
Antimicrobial Resistance Policy Protagonists and Processes—A Qualitative Study of Policy Advocacy and Implementation
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Results
2.1. Individual Championship Is Pivotal but Insufficient in the AMR Policymaking Arena
2.2. Policy Institutionalization Facilitates AMR Policy Prioritization and Implementation
2.3. Free Markets Play an Ambivalent Role While Social Norms Are a Driver in AMR Policymaking
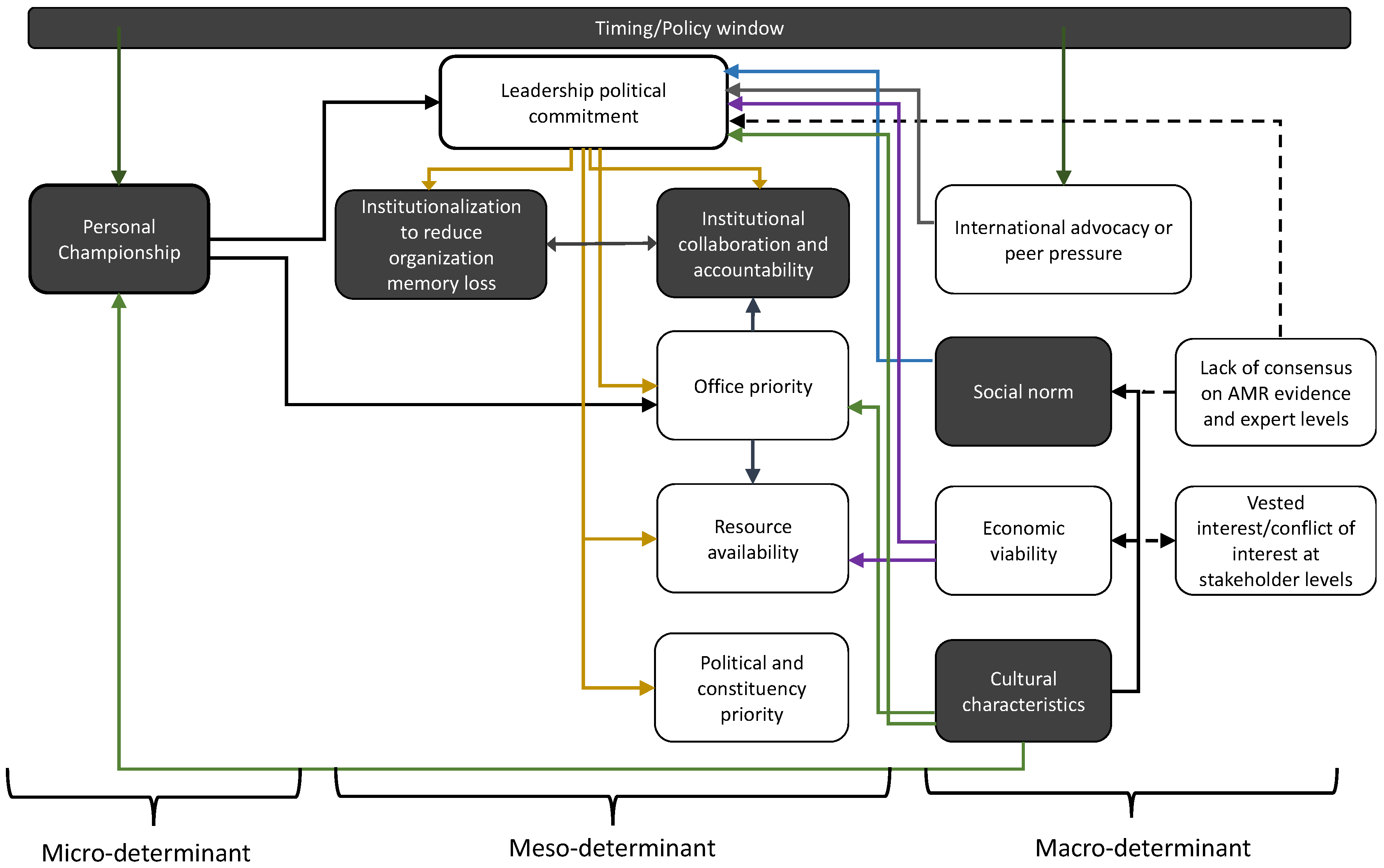
2.4. Summary of AMR Policy Advocacy and Implementation Variables
3. Discussion
4. Methods and Material
4.1. Sampling Technique, Enrolment, and Interview Methodology
4.2. Data Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Acknowledgments
Conflicts of Interest
References
- Paul, R.J.; Varghese, D. AMR in Animal Health: Issues and One Health Solutions for LMICs. In Antimicrobial Resistance; Springer: Berlin/Heidelberg, Germany, 2020; pp. 135–149. [Google Scholar]
- Tacconelli, E.; Pezzani, M.D. Public health burden of antimicrobial resistance in Europe. Lancet Infect. Dis. 2019, 19, 4–6. [Google Scholar] [CrossRef] [Green Version]
- George, A. Antimicrobial resistance, trade, food safety and security. One Health 2018, 5, 6. [Google Scholar] [CrossRef] [PubMed]
- Florez-Cuadrado, D.; Moreno, M.A.; Ugarte-Ruíz, M.; Domínguez, L. Antimicrobial resistance in the food chain in the European Union. Adv. Food Nutr. Res. 2018, 86, 115–136. [Google Scholar] [PubMed]
- Team, E.E. WHO member states adopt global action plan on antimicrobial resistance. Eurosurveillance 2015, 20, 21137. [Google Scholar]
- Mendelson, M.; Matsoso, M.P. The World Health Organization global action plan for antimicrobial resistance. SAMJ S. Afr. Med. J. 2015, 105, 325. [Google Scholar] [CrossRef] [Green Version]
- Hayes, L.; Smith, R.; Duggan, J.; Georgescu, C.; Cole, K. Implementation of an Antimicrobial Restriction Policy: Is the “Paper” More Persuasive? Open Forum Infect. Dis. 2017, 4, S261. [Google Scholar] [CrossRef] [Green Version]
- Sommanustweechai, A.; Tangcharoensathien, V.; Malathum, K.; Sumpradit, N.; Kiatying-Angsulee, N.; Janejai, N.; Jaroenpoj, S. Implementing national strategies on antimicrobial resistance in Thailand: Potential challenges and solutions. Public Health 2018, 157, 142–146. [Google Scholar] [CrossRef]
- Ahmed, S.M.; Naher, N.; Tune, S.N.B.K.; Islam, B.Z. The Implementation of National Action Plan (NAP) on Antimicrobial Resistance (AMR) in Bangladesh: Challenges and Lessons Learned from a Cross-Sectional Qualitative Study. Antibiotics 2022, 11, 690. [Google Scholar] [CrossRef]
- Kaier, K.; Meyer, E.; Dettenkofer, M.; Frank, U. Epidemiology meets econometrics: Using time-series analysis to observe the impact of bed occupancy rates on the spread of multidrug-resistant bacteria. J. Hosp. Infect. 2010, 76, 108–113. [Google Scholar] [CrossRef]
- Wielinga, P.R.; Jensen, V.F.; Aarestrup, F.M.; Schlundt, J. Evidence-based policy for controlling antimicrobial resistance in the food chain in Denmark. Food Control 2014, 40, 185–192. [Google Scholar] [CrossRef]
- Shen, L.; Wei, X.; Yin, J.; Haley, D.R.; Sun, Q.; Lundborg, C.S. Interventions to optimize the use of antibiotics in China: A scoping review of evidence from humans, animals, and the environment from a One Health perspective. One Health 2022, 14, 100388. [Google Scholar] [CrossRef]
- Coast, J.; Smith, R.D.; Millar, M.R. An economic perspective on policy to reduce antimicrobial resistance. Soc. Sci. Med. 1998, 46, 29–38. [Google Scholar] [CrossRef]
- Jit, M.; Ng, D.H.L.; Luangasanatip, N.; Sandmann, F.; Atkins, K.E.; Robotham, J.V.; Pouwels, K.B. Quantifying the economic cost of antibiotic resistance and the impact of related interventions: Rapid methodological review, conceptual framework and recommendations for future studies. BMC Med. 2020, 18, 38. [Google Scholar] [CrossRef] [Green Version]
- Haenssgen, M.J.; Charoenboon, N.; Khine Zaw, Y. It is time to give social research a voice to tackle antimicrobial resistance? J. Antimicrob. Chemother. 2018, 73, 1112–1113. [Google Scholar] [CrossRef] [Green Version]
- Heyman, G.; Cars, O.; Bejarano, M.-T.; Peterson, S. Access, excess, and ethics—Towards a sustainable distribution model for antibiotics. Upsala J. Med. Sci. 2014, 119, 134–141. [Google Scholar] [CrossRef]
- Chandler, C.I. Current accounts of antimicrobial resistance: Stabilisation, individualisation and antibiotics as infrastructure. Palgrave Commun. 2019, 5, 53. [Google Scholar] [CrossRef] [Green Version]
- Charoenboon, N.; Haenssgen, M.J.; Warapikuptanun, P.; Xayavong, T.; Zaw, Y.K. Translating antimicrobial resistance: A case study of context and consequences of antibiotic-related communication in three northern Thai villages. Palgrave Commun. 2019, 5, 23. [Google Scholar] [CrossRef] [Green Version]
- Thornberg, R.; Charmaz, K. Grounded theory and theoretical coding. In The SAGE Handbook of Qualitative Data Analysis; Sage: New York, NY, USA, 2014; Volume 5, pp. 153–169. [Google Scholar]
- Foley, G.; Timonen, V. Using grounded theory method to capture and analyze health care experiences. Health Serv. Res. 2015, 50, 1195–1210. [Google Scholar] [CrossRef] [Green Version]
- Belgrave, L.; Seide, K. Coding for grounded theory. In The SAGE Handbook of Current Developments in Grounded Theory; Sage: London, UK, 2019; pp. 167–185. [Google Scholar]
- Bryant, A.; Charmaz, K. The SAGE Handbook of Current Developments in Grounded Theory; SAGE Publications: London, UK, 2019. [Google Scholar]
- Ogyu, A.; Chan, O.; Littmann, J.; Pang, H.H.; Lining, X.; Liu, P.; Matsunaga, N.; Ohmagari, N.; Fukuda, K.; Wernli, D. National action to combat AMR: A One-Health approach to assess policy priorities in action plans. BMJ Glob. Health 2020, 5, e002427. [Google Scholar] [CrossRef]
- Léger, A.; Lambraki, I.; Graells, T.; Cousins, M.; Henriksson, P.J.; Harbarth, S.; Carson, C.; Majowicz, S.; Troell, M.; Parmley, E.J. AMR-Intervene: A social–ecological framework to capture the diversity of actions to tackle antimicrobial resistance from a One Health perspective. J. Antimicrob. Chemother. 2021, 76, 1–21. [Google Scholar] [CrossRef]
- Arnold, G. Does entrepreneurship work? Understanding what policy entrepreneurs do and whether it matters. Policy Stud. J. 2021, 49, 968–991. [Google Scholar] [CrossRef]
- Blaskovich, M.A. Antibiotics Special Issue: Challenges and Opportunities in Antibiotic Discovery and Development. ACS Infect. Dis. 2020, 6, 1286–1288. [Google Scholar] [CrossRef]
- Chan, O.S.K.; Wernli, D.; Liu, P.; Tun, H.M.; Fukuda, K.; Lam, W.; Xiao, Y.H.; Zhou, X.; Grépin, K.A. Unpacking Multi-Level Governance of Antimicrobial Resistance Policies: The Case of Guangdong, China. Health Policy Plan. 2022, 37, 1148–1157. [Google Scholar] [CrossRef]
- Schmid, N.; Sewerin, S.; Schmidt, T.S. Explaining Advocacy Coalition Change with Policy Feedback. Policy Stud. J. 2020, 48, 1109–1134. [Google Scholar] [CrossRef]
- Ancillotti, M.; Eriksson, S.; Veldwijk, J.; Fahlquist, J.N.; Andersson, D.I.; Godskesen, T. Public awareness and individual responsibility needed for judicious use of antibiotics: A qualitative study of public beliefs and perceptions. BMC Public Health 2018, 18, 1153. [Google Scholar] [CrossRef] [Green Version]
- Weible, C.M.; Sabatier, P.A. Theories of the Policy Process, 4th ed.; Routledge: London, UK, 2018; Volume 1. [Google Scholar]
- Axelrod, R. Structure of Decision: The Cognitive Maps of Political Elites; Princeton University Press: Princeton, NJ, USA, 2015. [Google Scholar]
- Pope, C.; Ziebland, S.; Mays, N. Analysing qualitative data. BMJ 2000, 320, 114–116. [Google Scholar] [CrossRef]
- Bradley, E.H.; Curry, L.A.; Devers, K.J. Qualitative data analysis for health services research: Developing taxonomy, themes, and theory. Health Serv. Res. 2007, 42, 1758–1772. [Google Scholar] [CrossRef] [Green Version]
- Gilson, L. Qualitative research synthesis for health policy analysis: What does it entail and what does it offer? Health Policy Plan. 2014, 29, iii1–iii5. [Google Scholar] [CrossRef] [Green Version]
- Barnett-Page, E.; Thomas, J. Methods for the synthesis of qualitative research: A critical review. BMC Med. Res. Methodol. 2009, 9, 59. [Google Scholar] [CrossRef] [Green Version]
- Tong, A.; Sainsbury, P.; Craig, J. Consolidated criteria for reporting qualitative research (COREQ): A 32-item checklist for interviews and focus groups. Int. J. Qual. Health Care 2007, 19, 349–357. [Google Scholar] [CrossRef]
- Jenkins-Smith, H.C.; Nohrstedt, D.; Weible, C.M.; Ingold, K. The advocacy coalition framework: An overview of the research program. In Theories of the Policy Process; Routledge: London, UK, 2018; pp. 135–171. [Google Scholar]
- Weible, C.M.; Sabatier, P.A. A guide to the advocacy coalition framework. In Handbook of Public Policy Analysis; CRC Press: Boca Raton, FL, USA, 2006; pp. 123–136. [Google Scholar]


{kind=link}
| Index-Code | Numbers | Variables to Be Determined | Sample Questions | Index-Code | Numbers | Variables to Be Determined | Sample Questions | ||
|---|---|---|---|---|---|---|---|---|---|
| Micro-determinants | MI | 1 | Perceived responsibility in personal advocacy/personal championship | Why do you decide to advocate for AMR issues? | Macro-determinants | MA | 1 | Social influence and consumer behavior influences AMR policy advocacy | When it comes to civil society and social norm, can you say a bit more about that? |
| MI | 2 | Perceived personal political capacity and connections | What was your role or goal in the (office/parliament/organization) related to AMR policies? | MA | 2 | International organization influence AMR policy advocacy | You can take an economic argument, you can take a political argument that everybody else is moving in this direction and will be left behind and so on. So, in terms of tools and strategies at that level were there any particular approach that (the country/office/organization) took? | ||
| MI | 3 | Perceived risk or benefits in political career | Why did you decide that you needed to achieve to prioritize or put AMR on the agenda? How does that affect your role and responsibility in your (cabinet/office/instiution)? | MA | 3 | Economic influence or pressure influence AMR policy advocacy | |||
| MI | 4 | Perception of sufficient support to advocate, prioritize or formulate policy | Do you see that AMR and (the country) moving on AMR the stars aligned and a group of things came together. What were the factors that prompt you to push for AMR? | MA | 4 | Resources and capacity availability limits or enables AMR policy advocacy | What logic, what arguments, what other factors did you find most important in successfully taking AMR forward? Including with peers and others. Specifically, how did you use health, science, politics, economic perspective | ||
| MI | 5 | Of opinion that AMR is a traceable problem translatable to policy | ….question then is, what were the primary goals that you were calling when taking on an AMR? What do you see about AMR that means to you in terms of advocating for prioritization on the agenda? | MA | 5 | Legislation ease, hurdles, and poltical climate influences AMR policy advocacy | Do you think that this was an approach primarily as a health issue that the political side could help facilitate, or, it was really more of a political issue and this was an opportunity to move on that in terms of, moving ahead with (country/s) concerns and enrolling others and trying to further those political aims? | ||
| MI | 6 | Perception of positive possibility to prioritize AMR on agenda | What were the most important reasons for you or for your Department in deciding to make AMR a major priority? | MA | 6 | Collaboration or isolation among different offices influences AMR policy development | What was the step, or what would have been the step for translating that Department of Health document into a priority, which mobilized you in the (your) Office? | ||
| MI | 7 | Of opinion that AMR is a solvable issue | Do you think AMR is a solvable issue? | MA | 7 | Consensus/social norm among entities and organization within country influences AMR policy development | Were they driving it? Were they holding it back? Were they as important as the government voices in initiating this conversation? | ||
| MI | 8 | Of opinion that AMR aligns with decision maker’s core belief | Do you think when you spoke to (Decision maker/policy entrepreneur), do you think AMR strikes with his/her core belief? | MA | 8 | Global and regional collaboration influences AMR policy advocacy | In the beginning when you were looking at AMR both as a national issue and as you get into the complexity, you see it more as an international issue. How did the perspective or goals evolve? Did they become more specific or general? | ||
| MI | 9 | Of opinion that AMR is a priority within office or former office | What was your job title and what were your general responsibilities? In the context of that, can you say a little bit about how your working relationship works in the day-to-day basis of your posting? How and what you would say about your office’s role in AMR policies(Personal/professional responsibility clarification)? | MA | 9 | Professional support or not influences AMR policy advocacy | Do you think AMR policy has the traction to win over everyone (medical professionals, farming industries, pharmaceuticals) that had to be won over? Do these stakeholders do what they have to do and is that important? | ||
| MI | 10 | Previous knowledge and experience influence belief in mitigating AMR | MA | 10 | Cultural, historical, geographical and anthropological contextual influences AMR policy development | Could these have come together for another topic or was AMR a relatively unique among the different health issues that, you know, (the country) was facing? Could (your country’s) cultural, historical, geographical and anthrological context influence how AMR policy developed? | |||
| Meso-determinants sample questions: | |||||||||
| |||||||||
| Main Position(s) and Role(s) Associated with Antimicrobial Resistance Policymaking | |||||||
|---|---|---|---|---|---|---|---|
| Countries | Number of Interviewees | Policy Makers | Hospital Directors and Leaders | Healthcare and Public Health Officials | Medical Professionals (Pharmacists, Dentists, Doctors & Veterinarians) | Diplomat, Bureacrats, and Policy Administrators | Policy Advisors |
| China * | 12 | 3 | 2 | 3 | 10 | 3 | 8 |
| Japan | 5 | 0 | 3 | 1 | 3 | 0 | 3 |
| Norway | 6 | 1 | 0 | 2 | 2 | 0 | 5 |
| UK | 6 | 2 | 0 | 1 | 2 | 2 | 6 |
| USA | 5 | 1 | 0 | 3 | 4 | 1 | 5 |
| Thematic Key Findings | Country-Based Key Findings | |
|---|---|---|
| 1 | Personal championship is key to initiation of AMR policy advocacy. | Norway’s AMR policy protagonists viewed unified understanding against AMR enables its policy advocacy. Interviewees also see coherent public health, healthcare, and farming system facilitators of AMR policy implementation. |
| 2 | Timing is important for policy protagonists to advocate and/or implement AMR policies | The UK AMR protagonists mobilized national effort to influence international and One Health AMR advocacy. |
| 3 | Institutional memory is important for policy durability and especially for implementation, which has proven to be a challenge in many countries. | China AMR policy protagonists sees top-to-bottom policies that advocate and implement AMR policies in food security, professional training, public education, and antimicrobial regulation issues. |
| 4 | Institutionalization, institutions’ connectedness, and collaboration are keys to sustain policy development but still faces challenges in change of constituencies. | The US policy protagonists view public-private partnership in AMR a key approach in policy advocacy and implementation in hospital and health insurance sectors. |
| 5 | Free market plays an ambivalent role while social norm is important enabler in AMR policy prioritization. | Japan and China’s AMR policy advocacy benefit from strong international AMR leadership and policy advocacy. |
| 6 | Culture, socioeconomic, and ethnographic variables enable or inhibit policy protagonists in AMR policy advocacy and/or implementation |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chan, O.S.K.; Lam, W.W.T.; Fukuda, K.; Tun, H.M.; Ohmagari, N.; Littmann, J.; Zhou, X.D.; Xiao, Y.; Liu, P.; Wernli, D. Antimicrobial Resistance Policy Protagonists and Processes—A Qualitative Study of Policy Advocacy and Implementation. Antibiotics 2022, 11, 1434. https://doi.org/10.3390/antibiotics11101434
Chan OSK, Lam WWT, Fukuda K, Tun HM, Ohmagari N, Littmann J, Zhou XD, Xiao Y, Liu P, Wernli D. Antimicrobial Resistance Policy Protagonists and Processes—A Qualitative Study of Policy Advocacy and Implementation. Antibiotics. 2022; 11(10):1434. https://doi.org/10.3390/antibiotics11101434
Chicago/Turabian StyleChan, Olivia S. K., Wendy W. T. Lam, Keiji Fukuda, Hein Min Tun, Norio Ohmagari, Jasper Littmann, Xu Dong Zhou, Yonghong Xiao, Ping Liu, and Didier Wernli. 2022. "Antimicrobial Resistance Policy Protagonists and Processes—A Qualitative Study of Policy Advocacy and Implementation" Antibiotics 11, no. 10: 1434. https://doi.org/10.3390/antibiotics11101434