
Population Pharmacokinetics of Orally Administered Clindamycin to Treat Prosthetic Joint Infections: A Prospective Study
 , ,
, ,
Abstract
:1. Introduction
2. Results
2.1. Patients
2.2. PK Parameters
2.3. Dosing-Regimen Evaluation
3. Discussion
4. Materials and Methods
4.1. Ethics
4.2. Patients
4.3. Treatment
4.4. PK Sampling
4.5. Analytical Methods
4.6. PK Models
4.7. Covariates
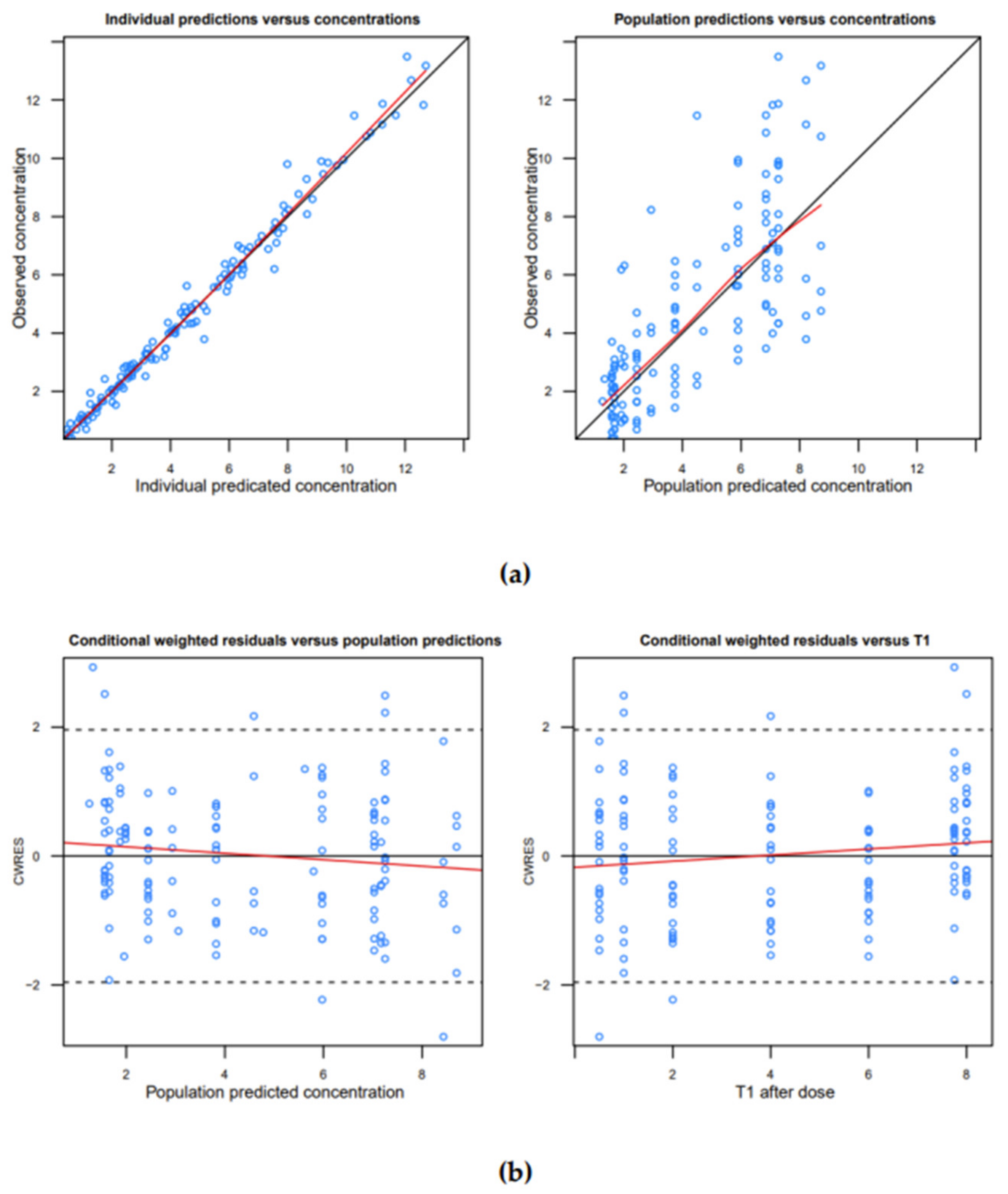
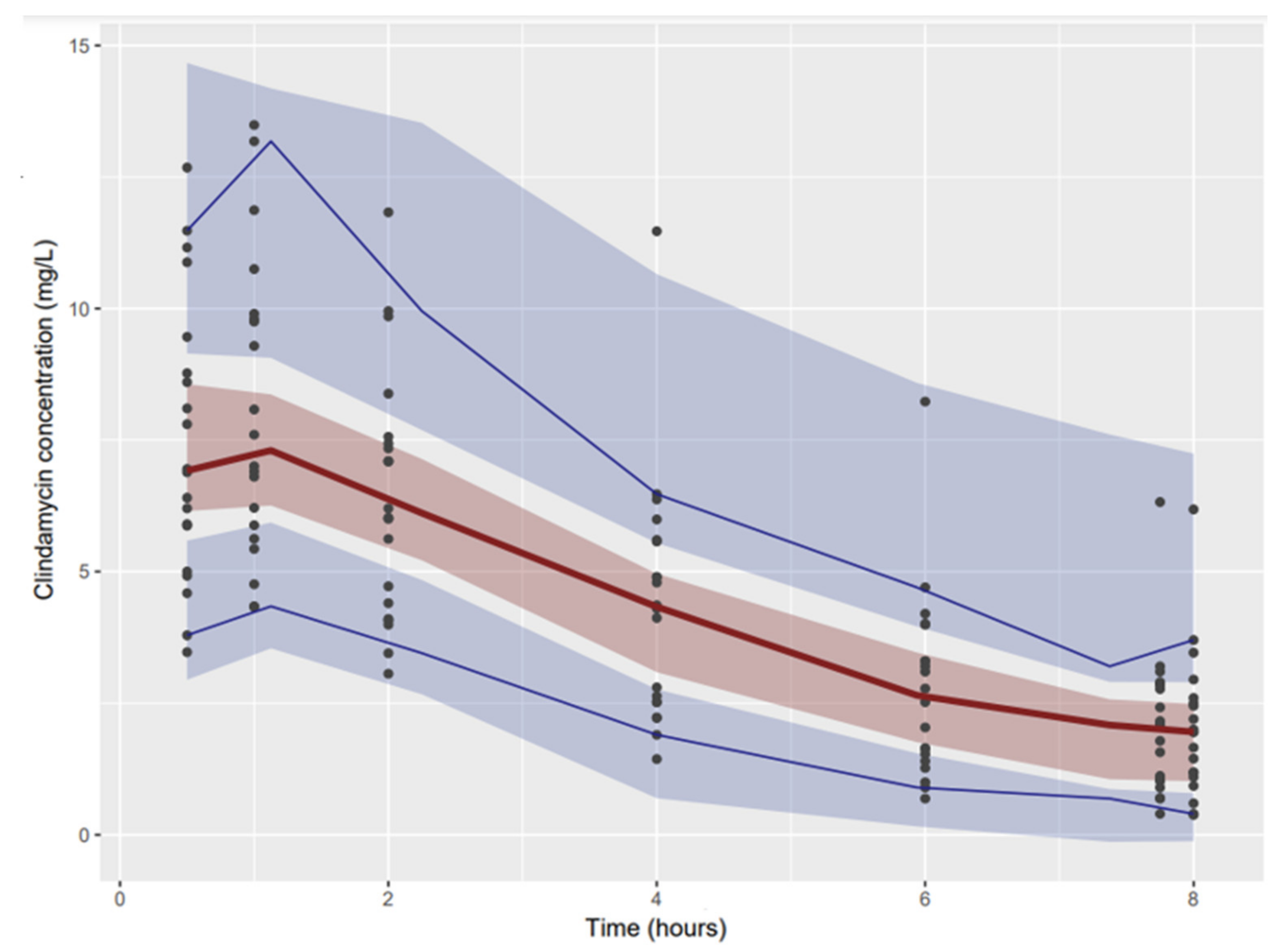
4.8. Model Evaluation
4.9. Dosing-Regimen Simulations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Benito, N.; Franco, M.; Ribera, A.; Soriano, A.; Rodriguez-Pardo, D.; Sorlí, L.; Fresco, G.; Fernández-Sampedro, M.; Dolores del Toro, M.; Guío, L.; et al. Time trends in the aetiology of prosthetic joint infections: A multicentre cohort study. Clin. Microbiol. Infect. 2016, 22, 732.e1–732.e8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Curis, E.; Pestre, V.; Jullien, V.; Eyrolle, L.; Archambeau, D.; Morand, P.; Gatin, L.; Karoubi, M.; Pinar, N.; Dumaine, V.; et al. Pharmacokinetic variability of clindamycin and influence of rifampicin on clindamycin concentration in patients with bone and joint infections. Infection 2015, 43, 473–481. [Google Scholar] [CrossRef] [PubMed]
- Zeller, V.; Dzeing-Ella, A.; Kitzis, M.-D.; Ziza, J.-M.; Mamoudy, P.; Desplaces, N. Continuous Clindamycin Infusion, an Innovative Approach to Treating Bone and Joint Infections. Antimicrob. Agents Chemother. 2010, 54, 88–92. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bouazza, N.; Pestre, V.; Jullien, V.; Curis, E.; Urien, S.; Salmon, D.; Tréluyer, J.-M. Population pharmacokinetics of clindamycin orally and intravenously administered in patients with osteomyelitis. Br. J. Clin. Pharmacol. 2012, 74, 971–977. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zeller, V.; Magreault, S.; Heym, B.; Salmon, D.; Kitzis, M.-D.; Billaud, E.; Marmor, S.; Jannot, A.-S.; Salomon, L.; Jullien, V. Influence of the clindamycin administration route on the magnitude of clindamycin–rifampicin interaction: A prospective pharmacokinetic study. Clin. Microbiol. Infect. 2021, 27, 1857.e1–1857.e7. [Google Scholar] [CrossRef] [PubMed]
- Carrasco-Portugal, M.D.C.; Luján, M.; Flores-Murrieta, F.J. Evaluation of gender in the oral pharmacokinetics of clindamycin in humans. Biopharm. Drug Dispos. 2008, 29, 427–430. [Google Scholar] [CrossRef] [PubMed]
- Gatti, G.; Flaherty, J.; Bubp, J.; White, J.; Borin, M.; Gambertoglio, J. Comparative study of bioavailabilities and pharmacokinetics of clindamycin in healthy volunteers and patients with AIDS. Antimicrob. Agents Chemother. 1993, 37, 1137–1143. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Courjon, J.; Demonchy, E.; Cua, E.; Bernard, E.; Roger, P.-M. Efficacy and safety of clindamycin-based treatment for bone and joint infections: A cohort study. Eur. J. Clin. Microbiol. Infect. Dis. 2017, 36, 2513–2518. [Google Scholar] [CrossRef] [PubMed]
- El Samad, Y.; Havet, E.; Bentayeb, H.; Olory, B.; Canarelli, B.; Lardanchet, J.-F.; Douadi, Y.; Rousseau, F.; Lescure, F.-X.; Mertl, P.; et al. Traitement des infections ostéoarticulaires par clindamycine chez l’adulte. Médecine Et Mal. Infect. 2008, 38, 465–470. [Google Scholar] [CrossRef] [PubMed]
- Bonnaire, A.; Vernet-Garnier, V.; Lebrun, D.; Bajolet, O.; Bonnet, M.; Hentzien, M.; Ohl, X.; Diallo, S.; Bani-Sadr, F. Clindamycin combination treatment for the treatment of bone and joint infections caused by clindamycin-susceptible, erythromycin-resistant Staphylococcus spp. Diagn. Microbiol. Infect. Dis. 2021, 99, 115225. [Google Scholar] [CrossRef] [PubMed]
- Roberts, J.A.; Norris, R.; Paterson, D.L.; Martin, J.H. Therapeutic drug monitoring of antimicrobials. Br. J. Clin. Pharmacol. 2011, 73, 27–36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guilhaumou, R.; Benaboud, S.; Bennis, Y.; Dahyot-Fizelier, C.; Dailly, E.; Gandia, P.; Goutelle, S.; Lefeuvre, S.; Mongardon, N.; Roger, C.; et al. Optimization of the treatment with beta-lactam antibiotics in critically ill patients—Guidelines from the French Society of Pharmacology and Therapeutics (Société Française de Pharmacologie et Thérapeutique—SFPT) and the French Society of Anaesthesia and Intensive Care Medicine (Société Française d’Anesthésie et Réanimation—SFAR). Crit. Care 2019, 23, 104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moore, R.D.; Lietman, P.S.; Smith, C.R. Clinical Response to Aminoglycoside Therapy: Importance of the Ratio of Peak Concentration to Minimal Inhibitory Concentration. J. Infect. Dis. 1987, 155, 93–99. [Google Scholar] [CrossRef]
- Gawronski, K.; Goff, D.A.; Brown, J.; Khadem, T.M.; Bauer, K.A. A Stewardship Program’s Retrospective Evaluation of Vancomycin AUC24/MIC and Time to Microbiological Clearance in Patients with Methicillin-Resistant Staphylococcus aureus Bacteremia and Osteomyelitis. Clin. Ther. 2013, 35, 772–779. [Google Scholar] [CrossRef]
- Scaglione, F. Can we transfer pharmacokinetics/pharmacodynamics of antimicrobials into clinical practice? Int. J. Antimicrob. Agents 2015, 46, S40–S42. [Google Scholar] [CrossRef] [PubMed]
- Thabit, A.K.; Fatani, D.F.; Bamakhrama, M.S.; Barnawi, O.A.; Basudan, L.O.; Alhejaili, S.F. Antibiotic penetration into bone and joints: An updated review. Int. J. Infect. Dis. 2019, 81, 128–136. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Landersdorfer, C.B.; Bulitta, J.B.; Kinzig, M.; Holzgrabe, U.; Sörgel, F. Penetration of Antibacterials into Bone. Clin. Pharmacokinet. 2009, 48, 89–124. [Google Scholar] [CrossRef] [PubMed]
- Ferry, T.; Seng, P.; Mainard, D.; Jenny, J.-Y.; Laurent, F.; Senneville, E.; Grare, M.; Jolivet-Gougeon, A.; Bernard, L.; Marmor, S. The CRIOAc healthcare network in France: A nationwide Health Ministry program to improve the management of bone and joint infection. Orthop. Traumatol. Surg. Res. 2019, 105, 185–190. [Google Scholar] [CrossRef] [PubMed]
- Keizer, R.J.; O Karlsson, M.; Hooker, A. Modeling and Simulation Workbench for NONMEM: Tutorial on Pirana, PsN, and Xpose. CPT Pharmacomet. Syst. Pharmacol. 2013, 2, e50. [Google Scholar] [CrossRef] [PubMed]
- Brendel, K.; Dartois, C.; Comets, E.; Lemenuel-Diot, A.; Laveille, C.; Tranchand, B.; Girard, P.; Laffont, C.M.; Mentré, F. Are population pharmacokinetic and/or pharmacodynamic models adequately evaluated? A survey of the literature from 2002 to 2004. Clin. Pharmacokinet. 2007, 46, 221–234. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristic | Value |
|---|---|
| Males/females, n | 13/7 |
| Body weight (kg) | 76.3 (14.4) |
| Age (years) | 66.5 (15.9) |
| Prothrombin time (%) | 85.7 (12.9) |
| Total proteins (g/L) | 72.8 (6.15) |
| Albumin (g/L) | 37.6 (5.11) |
| Aspartate aminotransferase (IU/L) | 16.0 (4.41) |
| Alanine aminotransferase (IU/L) | 14.6 (6.10) |
| Bilirubin (µmol/L) | 6.83 (3.49) |
| Creatinine (µmol/L) | 73.6 (17.2) |
| C-reactive protein (mg/L) | 47.6 (79.1) |
| Leucocytes (G/L) | 8.19 (3.55) |
| Infection localization, n | |
| Shoulder arthroplasty | 3 |
| Hip arthroplasty | 14 |
| Knee arthroplasty | 3 |
| Original Dataset | Bootstrap | |||
|---|---|---|---|---|
| Parameter | Estimate | RSE | Estimate | RSE |
| Structural model | ||||
| CL/F (L/h) | 23.00 | 8.7% | 23.05 | 9.2% |
| V/F (L) | 103.00 | 8.0% | 102.1 | 7.6% |
| Ka (/h) | 3.53 | 22.4% | 3.71 | 29.6% |
| Interindividual variability | ||||
| ω2 CL/F | 0.14 | 24.7% | 0.136 | 25.9% |
| ω2 V/F | 0.08 | 28.2% | 0.078 | 28.9% |
| ω2 Ka | 0.60 | 46.3% | 0.63 | 66% |
| Residual error | ||||
| Proportional error Additive error | 0.00976 0.0801 | 36.0% 49.0% | 0.009240 0.0827 | 34.4% 43.2% |
| Dosing Regimen | 450 Mg q6h | 600 Mg q8h | 600 Mg q6h | 750 Mg q8h | 750 Mg q6h | 900 Mg q8h | 900 Mg q6h |
|---|---|---|---|---|---|---|---|
| Median 90% CI | 1.73 0.42–4.10 | 1.31 0.21–4.67 | 2.10 0.41–5.51 | 1.51 0.19–4.92 | 2.81 0.63–6.73 | 1.92 0.31–5.89 | 3.38 0.71–8.55 |
| Probability of reaching Ctrough ≥ 2 × MIC | |||||||
| MIC = 0.5 mg/L | 75% | 64% | 81% | 70% | 89% | 76% | 92% |
| MIC = 0.25 mg/L | 93% | 86% | 94% | 85% | 97% | 91% | 98% |
| MIC = 0.125 mg/L | 97% | 93% | 97% | 93% | 99% | 97% | 99% |
| MIC = 0.0625 mg/L | 99% | 97% | 99% | 97% | 100% | 99% | 100% |
| MIC = 0.03125 mg/L | 100% | 99% | 100% | 98% | 100% | 99% | 100% |
| Global PTA for Staphylococcus | 98% | 95% | 98% | 95% | 100% | 98% | 100% |
| Global PTA for Streptococcus | 98% | 96% | 99% | 95% | 99% | 98% | 100% |
| Probability of reaching Ctrough ≥ 8 × MIC | |||||||
| MIC = 0.5 mg/L | 6% | 8% | 16% | 9% | 29% | 15% | 38% |
| MIC = 0.25 mg/L | 39% | 30% | 53% | 37% | 68% | 48% | 74% |
| MIC = 0.125 mg/L | 75% | 64% | 81% | 70% | 89% | 76% | 92% |
| MIC = 0.0625 mg/L | 93% | 86% | 94% | 85% | 97% | 91% | 98% |
| MIC = 0.03125 mg/L | 97% | 93% | 97% | 93% | 99% | 97% | 99% |
| Global PTA for Staphylococcus | 82% | 73% | 86% | 76% | 92% | 82% | 95% |
| Global PTA for Streptococcus | 87% | 79% | 90% | 80% | 94% | 86% | 96% |
| Probability to reach the upper limit concentration | |||||||
| >5 mg/L | 2% | 3% | 8% | 5% | 18% | 9% | 25% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mimram, L.; Magréault, S.; Kerroumi, Y.; Salmon, D.; Kably, B.; Marmor, S.; Jannot, A.-S.; Jullien, V.; Zeller, V. Population Pharmacokinetics of Orally Administered Clindamycin to Treat Prosthetic Joint Infections: A Prospective Study. Antibiotics 2022, 11, 1462. https://doi.org/10.3390/antibiotics11111462
Mimram L, Magréault S, Kerroumi Y, Salmon D, Kably B, Marmor S, Jannot A-S, Jullien V, Zeller V. Population Pharmacokinetics of Orally Administered Clindamycin to Treat Prosthetic Joint Infections: A Prospective Study. Antibiotics. 2022; 11(11):1462. https://doi.org/10.3390/antibiotics11111462
Chicago/Turabian StyleMimram, Léo, Sophie Magréault, Younes Kerroumi, Dominique Salmon, Benjamin Kably, Simon Marmor, Anne-Sophie Jannot, Vincent Jullien, and Valérie Zeller. 2022. "Population Pharmacokinetics of Orally Administered Clindamycin to Treat Prosthetic Joint Infections: A Prospective Study" Antibiotics 11, no. 11: 1462. https://doi.org/10.3390/antibiotics11111462