajeed M., Mohammed Y. Alzahrani, Mohammed A. Abujamal, Mariam H. Abdalla, Shuroug A. Alowais, Osamah M. Alfayez, Majed S. Alyami, Abdulaali R. Almutairi, and Omar A. Almohammed. 2022. "Comparative Risk of Acute Kidney Injury Following Concurrent Administration of Vancomycin with Piperacillin/Tazobactam or Meropenem: A Systematic Review and Meta-Analysis of Observational Studies" Antibiotics 11, no. 4: 526. https://doi.org/10.3390/antibiotics11040526