
Machine Learning and Antibiotic Management

 , , , , , ,
, , , , , ,
Abstract
:1. Introduction
2. Materials and Methods

2.1. Population and Data Collection
2.2. System Development
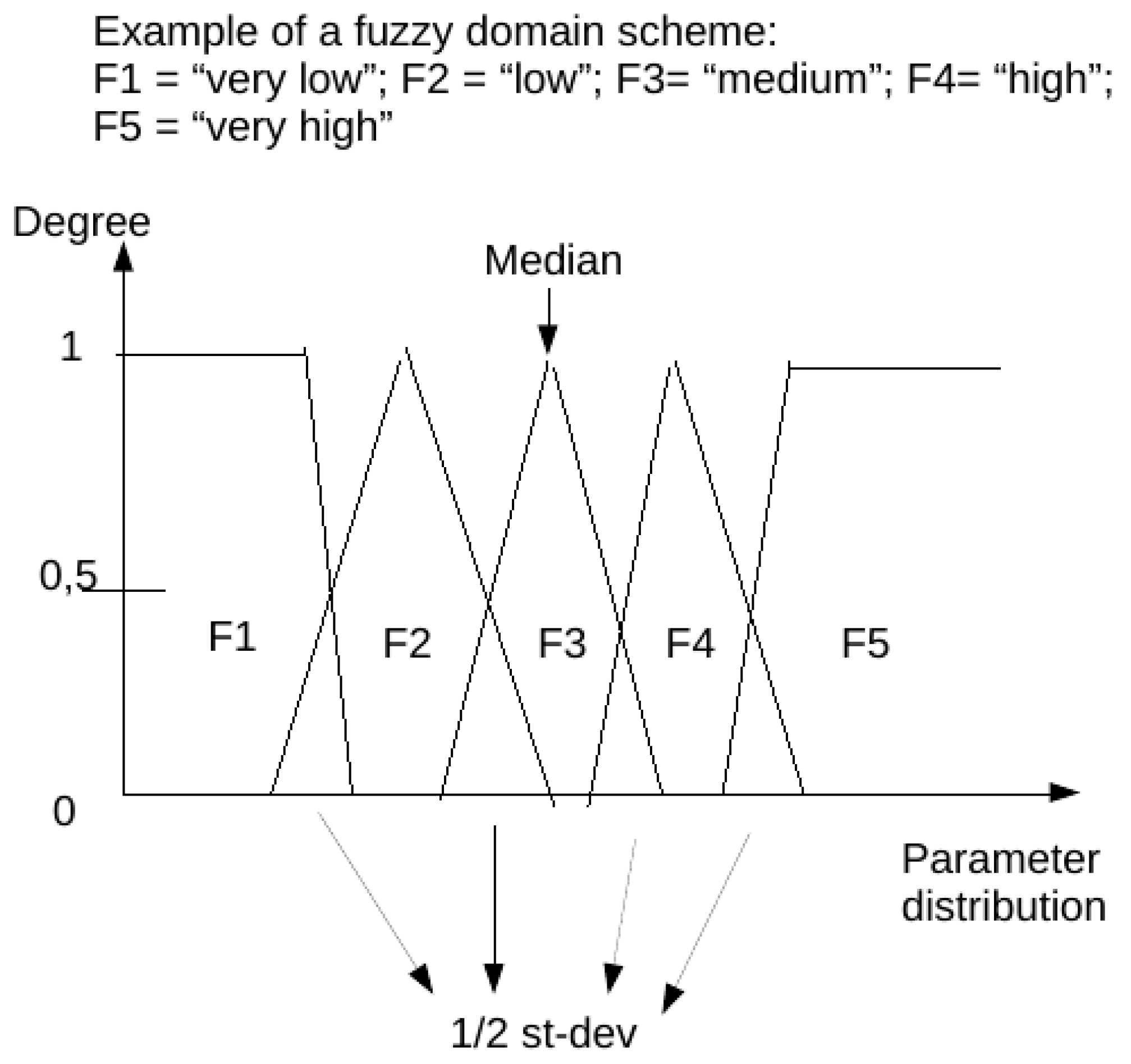
2.3. Fuzzy Domains and Subsets
2.4. Datasets
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Samuel, A.L. Some Studies in Machine Learning Using the Game of Checkers. IBM J. Res. Dev. 1959, 3, 210–229. [Google Scholar] [CrossRef]
- Gutierrez, G. Artificial Intelligence in the Intensive Care Unit. Crit. Care 2020, 24, 101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gavin Edwards discusses about Machine Learning: An Introduction. Available online: https://towardsdatascience.com/machine-learning-an-introduction-23b84d51e6d0 (accessed on 15 January 2022).
- Chollet, F. Deep Learning with Python; Simon and Schuster: New York, NY, USA, 2021. [Google Scholar]
- Hosny, A.; Parmar, C.; Quackenbush, J.; Schwartz, L.H.; Aerts, H.J.W.L. Artificial intelligence in radiology. Nat. Rev. Cancer 2018, 18, 500–510. [Google Scholar] [CrossRef] [PubMed]
- Litjens, G.; Sánchez, C.; Timofeeva, N.; Hermsen, M.; Nagtegaal, I.; Kovacs, I.; van de Kaa, C.H.; Bult, P.; van Ginneken, B.; van der Laak, J. Deep learning as a tool for increased accuracy and efficiency of histopathological diagnosis. Sci. Rep. 2016, 6, 26286. [Google Scholar] [CrossRef] [Green Version]
- Litjens, G.; Sánchez, C.I.; Timofeeva, N.; Hermsen, M.; Nagtegaal, I.; Kovacs, I.; van de Kaa, C.H.; Bult, P.; van Ginneken, B.; van der Laak, J. Surgical robotics beyond enhanced dexterity instrumentation: A survey of machine learning techniques and their role in intelligent and autonomous surgical actions. Int. J. Comput. Assist. Radiol. Surg. 2016, 11, 553–568. [Google Scholar] [CrossRef] [Green Version]
- Johnson, K.; Soto, J.T.; Glicksberg, B.; Shameer, K.; Miotto, R.; Ali, M.; Ashley, E.; Dudley, J.T. Artificial Intelligence in Cardiology. J. Am. Coll. Cardiol. 2018, 71, 2668–2679. [Google Scholar] [CrossRef]
- Tang, T.T.; Zawaski, J.A.; Francis, K.N.; Qutub, A.A.; Gaber, M.W. Image-based Classification of Tumor Type and Growth Rate using Machine Learning: A preclinical study. Sci. Rep. 2019, 9, 12529. [Google Scholar] [CrossRef] [Green Version]
- Muralitharan, S.; Nelson, W.; Di, S.; McGillion, M.; Devereaux, P.; Barr, N.G.; Petch, J. Machine Learning-Based Early Warning Systems for Clinical Deterioration: Systematic Scoping Review. J. Med. Internet Res. 2021, 23, e25187. [Google Scholar] [CrossRef]
- Romero-Brufau, S.; Whitford, D.; Johnson, M.G.; Hickman, J.; Morlan, B.W.; Therneau, T.; Naessens, J.; Huddleston, J.M. Using machine learning to improve the accuracy of patient deterioration predictions: Mayo Clinic Early Warning Score (MC-EWS). J. Am. Med. Inform. Assoc. 2021, 28, 1207–1215. [Google Scholar] [CrossRef]
- Choi, E.; Schuetz, A.; Stewart, W.F.; Sun, J. Using recurrent neural network models for early detection of heart failure onset. J. Am. Med. Inform. Assoc. 2017, 24, 361–370. [Google Scholar] [CrossRef]
- Essay, P.; Balkan, B.; Subbian, V. Decompensation in Critical Care: Early Prediction of Acute Heart Failure Onset. JMIR Med. Inform. 2020, 8, e19892. [Google Scholar] [CrossRef] [PubMed]
- Qian, Q.; Wu, J.; Wang, J.; Sun, H.; Yang, L. Prediction Models for AKI in ICU: A Comparative Study. Int. J. Gen. Med. 2021, 14, 623–632. [Google Scholar] [CrossRef] [PubMed]
- Hur, S.; Ko, R.E.; Yoo, J.; Ha, J.; Cha, W.C.; Chung, C.R. A Machine Learning-Based Algorithm for the Prediction of Intensive Care Unit Delirium (PRIDE): Retrospective Study. JMIR Med. Inform. 2021, 9, e23401. [Google Scholar] [CrossRef] [PubMed]
- Ginestra, J.C.; Giannini, H.; Schweickert, W.D.; Meadows, L.; Lynch, M.J.; Pavan, K.; Chivers, C.J.; Draugelis, M.; Donnelly, P.J.; Fuchs, B.D.; et al. Clinician Perception of a Machine Learning-Based Early Warning System Designed to Predict Severe Sepsis and Septic Shock. Crit. Care Med. 2019, 47, 1477–1484. [Google Scholar] [CrossRef] [PubMed]
- Warttig, S.; Alderson, P.; Evans, D.J.; Lewis, S.R.; Kourbeti, I.S.; Smith, A.F. Automated monitoring compared to standard care for the early detection of sepsis in critically ill patients. Cochrane Database Syst. Rev. 2018, 6, CD012404. [Google Scholar] [CrossRef]
- Yuan, S.; Sun, Y.; Xiao, X.; Long, Y.; He, H. Using Machine Learning Algorithms to Predict Candidaemia in ICU Patients with New-Onset Systemic Inflammatory Response Syndrome. Front. Med. 2021, 8, 720926. [Google Scholar] [CrossRef]
- Ripoli, A.; Sozio, E.; Sbrana, F.; Bertolino, G.; Pallotto, C.; Cardinali, G.; Meini, S.; Pieralli, F.; Azzini, A.M.; Concia, E.; et al. Personalized machine learning approach to predict candidemia in medical wards. Infection 2020, 48, 749–759. [Google Scholar] [CrossRef]
- Su, L.; Xu, Z.; Chang, F.; Ma, Y.; Liu, S.; Jiang, H.; Wang, H.; Li, D.; Chen, H.; Zhou, X.; et al. Early Prediction of Mortality, Severity, and Length of Stay in the Intensive Care Unit of Sepsis Patients Based on Sepsis 3.0 by Machine Learning Models. Front. Med. 2021, 8, 664966. [Google Scholar] [CrossRef]
- Barchitta, M.; Maugeri, A.; Favara, G.; Riela, P.; Gallo, G.; Mura, I.; Agodi, A. Early Prediction of Seven-Day Mortality in Intensive Care Unit Using a Machine Learning Model: Results from the SPIN-UTI Project. J. Clin. Med. 2021, 10, 992. [Google Scholar] [CrossRef]
- Corny, J.; Rajkumar, A.; Martin, O.; Dode, X.; Lajonchère, J.-P.; Billuart, O.; Bézie, Y.; Buronfosse, A. A machine learning-based clinical decision support system to identify prescriptions with a high risk of medication error. J. Am. Med. Inform. Assoc. 2020, 27, 1688–1694. [Google Scholar] [CrossRef]
- Helgason, C.M. The Application of Fuzzy Logic to the Prescription of Antithrombotic Agents in the Elderly. Drugs Aging 2004, 21, 731–736. [Google Scholar] [CrossRef]
- Evans, L.; Rhodes, A.; Alhazzani, W.; Antonelli, M.; Coopersmith, C.M.; French, C.; Machado, F.R.; Mcintyre, L.; Ostermann, M.; Prescott, H.C.; et al. Surviving sepsis campaign: International guidelines for management of sepsis and septic shock 2021. Intensive Care Med. 2021, 47, 1181–1247. [Google Scholar] [CrossRef]
- Postma, D.F.; van Werkhoven, H.; Van Elden, L.; Thijsen, S.F.; Hoepelman, A.I.; Kluytmans, J.A.; Boersma, W.G.; Compaijen, C.J.; Van Der Wall, E.; Prins, J.M.; et al. Antibiotic treatment strategies for community-acquired pneumonia in adults. N. Engl. J. Med. 2015, 372, 1312–1323. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luz, C.F.; Vollmer, M.; Decruyenaere, J.; Nijsten, M.W.; Glasner, C.; Sinha, B. Machine learning in infection management using routine electronic health records: Tools, techniques, and reporting of future technologies. Clin. Microbiol. Infect. 2020, 26, 1291–1299. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peiffer-Smadja, N.; Rawson, T.M.; Ahmad, R.; Buchard, A.; Georgiou, P.; Lescure, F.-X.; Birgand, G.; Holmes, A.H. Machine learning for clinical decision support in infectious diseases: A narrative review of current applications. Clin. Microbiol. Infect. 2020, 26, 584–595. [Google Scholar] [CrossRef] [PubMed]
- Catho, G.; de Kraker, M.; Suter, B.W.; Valotti, R.; Harbarth, S.; Kaiser, L.; Elzi, L.; Meyer, R.; Bernasconi, E.; Huttner, B. Study protocol for a multicentre, cluster randomised, superiority trial evaluating the impact of computerised decision support, audit and feedback on antibiotic use: The COMPuterized Antibiotic Stewardship Study (COMPASS). BMJ Open 2018, 8, e022666. [Google Scholar] [CrossRef]
- Heng, S.T.; Wong, J.; Young, B.; Tay, H.L.; Tan, S.H.; Yap, M.Y.; Teng, C.B.; Ang, B.; Lee, T.H.; Tan, H.L.; et al. Effective Antimicrobial StewaRdship StrategIES (ARIES): Cluster Randomized Trial of Computerized Decision Support System and Prospective Review and Feedback. Open Forum Infect. Dis. 2020, 7, ofaa254. [Google Scholar] [CrossRef]
- Catho, G.; Centemero, N.S.; Suter, B.W.; Vernaz, N.; Portela, J.; Da Silva, S.; Valotti, R.; Coray, V.; Pagnamenta, F.; Ranzani, A.; et al. How to Develop and Implement a Computerized Decision Support System Integrated for Antimicrobial Stewardship? Experiences from Two Swiss Hospital Systems. Front. Digit. Health 2021, 2, 583390. [Google Scholar] [CrossRef]
- Yuan, X.; Chen, K.; Zhao, W.; Hu, S.; Yu, F.; Diao, X.; Chen, X.; Hu, S. Open-label, single-centre, cluster-randomised controlled trial to Evaluate the Potential Impact of Computerised antimicrobial stewardship (EPIC) on the antimicrobial use after cardiovascular surgeries: EPIC trial study original protocol. BMJ Open 2020, 10, e039717. [Google Scholar] [CrossRef]
- Hirano, Y.; Kondo, Y.; Hifumi, T.; Yokobori, S.; Kanda, J.; Shimazaki, J.; Hayashida, K.; Moriya, T.; Yagi, M.; Takauji, S.; et al. Machine learning-based mortality prediction model for heat-related illness. Sci. Rep. 2021, 11, 9501. [Google Scholar] [CrossRef]
- Bloch, E.; Rotem, T.; Cohen, J.; Singer, P.; Aperstein, Y. Machine Learning Models for Analysis of Vital Signs Dynamics: A Case for Sepsis Onset Prediction. J. Health Eng. 2019, 2019, 5930379. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pettinati, M.J.; Chen, G.; Rajput, K.S.; Selvaraj, N. Practical Machine Learning-Based Sepsis Prediction. Annu. Int. Conf. IEEE Eng. Med. Biol. Soc. 2020, 2020, 4986–4991. [Google Scholar] [CrossRef] [PubMed]
- Mao, Q.; Jay, M.; Hoffman, J.L.; Calvert, J.; Barton, C.; Shimabukuro, D.; Shieh, L.; Chettipally, U.; Fletcher, G.; Kerem, Y.; et al. Multicentre validation of a sepsis prediction algorithm using only vital sign data in the emergency department, general ward and ICU. BMJ Open 2018, 8, e017833. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fleuren, L.M.; Klausch, T.L.T.; Zwager, C.L.; Schoonmade, L.J.; Guo, T.; Roggeveen, L.F.; Swart, E.L.; Girbes, A.R.J.; Thoral, P.; Ercole, A.; et al. Machine learning for the prediction of sepsis: A systematic review and meta-analysis of diagnostic test accuracy. Intensive Care Med. 2020, 46, 383–400. [Google Scholar] [CrossRef] [Green Version]
- Hou, N.; Li, M.; He, L.; Xie, B.; Wang, L.; Zhang, R.; Yu, Y.; Sun, X.; Pan, Z.; Wang, K. Predicting 30-days mortality for MIMIC-III patients with sepsis-3: A machine learning approach using XGboost. J. Transl. Med. 2020, 18, 462. [Google Scholar] [CrossRef]
- Wang, D.; Li, J.; Sun, Y.; Ding, X.; Zhang, X.; Liu, S.; Han, B.; Wang, H.; Duan, X.; Sun, T. A Machine Learning Model for Accurate Prediction of Sepsis in ICU Patients. Front. Public Health 2021, 9, 754348. [Google Scholar] [CrossRef]
- Dong, J.; Feng, T.; Thapa-Chhetry, B.; Cho, B.G.; Shum, T.; Inwald, D.P.; Newth, C.J.L.; Vaidya, V.U. Machine learning model for early prediction of acute kidney injury (AKI) in pediatric critical care. Crit. Care 2021, 25, 288. [Google Scholar] [CrossRef]
- Ozrazgat-Baslanti, T.; Loftus, T.J.; Ren, Y.; Ruppert, M.M.; Bihorac, A. Advances in artificial intelligence and deep learning systems in ICU-related acute kidney injury. Curr. Opin. Crit. Care 2021, 27, 560–572. [Google Scholar] [CrossRef]
- He, J.; Lin, J.; Duan, M. Application of Machine Learning to Predict Acute Kidney Disease in Patients with Sepsis Associated Acute Kidney Injury. Front. Med. 2021, 8, 792974. [Google Scholar] [CrossRef]
- Vagliano, I.; Hsu, W.H.; Schut, M.C. Machine Learning, Clinical Notes and Knowledge Graphs for Early Prediction of Acute Kidney Injury in the Intensive Care. Stud. Health Technol. Inform. 2022, 289, 329–332. [Google Scholar] [CrossRef]
- Liu, J.; Wu, J.; Liu, S.; Li, M.; Hu, K.; Li, K. Predicting mortality of patients with acute kidney injury in the ICU using XGBoost model. PLoS ONE 2021, 16, e0246306. [Google Scholar] [CrossRef] [PubMed]
- Alfieri, F.; Ancona, A.; Tripepi, G.; Crosetto, D.; Randazzo, V.; Paviglianiti, A.; Pasero, E.; Vecchi, L.; Cauda, V.; Fagugli, R.M. A deep-learning model to continuously predict severe acute kidney injury based on urine output changes in critically ill patients. J. Nephrol. 2021, 34, 1875–1886. [Google Scholar] [CrossRef] [PubMed]
- Vagliano, I.; Lvova, O.; Schut, M.C. Interpretable and Continuous Prediction of Acute Kidney Injury in the Intensive Care. Stud. Health Technol. Inform. 2021, 281, 103–107. [Google Scholar] [CrossRef] [PubMed]
- Staziaki, P.V.; Wu, D.; Rayan, J.C.; Santo, I.D.O.; Nan, F.; Maybury, A.; Gangasani, N.; Benador, I.; Saligrama, V.; Scalera, J.; et al. Machine learning combining CT findings and clinical parameters improves prediction of length of stay and ICU admission in torso trauma. Eur. Radiol. 2021, 31, 5434–5441. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, M.; Corbin, C.K.; Eulalio, T.; Ostberg, N.P.; Machiraju, G.; Marafino, B.J.; Baiocchi, M.; Rose, C.; Chen, J.H. Developing machine learning models to personalize care levels among emergency room patients for hospital admission. J. Am. Med. Inform. Assoc. 2021, 28, 2423–2432. [Google Scholar] [CrossRef]
- Zhu, Y.; Zhang, J.; Wang, G.; Yao, R.; Ren, C.; Chen, G.; Jin, X.; Guo, J.; Liu, S.; Zheng, H.; et al. Machine Learning Prediction Models for Mechanically Ventilated Patients: Analyses of the MIMIC-III Database. Front. Med. 2021, 8, 662340. [Google Scholar] [CrossRef]
- Ossai, C.I.; Wickramasinghe, N. Intelligent decision support with machine learning for efficient management of mechanical ventilation in the intensive care unit—A critical overview. Int. J. Med. Inform. 2021, 150, 104469. [Google Scholar] [CrossRef]
- Otaguro, T.; Tanaka, H.; Igarashi, Y.; Tagami, T.; Masuno, T.; Yokobori, S.; Matsumoto, H.; Ohwada, H.; Yokota, H. Machine Learning for Prediction of Successful Extubation of Mechanical Ventilated Patients in an Intensive Care Unit: A Retrospective Observational Study. J. Nippon Med. Sch. 2021, 88, 408–417. [Google Scholar] [CrossRef]
- Rahman, A.; Chang, Y.; Dong, J.; Conroy, B.; Natarajan, A.; Kinoshita, T.; Vicario, F.; Frassica, J.; Xu-Wilson, M. Early prediction of hemodynamic interventions in the intensive care unit using machine learning. Crit. Care 2021, 25, 388. [Google Scholar] [CrossRef]
- Comoretto, R.I.; Azzolina, D.; Amigoni, A.; Stoppa, G.; Todino, F.; Wolfler, A.; Gregori, D. on Behalf of The TIPNet Study Group. Predicting Hemodynamic Failure Development in PICU Using Machine Learning Techniques. Diagnostics 2021, 11, 1299. [Google Scholar] [CrossRef]
- van der Ven, W.H.; Terwindt, L.E.; Risvanoglu, N.; Ie, E.L.K.; Wijnberge, M.; Veelo, D.P.; Geerts, B.F.; Vlaar, A.P.J.; van der Ster, B.J.P. Performance of a machine-learning algorithm to predict hypotension in mechanically ventilated patients with COVID-19 admitted to the intensive care unit: A cohort study. J. Clin. Monit. Comput. 2021; 1–9, Epub ahead of print. [Google Scholar] [CrossRef]
- Radhakrishnan, S.; Nair, S.G.; Isaac, J. Analysis of parameters affecting blood oxygen saturation and modeling of fuzzy logic system for inspired oxygen prediction. Comput. Methods Programs Biomed. 2019, 176, 43–49. [Google Scholar] [CrossRef] [PubMed]
- Alexis Ruiz, A.; Wyszyńska, P.K.; Laudanski, K. Narrative Review of Decision-Making Processes in Critical Care. Anesth. Analg. 2019, 128, 962–970. [Google Scholar] [CrossRef] [PubMed]
- Petch, J.; Di, S.; Nelson, W. Opening the Black Box: The Promise and Limitations of Explainable Machine Learning in Cardiology. Can. J. Cardiol. 2022, 38, 204–213. [Google Scholar] [CrossRef] [PubMed]
- Aslam, T.M.; Hoyle, D.C. Translating the Machine: Skills that Human Clinicians Must Develop in the Era of Artificial Intelligence. Ophthalmol. Ther. 2022, 11, 69–80. [Google Scholar] [CrossRef] [PubMed]
- Dalatu, P.; Midi, H. New Approaches to Normalization Techniques to Enhance K-Means Clustering Algorithm. Malays. J. Math. Sci. 2020, 14, 41–62. [Google Scholar]
- Al-Dmour, J.A.; Sagahyroon, A.; Al-Ali, A.R.; Abusnana, S. A fuzzy logic-based warning system for patients classification. Health Inform. J. 2019, 25, 1004–1024. [Google Scholar] [CrossRef]
- Zhengbing, H.; Bodyanskiy, Y.V.; Tyshchenko, K.O.; Samitova, V.O. Fuzzy Clustering Data Given in the Ordinal Scale. I. J. Intell. Syst. Appl. 2017, 9, 67–74. [Google Scholar]
- Huang, Z. Clustering large data sets with mixed numeric and categorical values. In Proceedings of the First Pacific Asia Knowledge Discovery and Data Mining Conference, Singapore; 1997; pp. 21–34. [Google Scholar]
- Huang, Z. Extensions to the k-modes algorithm for clustering large data sets with categorical values. Data Min. Knowl. Discov. 1998, 2, 283–304. [Google Scholar] [CrossRef]
- Rousseeuw, P.J. Silhouettes: A graphical aid to the interpretation and validation of cluster analysis. J. Comput. Appl. Math. 1987, 20, 53–65. [Google Scholar] [CrossRef] [Green Version]
- Silhouette Visualizer. Available online: https://www.scikit-yb.org/en/latest/api/cluster/silhouette.html (accessed on 15 January 2022).
- Cao, F.; Liang, J.; Bai, L. A new initialization method for categorical data clustering. Expert Syst. Appl. 2009, 36, 10223–10228. [Google Scholar] [CrossRef]
- Gardner-Thorpe, J.; Love, N.; Wrightson, J.; Walsh, S.; Keeling, N. The value of Modified Early Warning Score (MEWS) in surgical in-patients: A prospective observational study. Ann. R. Coll. Surg. Engl. 2006, 88, 571–575. [Google Scholar] [CrossRef] [PubMed]
- Papachristou, N.; Barnaghi, P.; Cooper, B.A.; Hu, X.; Maguire, R.; Apostolidis, K.; Armes, J.; Conley, Y.P.; Hammer, M.; Katsaragakis, S.; et al. Congruence Between Latent Class and K-Modes Analyses in the Identification of Oncology Patients with Distinct Symptom Experiences. J. Pain Symptom Manag. 2018, 55, 318–333.e4. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Cluster | N Patterns | Non-Null | F1 | F2 | F3 | F4 | F5 |
|---|---|---|---|---|---|---|---|
| T0 | 3551 | 10,324 | 0.24 | 0.38 | 0.22 | 0.09 | 0.07 |
| T1 | 1159 | 4437 | 0.11 | 0.49 | 0.10 | 0.11 | 0.20 |
| T2 | 1569 | 4257 | 0.21 | 0.47 | 0.13 | 0.10 | 0.09 |
| T3 | 1484 | 5739 | 0.16 | 0.34 | 0.14 | 0.14 | 0.22 |
| Cluster | N | Non-Null | F1 | F2 | F3 | F4 | F5 |
|---|---|---|---|---|---|---|---|
| M0 | 11,520 | 80,158 | 0.07 | 0.17 | 0.27 | 0.34 | 0.14 |
| M1 | 10,017 | 73,525 | 0.09 | 0.38 | 0.34 | 0.10 | 0.10 |
| M2 | 14,624 | 93,037 | 0.10 | 0.27 | 0.35 | 0.14 | 0.14 |
| M3 | 7717 | 49,562 | 0.08 | 0.20 | 0.33 | 0.30 | 0.08 |
| M4 | 2391 | 16,732 | 0.09 | 0.34 | 0.28 | 0.25 | 0.05 |
| M5 | 3358 | 22,431 | 0.07 | 0.32 | 0.24 | 0.24 | 0.13 |
| M6 | 8339 | 54,657 | 0.12 | 0.39 | 027 | 0.10 | 0.12 |
| Mean | Minimum | Maximum | Observed | Median | Range | Standard Deviation | |||
|---|---|---|---|---|---|---|---|---|---|
| Days | 6.43 | 0 | 22 | 57329 | 11 | 22 | 5.7 | ||
| Very low (F1) | Low (F2) | Medium (F3) | High (F4) | Very high (F5) | |||||
| VLL | VLH | LL | LH | NL | NH | HL | HH | VHL | VHH |
| −1.8 | 3.6 | 1.8 | 9.1 | 7.3 | 14.6 | 12.8 | 20.2 | 18.3 | 23.8 |
| M0 | M1 | M2 | M3 | M4 | M5 | M6 | |
|---|---|---|---|---|---|---|---|
| T0 | 0.07 | 0.05 | 0.16 | 0.04 | 0.01 | 0.01 | 0.10 |
| T1 | 0.04 | 0.02 | 0.07 | 0.02 | 0.00 | 0.01 | 0.04 |
| T2 | 0.04 | 0.03 | 0.07 | 0.02 | 0.01 | 0.01 | 0.04 |
| T3 | 0.03 | 0.02 | 0.05 | 0.02 | 0.00 | 0.01 | 0.03 |
| Nabtcl 1 | Nabtcl 2 | Nabtcl 3 | Nabtcl 4 | ||||||
|---|---|---|---|---|---|---|---|---|---|
| N ICU stays (Total 4129) | 2377 | 1414 | 306 | 32 | |||||
| N hours (Total 543,190) | 137,667 | 276,361 | 113,197 | 15,965 | |||||
| Therapy clusters per ICU stay | Fuzzy subsets | ||||||||
| Therapy cluster | Nabtcl 1 | Nabtcl 2 | Nabtcl 3 | Nabtcl 4 | F1 | F2 | F3 | F4 | F5 |
| T0 | 0.78 | 0.38 | 0.25 | 0.12 | 0.24 | 0.38 | 0.22 | 0.09 | 0.07 |
| T1 | 0.00 | 0.24 | 0.28 | 0.40 | 0.11 | 0.49 | 0.10 | 0.11 | 0.20 |
| T2 | 0.13 | 0.22 | 0.24 | 0.28 | 0.21 | 0.47 | 0.13 | 0.10 | 0.09 |
| T3 | 0.09 | 0.16 | 0.23 | 0.21 | 0.16 | 0.34 | 0.14 | 0.14 | 0.22 |
| Chi-square 100,641.5; p < 0.05 | |||||||||
| Monitoring clusters per ICU stay | Fuzzy subsets | ||||||||
| Monitoring cluster | Nabtcl 1 | Nabtcl 2 | Nabtcl 3 | Nabtcl 4 | F1 | F2 | F3 | F4 | F5 |
| M0 | 0.16 | 0.16 | 0.18 | 0.23 | 0.07 | 0.17 | 0.27 | 0.34 | 0.14 |
| M1 | 0.12 | 0.13 | 0.12 | 0.12 | 0.09 | 0.38 | 0.34 | 0.10 | 0.10 |
| M2 | 0.35 | 0.34 | 0.34 | 0.31 | 0.10 | 0.27 | 0.35 | 0.14 | 0.14 |
| M3 | 0.09 | 0.10 | 0.10 | 0.09 | 0.08 | 0.20 | 0.33 | 0.30 | 0.08 |
| M4 | 0.03 | 0.03 | 0.04 | 0.02 | 0.09 | 0.34 | 0.28 | 0.25 | 0.05 |
| M5 | 0.03 | 0.03 | 0.04 | 0.04 | 0.07 | 0.32 | 0.24 | 0.24 | 0.13 |
| M6 | 0.22 | 0.21 | 0.19 | 0.19 | 0.12 | 0.39 | 0.27 | 0.10 | 0.12 |
| Chi-square 1918.8; p <0.05 | |||||||||
| Overall Consecutive Days of therapy as fuzzy subsets | |||||||||
| Fuzzy subset | Nabtcl 1 | Nabtcl 2 | Nabtcl 3 | Nabtcl 4 | |||||
| F1 | 0.28 | 0.14 | 0.07 | 0.06 | |||||
| F2 | 0.37 | 0.38 | 0.25 | 0.22 | |||||
| F3 | 0.13 | 0.16 | 0.17 | 0.16 | |||||
| F4 | 0.08 | 0.11 | 0.15 | 0.17 | |||||
| F5 | 0.14 | 0.22 | 0.35 | 0.39 | |||||
| Chi-square 40,867.1; p < 0.05 | |||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maviglia, R.; Michi, T.; Passaro, D.; Raggi, V.; Bocci, M.G.; Piervincenzi, E.; Mercurio, G.; Lucente, M.; Murri, R. Machine Learning and Antibiotic Management. Antibiotics 2022, 11, 304. https://doi.org/10.3390/antibiotics11030304
Maviglia R, Michi T, Passaro D, Raggi V, Bocci MG, Piervincenzi E, Mercurio G, Lucente M, Murri R. Machine Learning and Antibiotic Management. Antibiotics. 2022; 11(3):304. https://doi.org/10.3390/antibiotics11030304
Chicago/Turabian StyleMaviglia, Riccardo, Teresa Michi, Davide Passaro, Valeria Raggi, Maria Grazia Bocci, Edoardo Piervincenzi, Giovanna Mercurio, Monica Lucente, and Rita Murri. 2022. "Machine Learning and Antibiotic Management" Antibiotics 11, no. 3: 304. https://doi.org/10.3390/antibiotics11030304