
Effects of Curcumin and Tetracycline Gel on Experimental Induced Periodontitis as an Anti-Inflammatory, Osteogenesis Promoter and Enhanced Bone Density through Altered Iron Levels: Histopathological Study

 , ,
, , 
Abstract
:1. Introduction
2. Results
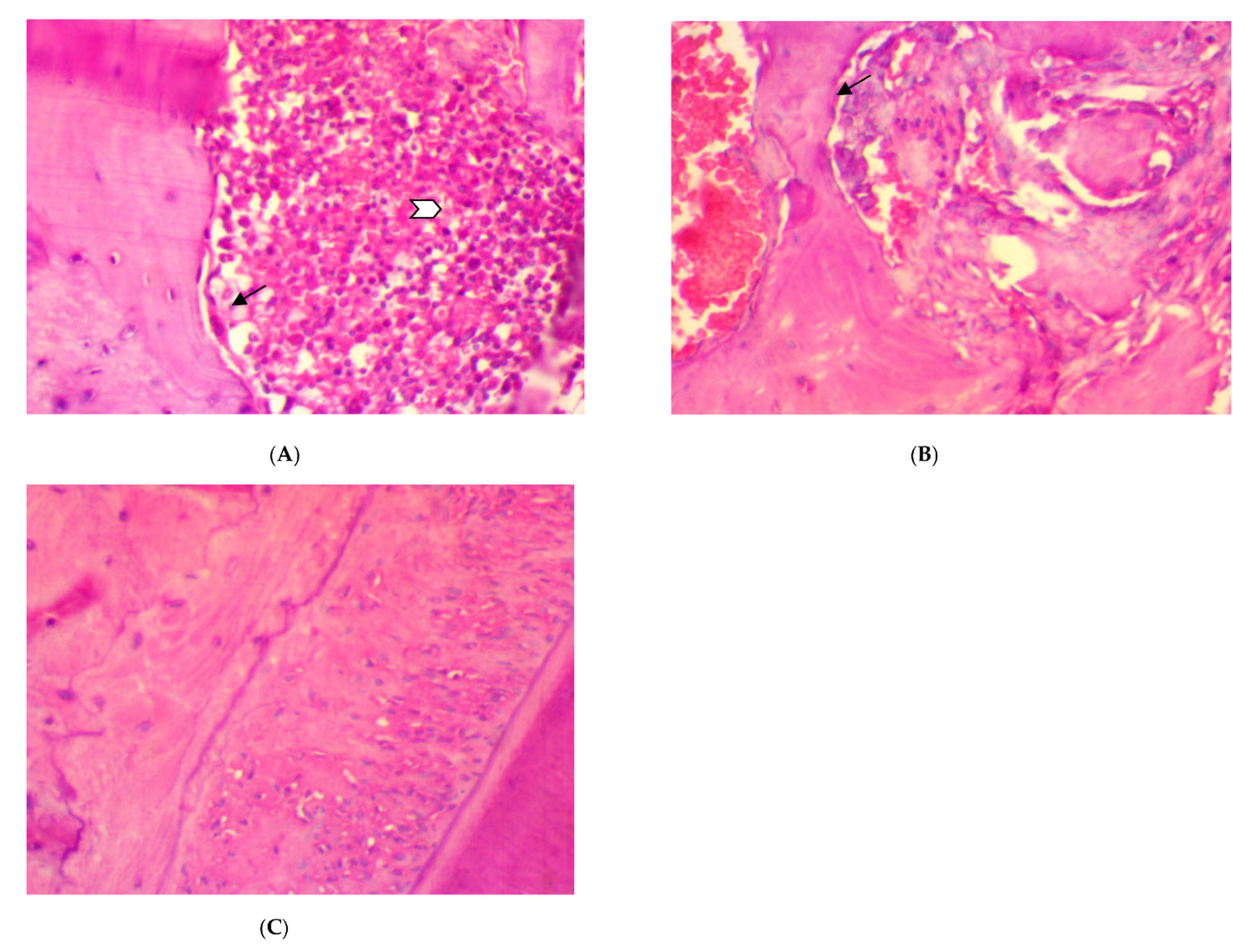
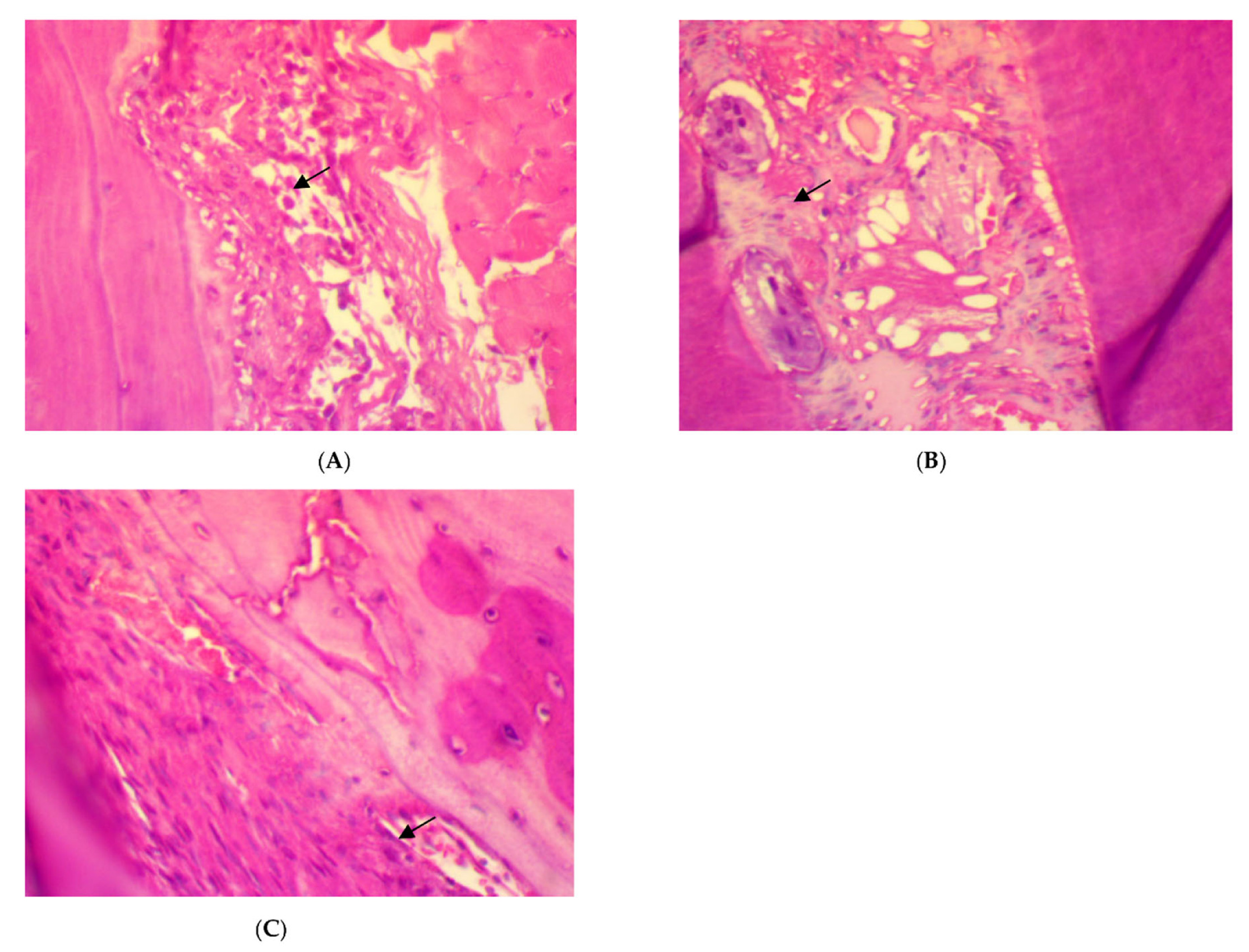
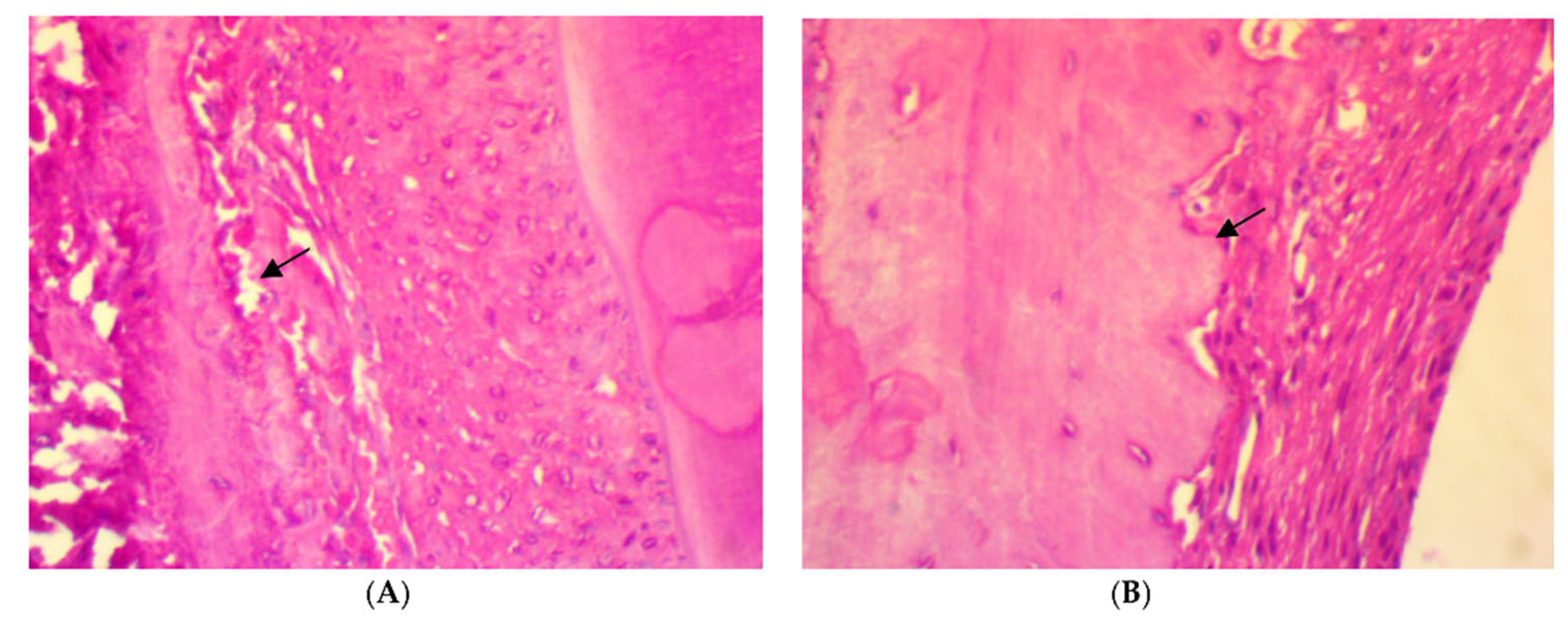
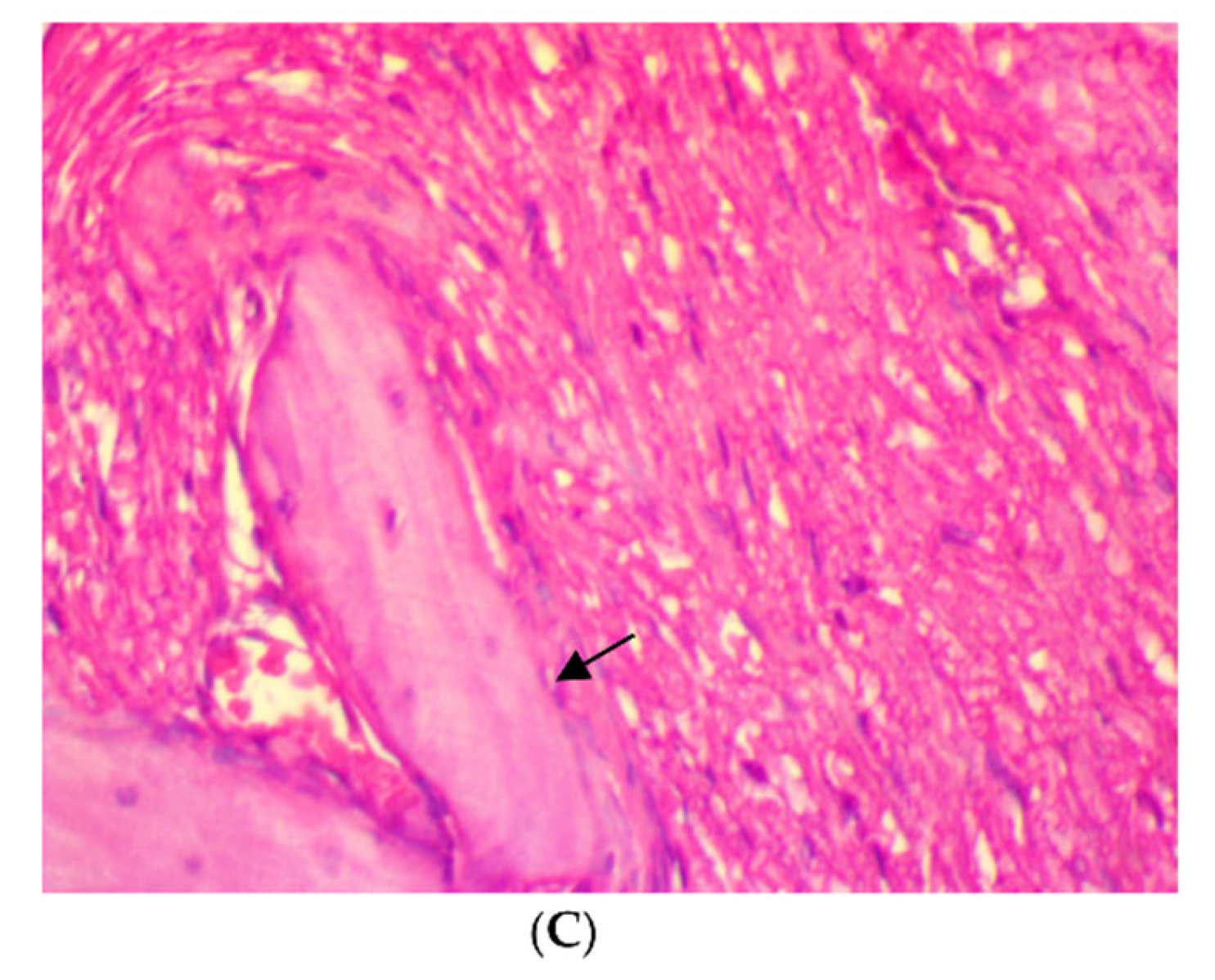
2.1. Histological Evaluation
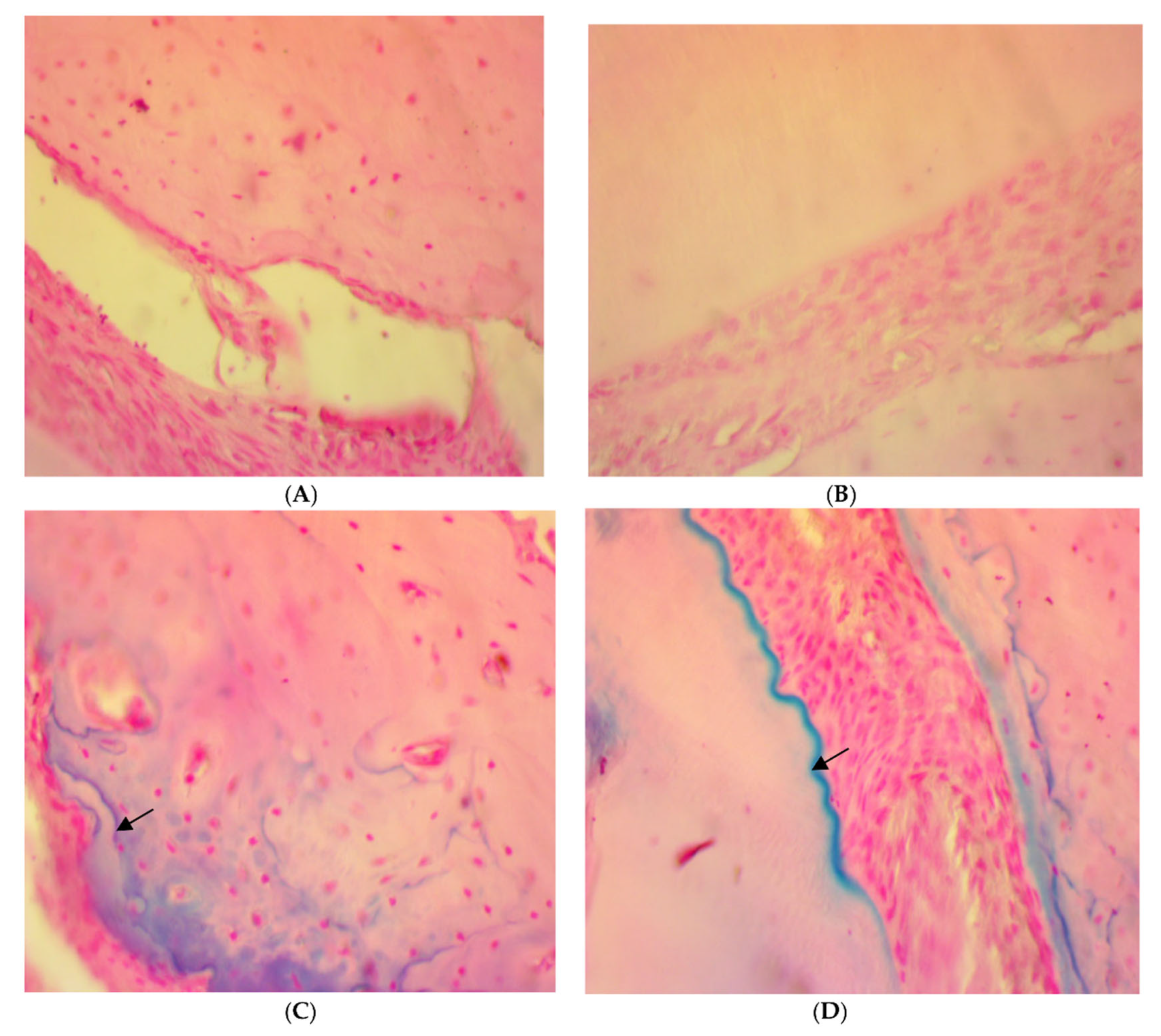
2.1.1. Inflammatory Reaction
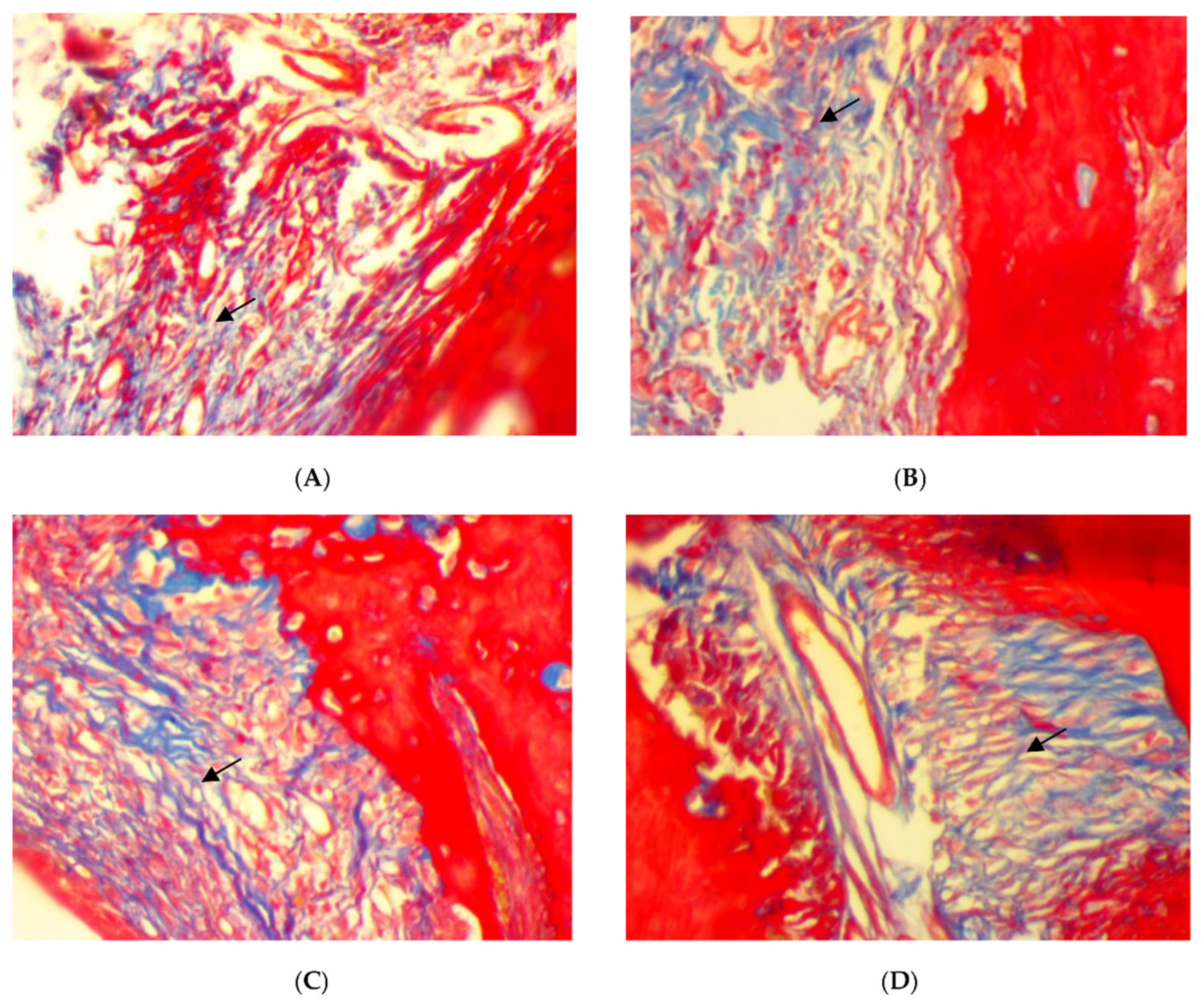
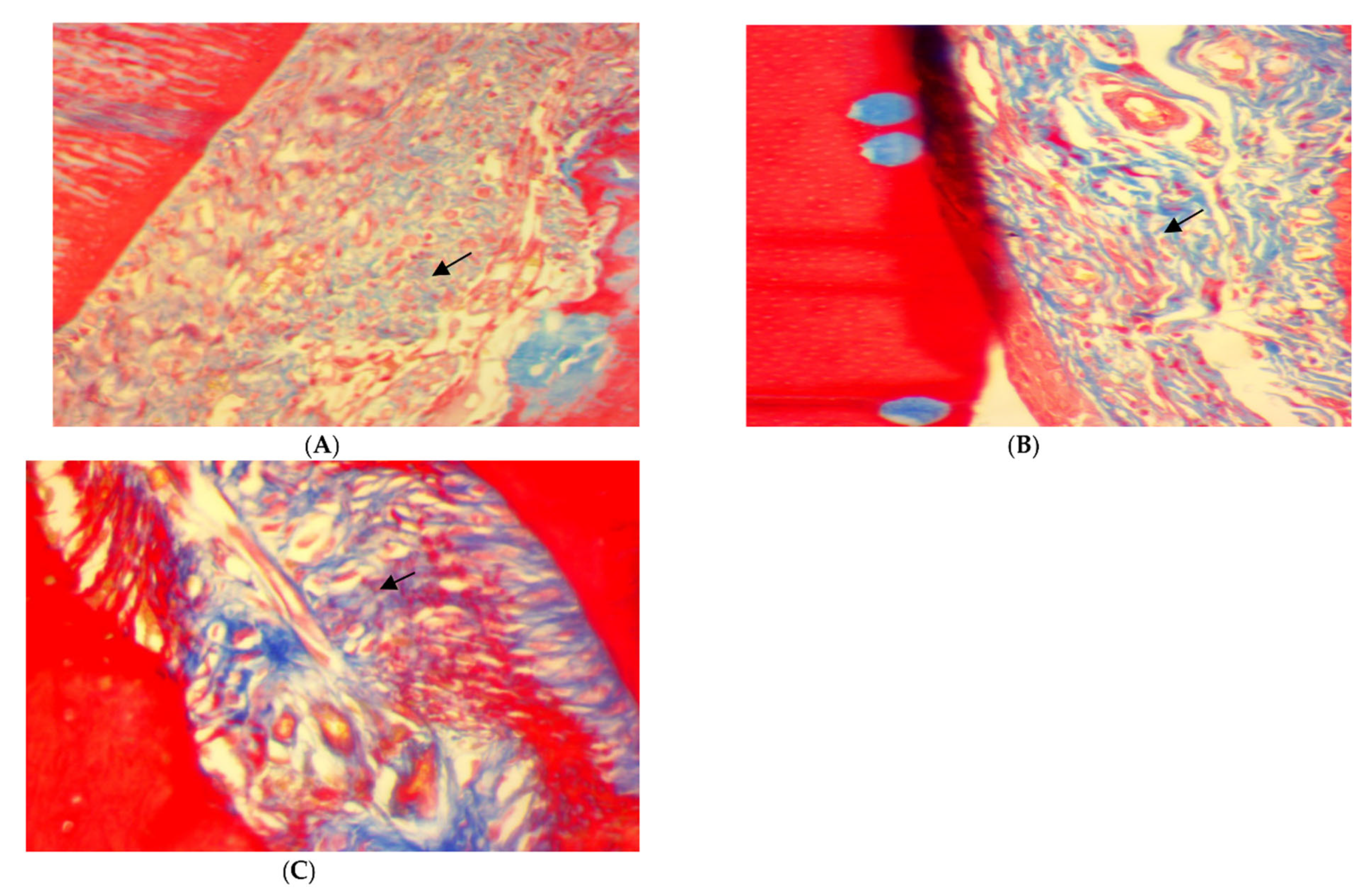
2.1.2. Special Stains
2.2. Inflammatory Cells and Osteoclast Counts
3. Discussion
4. Materials and Methods
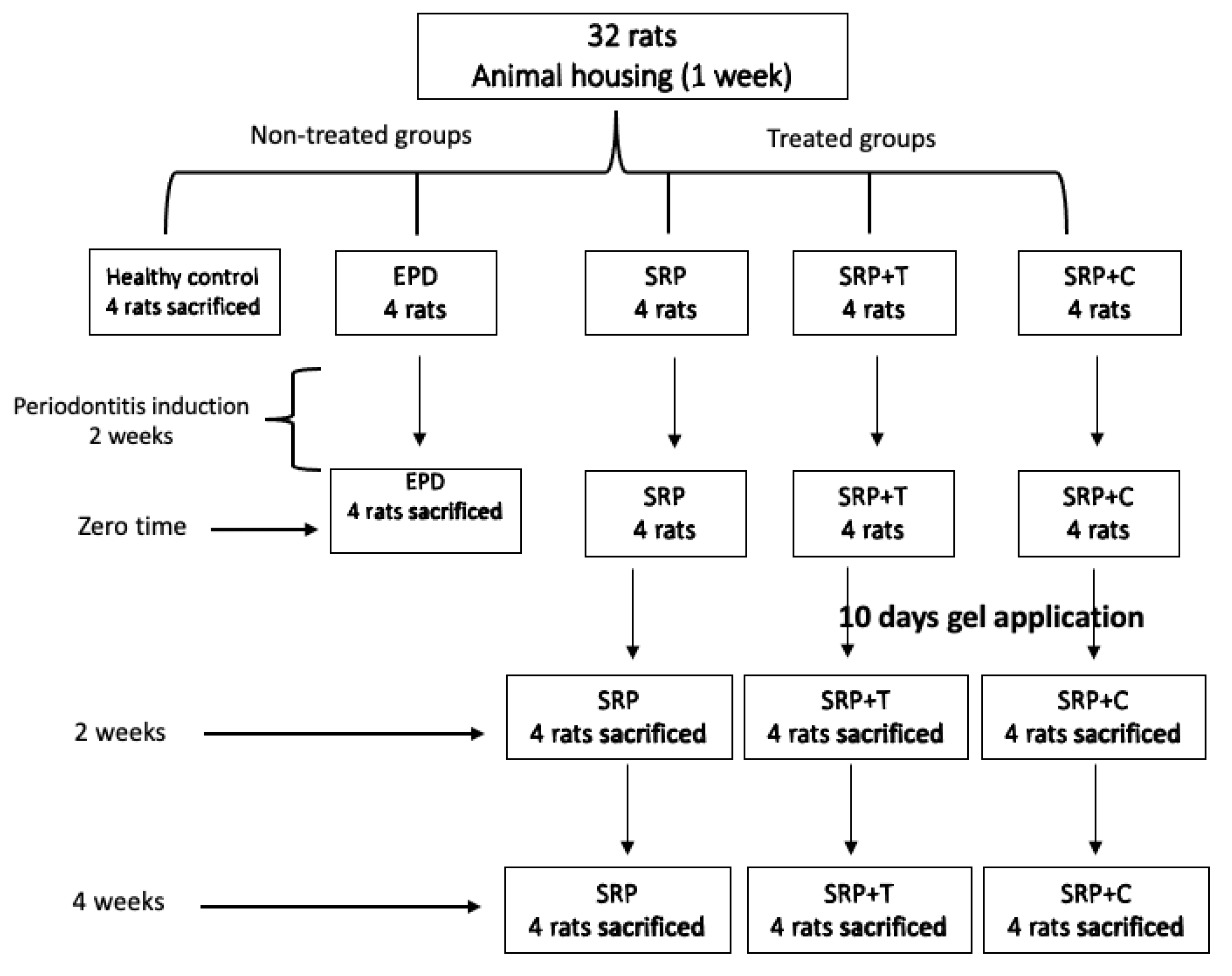
4.1. Rats and Housing
4.2. Induction of Experimental Periodontitis
4.3. Experimental Design
4.4. Curcumin Gel Composition and Preparation
- Dissolving and mixing 12.50 μg of CU with 100 mL propylene glygol and 25.00 mg potassium sorbate.
- Dissolving 4 mg of Metalose 90SH 10,000 in 850 mL purified water.
- The solutions from a and b were mixed and the volume was made up with water; finally, the mixing was continued until a homogenous gel was formed.
4.5. Tetracycline Gel Composition and Preparation
- Dissolving and mixing 6 μg of T with 100 mL propylene glygol and 25.00 mg of potassium sorbate.
- Dissolving 4 mg of Metalose 90SH 10,000 in 850 mL purified water.
- The solutions from a and b were mixed and the volume was made up with water; finally the mixing was continued until a homogenous gel was formed. Tetracycline gel was also prepared by Awa Medica Company, Hawler, Kurdistan Region, Iraq.
4.6. Histological Evaluation
4.7. Histo-Morphometric Assessment
4.8. Evaluation of Inflammatory Reaction
4.9. Special Stains
4.10. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Van Dyke, T.E. The etiology and pathogenesis of periodontitis revisited. J. Appl. Oral. Sci. 2009, 17, i. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Papapanou, P.N.; Sanz, M.; Buduneli, N.; Dietrich, T.; Feres, M.; Fine, D.H.; Flemmig, T.F.; Garcia, R.; Giannobile, W.V.; Graziani, F. Periodontitis: Consensus report of workgroup 2 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J. Periodontol. 2018, 89, S173–S182. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sabharwal, A.; Gomes-Filho, I.S.; Stellrecht, E.; Scannapieco, F.A. Role of periodontal therapy in management of common complex systemic diseases and conditions: An update. Periodontology 2018, 78, 212–226. [Google Scholar] [CrossRef] [PubMed]
- Ionel, A.; Lucaciu, O.; Moga, M.; Buhatel, D.; Ilea, A.; Tabaran, F.; Catoi, C.; Berce, C.; Toader, S.; Campian, R.S. Periodontal disease induced in Wistar rats-experimental study. J. Hum. Vet. Med. 2015, 7, 90–95. [Google Scholar]
- Kaldahl, W.B.; Kalkwarf, K.L.; Patil, K.D. A review of longitudinal studies that compared periodontal therapies. J. Periodontol. 1993, 64, 243–253. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matarazzo, F.; Figueiredo, L.C.; Cruz, S.E.; Faveri, M.; Feres, M. Clinical and microbiological benefits of systemic metronidazole and amoxicillin in the treatment of smokers with chronic periodontitis: A randomized placebo-controlled study. J. Clin. Periodontol. 2008, 35, 885–896. [Google Scholar] [CrossRef]
- Abdulkareem, A.; Abdulbaqi, H.; Gul, S.; Milward, M.; Chasib, N.; Alhashimi, R. Classic vs. Novel Antibacterial Approaches for Eradicating Dental Biofilm as Adjunct to Periodontal Debridement: An Evidence-Based Overview. Antibiotics 2022, 11, 9. [Google Scholar] [CrossRef]
- Christersson, L.A.; Norderyd, O.M.; Puchalsky, C.S. Topical application of tetracycline-HCl in human periodontitis. J. Clin. Periodontol. 1993, 20, 88–95. [Google Scholar] [CrossRef]
- Cattabriga, M.; Pedrazzoli, V.; Cattabriga, A.; Pannuti, E.; Trapani, M.; Verrocchi, G.C. Tetracycline fiber used alone or with scaling and root planing in periodontal maintenance patients: Clinical results. Quintessence. Int. 1996, 27, 395–400. [Google Scholar]
- Sholapurkar, A.; Sharma, D.; Glass, B.; Miller, C.; Nimmo, A.; Jennings, E. Professionally Delivered Local Antimicrobials in the Treatment of Patients with Periodontitis—A Narrative Review. Dent. J. 2021, 9, 2. [Google Scholar] [CrossRef]
- Walker, C.B.; Gordon, J.M.; McQuilkin, S.J.; Niebloom, T.A.; Socransky, S.S. Tetracycline: Levels of achievable in gingival crevice fluid and in vitro effect on subgingival organisms. Part II. Susceptibilities of periodontal bacteria. J. Periodontol. 1981, 52, 613–616. [Google Scholar] [CrossRef] [PubMed]
- Golub, L.M.; Ramamurthy, N.; McNamara, T.F.; Gomes, B.; Wolff, M.; Casino, A.; Kapoor, A.; Zambon, J.; Ciancio, S.; Schneir, M.; et al. Tetracyclines inhibit tissue collagenase activity. A new mechanism in the treatment of periodontal disease. J. Periodontal. Res. 1984, 19, 651–655. [Google Scholar] [CrossRef] [PubMed]
- Bhatia, M.; Urolagin, S.S.; Pentyala, K.B.; Urolagin, S.B.; Menaka, K.B.; Bhoi, S. Novel therapeutic approach for the treatment of periodontitis by curcumin. J. Clin. Diagn. Res. 2014, 8, ZC65–ZC69. [Google Scholar] [CrossRef] [PubMed]
- Aggarwal, B.B.; Sundaram, C.; Malani, N.; Ichikawa, H. Curcumin: The Indian solid gold. Adv. Exp. Med. Biol. 2007, 595, 1–75. [Google Scholar]
- Sha, A.M.; Garib, B.T. Antibacterial Effect of Curcumin against Clinically Isolated Porphyromonas gingivalis and Connective Tissue Reactions to Curcumin Gel in the Subcutaneous Tissue of Rats. BioMed. Res. Int. 2019, 2019, 6810936. [Google Scholar] [CrossRef] [Green Version]
- Edwards, D.F., 3rd; Miller, C.J.; Quintana-Martinez, A.; Wright, C.S.; Prideaux, M.; Atkins, G.J.; Thompson, W.R.; Clinkenbeard, E.L. Differential Iron Requirements for Osteoblast and Adipocyte Differentiation. JBMR Plus 2021, 5, e10529. [Google Scholar] [CrossRef]
- Sinha, S.; Kumar, S.; Dagli, N.; Dagli, R.J. Effect of tetracycline HCl in the treatment of chronic periodontitis—A clinical study. J. Int. Soc. Prev. Community Dent. 2014, 4, 149–153. [Google Scholar]
- Farzamfar, S.; Naseri-Nosar, M.; Sahrapeyma, H.; Ehterami, A.; Goodarzi, A.; Rahmati, M.; Ahmadi Lakalayeh, G.; Ghorbani, S.; Vaez, A.; Salehi, M. Tetracycline hydrochloride-containing poly (ε-caprolactone)/poly lactic acid scaffold for bone tissue engineering application: In vitro and in vivo study. Int. J. Polym. Mate. Polym. Biomate. 2019, 68, 472–479. [Google Scholar] [CrossRef]
- de Figueiredo, F.A.; Shimano, R.C.; Ervolino, E.; Pitol, D.L.; Gerlach, R.F.; Issa, J.P.M. Doxycycline reduces osteopenia in female rats. Sci. Rep. 2019, 9, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Rawal, S.Y.; Rawal, Y.B. Non-antimicrobial properties of tetracyclines--dental and medical implications. West Indian Med. J. 2001, 50, 105–108. [Google Scholar]
- Terranova, V.P.; Franzetti, L.C.; Hic, S.; DiFlorio, R.M.; Lyall, R.M.; Wikesjö, U.M.; Baker, P.J.; Christersson, L.A.; Genco, R.J. A biochemical approach to periodontal regeneration: Tetracycline treatment of dentin promotes fibroblast adhesion and growth. J. Periodontal. Res. 1986, 21, 330–337. [Google Scholar] [CrossRef] [PubMed]
- Fernandes, L.A.; Martins, T.M.; Almeida, J.M.D.; Nagata, M.J.H.; Theodoro, L.H.; Garcia, V.G.; Bosco, A.F. Experimental periodontal disease treatment by subgingival irrigation with tetracycline hydrochloride in rats. J. Appl. Oral. Sci. 2010, 18, 635–640. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hewlings, S.J.; Kalman, D.S. Curcumin: A Review of Its Effects on Human Health. Foods 2017, 6, 92. [Google Scholar] [CrossRef] [PubMed]
- Kaur, H.; Grover, V.; Malhotra, R.; Gupta, M. Evaluation of Curcumin Gel as Adjunct to Scaling & Root Planing in Management of Periodontitis—Randomized Clinical & Biochemical Investigation. Infect. Disord. Drug Targets 2019, 19, 171–178. [Google Scholar]
- Mohammad, C.A. Efficacy of Curcumin Gel on Zinc, Magnesium, Copper, IL-1β, and TNF-α in Chronic Periodontitis Patients. Biomed. Res. Int. 2020, 2020, 8850926. [Google Scholar]
- Xiao, C.-J.; Yu, X.-J.; Xie, J.-L.; Liu, S.; Li, S. Protective effect and related mechanisms of curcumin in rat experimental periodontitis. Head Face Med. 2018, 14, 12. [Google Scholar] [CrossRef]
- Tan, L.; Cao, Z.; Chen, H.; Xie, Y.; Yu, L.; Fu, C.; Zhao, W.; Wang, Y. Curcumin reduces apoptosis and promotes osteogenesis of human periodontal ligament stem cells under oxidative stress in vitro and in vivo. Life Sci. 2021, 270, 119125. [Google Scholar] [CrossRef]
- Zhou, T.; Chen, D.; Li, Q.; Sun, X.; Song, Y.; Wang, C. Curcumin inhibits inflammatory response and bone loss during experimental periodontitis in rats. Acta Odontol. Scand. 2013, 71, 349–356. [Google Scholar] [CrossRef]
- Sha, A.M.; Garib, B.T.; Azeez, S.H.; Gul, S.S. Effects of curcumin gel on osteoclastogenic bone markers in experimental periodontitis and alveolar bone loss in wistar rats. J. Dent. Sci. 2021, 16, 905–914. [Google Scholar] [CrossRef]
- Grynkiewicz, G.; Ślifirski, P. Curcumin and curcuminoids in quest for medicinal status. Acta Biochim. Pol. 2012, 59, 201–212. [Google Scholar] [CrossRef]
- Shakibaei, M.; Mobasheri, A.; Buhrmann, C. Curcumin synergizes with resveratrol to stimulate the MAPK signaling pathway in human articular chondrocytes in vitro. Genes Nutr. 2011, 6, 171–179. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mau, L.-P.; Cheng, W.-C.; Chen, J.-K.; Shieh, Y.-S.; Cochran, D.L.; Huang, R.-Y. Curcumin ameliorates alveolar bone destruction of experimental periodontitis by modulating osteoclast differentiation, activation and function. J. Funct. Foods 2016, 22, 243–256. [Google Scholar] [CrossRef]
- Butera, A.; Gallo, S.; Pascadopoli, M.; Maiorani, C.; Milone, A.; Alovisi, M.; Scribante, A. Paraprobiotics in Non-Surgical Periodontal Therapy: Clinical and Microbiological Aspects in a 6-Month Follow-Up Domiciliary Protocol for Oral Hygiene. Microorganisms 2022, 10, 337. [Google Scholar] [CrossRef] [PubMed]
- Scribante, A.; Butera, A.; Alovisi, M. Customized Minimally Invasive Protocols for the Clinical and Microbiological Management of the Oral Microbiota. Microorganisms 2022, 10, 675. [Google Scholar] [CrossRef]
- Hou, J.; Yamada, S.; Kajikawa, T.; Ozaki, N.; Awata, T.; Yamaba, S.; Fujihara, C.; Murakami, S. Iron plays a key role in the cytodifferentiation of human periodontal ligament cells. J. Periodontal. Res. 2014, 49, 260–267. [Google Scholar] [CrossRef]
- Yang, J.; Zhang, J.; Ding, C.; Dong, D.; Shang, P. Regulation of Osteoblast Differentiation and Iron Content in MC3T3-E1 Cells by Static Magnetic Field with Different Intensities. Biol. Trace. Elem. Res. 2018, 184, 214–225. [Google Scholar] [CrossRef] [Green Version]
- Tiekou Lorinczova, H.; Begum, G.; Temouri, L.; Renshaw, D.; Zariwala, M.G. Co-Administration of Iron and Bioavailable Curcumin Reduces Levels of Systemic Markers of Inflammation and Oxidative Stress in a Placebo-Controlled Randomised Study. Nutrients 2022, 14, 712. [Google Scholar] [CrossRef]
- Chakraborty, S.; Tewari, S.; Sharma, R.K.; Narula, S.C.; Ghalaut, P.S.; Ghalaut, V. Impact of iron deficiency anemia on chronic periodontitis and superoxide dismutase activity: A cross-sectional study. J. Periodontal. Implant. Sci. 2014, 44, 57–64. [Google Scholar] [CrossRef] [Green Version]
- National Research Council (US) Committee for the Update of the Guide for the Care and Use of Laboratory, Animals. The National Academies Collection: Reports funded by National Institutes of Health. In Guide for the Care and Use of Laboratory Animals, National Academies Press (US)Copyright © 2011; National Academy of Sciences: Washington, DC, USA, 2011. [Google Scholar]
- Armed Forces Institute of Pathology. Laboratory Methods in Histotechnology; American Registry of Pathology: Washington, DC, USA, 1992. [Google Scholar]
- Mitic, A.; Todorovic, K.; Stojiljkovic, N.; Stojanovic, N.; Ilic, S.; Todorovic, A.; Stojnev, S. Beneficial effects of curcumin on the wound-healing process after tooth extraction. Nat. Prod. Commun. 2017, 12, 1934578X1701201223. [Google Scholar] [CrossRef] [Green Version]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Time | Groups | Comparison | Total Inflammatory Cell Count Mean ± S.D. | p-Value | Osteoclast | p-Value |
|---|---|---|---|---|---|---|
| - | Normal | Normal vs. EPD | 2.33 ± 0.58 | 0.001 * | 0 | 0.001 * |
| EPD | 31.00 ± 1.00 | 4.67 ± 0.58 | ||||
| 2 Weeks | SRP | 20.33 ± 2.52 | 2.67 ± 0.58 | |||
| SRP+T | SRP vs. SRP+T | 5.00 ± 0.00 | 0.001 † | 1.67 ± 0.58 | 0.047 † | |
| SRP+CU | SRP vs. SRP+CU | 5.00 ± 0.00 | 0.001 † | 1.33 ± 0.58 | 0.026 † | |
| SRP+T vs. SRP+CU | 0.99 † | 0.047 † | ||||
| 4 Weeks | SRP | 5.00 ± 0.00 | 1.67 ± 0.58 | |||
| SRP+T | SRP vs. SRP+T | 3.33 ± 0.58 | 0.002 † | 1.67 ± 0.58 | 0.99 † | |
| SRP+CU | SRP vs. SRP+CU | 2.67 ± 0.58 | 0.0008 † | 1.00 ± 0.00 | 0.116 † | |
| SRP+T vs. SRP+CU | 0.48 † | 0.116 † |
| Groups | Time | Total Inflammatory Cell Mean ± SD | Osteoclasts Mean ± SD |
|---|---|---|---|
| SRP | 2 Weeks | 20.33 ± 2.51 | 2.67 ± 0.58 |
| 4 Weeks | 5.00 ± 0.00 | 1.67 ± 0.58 | |
| p value * | 0.005 * | 0.047 * | |
| SRP+T | 2 Weeks | 5.00 ± 0.00 | 1.67 ± 0.58 |
| 4 Weeks | 3.33 ± 0.58 | 1.67 ± 0.58 | |
| p value * | 0.007 * | 1.00 * | |
| SRP+CU | 2 Weeks | 5.00 ± 1.00 | 1.33 ± 0.58 |
| 4 Weeks | 2.67 ± 0.58 | 1.00 ± 0.00 | |
| p value * | 0.007 * | 0.37 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mohammad, C.A.; Ali, K.M.; Al-Rawi, R.A.; Gul, S.S. Effects of Curcumin and Tetracycline Gel on Experimental Induced Periodontitis as an Anti-Inflammatory, Osteogenesis Promoter and Enhanced Bone Density through Altered Iron Levels: Histopathological Study. Antibiotics 2022, 11, 521. https://doi.org/10.3390/antibiotics11040521
Mohammad CA, Ali KM, Al-Rawi RA, Gul SS. Effects of Curcumin and Tetracycline Gel on Experimental Induced Periodontitis as an Anti-Inflammatory, Osteogenesis Promoter and Enhanced Bone Density through Altered Iron Levels: Histopathological Study. Antibiotics. 2022; 11(4):521. https://doi.org/10.3390/antibiotics11040521
Chicago/Turabian StyleMohammad, Chenar Anwar, Khadeeja Mohammed Ali, Rafal AbdulRazaq Al-Rawi, and Sarhang Sarwat Gul. 2022. "Effects of Curcumin and Tetracycline Gel on Experimental Induced Periodontitis as an Anti-Inflammatory, Osteogenesis Promoter and Enhanced Bone Density through Altered Iron Levels: Histopathological Study" Antibiotics 11, no. 4: 521. https://doi.org/10.3390/antibiotics11040521