3. Discussion
The aim of our study was to determine phenotypic AMR data for bacterial pathogens of dogs and cats suffering from UTI and to collect metadata to identify possible risk factors for UTI in these animals.
Consistent with the results from previous studies, significantly more samples from female than from male dogs yielded bacterial growth (
p < 0.001), although the overall number of samples submitted from males was higher [
30,
31,
32,
33]. Likewise, in cats, the number of samples sent and thus the number of animals presenting with symptoms of lower urinary tract infection (LUTD) was much higher in males than in females, although samples from females more often yielded bacterial growth. This impression also emerged in other European studies: while male cats were more likely to have idiopathic LUTD, uroliths, or urethral plugs, evidence for an etiological role of bacteria as the cause of these symptoms was more often provided in female cats [
2,
3,
34,
35]. Additionally, in our study, a positive microbiological culture was significantly more often found among samples from neutered dogs (
p = 0.023) and cats (
p < 0.0001) compared with non-neutered animals.
UTI is typically caused by bacteria invading the urinary tract from the colon or skin [
22,
36]. It is commonly suggested that an increased detection of bacteria in female urethral samples is mainly due to anatomical reasons, i.e., the length of the urethra and the short distance between the urethral meatus and anus [
22,
37]. Moreover, the surgical removal of the uterus and ovaries (ovariohysterectomy) might impair the self-defence mechanisms of the bladder [
38,
39]. With the cessation of estrogen release, the production of mucopolysaccharides, which prevent bacterial pathogens from adhering to the bladder epithelium, is no longer under control. For males, an antimicrobial effect of prostatic secretions has been noted [
40].
Feline lower urinary tract disease (FLUTD) is mostly due to feline idiopathic cystitis (FIC) or urolithiasis and less frequently caused by bacterial infections [
34]. Bacterial UTI has been described as the cause of FLUTD in only 7.8–18.9% of cases studied in Europe [
2,
3,
34,
35,
41]. In our study, 38.5% of the feline samples yielded bacterial growth. This could be explained with the higher percentage of female cats in our study (40%) compared to the above-mentioned studies (13–26%).
Dorsch et al. (2014) reported that a majority of cats suffering from FLUTD had relevant predisposing comorbidities [
2]. This was in line with our observations: 72.9% of the attending veterinarians reported a comorbidity in the questionnaire. Almost 23% of the animals suffered from urolithiasis, a higher percentage than previously detected [
2,
3,
35,
41]. Only Gerber et al. (2005) reported a similar percentage (22%) of cats with uroliths, although it must be considered that nearly 90% of their study population consisted of males [
34].
A limitation of our study was the inability to distinguish between asymptomatic bacteriuria (ASB) and urinary tract infection. According to current guidelines, ASB is defined as “the presence of bacteria in urine as determined by positive bacterial culture from a properly collected urine specimen, in the absence of clinical evidence of infectious urinary tract disease” [
21] (p. 17). Since most veterinarians did not report back whether the animal had clinical signs, a bias in our results due to cases of ASB cannot be ruled out.
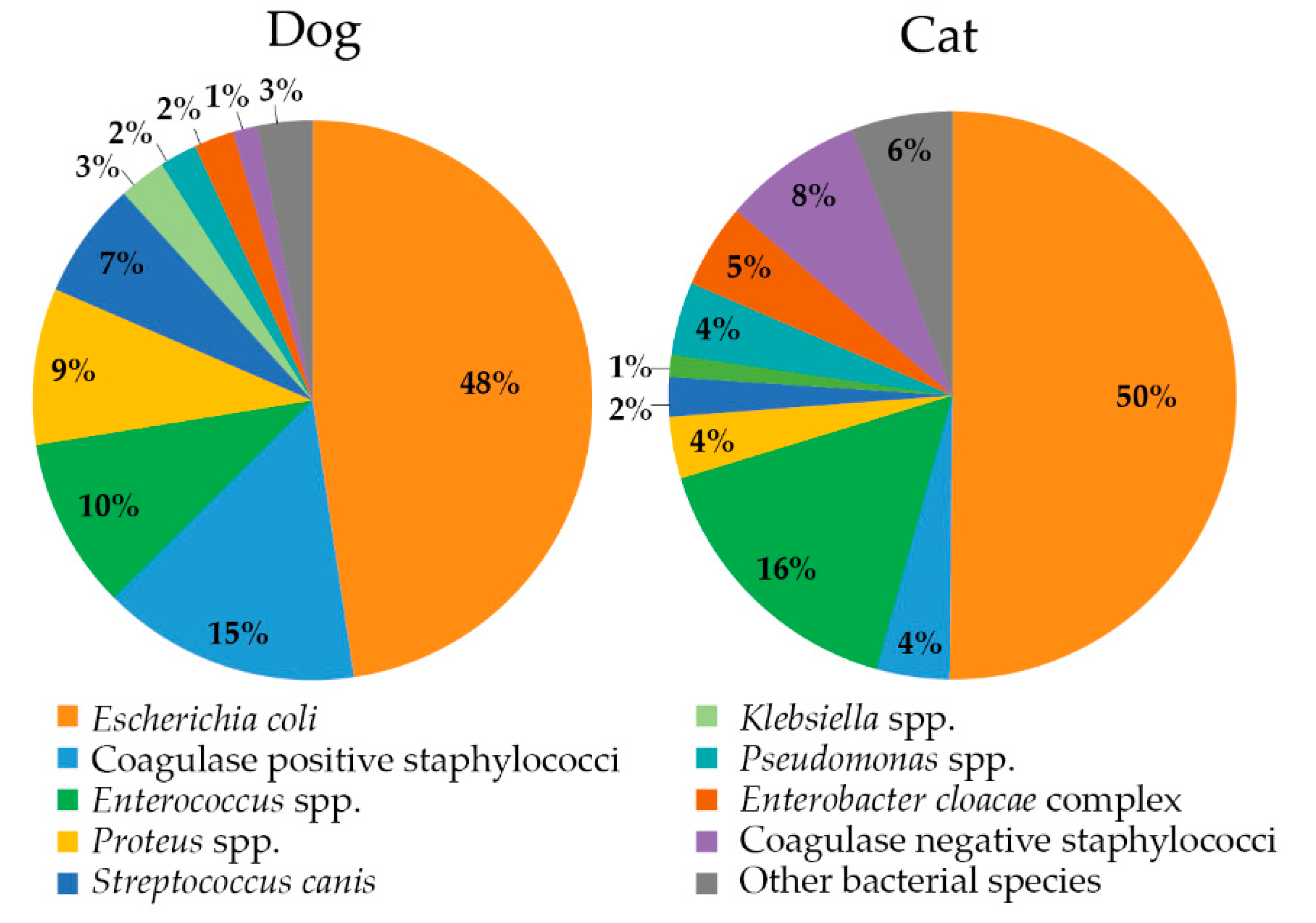
The incidence of polybacterial (22.6%) versus monobacterial (77.4%) infections in dogs and cats was consistent with other studies [
32,
42,
43]. Interestingly, mixed infection with more than three pathogens at the same time only occurred in dogs. Also in accordance with other studies worldwide, the most prevalent bacterium isolated from UTI in cats and dogs was
E. coli, followed by
Enterococcus spp., CoPS, and
Proteus spp. [
13,
17,
30,
31,
32,
44,
45,
46,
47,
48,
49]. CoPS,
Proteus spp., and
Sc. canis were preferentially found in dogs, whereas
Enterococcus spp. and
S. felis were more frequently found in cats (all with statistical support). Except for
E. coli, a predilection of a bacterial species for either dogs or cats has also been shown in other studies that compared feline and canine uropathogens [
17,
48,
49,
50]. However, a separation between CoPS and CoNS was rarely performed. If so,
S. felis was exclusively found in cats, and CoPS, especially
S. pseudintermedius, were significantly more often detected in dogs [
43]. Recent studies showed that the CoPS species
S. pseudintermedius is not part of the physiological skin microbiota of cats [
51,
52,
53]. Given the fact that one of the most common causes of UTI is ascending infection from skin, this may explain the much lower prevalence of
S. pseudintermedius as a uropathogen in cats compared with dogs. The majority of isolated enterococci species consisted of
E. faecalis (71.8%), followed by
E. faecium (7.6%) and seven other enterococci species (20.5%). The fact that
E. faecalis is more abundant can be explained by its increased virulence: it has, for example, a more pronounced ability to form biofilms, so that it adheres more strongly to biotic surfaces and is thus protected from urine flushing and local endogenous defences and antimicrobial substances [
54,
55,
56].
E. faecium, meanwhile, is much more resistant: all
E. faecium isolates presented an MDR pattern.
For the treatment of uropathogenic
E. coli, our results showed a reduced susceptibility to AMP in both animal species, which agrees with several other studies [
30,
31,
44,
57,
58]. Likewise, most of our and previously published strains were found to be AMC-susceptible according to CLSI document VET01S. For the other antimicrobials commonly used to treat UTI caused by UPEC, resistance of
E. coli was low in both animal species.
The second most isolated Gram-negative pathogen was Proteus spp. In contrast to cats, where susceptibility to AMP, SXT, ENR, and PRA was moderate to high (81.8–90.9%), dog isolates showed reduced susceptibility to AMP (69.8%), SXT (77.8%), ENR (77.8%), and PRA (73.0%). AMC continued to prove a good option for treatment of UTI with 96.8% of isolates being AMC susceptible.
Except for AMP (48.1%, cat-specific breakpoints applied in accordance with CLSI document VET09), susceptibility of canine CoPS to antibiotics recommended for the treatment of UTI was > 90%. In cats, however, the results are more worrying: even though only 4.2% CoPS were identified among all feline UTI cases, these isolates showed more or less reduced susceptibility to almost all antibiotics, including AMC (38.5% susceptible isolates), AMP (15.4%), SXT (53.8%), and the FQs (46.2%). Only for CFV, two-thirds of the isolates were still susceptible (75.0%). Almost 70% of feline CoPS exhibited an MDR phenotype. By comparing MIC
50 and MIC
90, feline CoPS proved to be significantly more resistant to all tested antibiotics (excluding SXT:
p = 0.0504) than canine CoPS (AMP
p = 0.0026, AMC
p < 0.001, CFX
p = 0.0023, CFV
p < 0.001, ENR
p = 0.0007, GEN
p < 0.001, and PRA
p = 0.0002). The lower susceptibility of feline staphylococci compared with canine isolates is consistent with recent studies. In a study from Spain, almost 46% of CoPS isolates recovered from cats with signs of UTI were categorized as MDR, and 23% were XDR [
49]. Marques et al. (2018) reported 12 times less CoPS in cats than in dogs. However, nearly all (91%) methicillin-resistant
S. aureus (MRSA) isolates detected in their study originated from cats [
13]. A study from Italy revealed resistance of three
S. pseudintermedius isolates from cats to all UTI-relevant antimicrobials and resistance of two
S. aureus isolates, also from cats, to all β-lactam antimicrobials, as well as reduced susceptibility to FQs [
20].
In
Enterococcus spp. isolates from our study, antimicrobial susceptibility differed only slightly between dog and cat isolates. As more than 90% of the isolates were susceptible to AMC and AMX, these drugs should be considered as agents of choice. Although in 87.5% of the isolates MIC values for ENR and PRA ranged between 0.03125 and 1 mg/L, FQs cannot be recommend for the treatment of enterococcal UTI because of the reduced efficacy of FQs against enterococci in vivo [
29]. The validity of these results is limited by the lack of animal species- or even human-derived breakpoints for enterococci, as only for AMP is a human-derived CLSI breakpoint given. As shown in
Figure 3, the manufacturer’s breakpoint interpretation of susceptible, intermediate, and resistant (S/I/R) appears reasonable. The MIC data distribution is bimodal, suggesting there might be a resistant subgroup of isolates [
59]. Naturally, enterococci are not the only bacteria with a bimodal distribution. For example, the distribution of ENR- and PRA-MIC data of
E. coli also shows this distribution (
Table 6).
The percentage of
P. aeruginosa was significantly higher in samples from animals with repeated samples (four or more) during the study period (10.5%) compared to the entire sample pool (2.8%). Repeated submission of samples could suggest recurrent UTI in these animals. Indeed, increased isolation rates of
P. aeruginosa in samples from recurrent UTIs are consistent with previous studies, as they have many intrinsic resistances and are often MDR (41.7% in our study) [
32,
60]. In case of
P. aeruginosa infection, FQs are considered the drugs of choice. Notably, our data showed reduced susceptibility for a considerable part of these isolates (dog, ENR 66.7%, PRA 16.6%; cat, ENR and PRA 50%). The isolates showed a much higher susceptibility to gentamicin; however, the use of aminoglycosides in UTI is limited: they are potentially nephrotoxic, must be administered parenterally on a daily schedule, have significantly decreased activity in acidic urine, and are potentially inactivated by purulent debris [
61].
Overall, the number of MDR isolates was significantly higher in Gram-positive cocci (
Enterococcus spp., 50.4%; CoPS, 42.7%;
Sc. canis, 11.3%;
S. felis, 0%; total, 37.2%) than in Gram-negative species (
E. coli, 11.9%;
Proteus spp., 18.9%;
ECC, 25.8%;
Klebsiella spp., 21.7%;
P. aeruginosa, 41.7%; total, 14.8%) (
p < 0.001). Although
E. coli was the most frequently detected uropathogen, the number of MDR isolates was low compared to other
Enterobacterales, which is consistent with the results from other studies [
13,
49]. Among Gram-positive cocci, particularly
Enterococcus spp. isolates showed a high number of MDR bacteria. The frequency of MDR enterococci from the urine of dogs and cats varied largely among different studies (20–100%) but is partially comparable to our findings [
31,
43,
46,
54,
62,
63]. It should be noted that most veterinarians would rather submit urine specimens in case antimicrobial treatment without prior urine culture and antimicrobial susceptibility data (empiric therapy) failed or if the patient suffers from recurrent infection (either relapsing infection or reinfection) [
64]. In other words, the corresponding isolates have most likely been previously exposed to antimicrobials and might have developed resistance. This is supported by our data as according to the replies to the questionnaire: 47.7% of the animals have undergone antimicrobial treatment prior to sampling and culturing of bacteria [
65,
66]. Nonetheless, unlike with livestock, MDR infections are more common in companion animals, and the treatment of such infections is challenging. In particular serious cases, it may even create the need for off-label use of antimicrobials reserved for humans [
67].
International guidelines for the management of UTI have been available from the International Society for Companion Animal Infectious Diseases since 2011 and in a current iteration (2019). Recommendations for the treatment of UTI are also available in several national guidelines online or in textbook form [
21,
61,
68,
69,
70,
71,
72,
73]. In the vast majority of these documents, a classification is made between sporadic bacterial cystitis (formerly termed as uncomplicated cystitis) and recurrent cystitis (complicated cystitis). For the treatment of sporadic cystitis, first-line antibiotics such as AMX or SXT are recommended. The use of a β-lactamase inhibitor such as clavulanic acid should only be used for empirical therapy when regional susceptibility data demonstrate a high prevalence for AMX resistance but susceptibility for AMC [
21]. If first-line antibiotics are not appropriate according to AST results, the second-line antibiotics NIT, FQs, or 3GC can be administered. However, these antimicrobial agents should be used with care regarding their importance in human health. In case of recurrent bacterial cystitis, AST should always be performed; initial antimicrobial therapy with first-line antibiotics or administration of NSAIDs is indicated while awaiting AST results. Antimicrobial treatment should be adjusted depending on AST results [
22].
According to the questionnaire, most animals in our study received prior treatment with AMC. In the year 2019, Weese et al. stated: “If the expected incidence of treatment failure to a given antimicrobial increases, an alternate antimicrobial should be considered” [
21] (p. 10). The Infectious Diseases Society of America and European Society for Microbiology and Infectious Diseases guidelines for humans for acute uncomplicated urinary tract infections do not recommend the use of AMP or AMX, given the high resistance (approx. 30%) determined in human isolates. Other antibiotics, such as SXT, should be withdrawn from use when resistance prevalence has increased above a threshold of 20%, i.e., in this case, the agent is no longer recommended for treatment [
74]. Considering that many
Enterobacterales are intrinsically resistant to AMX and that, except for enterococci and
Sc. canis, susceptibility was considerably lower to AMP than to AMC (76.1% vs. 93.4%,
Table S13), the use of AMX as a first-line antibiotic for UTI should be reconsidered. Instead, direct use of AMC should be taken in consideration.
SXT was used to treat UTI in only 4.4% of the study cases and only in dogs. While the use of SXT in veterinary medicine was widely described in the 1970s, 1980s, and 1990s, the use of this antimicrobial agent declined in the 2000s due to the increasingly observed side effects [
68,
75,
76]. Current guidelines recommend the use of SXT but also point out a shorter usage of antimicrobials in the treatment of UTI [
21]. Since most side effects occur only after a longer treatment period (average of 12 days), SXT is a good alternative to AMX as a first-line antibiotic for sporadic bacterial cystitis when administered for a short period of time [
76]. This is shown in the study by Clare et al. (2014) and is consistent with our findings regarding high susceptibility of
Enterobacterales, despite
Proteus spp., to this drug [
77]. However, if the animal suffers from recurrent bacterial cystitis, short-term sulphonamide treatment may not be sufficient, as high clinical remission rates were previously reported for such cases [
77].
In most of the current guidelines, first-generation cephalosporins are not recommended for first- or second-line treatment, but in Germany, CFX is approved for the treatment of cystitis for susceptible Enterobacteriaceae, streptococci, and staphylococci for dogs and cats. According to AST results, most Enterobacterales showed susceptibility of more than 90% to this drug. The susceptibility results for streptococci and staphylococci in dogs support the choice of CFX for canine bacterial UTI. However, it must be taken into consideration that in cats, enterococci were the most commonly detected Gram-positive bacteria and that these are intrinsically resistant to CFX. Therefore, when Gram-positive cocci are detected in the cat, the use of CFX should be discouraged.
Nitrofurantoin is recommend by current guidelines as a second-line antimicrobial in sporadic bacterial cystitis [
21]. However, due to its toxicity and poor pharmacokinetic properties, it should only be considered in cases of UTI caused by MDR bacteria [
78,
79,
80,
81]. The excellent efficacy of NIT is also supported by our data, as 94.5% of the MDR isolates identified in this study were susceptible to this drug. Only for
Klebsiella spp.,
ECC, and
Enterococcus faecium, treatment with NIT cannot be recommended due to high resistance rates in our study. It should also not be applied in infections caused by
Proteus spp. and
Pseudomonas spp., as these bacteria are intrinsically resistant to NIT [
82]. In contrast to earlier reports, the macrocrystalline formulation of NIT prescribed today rarely causes gastrointestinal side effects [
80,
83]. Clinical treatment with NIT also requires excellent compliance from the owner, as the drug must be administered every 8 h due to its low plasma concentration [
21,
78,
83]. It has to be used as an off-label drug under the Cascade principle, as there is no equivalent product licensed for veterinary usage in Germany.
Prudent use of antibiotics, particularly of drugs that are critically important for humans, such as FQs and 3GC, is one essential element in the global fight against AMR. Our data, although limited to a small study population, suggest that empiric UTI therapy was often performed with ENR, MAR, or CFV. This was particularly the case in cats, which was previously also noted by Weese et al. (2021) [
84,
85]. FQs and 3GC are classified by the European Medicines Agency (EMA) for “restrict use” in animals to mitigate public health risk, and the WHO classifies them as HPCIA [
12,
86]. They are also first-line agents for treatment of pyelonephritis and other infections with MDR bacteria in veterinary medicine [
21]. Prescription of these antimicrobials is very common in cats [
7,
9,
84,
87,
88,
89]. This could likely be explained with convenient application. Whereas AMX, AMC, or SXT must be given orally every 12 h, FQs require this only every 24 h, and a single injection with CFV is sufficient for up to 14 days [
21]. According to a previous study evaluating electronic medical records, the most common reason for prescribing CFV was the inability to treat cats orally [
10].
The problem of overprescribing is not limited to cats. Several studies observed that antimicrobial therapy is initiated far too often in animals that are presenting urinary symptoms [
5,
9,
90]. According to a Danish study, verification of the suspected UTI diagnosis was achieved in 80.1% of the cases by microscopy and in only 56% by microbiological culture [
91]. This is in agreement with the results of a Swiss study, which reported that in only 40% of all FLUDT cases was a diagnostic work up with microbiological culture initiated [
90]. This kind of diagnostic approach favours the selection of MDR bacteria and increases the risk of transmission of MDR bacteria between companion animals and humans [
14,
92,
93].







{kind=link}
{kind=link}
{kind=link}