1. Introduction
Periprosthetic joint infection (PJI) following total joint arthroplasty (TJA) is a serious complication that almost always requires revision surgery [
1]. In chronic PJI, exchange arthroplasty is the method of choice. The exchange arthroplasty can be performed as a one- or two-stage procedure. Two-stage exchange arthroplasty involves at minimum two separate operations, with the first involving removal of all implants, thorough irrigation and debridement, and implantation of a temporary ‘spacer’ implant. The patient is then placed on intravenous antibiotics, and followed clinically for evidence of infection resolution, at which time the second stage is planned for implantation of a definitive implant.
Similar to the two-stage procedure, the therapeutic target of the one-stage technique is the eradication of the infection, but with only one surgical intervention in carefully selected patients. According to current literature, medium- to long-term success, following the one-stage revision ranges from 75% to 98% [
2,
3,
4,
5,
6,
7,
8,
9]. A recently published systematic review by Pangaud et al. showed that the one-stage method is a viable alternative to the two-stage revision with similar eradication rates [
10], while the one-stage procedure was associated with lower cost and morbidity compared to the two-stage method [
10].
Despite several studies focusing on clinical outcomes, there are no comparative studies that report on the patient-reported outcome measure (PROMs) and quality-adjusted life years (QALYs) in septic revision knee procedures. Focusing on hip procedures, Tirumala et al. (2021) were able to show significantly better results for PROMs in patients with a one-stage septic hip revision compared to the two-stage revision [
11].
The aim of this current study was to find out if PROMs differ between the one-stage and two-stage revision for septic TKAs. We hypothesized that the one-stage septic knee exchange might be associated with a higher PROMs and QALYs compared to the two-stage septic knee exchange.
2. Material and Methods
At our institution, we mainly perform one-stage septic exchange arthroplasty in the management of PJI. Therefore, all patients who were surgically treated with the two-stage septic knee revision in the period from 1 January 2017 to 31 December 2018 were initially selected (47 patients). The exclusion criteria were: patients treated surgically at another hospital, patients without complete documentation, patients without preoperative aspiration to determine the microorganism, and patients with a follow-up period of less than 3 years. At our institution, a PJI is diagnosed using the 2018 PJI criteria by Parvizi et al. [
12].
A total of 36 patients met the inclusion and exclusion criteria. During the same period, 47 patients who underwent a one-stage septic knee revision were randomly selected. The same inclusion and exclusion criteria were set. Patients were matched for age and pre-existing conditions.
The following data were collected for all patients: age, gender, weight (in kg), height (in cm), body mass index (BMI), hypertension, diabetes mellitus, admission diagnosis, Charlson Comorbidity Index (CCI), hospital stay, number of germs, type of germs (high virulent, low virulent), postoperative complications/re-revisions during the inpatient stay and at the time of the latest follow up, and postoperative mortality during the inpatient stay and at the time of the latest follow up.
In addition, a correlation analysis between one-stage and two-stage revision was performed. The correlation between the two procedures was examined for the following variables: gender, number of germs, high virulent vs. low virulent germs, gram positive vs. gram negative germs, postoperative deep vein thrombosis (DVT), postoperative pulmonary embolism, and admission to the intensive care unit (ICU).
The patients’ function and health-related quality of life for both procedures was determined by PROMs. For this purpose, the following standardized and well-studied questionnaires were sent to all patients by post: Oxford Knee Score (OKS), European Quality of Life 5 Dimensions 5 Level Version (EQ-5D-5L), Surgical Satisfaction Questionnaire-8 (SSQ-8), and Short From 36 (SF-36). To determine the quality-adjusted life years (QALY), the EQ-5D-5L index was used. The QALYs are calculated as followed: QALYs = Follow-up (in years) × EQ-5D-5L Index.
A total of 35 patients responded (response rate of 53%). Patients who did not respond to the letter were contacted by telephone. At the time of the last survey, a total of 7 patients had died (4 patients in the one-stage group and 3 patients in the two-stage group). No information on the causes of death were provided by the relatives. The remaining patients could not be reached due to a change of telephone number and/or address. Therefore, the final cohort included 35 patients (n = 19 one-stage, n = 16 two-stage) with a minimum follow-up of three years.
This study was performed after obtaining approval from the local ethics committee.
2.1. Surgical Technique
2.1.1. One-Stage Exchange Arthroplasty Technique
The one-stage exchange technique to treat PJI was first described by Buchholz in 1970s, after mixing antibiotics with bone cement to enhance the local antibiotics concentrations [
13]. The success of this technique depends on the complete removal of all implanted hardware, cement removal, and radical debridement with excision of infected and necrotic soft and bone tissue. Re-draping the patient and re-scrubbing the surgical team must be performed with the use of new instruments for re-implantation. The indication for one-stage septic exchange technique depends on the preoperative diagnostic joint aspiration after recognition of the causative microorganism and obtaining the antibiotic sensitivity results. Routinely, postoperative 2 week-intravenous antibiotic therapy is administered [
14].
2.1.2. Two-Stage Exchange Arthroplasty Technique
The two-stage exchange technique is considered the gold standard worldwide for treating chronic PJI. It was first described in 1983 by Insall et al. [
15]. A preoperative diagnostic joint aspiration is performed for culture and sensitivity as well. This technique is divided into two stages; in the first stage, removal of all implanted hardware with debridement and excision of infected and necrotic tissue is performed followed by implanting an antibiotic loaded spacer. After a spacer retention interval which lasts 6 to 8 weeks with antibiotic treatment of 6–8 weeks, a second stage is performed with spacer removal, debridement, obtaining biopsies for culture and sensitivity, and re-implantation is performed after proper wound healing and low serum C-reactive protein (CRP) and erythrocyte sedimentation rate (ESR) thresholds. The antibiotic therapy is continued after the 2nd stage for another 4–6 weeks. In most cases, a minimum of a 12-week period of systemic antibiotic therapy is recommended [
16,
17,
18,
19].
2.2. Statistical Analysis
Statistical analysis and charting were performed using the GraphPad Prism software package (Prism 6 for Mac OS X, version 5.0d; La Jolla, CA, USA) and Microsoft Excel for Mac 2011 (version 14.7.7). The distribution of categorical data was described using absolute and relative frequencies. To compare the location of the distribution of a metric variable of two independent groups, the Shapiro–Wilk test was first used to check whether the data of both groups were normally distributed. If the normal distribution assumption was not rejected (p-value ≥ 0.1), the comparison was carried out with the t-test. In the case of rejection of the normal distribution assumption, the Mann–Whitney-U test was applied. To compare the frequency distributions of a categorical variable of independent groups, the Chi-square test or Fisher’s exact test (if there were expected cell frequencies smaller than five) was used.
3. Results
After an average follow-up of 54.5 months (SD = 5.5), a total of 35 patients with an average age of 67.7 years (SD = 8.9) were included in the study. The male gender predominated with 60%. The mean body mass index (BMI) of the total cohort was 28.8 kg/m
2 (SD = 5.5). The BMI was significantly higher in the one-stage revision group with an average BMI of 30.7 kg/m
2 (SD = 6.0) than in the two-stage revision group with an average BMI of 26.2 kg/m
2 (SD = 4.0) (
p = 0.040). Both groups were preoperatively matched for age and previous diseases. Therefore, no significant differences were found for age (
p = 0.781) and pre-existing conditions, measured by the Charlson Comorbidity Index (CCI) (
p = 0.445) (
Table 1).
The mean inpatient stay was 20 days (15–17 days, SD 3.5) in the one-stage revision group. The inpatient stays after the two-stage revision group were on average 21 days (16–31 days; SD = 4.1) (
p = 0.540) after the 1st stay and 18.7 days (14–28 days, SD = 3.6) (
p = 0.083) after the 2nd stay. When comparing total length of stay including both stages versus one-stage, there was a significant difference, with two-stage revision resulting in a longer length of stay (
p < 0.05). There were no significant differences for the isolated number of germs in both groups (
Table 2).
A total of four complications occurred in both groups. In the one-stage revision group, there were 2 cases of deep vein thrombosis and 2 cases of pulmonary embolism. No further surgery was required in the one-stage revision group. In the two-stage revision group, the following complications occurred: acute kidney failure, deep vein thrombosis, pulmonary embolism, and reoperation due to reinfection. There were no significant differences in mortality between the two groups.
For every patient, the identified germs are shown in
Table 3.
Staphylococcus epidermidis was isolated in both groups most often (one-stage group: 5 times; two-stage group: 2 times). Furthermore, various
Staphylococcus and
Streptococcus species were isolated.
The mean Oxford Knee Score in the one-stage revision group was 27 (6–45; SD = 10.7) and in the two-stage revision group was 27.7 (18–42; SD = 7.2) (
p = 0.928). With regard to pain in the area of the operated knee joint, only 2 patients (5.7%) in the dataset had no pain, with 16 patients (45.7%) having moderate to severe pain. Nine patients of these patients were (47.4%) from the one-stage revision group (
Table 4).
The mean EQ-5D-5L Index in the one-stage revision group was 0.634 (range: 0.5–1; SD = 0.342) and in the two-stage revision group was 0.671 (range: 0.42–0.91; SD = 0.161) (
p = 0.647) (
Table 3). There was also no significant difference in the mean SSQ-8 Score (
p = 0.904) (
Table 3). In the evaluation of the SF-36 questionnaires, no significant differences were found between the one- and the two-stage revision group (
Table 5).
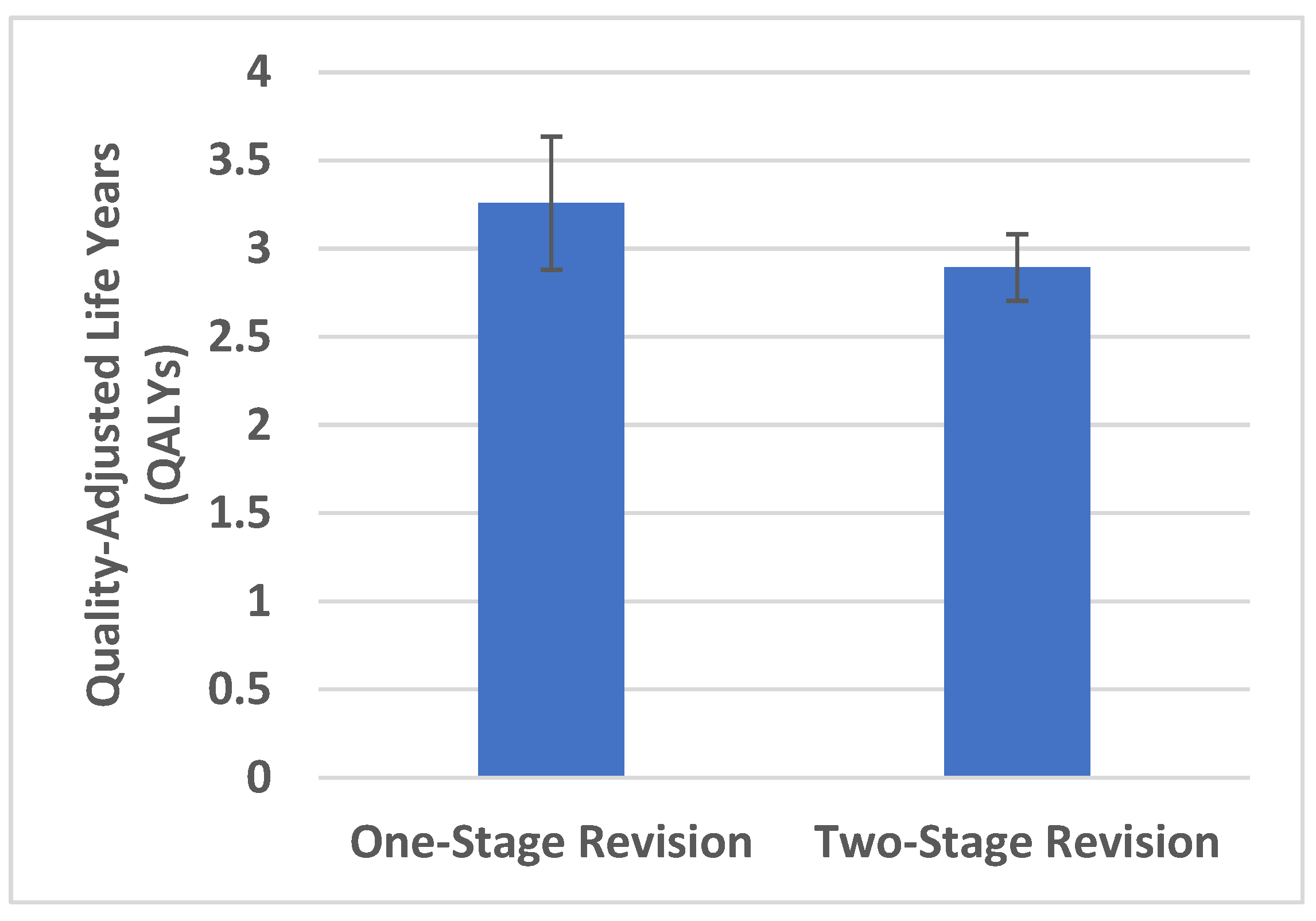
The mean QALYs were higher for the one-stage revision at 3.26 (SD = 1.41) than for the two-stage revision at 2.89 (SDA = 0.71) (
Figure 1). The average difference in QALYs between the one- and two-stage revision group was 0.37 with no statistically significant difference (
p = 0.395).
4. Discussion
Periprosthetic joint infection is a serious complication that can be associated with a reduction in quality of life and significant costs. There are various studies in the literature that present the outcomes after one- and two-stage revisions, as presented in the systematic review from Panguad et al., 2019 [
10]. However, the main focus of many studies is on clinical outcomes, particularly the eradication rates and revision rates of both procedures. There are few studies comparing the two surgical procedures. The eradication of infection is crucial when treating PJIs, not only for the surgeon but also for the patient. Another important factor is to achieve the best possible quality of life as well as functionality following the surgery. In this context, no robust data are available in the literature examining clinical outcomes and patient’s function or quality of life measured by PROMs.
In terms of clinical outcomes, our study could not identify any significant differences in complication rates between the one- and two- stage revision. Thiesen et al. (2021) showed that patients with a two-stage revision had significantly higher risks for medical complications [
20]. The authors found that acute renal failure was significantly more frequent with a two-stage revision, especially in multimorbid patients with a high CCI index [
20]. In our cohort, acute renal failure occurred in only one patient (6.3%) after a two-stage revision. Regarding mortality during the inpatient stay, Thiesen et al. (2021) found no significant differences between the one- and two-stage revision, analogous to our data. A study from the Norwegian registry showed a significantly higher mortality for the two-stage revision [
21].
In our study, only one patient required reoperation due to reinfection after a two-stage revision. This corresponds to a periprosthetic knee joint infection cure rate of 93.8%, which is comparable to the current literature [
10]. In the single-stage revision group, no reoperation was required. Due to the lack of a 100% response rate, these results need a careful interpretation. Zahar et al. (2016) showed a 93% eradication success rate after ten years with the one-stage revision [
9].
The primary goal of this study was to prove that the one-stage revision may lead to a better quality of life for patients. However, this hypothesis could not be confirmed. Tirumala et al. (2021) were able to demonstrate better results for the one-stage revision in periprosthetic hip joint infections [
11]. In this study, the one-stage revision was significantly better for all dimensions, such as physical function and mental health [
11]. In our study, the SF-36 questionnaire was used to examine several dimensions, including physical and mental health. However, no significant differences between one- and two-stage revision for a periprosthetic knee joint infection could be found.
Walter et al. (2021) showed that patients with a PJI have a significantly lower quality of life compared to normative data, even years after successful surgical treatment [
22]. Our study showed that a relatively large number of patients had severe to very severe pain in the operated joint at the time of the last follow-up examination. The quality of life measured by PROMs was not ideal in various cases. Nonetheless, many patients would have undergone the same operation again. Of the total study population, 19 patients (54.3%) would have undergone the surgery again, with a preponderance in the one-stage group (one-stage group: 70.6%; two-stage group: 46.7%). The reason for this could be that patients were generally satisfied with the eradication of the infection despite functional limitations and sometimes severe pain. This means that patients may be grateful that they “survived” the serious, sometimes life-threatening, diagnosis of a periprosthetic joint infection without more serious limitations.
The question that now arises is whether the current PROMs are ideally suited for the evaluation of patients with a periprosthetic joint infection. It may be that special questionnaires with a special focus on periprosthetic join infections need to be established for the evaluation of PROMs. A currently ongoing prospective, randomized multicenter study is planned to compare one-stage and two-stage septic knee revisions [
23]. This study is currently ongoing in 7 centers in Denmark. Clinical follow-up of patients will be done using PROM questionnaires, which will be evaluated at planned intervals of 6 weeks to 10 years. In addition to the Oxford Knee Score, the evaluation of EQ-5D questionnaires is planned. Based on these data and further prospective studies, it may be possible to see which of the two procedures lead to a better quality of life for patients.
Our study provides new results. Nevertheless, these data have to be assessed with limitations. On the one hand, the choice of a retrospective/prospective study design proved to be a disadvantage, as no PROMs data were available preoperatively. PROMs data were only obtained at the time of the last follow-up. Therefore, a prospective study with both pre- and postoperative check-ups (preoperative; 3, 6, 12 months postoperatively) would deliver more valid data. Another disadvantage is the low response rate. For many patients, an analysis was not possible because the patients could not be included in the final evaluation for various reasons. Moreover, the type of primary prostheses was not investigated as this did not influence the indication of one- or two-stage septic exchange technique.
5. Conclusions
The one-stage revision had a significantly higher proportion of patients who would have undergone the surgery again. The QALYs tended to be better in the one-stage group. However, there was no statistically significant difference in the QALYs between the one- and two-stage group.
Due to a lack of data, further studies, especially prospective randomized trials, need to be done. These studies will hopefully show whether the one-stage revision for treating a periprosthetic joint infection will become the gold standard.
Author Contributions
Conceptualization: M.C., M.B. and S.A.; Methodology: M.C., M.B. and S.A.; Validation: M.C., M.B. and S.A.; Formal analysis: M.C., M.B. and S.E.; Investigation: M.C., M.B. and G.T.; Data curation: M.C., M.B., S.A. and G.T.; Writing—original draft: M.C., M.B. and S.A., Writing—review and editing: M.C., M.B., S.A., G.T., R.S., S.E. and T.G.; Visualization: M.C., M.B., S.A., G.T. and S.E.; Supervision: M.C.; Project administration: M.C., M.B. and S.A. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Approval for this study was given by the ethics committee “Ethik-Kommission der Ärztekammer Hamburg (2020-10348-BO-ff)”.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Data and materials are available, consent to participate was given, consent to publish was given.
Conflicts of Interest
The authors declare that they have no conflict of interest regarding this manuscript. Independent from the submitted manuscript, received royalties/payments of all authors are listed: payments for presentations from Waldemar Link, Hamburg, Germany, Zimmer Biomet Inc., Warsaw, USA, Heraeus, Ceramtec Co.
References
- Tande, A.J.; Patel, R. Prosthetic joint infection. Clin. Microbiol. Rev. 2014, 27, 302–345. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buechel, F.F.; Femino, F.P.; D’Alessio, J. Primary exchange revision arthroplasty for infected total knee replacement: A long-term study. Am. J. Orthop. 2004, 33, 190–198. [Google Scholar] [PubMed]
- Haddad, F.S.; Sukeik, M.; Alazzawi, S. Is single-stage revision according to a strict protocol effective in treatment of chronic knee arthroplasty infections? Clin. Orthop. Relat. Res. 2015, 473, 8–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jenny, J.Y.; Barbe, B.; Gaudias, J.; Boeri, C.; Argenson, J.N. High infection control rate and function after routine one-stage exchange for chronically infected TKA. Clin. Orthop. Relat. Res. 2013, 471, 238–243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Macheras, G.A.; Kateros, K.; Galanakos, S.P.; Koutsostathis, S.D.; Kontou, E.; Papadakis, S.A. The long-term results of a two-stage protocol for revision of an infected total knee replacement. J. Bone Jt. Surg. Br. Vol. 2011, 93, 1487–1492. [Google Scholar] [CrossRef] [Green Version]
- Selmon, G.P.; Slater, R.N.; Shepperd, J.A.; Wright, E.P. Successful 1-stage exchange total knee arthroplasty for fungal infection. J. Arthroplast. 1998, 13, 114–115. [Google Scholar] [CrossRef]
- Singer, J.; Merz, A.; Frommelt, L.; Fink, B. High rate of infection control with one-stage revision of septic knee prostheses excluding MRSA and MRSE. Clin. Orthop. Relat. Res. 2012, 470, 1461–1471. [Google Scholar] [CrossRef] [Green Version]
- Tibrewal, S.; Malagelada, F.; Jeyaseelan, L.; Posch, F.; Scott, G. Single-stage revision for the infected total knee replacement: Results from a single centre. Bone Jt. J. 2014, 96, 759–764. [Google Scholar] [CrossRef]
- Zahar, A.; Kendoff, D.O.; Klatte, T.O.; Gehrke, T.A. Can Good Infection Control Be Obtained in One-stage Exchange of the Infected TKA to a Rotating Hinge Design? 10-year Results. Clin. Orthop. Relat. Res. 2016, 474, 81–87. [Google Scholar] [CrossRef] [Green Version]
- Pangaud, C.; Ollivier, M.; Argenson, J. Outcome of single-stage versus two-stage exchange for revision knee arthroplasty for chronic periprosthetic infection. EFORT Open Rev. 2019, 4, 495–502. [Google Scholar] [CrossRef]
- Tirumala, V.; Klemt, C.; van den Kieboom, J.; Xiong, L.; Kwon, Y. Comparison of patient reported outcome measures after single versus two-stage revision for chronic infection of total hip arthroplasty: A retrospective propensity score matched cohort study. Arch. Orthop. Trauma Surg. 2021, 141, 1789–1796. [Google Scholar] [CrossRef] [PubMed]
- Parvizi, J.; Tan, T.L.; Goswami, K.; Higuera, C.; Della Valle, C.; Chen, A.F.; Shohat, N. The 2018 Definition of Periprosthetic Hip and Knee Infection: An Evidence-Based and Validated Criteria. J. Arthroplast. 2018, 33, 1309–1314.e1302. [Google Scholar] [CrossRef] [PubMed]
- Buchholz, H.W.; Elson, R.A.; Heinert, K. Antibiotic-loaded acrylic cement: Current concepts. Clin. Orthop. Relat. Res. 1984, 96–108. [Google Scholar] [CrossRef]
- Zahar, A.; Webb, J.; Gehrke, T.; Kendoff, D. One-stage exchange for prosthetic joint infection of the hip. Hip. Int. 2015, 25, 301–307. [Google Scholar] [CrossRef]
- Insall, J.N.; Thompson, F.M.; Brause, B.D. Two-stage reimplantation for the salvage of infected total knee arthroplasty. J. Bone Jt. Surg. Am. Vol. 1983, 65, 1087–1098. [Google Scholar] [CrossRef] [Green Version]
- Vielgut, I.; Sadoghi, P.; Wolf, M.; Holzer, L.; Leithner, A.; Schwantzer, G.; Poolman, R.; Frankl, B.; Glehr, M. Two-stage revision of prosthetic hip joint infections using antibiotic-loaded cement spacers: When is the best time to perform the second stage? Int. Orthop. 2015, 39, 1731–1736. [Google Scholar] [CrossRef]
- Izakovicova, P.; Borens, O.; Trampuz, A. Periprosthetic joint infection: Current concepts and outlook. EFORT Open Rev. 2019, 4, 482–494. [Google Scholar] [CrossRef]
- Franceschini, M.; Pedretti, L.; Cerbone, V.; Sandiford, N.A. Two stage revision: Indications, techniques and results. Ann. Jt. 2022, 7, 4. [Google Scholar] [CrossRef]
- Charette, R.S.; Melnic, C.M. Two-Stage Revision Arthroplasty for the Treatment of Prosthetic Joint Infection. Curr. Rev. Musculoskelet. Med. 2018, 11, 332–340. [Google Scholar] [CrossRef]
- Thiesen, D.; Sobhani, H.; Gehrke, T.; Suero, E.; Klatte, T.; Citak, M. A comparison of short term complication rate between 44 two- and 385 one-stage septic exchange arthroplasties in chronic periprosthetic joint infections. Orthop. Traumatol. Surg. Res. 2021, 107, 102668. [Google Scholar] [CrossRef]
- Leta, T.; Lygre, S.; Schrama, J.; Hallan, G.; Gjertsen, J.; Dale, H.; Furnes, O. Outcome of Revision Surgery for Infection After Total Knee Arthroplasty: Results of 3 Surgical Strategies. JBJS Rev. 2019, 7, e4. [Google Scholar] [CrossRef] [PubMed]
- Walter, N.; Rupp, M.; Hierl, K.; Koch, M.; Kerschbaum, M.; Worlicek, M.; Alt, V. Long-Term Patient-Related Quality of Life after Knee Periprosthetic Joint Infection. J. Clin. Med. 2021, 10, 907. [Google Scholar] [CrossRef] [PubMed]
- Lindberg-Larsen, M.; Odgaard, A.; Fredborg, C.; Morville, H.; Schrøder, H. One-stage versus two-stage revision of the infected knee arthroplasty—A randomized multicenter clinical trial study protocol. BMC Musculoskelet. Disord. 2021, 22, 175. [Google Scholar] [CrossRef] [PubMed]
| Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).




{kind=link}