
National Early Warning Score (NEWS) Outperforms Quick Sepsis-Related Organ Failure (qSOFA) Score for Early Detection of Sepsis in the Emergency Department
 , , , and
, , , and
Abstract
:1. Introduction
2. Results
3. Discussion
4. Material and Methods
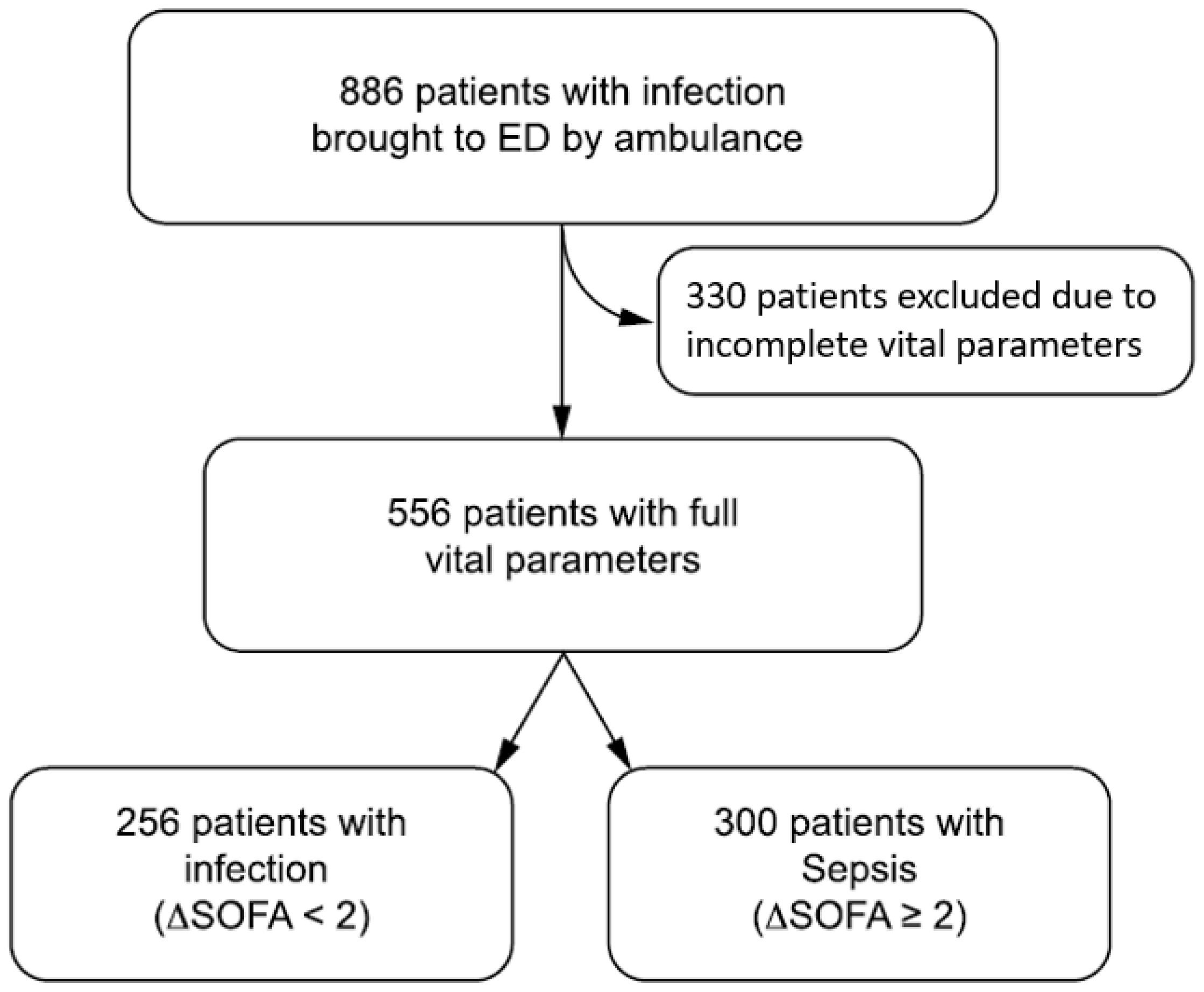
4.1. Study Design, Setting, and Participants
4.2. Score Computation
4.3. Statistical Analyses
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.-D.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef] [PubMed]
- Evans, L.; Rhodes, A.; Alhazzani, W.; Antonelli, M.; Coopersmith, C.M.; French, C.; Machado, F.R.; Mcintyre, L.; Ostermann, M.; Prescott, H.C.; et al. Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock 2021. Crit. Care Med. 2021, 49, e1063–e1143. [Google Scholar] [CrossRef] [PubMed]
- Singer, M.; Shankar-Hari, M. qSOFA, Cue Confusion. Ann. Intern. Med. 2018, 168, 293. [Google Scholar] [CrossRef] [PubMed]
- Seymour, C.W.; Liu, V.X.; Kahn, J.M.; Shankar-Hari, M.; Singer, M.; Deutschman, C.S.; Escobar, G.J.; Angus, D.C.; Iwashyna, T.J.; Brunkhorst, F.M.; et al. Assessment of Clinical Criteria for Sepsis: For the Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 762–774. [Google Scholar] [CrossRef] [Green Version]
- Usman, O.A.; Usman, A.A.; Ward, M.A. Comparison of SIRS, qSOFA, and NEWS for the early identification of sepsis in the Emergency Department. Am. J. Emerg. Med. 2019, 37, 1490–1497. [Google Scholar] [CrossRef]
- Tusgul, S.; Carron, P.-N.; Yersin, B.; Calandra, T.; Dami, F. Low sensitivity of qSOFA, SIRS criteria and sepsis definition to identify infected patients at risk of complication in the prehospital setting and at the emergency department triage. Scand. J. Trauma Resusc. Emerg. Med. 2017, 25, 108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mellhammar, L.; Linder, A.; Tverring, J.; Christensson, B.; Boyd, J.H.; Sendi, P.; Åkesson, P.; Kahn, F. NEWS2 Is Superior to qSOFA in Detecting Sepsis with Organ Dysfunction in the Emergency Department. J. Clin. Med. 2019, 8, 1128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Churpek, M.M.; Snyder, A.; Han, X.; Sokol, S.; Pettit, N.; Howell, M.D.; Edelson, D.P. Quick Sepsis-related Organ Failure Assessment, Systemic Inflammatory Response Syndrome, and Early Warning Scores for Detecting Clinical Deterioration in Infected Patients outside the Intensive Care Unit. Am. J. Respir. Crit. Care Med. 2017, 195, 906–911. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pullyblank, A.; Tavaré, A.; Little, H.; Redfern, E.; Le Roux, H.; Inada-Kim, M.; Cheema, K.; Cook, A. Implementation of the National Early Warning Score in patients with suspicion of sepsis: Evaluation of a system-wide quality improvement project. Br. J. Gen. Pract. 2020, 70, e381–e388. [Google Scholar] [CrossRef] [PubMed]
- Vincent, J.-L.; De Mendonca, A.; Cantraine, F.; Moreno, R.; Takala, J.; Suter, P.M.; Sprung, C.L.; Colardyn, F.; Blecher, S. Use of the SOFA score to assess the incidence of organ dysfunction/failure in intensive care units. Crit. Care Med. 1998, 26, 1793–1800. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leung, T.S.; Outlaw, F.; Macdonald, L.W.; Meek, J. Jaundice Eye Color Index (JECI): Quantifying the yellowness of the sclera in jaundiced neonates with digital photography. Biomed. Opt. Express 2019, 10, 1250–1256. [Google Scholar] [CrossRef] [PubMed]
- Prytherch, D.R.; Smith, G.B.; Schmidt, P.E.; Featherstone, P.I. ViEWS—Towards a national early warning score for detecting adult inpatient deterioration. Resuscitation 2010, 81, 932–937. [Google Scholar] [CrossRef] [PubMed]
- Debeer, D.; Strobl, C. Conditional permutation importance revisited. BMC Bioinform. 2020, 21, 1–30. [Google Scholar] [CrossRef] [PubMed]
- Liaw, A.; Wiener, M. Classification and Regression by randomForest. R News 2002, 3, 18–22. [Google Scholar]
- Robin, X.; Turck, N.; Hainard, A.; Tiberti, N.; Lisacek, F.; Sanchez, J.-C.; Müller, M. pROC: An open-source package for R and S+ to analyze and compare ROC curves. BMC Bioinform. 2011, 12, 77. [Google Scholar] [CrossRef] [PubMed]
- Goodwin, A.; Srivastava, V.; Shotton, H.; Protopapa, K.; Butt, A.; Mason, M. Just Day Sepsis! A Review of the Process of Care Received by Patients with Sepsis; National Confidential Enquiry into Patient Outcome and Death: London, UK, 2015; pp. 1–130. Available online: https://www.ncepod.org.uk/2015report2/downloads/JustSaySepsis_FullReport.pdf (accessed on 8 September 2022).
- Wu, C.-L.; Kuo, C.-T.; Shih, S.-J.; Chen, J.-C.; Lo, Y.-C.; Yu, H.-H.; Huang, M.-D.; Sheu, W.; Liu, S.-A. Implementation of an Electronic National Early Warning System to Decrease Clinical Deterioration in Hospitalized Patients at a Tertiary Medical Center. Int. J. Environ. Res. Public Health 2021, 18, 4550. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| NEWS ≥ 5 | qSOFA ≥ 2 | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| N | Sensitivity (95% CI) | Specificity (95% CI) | Positive Predictive Value | Negative Predictive Value | Sensitivity (95% CI) | Specificity (95% CI) | Positive Predictive Value | Negative Predictive Value | |
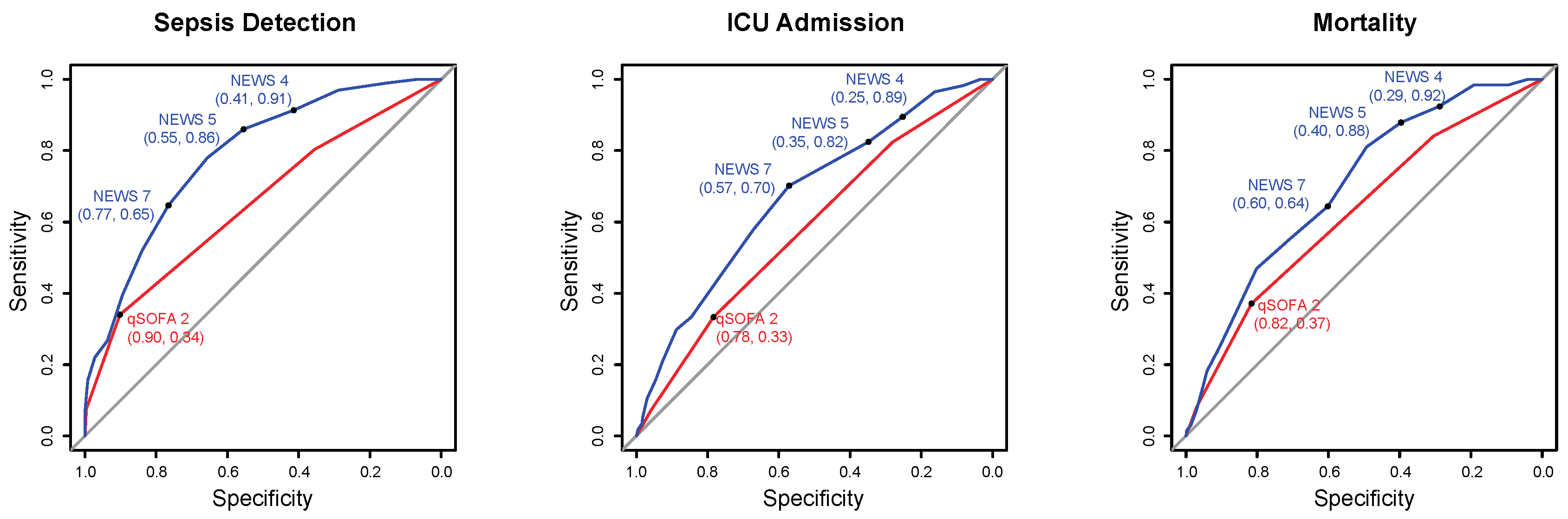
| Sepsis | 300 (54.0%) | 86 (82–90) | 55 (49–62) | 69 (64–74) | 77 (70–83) | 34 (29–40) | 90 (86–94) | 80 (72–87) | 54 (49–59) |
| ICU admission | 57 (10.3%) | 82 (70–91) | 35 (31–39) | 13 (9–16) | 95 (90–97) | 33 (21–47) | 78 (74–82) | 15 (9–22) | 91 (88–94) |
| 28-day mortality | 132 (23.7%) | 88 (81–93) | 40 (35–44) | 31 (27–36) | 91 (86–95) | 37 (29–46) | 82 (78–85) | 39 (30–48) | 81 (77–84) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Durr, D.; Niemi, T.; Despraz, J.; Tusgul, S.; Dami, F.; Akrour, R.; Carron, P.-N.; Le Pogam, M.-A.; Calandra, T.; Meylan, S. National Early Warning Score (NEWS) Outperforms Quick Sepsis-Related Organ Failure (qSOFA) Score for Early Detection of Sepsis in the Emergency Department. Antibiotics 2022, 11, 1518. https://doi.org/10.3390/antibiotics11111518
Durr D, Niemi T, Despraz J, Tusgul S, Dami F, Akrour R, Carron P-N, Le Pogam M-A, Calandra T, Meylan S. National Early Warning Score (NEWS) Outperforms Quick Sepsis-Related Organ Failure (qSOFA) Score for Early Detection of Sepsis in the Emergency Department. Antibiotics. 2022; 11(11):1518. https://doi.org/10.3390/antibiotics11111518
Chicago/Turabian StyleDurr, Dimitri, Tapio Niemi, Jeremie Despraz, Selin Tusgul, Fabrice Dami, Rachid Akrour, Pierre-Nicolas Carron, Marie-Annick Le Pogam, Thierry Calandra, and Sylvain Meylan. 2022. "National Early Warning Score (NEWS) Outperforms Quick Sepsis-Related Organ Failure (qSOFA) Score for Early Detection of Sepsis in the Emergency Department" Antibiotics 11, no. 11: 1518. https://doi.org/10.3390/antibiotics11111518