
A Novel Machine Learning-Based Point-Score Model as a Non-Invasive Decision-Making Tool for Identifying Infected Ascites in Patients with Hydropic Decompensated Liver Cirrhosis: A Retrospective Multicentre Study

 , ,
, ,  , , , and add
Show full author list
, , , and add
Show full author list
Abstract
:1. Introduction
2. Results
2.1. Baseline Characteristics
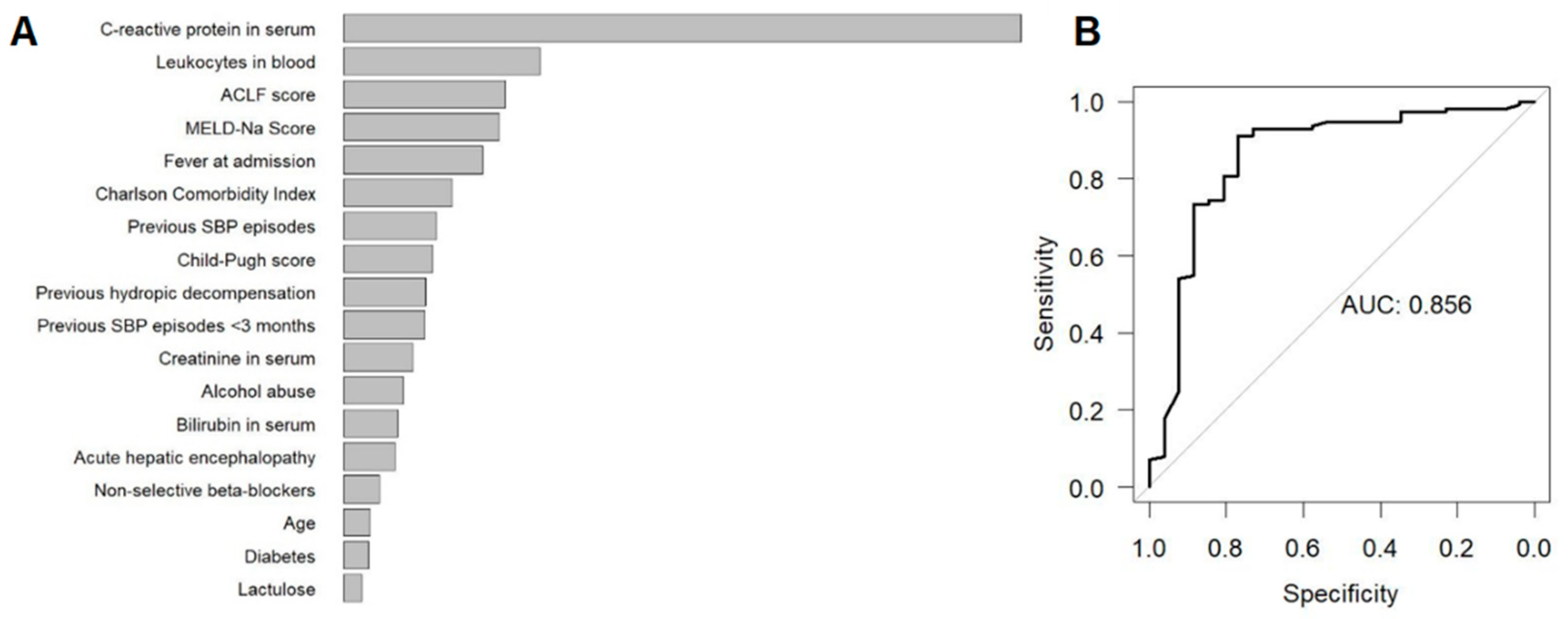
2.2. Random Forest Importance Measures
2.3. Scoring Model
3. Discussion
4. Materials and Methods
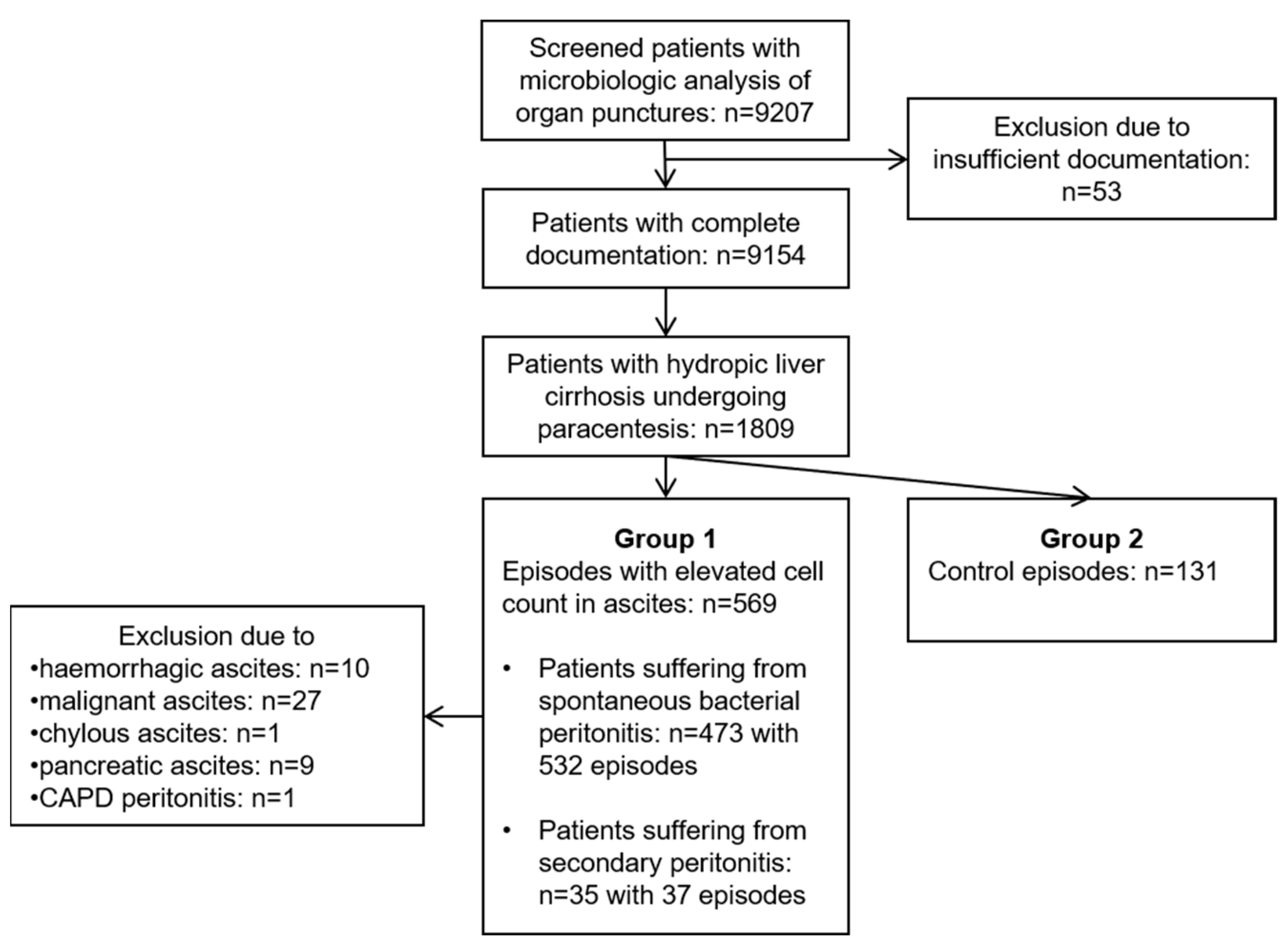
4.1. Study Population
4.2. Assessment of Predictors for SBP and SecP
4.3. Ethical Statement
4.4. Statistical Analysis
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tay, P.W.L.; Xiao, J.; Tan, D.J.H.; Ng, C.; Lye, Y.N.; Lim, W.H.; Teo, V.X.Y.; Heng, R.R.Y.; Yeow, M.W.X.; Lum, L.H.W.; et al. An Epidemiological Meta-Analysis on the Worldwide Prevalence, Resistance, and Outcomes of Spontaneous Bacterial Peritonitis in Cirrhosis. Front. Med. 2021, 8, 693652. [Google Scholar] [CrossRef] [PubMed]
- Soriano, G.; Castellote, J.; Álvarez, C.; Girbau, A.; Gordillo, J.; Baliellas, C.; Casas, M.; Pons, C.; Román, E.M.; Maisterra, S.; et al. Secondary bacterial peritonitis in cirrhosis: A retrospective study of clinical and analytical characteristics, diagnosis and management. J. Hepatol. 2010, 52, 39–44. [Google Scholar] [CrossRef]
- Wiest, R.; Schoelmerich, J. Secondary peritonitis in cirrhosis: “Oil in fire”. J. Hepatol. 2009, 52, 7–9. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.J.; Tsukamoto, M.M.; Mathur, A.K.; Ghomri, Y.M.; Hou, L.; Sheibani, S.; A Runyon, B. Delayed Paracentesis Is Associated with Increased In-Hospital Mortality in Patients with Spontaneous Bacterial Peritonitis. Am. J. Gastroenterol. 2014, 109, 1436–1442. [Google Scholar] [CrossRef] [PubMed]
- Angeli, P.; Bernardi, M.; Villanueva, C.; Francoz, C.; Mookerjee, R.P.; Trebicka, J.; Krag, A.; Laleman, W.; Gines, P. EASL Clinical Practice Guidelines for the management of patients with decompensated cirrhosis. J. Hepatol. 2018, 69, 406–460. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- European Association for the Study of the Liver. EASL clinical practice guidelines on the management of ascites, spontaneous bacterial peritonitis, and hepatorenal syndrome in cirrhosis. J. Hepatol. 2010, 53, 397–417. [Google Scholar] [CrossRef]
- Aithal, G.P.; Palaniyappan, N.; China, L.; Härmälä, S.; Macken, L.; Ryan, J.M.; Wilkes, E.A.; Moore, K.; Leithead, J.A.; Hayes, P.C.; et al. Guidelines on the management of ascites in cirrhosis. Gut 2021, 70, 9–29. [Google Scholar] [CrossRef] [PubMed]
- Pache, I.; Bilodeau, M. Severe haemorrhage following abdominal paracentesis for ascites in patients with liver disease. Aliment. Pharmacol. Ther. 2005, 21, 525–529. [Google Scholar] [CrossRef]
- Kurup, A.N.; Lekah, A.; Reardon, S.T.; Schmit, G.D.; McDonald, J.S.; Carter, R.E.; Kamath, P.S.; Callstrom, M.R.; Atwell, T.D. Bleeding Rate for Ultrasound-Guided Paracentesis in Thrombocytopenic Patients. J. Ultrasound Med. 2015, 34, 1833–1838. [Google Scholar] [CrossRef]
- Lin, S.; Wang, M.; Zhu, Y.; Dong, J.; Weng, Z.; Shao, L.; Chen, J.; Jiang, J. Hemorrhagic Complications Following Abdominal Paracentesis in Acute on Chronic Liver Failure. Medicine 2015, 94, e2225. [Google Scholar] [CrossRef]
- Würstle, S.; Hapfelmeier, A.; Karapetyan, S.; Studen, F.; Isaakidou, A.; Schneider, T.; Schmid, R.M.; von Delius, S.; Gundling, F.; Triebelhorn, J.; et al. Web Application. A Novel Machine Learning-Based Point-Score Model as a Non-Invasive Decision-Making Tool for Identifying Infected Ascites in Patients with Hydropic Decompensated Liver Cirrhosis: A Retrospective Multicentre Study. 2022. Available online: https://bookerar.shinyapps.io/Infected_ascites/ (accessed on 20 June 2022).
- Alaniz, C.; Regal, R.E. Spontaneous bacterial peritonitis: A review of treatment options. P T. 2009, 34, 204–210. [Google Scholar] [PubMed]
- Abdel-Razik, A.; Mousa, N.; Abdel-Aziz, M.; Elsherbiny, W.; Zakaria, S.; Shabana, W.; Abed, S.; Elhelaly, R.; Elzehery, R.; Eldars, W.; et al. Mansoura simple scoring system for prediction of spontaneous bacterial peritonitis: Lesson learnt. Eur. J. Gastroenterol. Hepatol. 2019, 31, 1017–1024. [Google Scholar] [CrossRef] [PubMed]
- Wehmeyer, M.H.; Krohm, S.; Kastein, F.; Lohse, A.W.; Lüth, S. Prediction of spontaneous bacterial peritonitis in cirrhotic ascites by a simple scoring system. Scand. J. Gastroenterol. 2014, 49, 595–603. [Google Scholar] [CrossRef]
- Metwally, K.; Fouad, T.; Assem, M.; Abdelsameea, E.; Yousery, M. Predictors of Spontaneous Bacterial Peritonitis in Patients with Cirrhotic Ascites. J. Clin. Transl. Hepatol. 2018, 6, 372–376. [Google Scholar] [CrossRef] [Green Version]
- Shi, K.-Q.; Fan, Y.-C.; Ying, L.; Lin, X.-F.; Song, M.; Li, L.-F.; Yu, X.-Y.; Chen, Y.-P.; Zheng, M.-H. Risk stratification of spontaneous bacterial peritonitis in cirrhosis with ascites based on classification and regression tree analysis. Mol. Biol. Rep. 2011, 39, 6161–6169. [Google Scholar] [CrossRef] [PubMed]
- Min, Y.W.; Lim, K.S.; Min, B.-H.; Gwak, G.-Y.; Paik, Y.H.; Choi, M.S.; Lee, J.H.; Kim, J.J.; Koh, K.C.; Paik, S.W.; et al. Proton pump inhibitor use significantly increases the risk of spontaneous bacterial peritonitis in 1965 patients with cirrhosis and ascites: A propensity score matched cohort study. Aliment. Pharmacol. Ther. 2014, 40, 695–704. [Google Scholar] [CrossRef]
- Dam, G.; Vilstrup, H.; Watson, H.; Jepsen, P. Proton pump inhibitors as a risk factor for hepatic encephalopathy and spontaneous bacterial peritonitis in patients with cirrhosis with ascites. Hepatology 2016, 64, 1265–1272. [Google Scholar] [CrossRef] [Green Version]
- Elzouki, A.-N.; Neffati, N.; Rasoul, F.A.; Abdallah, A.; Othman, M.; Waness, A. Increased Risk of Spontaneous Bacterial Peritonitis in Cirrhotic Patients Using Proton Pump Inhibitors. GE-Port. J. Gastroenterol. 2018, 26, 83–89. [Google Scholar] [CrossRef]
- Ratelle, M.; Perreault, S.; Villeneuve, J.-P.; Tremblay, L. Association Between Proton Pump Inhibitor Use and Spontaneous Bacterial Peritonitis in Cirrhotic Patients with Ascites. Can. J. Gastroenterol. Hepatol. 2014, 28, 330–334. [Google Scholar] [CrossRef] [Green Version]
- Lohse, A.W.; Kluwe, J.; Wehmeyer, M.H.; Horvatits, T. Stop of Proton-Pump Inhibitor Treatment in Patients with Liver Cirrhosis—A Double-blind, Placebo-controlled Trial (STOPPIT). ClinicalTrials.gov Identifier, NCT04448028. ClinicalTrials.gov 2020. Available online: https://www.clinicaltrials.gov/ct2/show/NCT04448028 (accessed on 20 June 2022).
- Leithead, J.A.; Rajoriya, N.; Tehami, N.; Hodson, J.; Gunson, B.K.; Tripathi, D.; Ferguson, J.W. Non-selective β-blockers are associated with improved survival in patients with ascites listed for liver transplantation. Gut 2015, 64, 1111–1119. [Google Scholar] [CrossRef] [PubMed]
- Thalheimer, U.; Triantos, C.K.; Samonakis, D.N.; Patch, D.; Burroughs, A.K. Infection, coagulation, and variceal bleeding in cirrhosis. Gut 2005, 54, 556–5563. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Paramo, M.; Muñoz, J.; Albillos, A.; Freile, I.; Portero, F.; Santos, M.; Ortiz-Berrocal, J. Effect of propranolol on the factors promoting bacterial translocation in cirrhotic rats with ascites. Hepatology 2000, 31, 43–48. [Google Scholar] [CrossRef] [PubMed]
- Senzolo, M.; Cholongitas, E.; Burra, P.; Leandro, G.; Thalheimer, U.; Patch, D.; Burroughs, A.K. Beta-Blockers protect against spontaneous bacterial peritonitis in cirrhotic patients: A meta-analysis. Liver Int. 2009, 29, 1189–1193. [Google Scholar] [CrossRef]
- Mandorfer, M.; Bota, S.; Schwabl, P.; Bucsics, T.; Pfisterer, N.; Kruzik, M.; Hagmann, M.; Blacky, A.; Ferlitsch, A.; Sieghart, W.; et al. Nonselective β Blockers Increase Risk for Hepatorenal Syndrome and Death in Patients with Cirrhosis and Spontaneous Bacterial Peritonitis. Gastroenterology 2014, 146, 1680–1690.e1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moreau, R.; Jalan, R.; Gines, P.; Pavesi, M.; Angeli, P.; Cordoba, J.; Durand, F.; Gustot, T.; Saliba, F.; Domenicali, M.; et al. Acute-on-Chronic Liver Failure Is a Distinct Syndrome That Develops in Patients with Acute Decompensation of Cirrhosis. Gastroenterology 2013, 144, 1426–1437.e9. [Google Scholar] [CrossRef]
- CLIF-C-ACFL Calculator. European Foundation for the Study of Chronic Liver Failure 2022. Available online: https://www.efclif.com/scientific-activity/score-calculators/clif-c-aclf (accessed on 10 May 2022).
- Hapfelmeier, A.; Hornung, R.; Haller, B. Sequential Permutation Testing of Random Forest Variable Importance Measures. arXiv 2022, arXiv:2206.01284. [Google Scholar]
- Hothorn, T.; Lausen, B. On the exact distribution of maximally selected rank statistics. Comput. Stat. Data Anal. 2003, 43, 121–137. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Measurement | Score Points | Simplified Model |
|---|---|---|
| CRP > 4.2 mg/dL | +87 | +26 |
| Previous hydropic decompensation | +60 | +17 |
| White blood cell counts > 11.49 G/L | +52 | +16 |
| Organ failure * | +45 | +14 |
| Fever | +39 | +13 |
| Acute gastrointestinal bleeding | +31 | +8 |
| PPI medication | +26 | +8 |
| Previous SBP | +8 | +5 |
| Charlson Comorbidity Index > 6 | +6 | - |
| No propranolol or carvedilol medication | +1 | +2 |
| MELD-Na score > 24.9 | +1 | - |
| Child-Pugh class C | - | +1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Würstle, S.; Hapfelmeier, A.; Karapetyan, S.; Studen, F.; Isaakidou, A.; Schneider, T.; Schmid, R.M.; von Delius, S.; Gundling, F.; Triebelhorn, J.; et al. A Novel Machine Learning-Based Point-Score Model as a Non-Invasive Decision-Making Tool for Identifying Infected Ascites in Patients with Hydropic Decompensated Liver Cirrhosis: A Retrospective Multicentre Study. Antibiotics 2022, 11, 1610. https://doi.org/10.3390/antibiotics11111610
Würstle S, Hapfelmeier A, Karapetyan S, Studen F, Isaakidou A, Schneider T, Schmid RM, von Delius S, Gundling F, Triebelhorn J, et al. A Novel Machine Learning-Based Point-Score Model as a Non-Invasive Decision-Making Tool for Identifying Infected Ascites in Patients with Hydropic Decompensated Liver Cirrhosis: A Retrospective Multicentre Study. Antibiotics. 2022; 11(11):1610. https://doi.org/10.3390/antibiotics11111610
Chicago/Turabian StyleWürstle, Silvia, Alexander Hapfelmeier, Siranush Karapetyan, Fabian Studen, Andriana Isaakidou, Tillman Schneider, Roland M. Schmid, Stefan von Delius, Felix Gundling, Julian Triebelhorn, and et al. 2022. "A Novel Machine Learning-Based Point-Score Model as a Non-Invasive Decision-Making Tool for Identifying Infected Ascites in Patients with Hydropic Decompensated Liver Cirrhosis: A Retrospective Multicentre Study" Antibiotics 11, no. 11: 1610. https://doi.org/10.3390/antibiotics11111610